
Radiation-Free Microwave Technology for Breast Lesion Detection Using Supervised Machine Learning Model

 ,
,  ,
, 
 ,
,  and
and
Abstract
1. Introduction
Contribution towards This Research
2. Materials and Methods
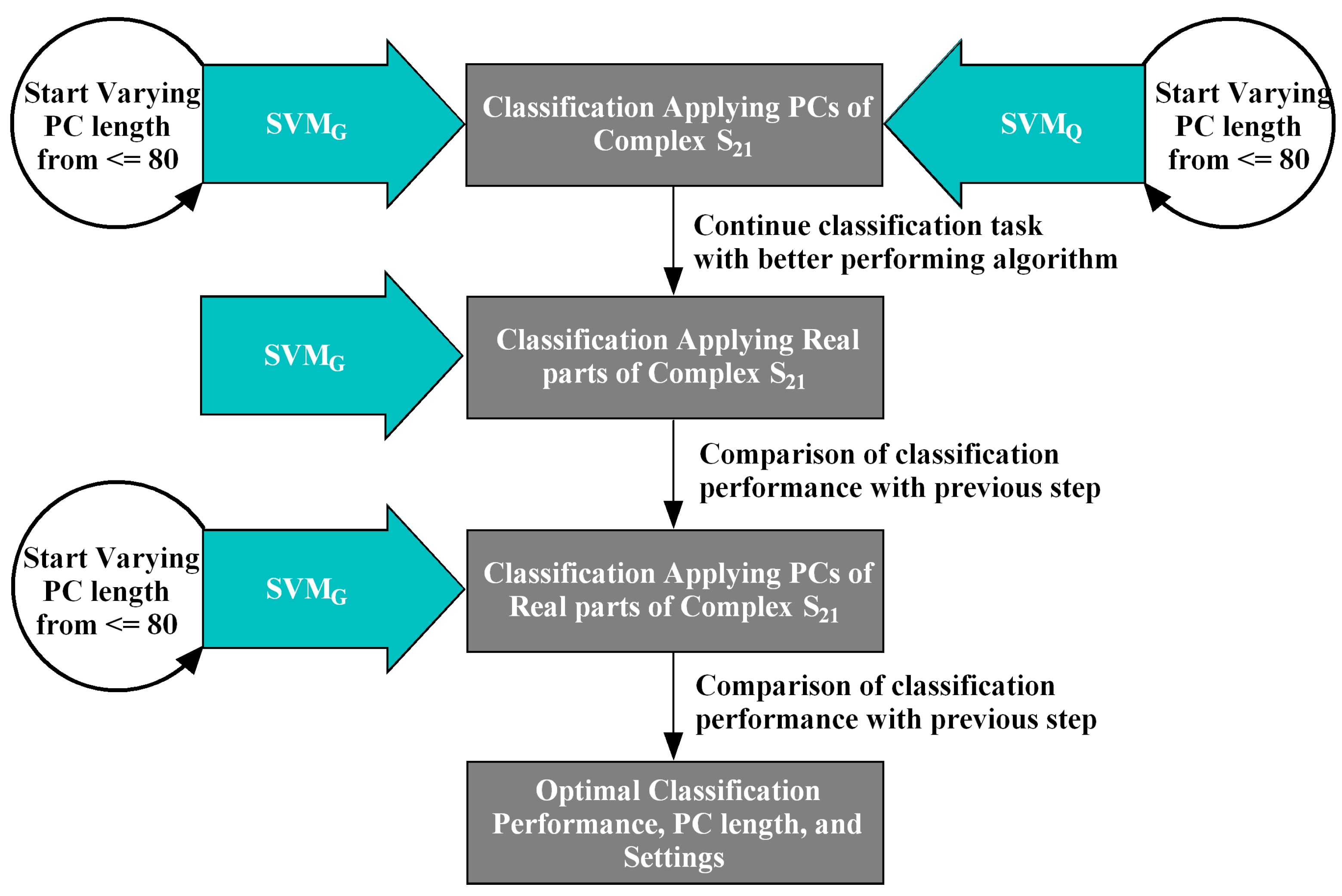
- MammoWave breast signal classification considering features extracted from the complex responses. Features have been extracted using PCA a powerful mathematical tool for multivariate data transformation. has been chosen for the ML task applying the team’s previous research. Subsequently, has been experimented alongside observing spherical data shapes for improved classification performed better than here, thus has been further adopted for the following classification tasks.
- MammoWave breast signal classification considering real parts of complex responses and employing .
