
Diagnostic Efficacy of Chest Computed Tomography with a Dual-Reviewer Approach in Patients Diagnosed with Pneumonia Secondary to Severe Acute Respiratory Syndrome Coronavirus 2

 ,
,  ,
,  , , , , ,
, , , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Song, F.; Shi, N.; Shan, F.; Zhang, Z.; Shen, J.; Lu, H.; Ling, Y.; Jiang, Y.; Shi, Y. Emerging 2019 novel coronavirus (2019-nCoV) pneumonia. Radiology 2020, 295, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Umakanthan, S.; Sahu, P.; Ranade, A.V.; Bukelo, M.M.; Rao, J.S.; Abrahao-Machado, L.F.; Dahal, S.; Kumar, H.; Kv, D. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad. Med. J. 2020, 96, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Wang, G.; Cai, X.P.; Deng, J.W.; Zheng, L.; Zhu, H.H.; Zheng, M.; Yang, B.; Chen, Z. An overview of COVID-19. J. Zhejiang Univ. Sci. B 2020, 21, 343–360. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Liu, X.; Xiong, L.; Cai, K. Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2: A systematic review and meta-analysis. J. Med. Virol. 2020, 92, 1449–1459. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Lu, Y.; Lure, F.; Jaeger, S.; Lu, P. Clinical and radiological features of novel coronavirus pneumonia. J. X-ray Sci. Technol. 2020, 28, 391–404. [Google Scholar] [CrossRef] [PubMed]
- Filchakova, O.; Dossym, D.; Ilyas, A.; Kuanysheva, T.; Abdizhamil, A.; Bukasov, R. Review of COVID-19 testing and diagnostic methods. Talanta 2022, 244, 123409. [Google Scholar] [CrossRef] [PubMed]
- Falaschi, Z.; Danna, P.S.C.; Arioli, R.; Pasché, A.; Zagaria, D.; Percivale, I.; Tricca, S.; Barini, M.; Aquilini, F.; Andreoni, S.; et al. Chest CT accuracy in diagnosing COVID-19 during the peak of the Italian epidemic: A retrospective correlation with RT-PCR testing and analysis of discordant cases. Eur. J. Radiol. 2020, 130, 109192. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Simundic, A.M.; Plebani, M. Potential preanalytical and analytical vulnerabilities in the laboratory diagnosis of coronavirus disease 2019 (COVID-19). Clin. Chem. Lab. Med. 2020, 58, 1070–1076. [Google Scholar] [CrossRef]
- Guo, J.; Ge, J.; Guo, Y. Recent advances in methods for the diagnosis of Corona Virus Disease 2019. J. Clin. Lab. Anal. 2022, 36, e24178. [Google Scholar] [CrossRef]
- Prokop, M.; Van Everdingen, W.; van Rees Vellinga, T.; Quarles van Ufford, H.; Stöger, L.; Beenen, L.; Geurts, B.; Gietema, H.; Krdzalic, J.; Schaefer-Prokop, C.; et al. CO-RADS: A Categorical CT Assessment Scheme for Patients Suspected of Having COVID-19-Definition and Evaluation. Radiology 2020, 296, E97–E104. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Jiang, X.; Hong, Y.; Wen, Z.; Wei, S.; Peng, G.; Wei, X. Can Chest CT Features Distinguish Patients with Negative from Those with Positive Initial RT-PCR Results for Coronavirus Disease (COVID-19)? Am. J. Roentgenol. 2021, 216, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Alsharif, W.; Qurashi, A. Effectiveness of COVID-19 diagnosis and management tools: A review. Radiography 2021, 27, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Reginelli, A.; Grassi, R.; Feragalli, B.; Belfiore, M.P.; Montanelli, A.; Patelli, G.; La Porta, M.; Urraro, F.; Fusco, R.; Granata, V.; et al. Coronavirus Disease 2019 (COVID-19) in Italy: Double Reading of Chest CT Examination. Biology 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, E.K.U.N.; Loureiro, B.M.C.; Strabelli, D.G.; Farias, L.D.P.G.D.; Garcia, J.V.R.; Gama, V.A.A.; Ferreira, L.C.; Chate, R.C. Evaluation of the RSNA and CORADS classifications for COVID-19 on chest computed tomography in the Brazilian population. Clinics 2021, 76, e2476. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Ravikanth, R. Diagnostic accuracy and false-positive rate of chest CT as compared to RT-PCR in coronavirus disease 2019 (COVID-19) pneumonia: A prospective cohort of 612 cases from India and review of literature. Indian J. Radiol. Imaging 2021, 31 (Suppl. S1), S161–S169. [Google Scholar] [CrossRef]
- Kovács, A.; Palásti, P.; Veréb, D.; Bozsik, B.; Palkó, A.; Kincses, Z.T. The sensitivity and specificity of chest CT in the diagnosis of COVID-19. Eur. Radiol. 2021, 31, 2819–2824. [Google Scholar] [CrossRef]
- Böger, B.; Fachi, M.M.; Vilhena, R.O.; Cobre, A.F.; Tonin, F.S.; Pontarolo, R. Systematic review with meta-analysis of the accuracy of diagnostic tests for COVID-19. Am. J. Infect. Control. 2021, 49, 21–29. [Google Scholar] [CrossRef]
- Long, C.; Xu, H.; Shen, Q.; Zhang, X.; Fan, B.; Wang, C.; Zeng, B.; Li, Z.; Li, X.; Li, H. Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur. J. Radiol. 2020, 126, 108961. [Google Scholar] [CrossRef]
- Udugama, B.; Kadhiresan, P.; Kozlowski, H.N.; Malekjahani, A.; Osborne, M.; Li, V.Y.C.; Chen, H.; Mubareka, S.; Gubbay, J.B.; Chan, W.C.W. Diagnosing COVID-19: The Disease and Tools for Detection. ACS Nano. 2020, 14, 3822–3835. [Google Scholar] [CrossRef] [PubMed]
- Younes, N.; Al-Sadeq, D.W.; Al-Jighefee, H.; Younes, S.; Al-Jamal, O.; Daas, H.I.; Yassine, H.M.; Nasrallah, G.K. Challenges in Laboratory Diagnosis of the Novel Coronavirus SARS-CoV-2. Viruses 2020, 12, 582. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Chen, Y.; Runa, A.; Liu, J. Diagnostic performance of CO-RADS for COVID-19: A systematic review and meta-analysis. Eur. Radiol. 2022, 32, 4414–4426. [Google Scholar] [CrossRef] [PubMed]
- Inanc, I.H.; Bursa, N.; Gultepe, A.; Bayramoğlu, M.; Sabanoglu, C.; Inanc, F.A. Association among CO-RADS score, co-morbid diseases, and short-term prognosis in COVID-19 infection. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 653–663. [Google Scholar] [PubMed]
- Vicini, S.; Panvini, N.; Bellini, D.; Rengo, M.; Ciotola, M.; De Vivo, M.; Gambaretto, C.; Caldon, V.; Panno, S.; Del Borgo, C.; et al. Radiographers and COVID-19 pneumonia: Diagnostic performance using CO-RADS. Radiography 2021, 27, 1078–1084. [Google Scholar] [CrossRef] [PubMed]