- MammoWave breast signal classification considering features extracted (by PCA) from real parts of complex and employing .
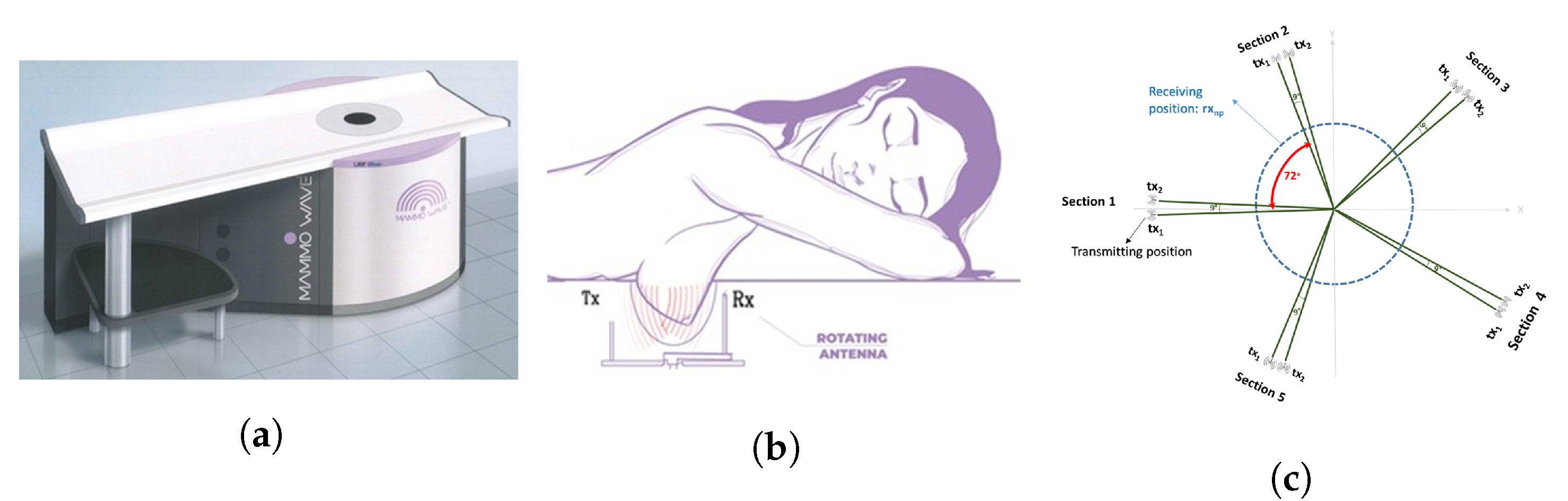
Apparatus Description and Data Collection
3. Proposed Methodology
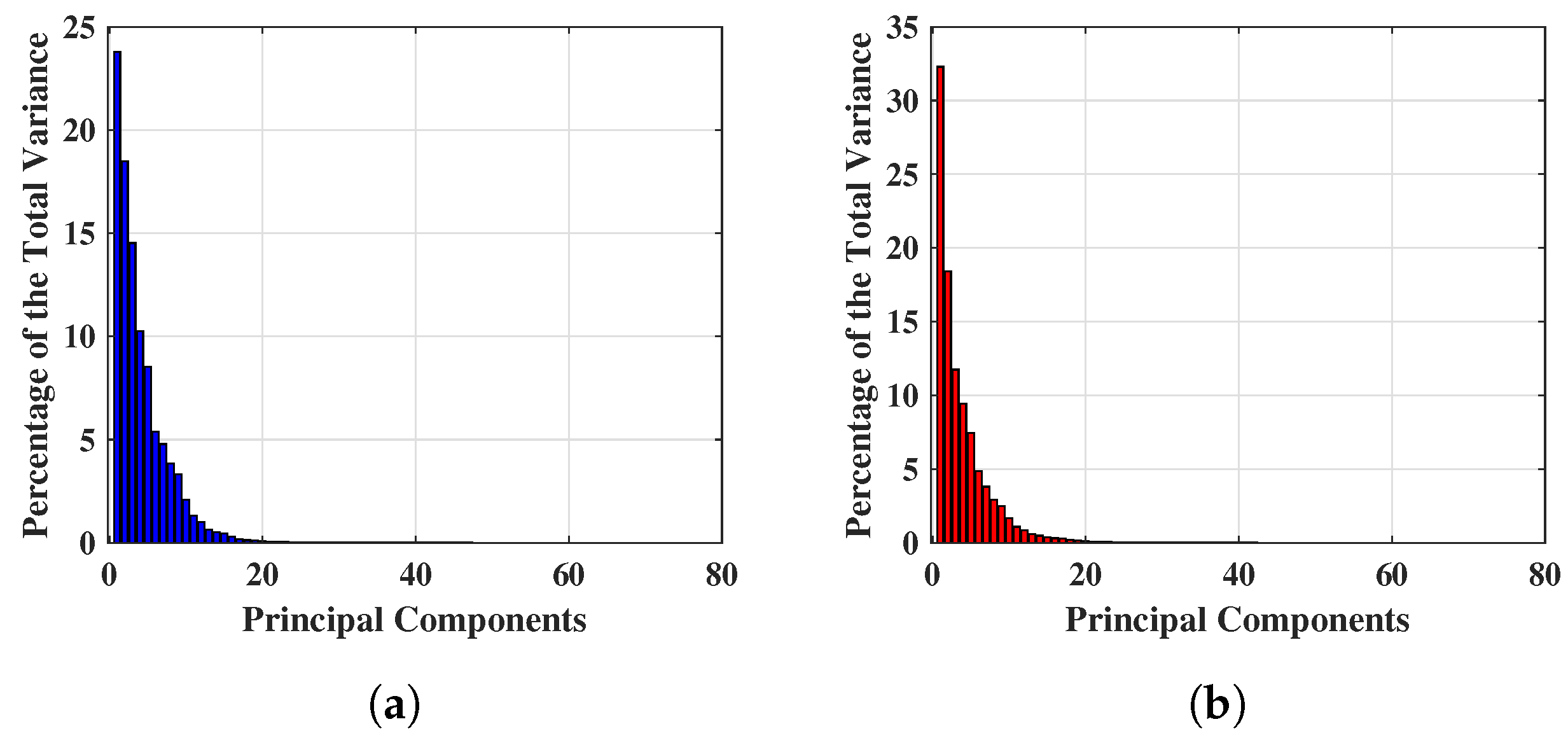
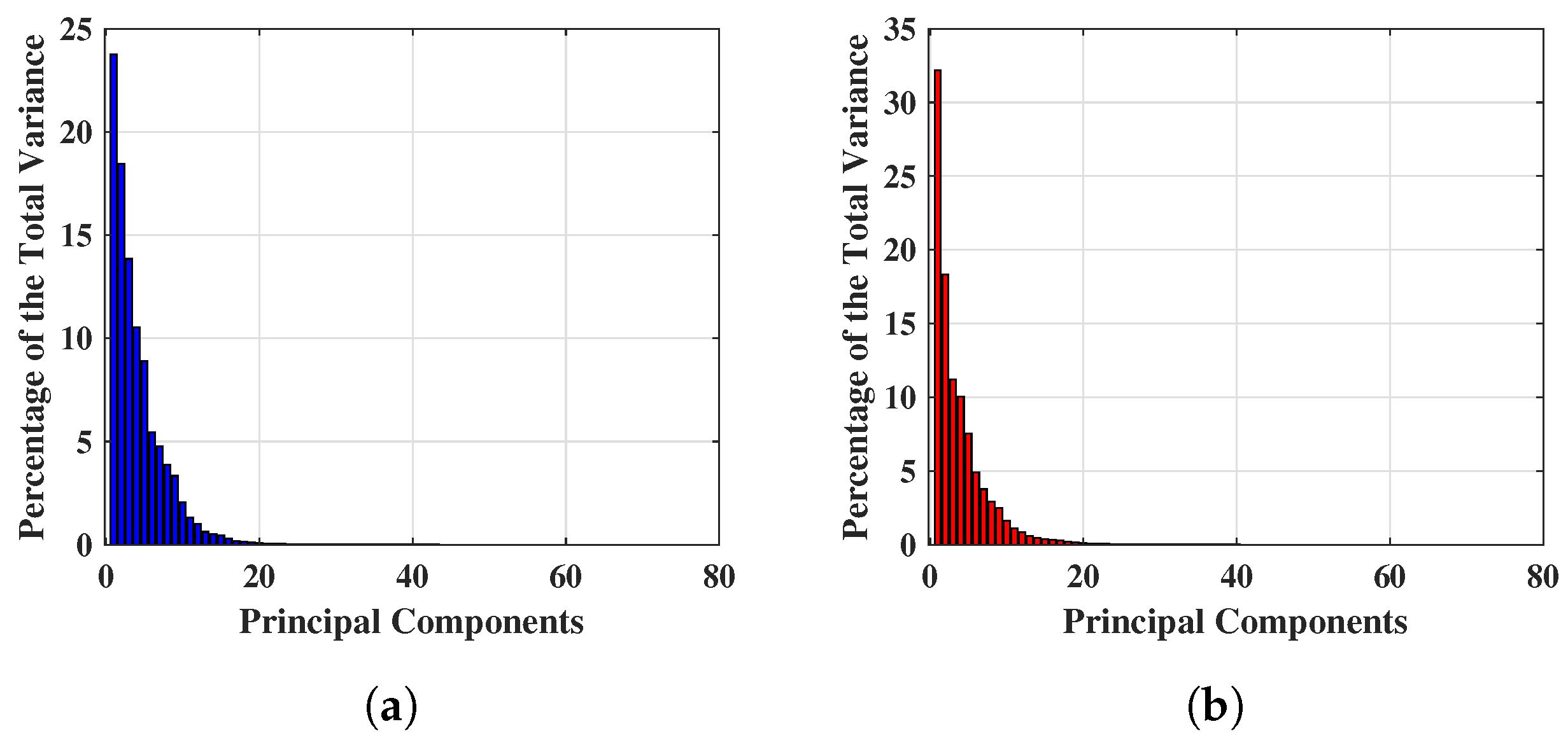
3.1. Principal Component Analysis
3.2. Basic Theory of the Proposed Algorithms
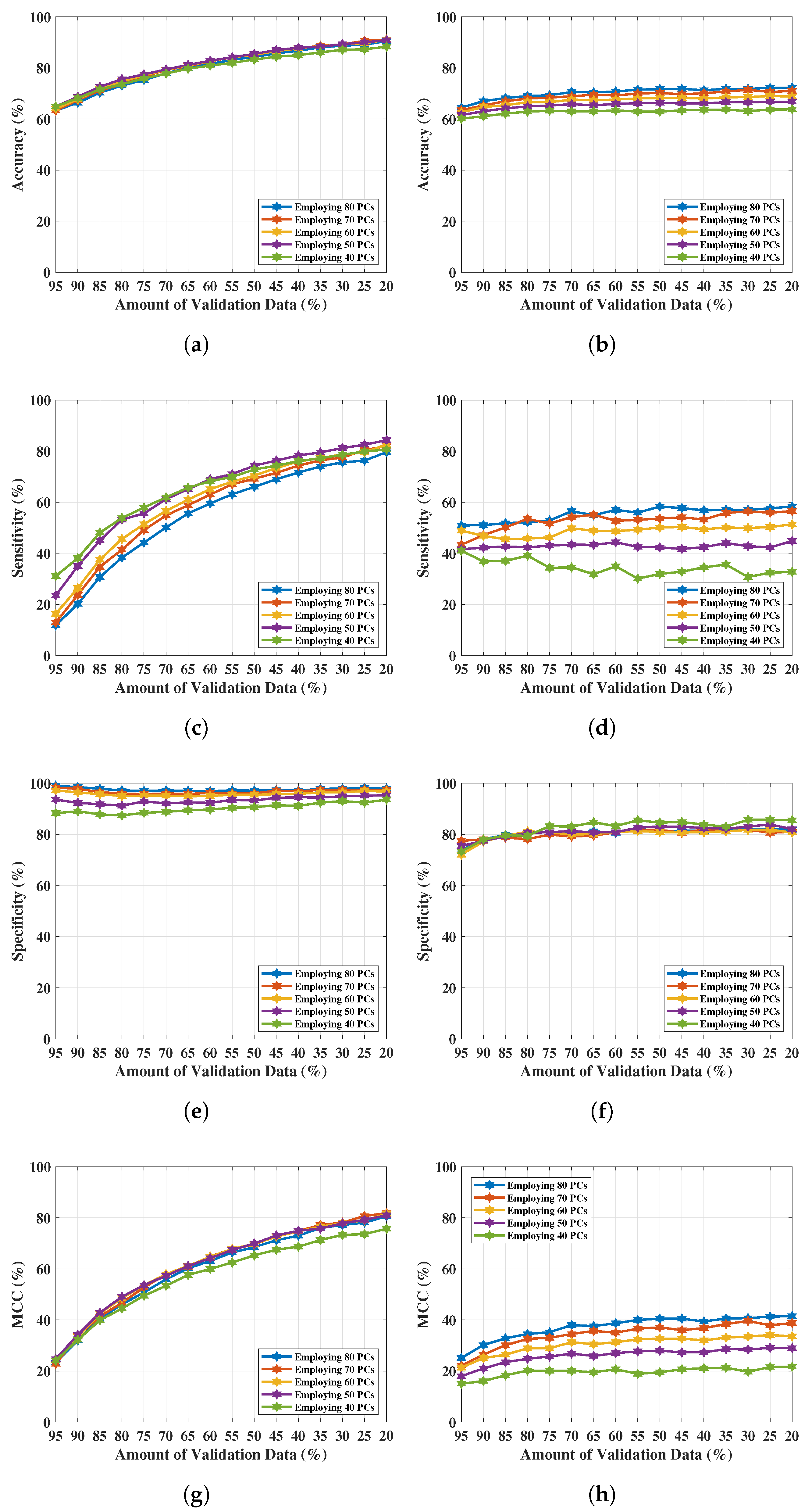
3.3. Performance Analysis
4. Results Analysis
4.1. Classification Applying PCs of Complex
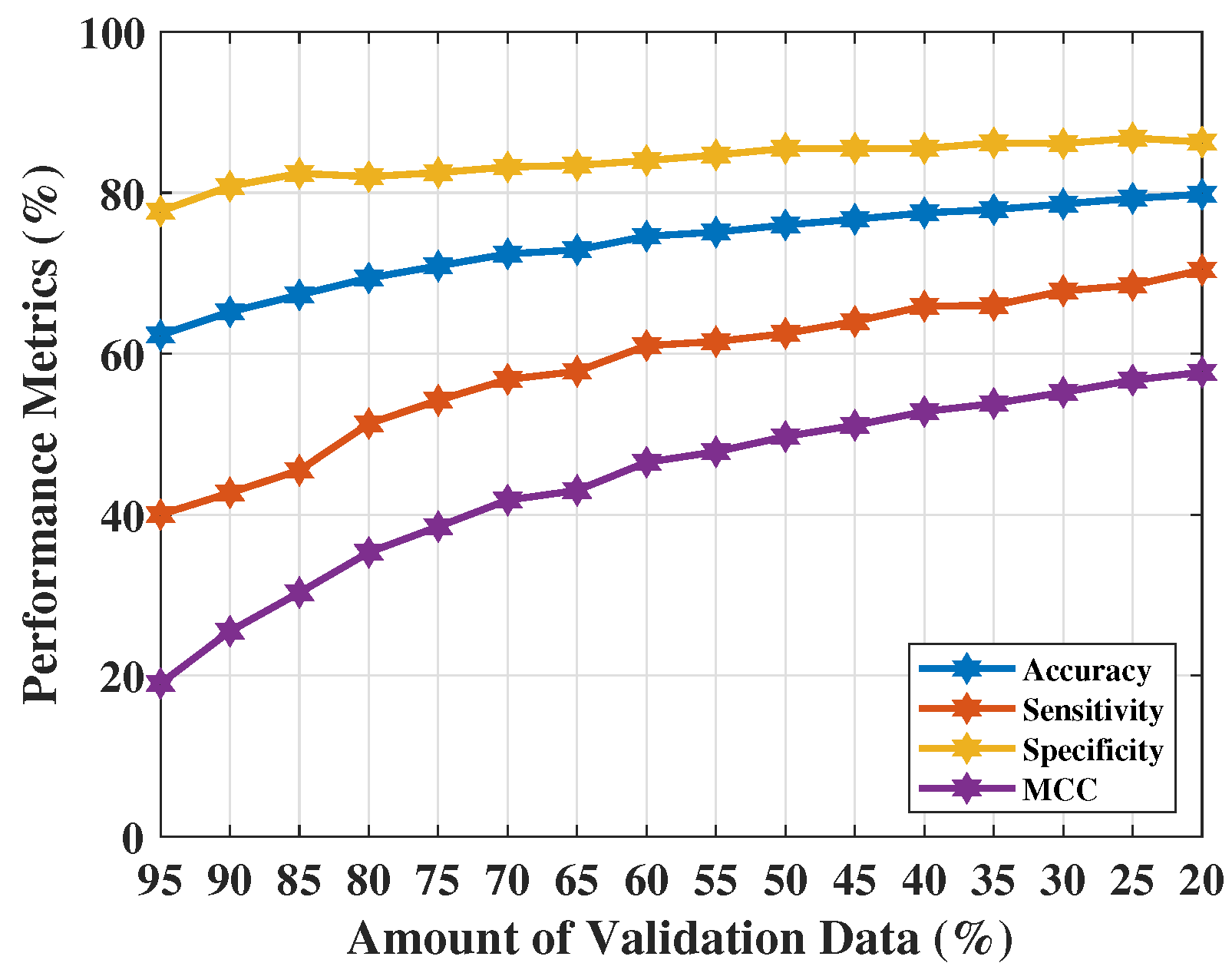
4.2. Classification Applying Real parts of Complex
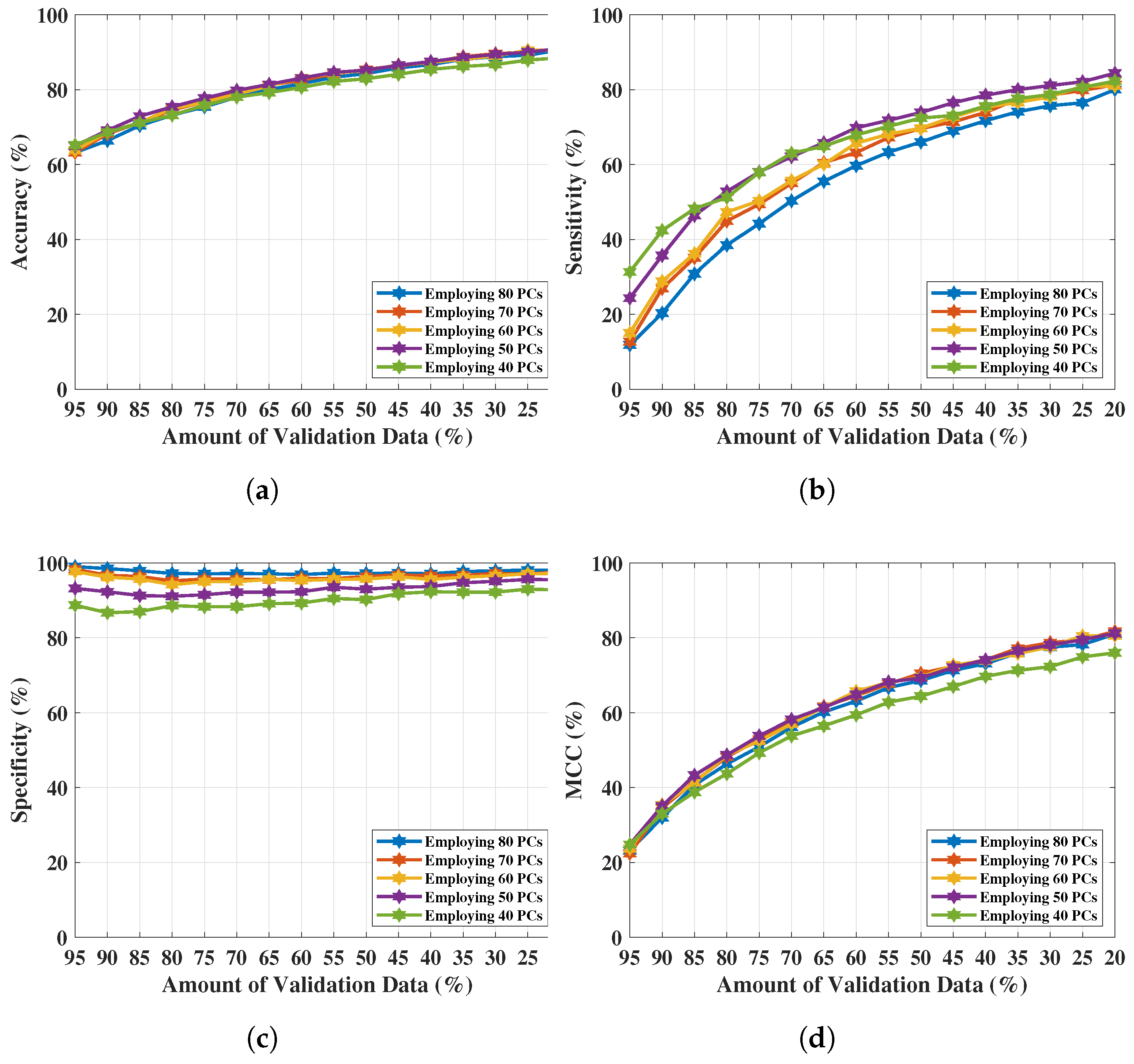
4.3. Classification Applying PCs of Real Parts of Complex
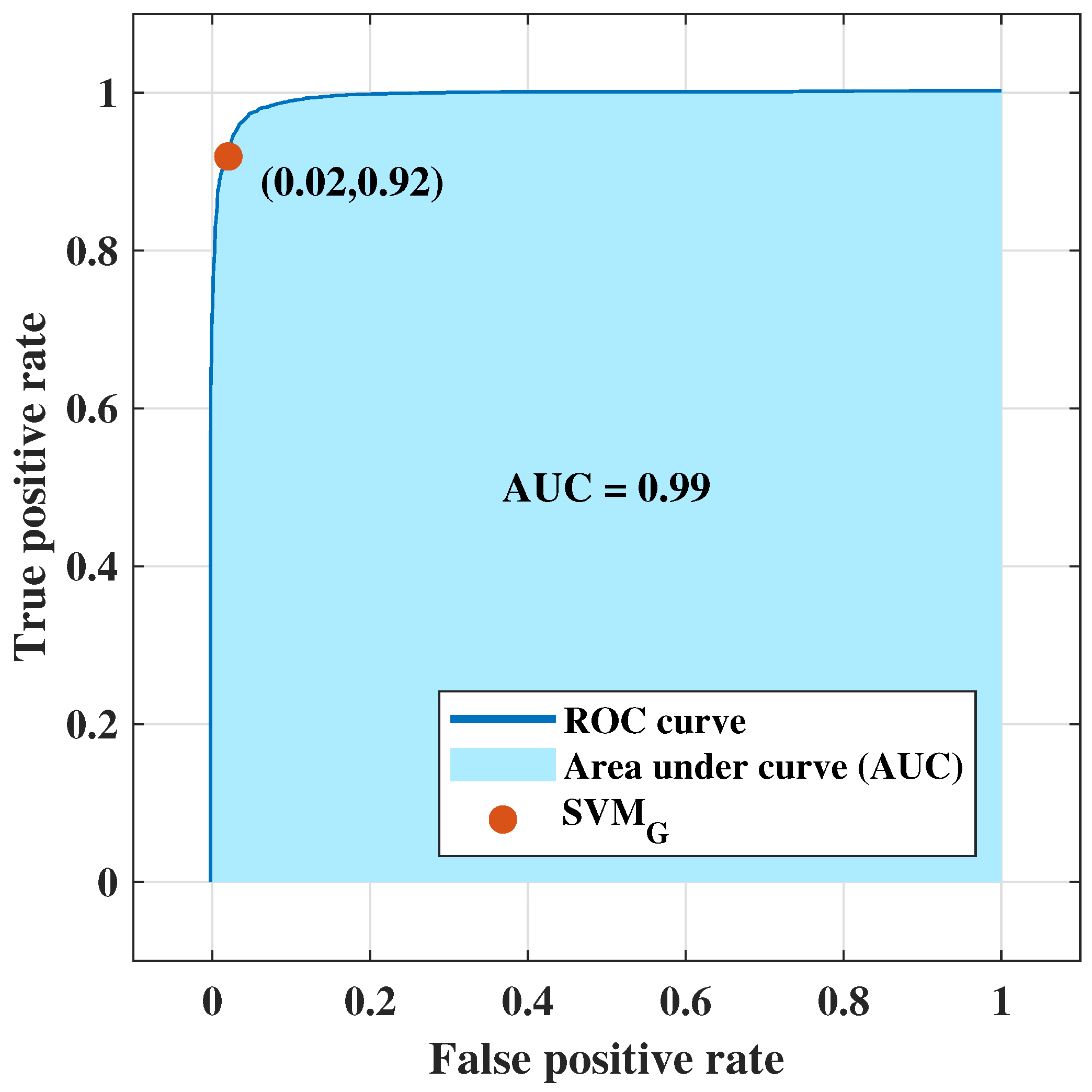
4.4. Classification Applying Optimal Settings: Training, Validation, Testing Experiment