- Valentin, B.; Steuwe, A.; Wienemann, T.; Andree, M.; Keitel, V.; Ljimani, A.; Appel, E.; Köhler, M.-H.; Rademacher, C.; Aissa, J.; et al. Applicability of CO-RADS in anonymized cohort including early and advanced stages of COVID-19 in comparison to the recommendations of the German Radiological Society and Radiological Society of North America. Thieme 2022, 194, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Wu, X.; Zeng, W.; Guo, D.; Fang, Z.; Chen, L.; Huang, H.; Li, C. Chest CT Findings in Patients with Coronavirus Disease 2019 and Its Relationship with Clinical Features. Investig. Radiol. 2020, 55, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Himoto, Y.; Sakata, A.; Kirita, M.; Hiroi, T.; Kobayashi, K.-I.; Kubo, K.; Kim, H.; Nishimoto, A.; Maeda, C.; Kawamura, A.; et al. Diagnostic performance of chest CT to differentiate COVID-19 pneumonia in non-high-epidemic area in Japan. Jpn. J. Radiol. 2020, 38, 400–406. [Google Scholar] [CrossRef]
- Cheng, Z.; Lu, Y.; Cao, Q.; Qin, L.; Pan, Z.; Yan, F.; Yang, W. Clinical Features and Chest CT Manifestations of Coronavirus Disease 2019 (COVID-19) in a Single-Center Study in Shanghai, China. Am. J. Roentgenol. 2020, 215, 121–126. [Google Scholar] [CrossRef]
- Caruso, D.; Zerunian, M.; Polici, M.; Pucciarelli, F.; Polidori, T.; Rucci, C.; Guido, G.; Bracci, B.; De Dominicis, C.; Laghi, A. Chest CT Features of COVID-19 in Rome, Italy. Radiology 2020, 296, E79–E85. [Google Scholar] [CrossRef]
- Islam, N.; Ebrahimzadeh, S.; Salameh, J.P.; Kazi, S.; Fabiano, N.; Treanor, L.; Absi, M.; Hallgrimson, Z.; Leeflang, M.M.; Hooft, L.; et al. Thoracic imaging tests for the diagnosis of COVID-19. Cochrane Database Syst. Rev. 2020, 11, CD013639. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CO-RADS | |||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| Reviewer 1 | 94 (10.6%) | 134 (15.1%) | 146 (16.4%) | 129 (14.5%) | 387 (43.5%) |
| Reviewer 2 | 104 (11.7%) | 97 (10.9%) | 226 (25.4%) | 149 (16.7%) | 314 (35.6%) |
| Consensus | 93 (10.4%) | 116 (13%) | 152 (17.1%) | 153 (17.2%) | 376 (42.2%) |
| RT–PCR SARS-CoV-2 | |||
|---|---|---|---|
| CO-RADS | Positive (A) | Negative (B) | |
| Reviewer 1 | 1 | 12 (2.5%) | 82 (20.1%) |
| 2 | 8 (1.7%) | 126 (30.9%) | |
| 3 | 88 (18.3%) | 58 (14.2%) | |
| 4 | 96 (19.9%) | 33 (8.1%) | |
| 5 | 278 (57.7%) | 109 (26.7%) | |
| Reviewer 2 | 1 | 17 (3.5%) | 87 (21.3%) |
| 2 | 17 (3.5%) | 80 (19.6%) | |
| 3 | 116 (24.1%) | 110 (27%) | |
| 4 | 101 (21%) | 48 (11.8%) | |
| 5 | 231 (47.9%) | 83 (20.3%) | |
| Consensus | 1 | 11 (2.2%) | 82 (20.1%) |
| 2 | 4 (0.9%) | 112 (27.4%) | |
| 3 | 72 (14.9%) | 80 (19.6%) | |
| 4 | 122 (25.3%) | 31 (7.6%) | |
| 5 | 273 (56.6%) | 103 (25.2%) | |
| RT–PCR SARS-CoV-2 Chest CT | Positive for SARS-CoV-2 | Negative for SARS-CoV-2 |
|---|---|---|
| Reviewer 1 | ||
| Positive for COVID-19 | 374 | 142 |