5. Discussion & Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yedjou, C.G.; Sims, J.N.; Miele, L.; Noubissi, F.; Lowe, L.; Fonseca, D.D.; Alo, R.A.; Payton, M.; Tchounwou, P.B. Health and racial disparity in breast cancer. In Breast Cancer Metastasis Drug Resistance; Springer: Basel, Switzerland, 2019; pp. 31–49. [Google Scholar]
- Miglioretti, D.L.; Lange, J.; Van Den Broek, J.J.; Lee, C.I.; Van Ravesteyn, N.T.; Ritley, D.; Kerlikowske, K.; Fenton, J.J.; Melnikow, J.; De Koning, H.J.; et al. Radiation-induced breast cancer incidence and mortality from digital mammography screening: A modeling study. Ann. Intern. Med. 2016, 164, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Seiffert, K.; Thoene, K.; Zu Eulenburg, C.; Behrens, S.; Schmalfeldt, B.; Becher, H.; Chang-Claude, J.; Witzel, I. The effect of family history on screening procedures and prognosis in breast cancer patients-Results of a large population-based case-control study. Breast 2021, 55, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.M.; Champion, V.L. Attitudes about breast cancer and mammography: Racial, income, and educational differences. Women Health 1997, 26, 41–63. [Google Scholar] [CrossRef]
- Loving, V.A.; Aminololama-Shakeri, S.; Leung, J.W. Anxiety and its association with screening mammography. J. Breast Imaging 2021, 3, 266–272. [Google Scholar] [CrossRef]
- Tiberi, G.; Raspa, G. Apparatus for Testing the Integrity of Mammary Tissues. US Patent 10,349,863, 2019. [Google Scholar]
- Sensitivity, Specificity, and False Negative Rate for 1,682,504 Screening Mammography Examinations from 2007–2013. In Technical Report; Breast Cancer Surveillance Consortium (BCSC): Seattle, WA, USA, 2017.
- Stout, N.K.; Lee, S.J.; Schechter, C.B.; Kerlikowske, K.; Alagoz, O.; Berry, D.; Buist, D.S.; Cevik, M.; Chisholm, G.; De Koning, H.J.; et al. Benefits, harms, and costs for breast cancer screening after US implementation of digital mammography. JNCI: J. Natl. Cancer Inst. 2014, 106, dju092. [Google Scholar] [CrossRef] [PubMed]
- Nelson, H.D.; Pappas, M.; Cantor, A.; Griffin, J.; Daeges, M.; Humphrey, L. Harms of breast cancer screening: Systematic review to update the 2009 US Preventive Services Task Force recommendation. Ann. Intern. Med. 2016, 164, 256–267. [Google Scholar] [CrossRef]
- Fanizzi, A.; Basile, T.; Losurdo, L.; Amoroso, N.; Bellotti, R.; Bottigli, U.; Dentamaro, R.; Didonna, V.; Fausto, A.; Massafra, R.; et al. Hough transform for clustered microcalcifications detection in full-field digital mammograms. In Applications of Digital Image Processing XL; International Society for Optics and Photonics: San Diego, CA, USA, 2017; Volume 10396, p. 1039616. [Google Scholar]
- Bibault, J.E.; Giraud, P.; Burgun, A. Big data and machine learning in radiation oncology: State of the art and future prospects. Cancer Lett. 2016, 382, 110–117. [Google Scholar] [CrossRef]
- Zhang, B.; He, X.; Ouyang, F.; Gu, D.; Dong, Y.; Zhang, L.; Mo, X.; Huang, W.; Tian, J.; Zhang, S. Radiomic machine-learning classifiers for prognostic biomarkers of advanced nasopharyngeal carcinoma. Cancer Lett. 2017, 403, 21–27. [Google Scholar] [CrossRef]
- Huang, S.; Yang, J.; Fong, S.; Zhao, Q. Artificial intelligence in cancer diagnosis and prognosis: Opportunities and challenges. Cancer Lett. 2020, 471, 61–71. [Google Scholar] [CrossRef]
- McKinney, S.M.; Sieniek, M.; Godbole, V.; Godwin, J.; Antropova, N.; Ashrafian, H.; Back, T.; Chesus, M.; Corrado, G.S.; Darzi, A.; et al. International evaluation of an AI system for breast cancer screening. Nature 2020, 577, 89–94. [Google Scholar] [CrossRef]
- Hickman, S.E.; Baxter, G.C.; Gilbert, F.J. Adoption of artificial intelligence in breast imaging: Evaluation, ethical constraints and limitations. Br. J. Cancer 2021, 125, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Meaney, P.M.; Fanning, M.W.; Raynolds, T.; Fox, C.J.; Fang, Q.; Kogel, C.A.; Poplack, S.P.; Paulsen, K.D. Initial clinical experience with microwave breast imaging in women with normal mammography. Acad. Radiol. 2007, 14, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Bahramiabarghouei, H.; Porter, E.; Santorelli, A.; Gosselin, B.; Popović, M.; Rusch, L.A. Flexible 16 antenna array for microwave breast cancer detection. IEEE Trans. Biomed. Eng. 2015, 62, 2516–2525. [Google Scholar] [CrossRef]
- Bond, E.J.; Li, X.; Hagness, S.C.; Van Veen, B.D. Microwave imaging via space-time beamforming for early detection of breast cancer. IEEE Trans. Antennas Propag. 2003, 51, 1690–1705. [Google Scholar] [CrossRef]
- Fear, E.C.; Li, X.; Hagness, S.C.; Stuchly, M.A. Confocal microwave imaging for breast cancer detection: Localization of tumors in three dimensions. IEEE Trans. Biomed. Eng. 2002, 49, 812–822. [Google Scholar] [CrossRef]
- Meaney, P.M.; Fanning, M.W.; Li, D.; Poplack, S.P.; Paulsen, K.D. A clinical prototype for active microwave imaging of the breast. IEEE Trans. Microw. Theory Tech. 2000, 48, 1841–1853. [Google Scholar]
- O’Loughlin, D.; O’Halloran, M.; Moloney, B.M.; Glavin, M.; Jones, E.; Elahi, M.A. Microwave breast imaging: Clinical advances and remaining challenges. IEEE Trans. Biomed. Eng. 2018, 65, 2580–2590. [Google Scholar] [CrossRef]
- Sani, L.; Vispa, A.; Loretoni, R.; Duranti, M.; Ghavami, N.; Alvarez Sánchez-Bayuela, D.; Caschera, S.; Paoli, M.; Bigotti, A.; Badia, M.; et al. Breast lesion detection through MammoWave device: Empirical detection capability assessment of microwave images’ parameters. PLoS ONE 2021, 16, e0250005. [Google Scholar] [CrossRef]
- Meaney, P.M.; Kaufman, P.A.; Muffly, L.S.; Click, M.; Poplack, S.P.; Wells, W.A.; Schwartz, G.N.; di Florio-Alexander, R.M.; Tosteson, T.D.; Li, Z.; et al. Microwave imaging for neoadjuvant chemotherapy monitoring: Initial clinical experience. Breast Cancer Res. 2013, 15, 1–16. [Google Scholar] [CrossRef]
- Preece, A.W.; Craddock, I.; Shere, M.; Jones, L.; Winton, H.L. MARIA M4: Clinical evaluation of a prototype ultrawideband radar scanner for breast cancer detection. J. Med Imaging 2016, 3, 033502. [Google Scholar] [CrossRef]
- Massey, H.; Ridley, N.; Lyburn, I.; Taylor, S.; Schoenleber-Lewis, M.; Bannister, P.; Shere, M.H. Radio-wave detection of breast cancer in the symptomatic clinic—a multi-centre study. In Proceedings of the International Cambridge Conference on Breast Imaging, Cambridge, UK, 3–4 July 2017; pp. 3–4. [Google Scholar]
- Curtis, C.; Lavoie, B.R.; Fear, E. An analysis of the assumptions inherent to near-field beamforming for biomedical applications. IEEE Trans. Comput. Imaging 2017, 3, 953–965. [Google Scholar] [CrossRef]
- Yang, F.; Sun, L.; Hu, Z.; Wang, H.; Pan, D.; Wu, R.; Zhang, X.; Chen, Y.; Zhang, Q. A large-scale clinical trial of radar-based microwave breast imaging for Asian women: Phase I. In Proceedings of the 2017 IEEE International Symposium on Antennas and Propagation & USNC/URSI National Radio Science Meeting, San Diego, CA, USA, 9–14 July 2017; pp. 781–783. [Google Scholar]
- Kurrant, D.; Bourqui, J.; Fear, E. Surface estimation for microwave imaging. Sensors 2017, 17, 1658. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Sasada, S.; Kadoya, T.; Okada, M.; Arihiro, K.; Xiao, X.; Kikkawa, T. Detectability of breast tumor by a hand-held impulse-radar detector: Performance evaluation and pilot clinical study. Sci. Rep. 2017, 7, 1–11. [Google Scholar] [CrossRef]
- Porter, E.; Duff, K.; Popovic, M.; Coates, M. Investigation of time-domain microwave radar with breast clinic patients. In Proceedings of the 2016 10th European Conference on Antennas and Propagation (EuCAP), Davos, Switzerland, 10–15 April 2016; pp. 1–3. [Google Scholar]
- Kuwahara, Y.; Malik, A. Microwave imaging for early breast cancer detection. New Perspectives Breast Imaging; IntechOpen: London, UK, 2017; pp. 45–71. [Google Scholar]
- Ghavami, N.; Tiberi, G.; Edwards, D.J.; Monorchio, A. UWB microwave imaging of objects with canonical shape. IEEE Trans. Antennas Propag. 2011, 60, 231–239. [Google Scholar] [CrossRef]
- Tiberi, G.; Sani, L.; Ghavami, N.; Paoli, M.; Vispa, A.; Raspa, G.; Vannini, E.; Saracini, A.; Duranti, M. Sensitivity assessment of a microwave apparatus for breast cancer detection. In Proceedings of the European Congress of Radiology-ECR 2018, Vienna, Austria, 28 February–4 March 2018. [Google Scholar]
- Da Silva, D.; Kaduri, M.; Poley, M.; Adir, O.; Krinsky, N.; Shainsky-Roitman, J.; Schroeder, A. Biocompatibility, biodegradation and excretion of polylactic acid (PLA) in medical implants and theranostic systems. Chem. Eng. J. 2018, 340, 9–14. [Google Scholar] [CrossRef]
- Sani, L.; Ghavami, N.; Vispa, A.; Paoli, M.; Raspa, G.; Ghavami, M.; Sacchetti, F.; Vannini, E.; Ercolani, S.; Saracini, A.; et al. Novel microwave apparatus for breast lesions detection: Preliminary clinical results. Biomed. Signal Process. Control 2019, 52, 257–263. [Google Scholar] [CrossRef]
- Lazebnik, M.; Popovic, D.; McCartney, L.; Watkins, C.B.; Lindstrom, M.J.; Harter, J.; Sewall, S.; Ogilvie, T.; Magliocco, A.; Breslin, T.M.; et al. A large-scale study of the ultrawideband microwave dielectric properties of normal, benign and malignant breast tissues obtained from cancer surgeries. Phys. Med. Biol. 2007, 52, 6093. [Google Scholar] [CrossRef]
- Conceição, R.C.; Mohr, J.J.; O’Halloran, M. An Introduction to Microwave Imaging for Breast Cancer Detection; Springer: Basel, Switzerland, 2016. [Google Scholar]
- Noble, W.S. What is a support vector machine. Nat. Biotechnol. 2006, 24, 1565–1567. [Google Scholar] [CrossRef]
- Rana, S.P.; Dey, M.; Tiberi, G.; Sani, L.; Vispa, A.; Raspa, G.; Duranti, M.; Ghavami, M.; Dudley, S. Machine learning approaches for automated lesion detection in microwave breast imaging clinical data. Sci. Rep. 2019, 9, 1–12. [Google Scholar] [CrossRef]
- He, Q.; Kong, F.; Yan, R. Subspace-based gearbox condition monitoring by kernel principal component analysis. Mech. Syst. Signal Process. 2007, 21, 1755–1772. [Google Scholar] [CrossRef]
- Xu, Q.S.; Liang, Y.Z. Monte Carlo cross validation. Chemom. Intell. Lab. Syst. 2001, 56, 1–11. [Google Scholar] [CrossRef]
- Powers, D.M. Evaluation: From precision, recall and F-measure to ROC, informedness, markedness and correlation. arXiv 2020, arXiv:2010.16061. [Google Scholar]
- Matthews, B.W. Comparison of the predicted and observed secondary structure of T4 phage lysozyme. Biochim. Et Biophys. Acta (BBA)-Protein Struct. 1975, 405, 442–451. [Google Scholar] [CrossRef]
- Pisano, E.D.; Hendrick, R.E.; Yaffe, M.J.; Baum, J.K.; Acharyya, S.; Cormack, J.B.; Hanna, L.A.; Conant, E.F.; Fajardo, L.L.; Bassett, L.W.; et al. Diagnostic accuracy of digital versus film mammography: Exploratory analysis of selected population subgroups in DMIST. Radiology 2008, 246, 376–383. [Google Scholar] [CrossRef]
- Zeeshan, M.; Salam, B.; Khalid, Q.S.B.; Alam, S.; Sayani, R. Diagnostic accuracy of digital mammography in the detection of breast cancer. Cureus 2018, 10. [Google Scholar] [CrossRef]
- Massafra, R.; Bove, S.; Lorusso, V.; Biafora, A.; Comes, M.C.; Didonna, V.; Diotaiuti, S.; Fanizzi, A.; Nardone, A.; Nolasco, A.; et al. Radiomic Feature Reduction Approach to Predict Breast Cancer by Contrast-Enhanced Spectral Mammography Images. Diagnostics 2021, 11, 684. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT04253366 (accessed on 24 August 2021).