| Negative for COVID-19 | 108 | 266 |
| Reviewer 2 | ||
| Positive for COVID-19 | 332 | 131 |
| Negative for COVID-19 | 150 | 277 |
| Consensus | ||
| Positive for COVID-19 | 395 | 134 |
| Negative for COVID-19 | 87 | 274 |
| Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value | |
|---|---|---|---|---|
| Reviewer 1 | 78% | 65% | 72% | 71% |
| Reviewer 2 | 69% | 68% | 72% | 65% |
| Consensus | 82% | 67% | 75% | 76% |
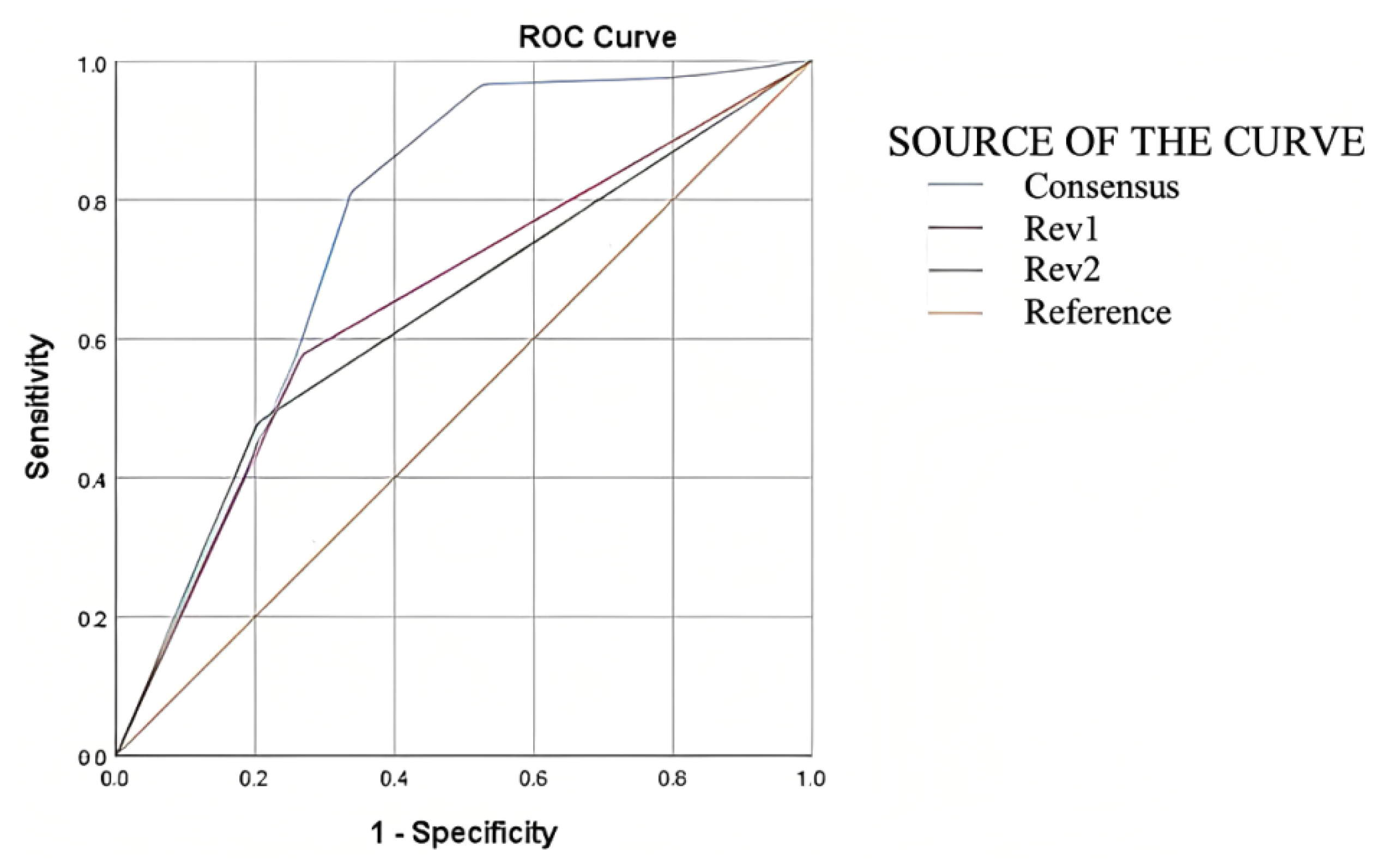
| Area under the ROC Curve | |||||
|---|---|---|---|---|---|
| Test Result Variable(s) | Area | Std. Error | Asymptotic Sig. | Asymptotic 95% Confidence Interval | |
| p | Lower Bound | Upper Bound | |||
| Reviewer 1 | 0.655 | 0.018 | <0.001 | 0.619 | 0.691 |
| Reviewer 2 | 0.638 | 0.019 | <0.001 | 0.602 | 0.674 |
| Consensus | 0.760 | 0.017 | <0.001 | 0.726 | 0.798 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castellanos-Bermejo, J.E.; Cervantes-Guevara, G.; Cervantes-Pérez, E.; Cervantes-Cardona, G.A.; Ramírez-Ochoa, S.; Fuentes-Orozco, C.; Delgado-Hernández, G.; Tavares-Ortega, J.A.; Gómez-Mejía, E.; Chejfec-Ciociano, J.M.; et al. Diagnostic Efficacy of Chest Computed Tomography with a Dual-Reviewer Approach in Patients Diagnosed with Pneumonia Secondary to Severe Acute Respiratory Syndrome Coronavirus 2. Tomography 2023, 9, 1617-1628. https://doi.org/10.3390/tomography9050129
Castellanos-Bermejo JE, Cervantes-Guevara G, Cervantes-Pérez E, Cervantes-Cardona GA, Ramírez-Ochoa S, Fuentes-Orozco C, Delgado-Hernández G, Tavares-Ortega JA, Gómez-Mejía E, Chejfec-Ciociano JM, et al. Diagnostic Efficacy of Chest Computed Tomography with a Dual-Reviewer Approach in Patients Diagnosed with Pneumonia Secondary to Severe Acute Respiratory Syndrome Coronavirus 2. Tomography. 2023; 9(5):1617-1628. https://doi.org/10.3390/tomography9050129
Chicago/Turabian StyleCastellanos-Bermejo, Jaime E., Gabino Cervantes-Guevara, Enrique Cervantes-Pérez, Guillermo A. Cervantes-Cardona, Sol Ramírez-Ochoa, Clotilde Fuentes-Orozco, Gonzalo Delgado-Hernández, Jaime A. Tavares-Ortega, Erika Gómez-Mejía, Jonathan M. Chejfec-Ciociano, and et al. 2023. "Diagnostic Efficacy of Chest Computed Tomography with a Dual-Reviewer Approach in Patients Diagnosed with Pneumonia Secondary to Severe Acute Respiratory Syndrome Coronavirus 2" Tomography 9, no. 5: 1617-1628. https://doi.org/10.3390/tomography9050129
APA StyleCastellanos-Bermejo, J. E., Cervantes-Guevara, G., Cervantes-Pérez, E., Cervantes-Cardona, G. A., Ramírez-Ochoa, S., Fuentes-Orozco, C., Delgado-Hernández, G., Tavares-Ortega, J. A., Gómez-Mejía, E., Chejfec-Ciociano, J. M., Flores-Prado, J. A., Barbosa-Camacho, F. J., & González-Ojeda, A. (2023). Diagnostic Efficacy of Chest Computed Tomography with a Dual-Reviewer Approach in Patients Diagnosed with Pneumonia Secondary to Severe Acute Respiratory Syndrome Coronavirus 2. Tomography, 9(5), 1617-1628. https://doi.org/10.3390/tomography9050129