- Tiberi, G. Presenting MammoScreen project: Innovative and safe microwave-based imaging technology to make breast cancer screening more accurate, inclusive, and female-friendly, ECR 2023, RPS 702, Advanced applications in breast imaging. 2023; Vienna, Austria on 1–5 March 2023. (Just accepted). [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name of Parameters | Values |
|---|---|
| Total patients | 34 |
| Total subjects (breasts) | 61 |
| Number of patients age between 20–49 year | 23 |
| Number of patients age between 50–80 year | 38 |
| Mean of patient’s age (in year) | 52 |
| Standard deviation of patient’s age (in year) | 12 |
| Age | Breast (L/R) | ACR Breast Density | Mammography BI-RADS | Echography BI-RADS | Radiologist’s Output Details: Sizes (mm) & Notes (if Available) | Pathology or 1-Year Clinical Follow-up Output |
|---|---|---|---|---|---|---|
| 48 | L | D | 3 | - | Microcalcifications | Benign |
| 65 | L | C | 4 | - | Cluster of microcalcifications | Benign |
| 40 | L | B | 2 | 2 | Three masses: 15 mm, 21 mm, and 23 mm | Benign |
| R | B | 2 | 2 | Microcalcifications | Not available | |
| 52 | L | C | 5 | - | Microcalcifications | Malignant |
| 47 | L | D | 2 | 2 | Microcalcifications | Benign |
| 55 | R | C | 2 | 2 | 1.6 mm microcalcifications | Benign |
| L | C | 2 | 2 | 3.8 mm microcalcifications | Benign | |
| 51 | L | C | 2 | 2 | Presence of metallic marker | Benign |
| 54 | R | A | 2 | 2 | Microcalcifications | Benign |
| 77 | R | D | - | 5 | 17 mm mass | Malignant |
| 61 | R | C | 4 | - | Multifocal lobular type suspected carcinoma (MRI BI-RADS 4) | Malignant |
| L | C | 2 | - | Macrocalcification and Focal contrast enh. (MRI BI-RADS 3) | Not available | |
| 50 | L | B | 2 | 2 | 10 mm mass | Benign |
| 67 | L | C | 4 | - | Microcalcifications | Malignant |
| 49 | L | A | 3 | - | Microcalcifications | Benign |
| 70 | L | D | 3 | 4 | Mass | Malignant |
| 42 | L | C | 2 | 3 | 7 mm mass, hypoechoic | Benign |
| 67 | L | B | 3 | - | Architectural distortion | Benign |
| 56 | R | B | 4 | 4 | 31 mm mass, hypoechoic, irregular borders | Malignant |
| 43 | R | D | 1 | 3 | 12 mm mass | Benign |
| 51 | L | C | 3 | - | Microcalcifications | Benign |
| 59 | L | B | - | 4 | 11 mm areolar, suspicious of malignancy | Malignant |
| 40 | L | D | 2 | 2 | 30 mm mass | Benign |
| 35 | R | C | 2 | 3 | 7 mm, hypoechoic | Benign |
| 37 | L | A | 2 | 3 | 25 mm mass | Benign |
| 43 | R | B | 3 | 2 | Microcalcifications | Malignant |
| 54 | R | B | 2 | 2 | 18 mm mass | Benign |
| 49 | L | A | 2 | 3 | 16 mm mass | Benign |
| 56 | L | D | 4 | 4 | 27 mm mass | Malignant |
| 63 | L | A | 3 | 4 | 6 mm mass | Malignant |
| 55 | R | C | 4 | 4 | 23 mm mass | Malignant |
| L | C | 2 | 2 | Multiple cysts | Benign | |
| 64 | R | B | 3 | - | 1.6 mm microcalcifications | Benign |
| 37 | R | - | - | 3 | 15.4 mm mass | Benign |
| L | - | - | 2 | Multiple cysts | Not available |
| Breast Type | Mean | Maximum | Minimum | Median | Standard Deviation | Variance |
|---|---|---|---|---|---|---|
| No-Finding (NF) | 2.179 × 10 | 0.114 | −0.105 | −8.286 × 10 | 0.011 | 4.578 × 10 |
| With-Finding (WF) | 1.985 × 10 | 0.118 | −0.108 | −1.640 × 10 | 0.011 | 4.651 × 10 |
| Null Hypothesis () | Probabilty (p) | Confidence Interval () | Confidence Interval () |
|---|---|---|---|
| 1 |
| Feature Dimension → | PC-80 | PC-70 | PC-60 | PC-50 | PC-40 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Validation Data↓ | ||||||||||||||||||||
| 95% | 0.644 | 0.509 | 0.737 | 0.251 | 0.635 | 0.434 | 0.774 | 0.221 | 0.626 | 0.489 | 0.720 | 0.213 | 0.616 | 0.416 | 0.754 | 0.180 | 0.601 | 0.410 | 0.733 | 0.150 |
| 90% | 0.670 | 0.510 | 0.781 | 0.302 | 0.653 | 0.471 | 0.781 | 0.264 | 0.647 | 0.468 | 0.772 | 0.251 | 0.630 | 0.422 | 0.775 | 0.210 | 0.611 | 0.368 | 0.779 | 0.161 |
| 85% | 0.682 | 0.518 | 0.797 | 0.328 | 0.670 | 0.501 | 0.787 | 0.301 | 0.654 | 0.455 | 0.793 | 0.264 | 0.642 | 0.427 | 0.791 | 0.235 | 0.621 | 0.370 | 0.796 | 0.183 |
| 80% | 0.690 | 0.522 | 0.807 | 0.345 | 0.680 | 0.535 | 0.781 | 0.326 | 0.666 | 0.458 | 0.811 | 0.289 | 0.649 | 0.423 | 0.806 | 0.248 | 0.629 | 0.391 | 0.794 | 0.202 |
| 75% | 0.693 | 0.528 | 0.808 | 0.352 | 0.684 | 0.516 | 0.799 | 0.330 | 0.666 | 0.462 | 0.808 | 0.289 | 0.653 | 0.430 | 0.808 | 0.257 | 0.632 | 0.343 | 0.832 | 0.201 |
| 70% | 0.706 | 0.565 | 0.804 | 0.380 | 0.689 | 0.542 | 0.791 | 0.345 | 0.676 | 0.498 | 0.799 | 0.313 | 0.658 | 0.434 | 0.813 | 0.268 | 0.630 | 0.345 | 0.830 | 0.201 |
| 65% | 0.704 | 0.549 | 0.812 | 0.376 | 0.695 | 0.551 | 0.795 | 0.357 | 0.673 | 0.488 | 0.801 | 0.305 | 0.654 | 0.433 | 0.807 | 0.259 | 0.630 | 0.318 | 0.847 | 0.195 |
| 60% | 0.708 | 0.570 | 0.805 | 0.387 | 0.692 | 0.527 | 0.808 | 0.350 | 0.676 | 0.487 | 0.808 | 0.313 | 0.659 | 0.443 | 0.808 | 0.270 | 0.634 | 0.349 | 0.832 | 0.207 |
| 55% | 0.715 | 0.559 | 0.824 | 0.400 | 0.700 | 0.531 | 0.818 | 0.366 | 0.681 | 0.492 | 0.813 | 0.324 | 0.662 | 0.425 | 0.826 | 0.277 | 0.629 | 0.301 | 0.855 | 0.189 |
| 50% | 0.717 | 0.583 | 0.809 | 0.405 | 0.702 | 0.536 | 0.818 | 0.371 | 0.682 | 0.501 | 0.809 | 0.327 | 0.663 | 0.423 | 0.831 | 0.280 | 0.629 | 0.319 | 0.846 | 0.195 |
| 45% | 0.718 | 0.577 | 0.815 | 0.405 | 0.697 | 0.541 | 0.805 | 0.360 | 0.683 | 0.503 | 0.807 | 0.327 | 0.661 | 0.417 | 0.829 | 0.273 | 0.634 | 0.328 | 0.848 | 0.207 |
| 40% | 0.713 | 0.568 | 0.813 | 0.394 | 0.701 | 0.532 | 0.819 | 0.368 | 0.680 | 0.494 | 0.808 | 0.320 | 0.661 | 0.424 | 0.825 | 0.273 | 0.636 | 0.345 | 0.838 | 0.211 |
| 35% | 0.718 | 0.571 | 0.820 | 0.406 | 0.708 | 0.558 | 0.811 | 0.384 | 0.685 | 0.501 | 0.812 | 0.331 | 0.666 | 0.440 | 0.822 | 0.286 | 0.637 | 0.356 | 0.830 | 0.213 |
| 30% | 0.718 | 0.570 | 0.822 | 0.407 | 0.714 | 0.564 | 0.818 | 0.396 | 0.686 | 0.499 | 0.817 | 0.335 | 0.665 | 0.428 | 0.830 | 0.284 | 0.631 | 0.307 | 0.857 | 0.197 |
| 25% | 0.722 | 0.576 | 0.822 | 0.413 | 0.706 | 0.559 | 0.806 | 0.379 | 0.690 | 0.503 | 0.818 | 0.341 | 0.668 | 0.423 | 0.839 | 0.291 | 0.637 | 0.324 | 0.857 | 0.216 |
| 20% | 0.723 | 0.583 | 0.818 | 0.415 | 0.710 | 0.565 | 0.810 | 0.388 | 0.688 | 0.513 | 0.807 | 0.336 | 0.668 | 0.448 | 0.820 | 0.290 | 0.638 | 0.327 | 0.855 | 0.217 |
| 95% | 0.633 | 0.118 | 0.990 | 0.233 | 0.633 | 0.129 | 0.983 | 0.228 | 0.641 | 0.163 | 0.972 | 0.242 | 0.649 | 0.235 | 0.936 | 0.247 | 0.649 | 0.311 | 0.883 | 0.241 |
| 90% | 0.664 | 0.202 | 0.985 | 0.320 | 0.674 | 0.237 | 0.978 | 0.338 | 0.677 | 0.264 | 0.964 | 0.334 | 0.687 | 0.350 | 0.923 | 0.342 | 0.682 | 0.381 | 0.890 | 0.322 |
| 85% | 0.703 | 0.307 | 0.978 | 0.405 | 0.711 | 0.347 | 0.965 | 0.414 | 0.719 | 0.375 | 0.957 | 0.426 | 0.726 | 0.450 | 0.918 | 0.428 | 0.716 | 0.481 | 0.878 | 0.399 |
| 80% | 0.731 | 0.383 | 0.972 | 0.461 | 0.736 | 0.414 | 0.960 | 0.467 | 0.748 | 0.456 | 0.950 | 0.485 | 0.756 | 0.532 | 0.912 | 0.491 | 0.736 | 0.538 | 0.874 | 0.445 |
| 75% | 0.753 | 0.442 | 0.970 | 0.508 | 0.766 | 0.491 | 0.957 | 0.527 | 0.771 | 0.514 | 0.951 | 0.536 | 0.775 | 0.556 | 0.929 | 0.536 | 0.759 | 0.579 | 0.884 | 0.495 |
| 70% | 0.779 | 0.501 | 0.972 | 0.559 | 0.792 | 0.548 | 0.960 | 0.579 | 0.793 | 0.566 | 0.951 | 0.579 | 0.794 | 0.612 | 0.921 | 0.573 | 0.778 | 0.619 | 0.888 | 0.534 |
| 65% | 0.800 | 0.556 | 0.970 | 0.602 | 0.807 | 0.588 | 0.958 | 0.608 | 0.810 | 0.610 | 0.949 | 0.612 | 0.812 | 0.651 | 0.925 | 0.611 | 0.797 | 0.657 | 0.894 | 0.576 |
| 60% | 0.815 | 0.595 | 0.969 | 0.631 | 0.826 | 0.630 | 0.962 | 0.648 | 0.827 | 0.651 | 0.950 | 0.647 | 0.828 | 0.690 | 0.923 | 0.642 | 0.809 | 0.682 | 0.897 | 0.600 |
| 55% | 0.832 | 0.631 | 0.972 | 0.664 | 0.842 | 0.670 | 0.960 | 0.678 | 0.842 | 0.680 | 0.955 | 0.678 | 0.842 | 0.710 | 0.935 | 0.674 | 0.820 | 0.699 | 0.904 | 0.625 |
| 50% | 0.843 | 0.660 | 0.971 | 0.685 | 0.851 | 0.692 | 0.960 | 0.695 | 0.852 | 0.704 | 0.955 | 0.698 | 0.855 | 0.743 | 0.932 | 0.699 | 0.833 | 0.728 | 0.906 | 0.653 |
| 45% | 0.857 | 0.690 | 0.973 | 0.712 | 0.866 | 0.715 | 0.971 | 0.729 | 0.866 | 0.734 | 0.957 | 0.726 | 0.870 | 0.763 | 0.943 | 0.731 | 0.844 | 0.743 | 0.914 | 0.675 |
| 40% | 0.867 | 0.716 | 0.971 | 0.730 | 0.876 | 0.743 | 0.968 | 0.748 | 0.877 | 0.759 | 0.958 | 0.747 | 0.879 | 0.783 | 0.945 | 0.749 | 0.850 | 0.761 | 0.911 | 0.687 |
| 35% | 0.881 | 0.740 | 0.978 | 0.760 | 0.887 | 0.764 | 0.974 | 0.772 | 0.885 | 0.773 | 0.964 | 0.765 | 0.883 | 0.795 | 0.944 | 0.758 | 0.861 | 0.772 | 0.924 | 0.713 |
| 30% | 0.887 | 0.756 | 0.979 | 0.772 | 0.892 | 0.775 | 0.974 | 0.781 | 0.892 | 0.787 | 0.965 | 0.779 | 0.893 | 0.812 | 0.949 | 0.778 | 0.871 | 0.786 | 0.930 | 0.733 |
| 25% | 0.891 | 0.763 | 0.981 | 0.781 | 0.906 | 0.804 | 0.975 | 0.807 | 0.897 | 0.795 | 0.969 | 0.790 | 0.900 | 0.825 | 0.951 | 0.792 | 0.873 | 0.799 | 0.924 | 0.736 |
| 20% | 0.905 | 0.796 | 0.979 | 0.806 | 0.911 | 0.820 | 0.974 | 0.818 | 0.910 | 0.826 | 0.968 | 0.815 | 0.909 | 0.843 | 0.953 | 0.810 | 0.883 | 0.806 | 0.936 | 0.757 |
| Null Hypothesis () | Probabilty(p) | Confidence Interval () | Confidence Interval () |
|---|---|---|---|
| 1 |
| Validation Data | ||||
|---|---|---|---|---|
| 95% | 0.623 | 0.400 | 0.777 | 0.190 |
| 90% | 0.652 | 0.427 | 0.808 | 0.255 |
| 85% | 0.673 | 0.455 | 0.824 | 0.303 |
| 80% | 0.694 | 0.513 | 0.820 | 0.353 |
| 75% | 0.709 | 0.542 | 0.825 | 0.385 |
| 70% | 0.724 | 0.568 | 0.832 | 0.418 |
| 65% | 0.729 | 0.578 | 0.834 | 0.430 |
| 60% | 0.746 | 0.610 | 0.840 | 0.465 |
| 55% | 0.751 | 0.615 | 0.847 | 0.478 |
| 50% | 0.760 | 0.625 | 0.855 | 0.497 |
| 45% | 0.767 | 0.640 | 0.855 | 0.511 |
| 40% | 0.775 | 0.659 | 0.855 | 0.528 |
| 35% | 0.779 | 0.660 | 0.862 | 0.538 |
| 30% | 0.786 | 0.678 | 0.861 | 0.552 |
| 25% | 0.793 | 0.685 | 0.868 | 0.567 |
| 20% | 0.798 | 0.704 | 0.863 | 0.577 |
| Null Hypothesis () | Probabilty (p) | Confidence Interval () | Confidence Interval () |
|---|---|---|---|
| 1 |
| Feature Dimension → | PC-80 | PC-70 | PC-60 | PC-50 | PC-40 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Validation Data↓ | ||||||||||||||||||||
| 95% | 0.632 | 0.118 | 0.990 | 0.232 | 0.632 | 0.127 | 0.983 | 0.224 | 0.638 | 0.150 | 0.977 | 0.237 | 0.650 | 0.243 | 0.932 | 0.248 | 0.652 | 0.313 | 0.887 | 0.248 |
| 90% | 0.664 | 0.203 | 0.985 | 0.320 | 0.682 | 0.269 | 0.967 | 0.346 | 0.686 | 0.288 | 0.962 | 0.354 | 0.691 | 0.357 | 0.923 | 0.351 | 0.686 | 0.424 | 0.867 | 0.330 |
| 85% | 0.704 | 0.308 | 0.979 | 0.407 | 0.712 | 0.351 | 0.964 | 0.416 | 0.712 | 0.362 | 0.957 | 0.413 | 0.729 | 0.464 | 0.913 | 0.433 | 0.711 | 0.482 | 0.870 | 0.388 |
| 80% | 0.732 | 0.385 | 0.972 | 0.463 | 0.746 | 0.449 | 0.952 | 0.482 | 0.750 | 0.473 | 0.942 | 0.487 | 0.754 | 0.528 | 0.911 | 0.487 | 0.732 | 0.512 | 0.886 | 0.437 |
| 75% | 0.754 | 0.442 | 0.971 | 0.509 | 0.767 | 0.494 | 0.957 | 0.529 | 0.766 | 0.503 | 0.950 | 0.524 | 0.777 | 0.580 | 0.915 | 0.538 | 0.758 | 0.579 | 0.883 | 0.493 |
| 70% | 0.780 | 0.503 | 0.972 | 0.561 | 0.790 | 0.550 | 0.957 | 0.575 | 0.788 | 0.557 | 0.950 | 0.570 | 0.798 | 0.621 | 0.922 | 0.582 | 0.780 | 0.630 | 0.883 | 0.538 |
| 65% | 0.800 | 0.555 | 0.971 | 0.602 | 0.812 | 0.605 | 0.955 | 0.617 | 0.810 | 0.601 | 0.956 | 0.615 | 0.814 | 0.658 | 0.922 | 0.614 | 0.792 | 0.649 | 0.891 | 0.565 |
| 60% | 0.816 | 0.597 | 0.969 | 0.631 | 0.825 | 0.632 | 0.959 | 0.645 | 0.832 | 0.657 | 0.953 | 0.657 | 0.831 | 0.698 | 0.923 | 0.649 | 0.806 | 0.679 | 0.893 | 0.594 |
| 55% | 0.833 | 0.633 | 0.973 | 0.667 | 0.842 | 0.672 | 0.958 | 0.677 | 0.844 | 0.681 | 0.956 | 0.681 | 0.846 | 0.718 | 0.935 | 0.682 | 0.822 | 0.702 | 0.905 | 0.628 |
| 50% | 0.843 | 0.660 | 0.972 | 0.686 | 0.854 | 0.696 | 0.964 | 0.705 | 0.851 | 0.697 | 0.957 | 0.695 | 0.852 | 0.739 | 0.930 | 0.693 | 0.829 | 0.724 | 0.902 | 0.644 |
| 45% | 0.858 | 0.690 | 0.973 | 0.713 | 0.864 | 0.714 | 0.968 | 0.724 | 0.866 | 0.727 | 0.963 | 0.727 | 0.865 | 0.765 | 0.935 | 0.721 | 0.841 | 0.731 | 0.918 | 0.670 |
| 40% | 0.867 | 0.717 | 0.971 | 0.731 | 0.873 | 0.739 | 0.966 | 0.741 | 0.873 | 0.753 | 0.956 | 0.739 | 0.875 | 0.785 | 0.937 | 0.741 | 0.854 | 0.756 | 0.923 | 0.697 |
| 35% | 0.881 | 0.741 | 0.977 | 0.760 | 0.888 | 0.775 | 0.967 | 0.772 | 0.881 | 0.766 | 0.962 | 0.758 | 0.886 | 0.800 | 0.947 | 0.765 | 0.862 | 0.776 | 0.922 | 0.713 |
| 30% | 0.888 | 0.757 | 0.979 | 0.775 | 0.896 | 0.785 | 0.972 | 0.787 | 0.890 | 0.781 | 0.966 | 0.776 | 0.894 | 0.811 | 0.951 | 0.781 | 0.867 | 0.787 | 0.922 | 0.723 |
| 25% | 0.892 | 0.765 | 0.981 | 0.782 | 0.900 | 0.798 | 0.970 | 0.795 | 0.905 | 0.809 | 0.971 | 0.805 | 0.900 | 0.821 | 0.956 | 0.795 | 0.879 | 0.806 | 0.930 | 0.749 |
| 20% | 0.906 | 0.800 | 0.980 | 0.810 | 0.910 | 0.813 | 0.977 | 0.817 | 0.905 | 0.810 | 0.972 | 0.806 | 0.910 | 0.844 | 0.955 | 0.812 | 0.885 | 0.823 | 0.928 | 0.760 |
| Total Breasts | Training-Validation Data | Training Data | Validation Data | Feature Dimension PC-50 | Testing Data | Feature Dimension PC-50 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 61 Breasts | 75% of Data (46 Breasts) | 80% | 20% | 84.20% | 88.20% | 82.20% | 67.40% | 25% of Data (15 breasts) | 94.40% | 96.20% | 93.40% | 88.50% |
| 61 Breasts | 80% of Data (49 Breasts) | 80% | 20% | 85.40% | 88.80% | 83.60% | 69.70% | 20% of Data (12 breasts) | 95.50% | 97.20% | 94.50% | 90.90% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rana, S.P.; Dey, M.; Loretoni, R.; Duranti, M.; Ghavami, M.; Dudley, S.; Tiberi, G. Radiation-Free Microwave Technology for Breast Lesion Detection Using Supervised Machine Learning Model. Tomography 2023, 9, 105-129. https://doi.org/10.3390/tomography9010010
Rana SP, Dey M, Loretoni R, Duranti M, Ghavami M, Dudley S, Tiberi G. Radiation-Free Microwave Technology for Breast Lesion Detection Using Supervised Machine Learning Model. Tomography. 2023; 9(1):105-129. https://doi.org/10.3390/tomography9010010
Chicago/Turabian StyleRana, Soumya Prakash, Maitreyee Dey, Riccardo Loretoni, Michele Duranti, Mohammad Ghavami, Sandra Dudley, and Gianluigi Tiberi. 2023. "Radiation-Free Microwave Technology for Breast Lesion Detection Using Supervised Machine Learning Model" Tomography 9, no. 1: 105-129. https://doi.org/10.3390/tomography9010010
APA StyleRana, S. P., Dey, M., Loretoni, R., Duranti, M., Ghavami, M., Dudley, S., & Tiberi, G. (2023). Radiation-Free Microwave Technology for Breast Lesion Detection Using Supervised Machine Learning Model. Tomography, 9(1), 105-129. https://doi.org/10.3390/tomography9010010