
Clinical Low Dose Photon Counting CT for the Detection of Urolithiasis: Evaluation of Image Quality and Radiation Dose

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. CT Protocols and Image Acquisition
2.3. Radiation Dose
2.4. Quantitative Image Analysis
2.5. Qualitative Image Analysis
2.6. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Radiation Dose
3.3. Quantitative Image Analysis
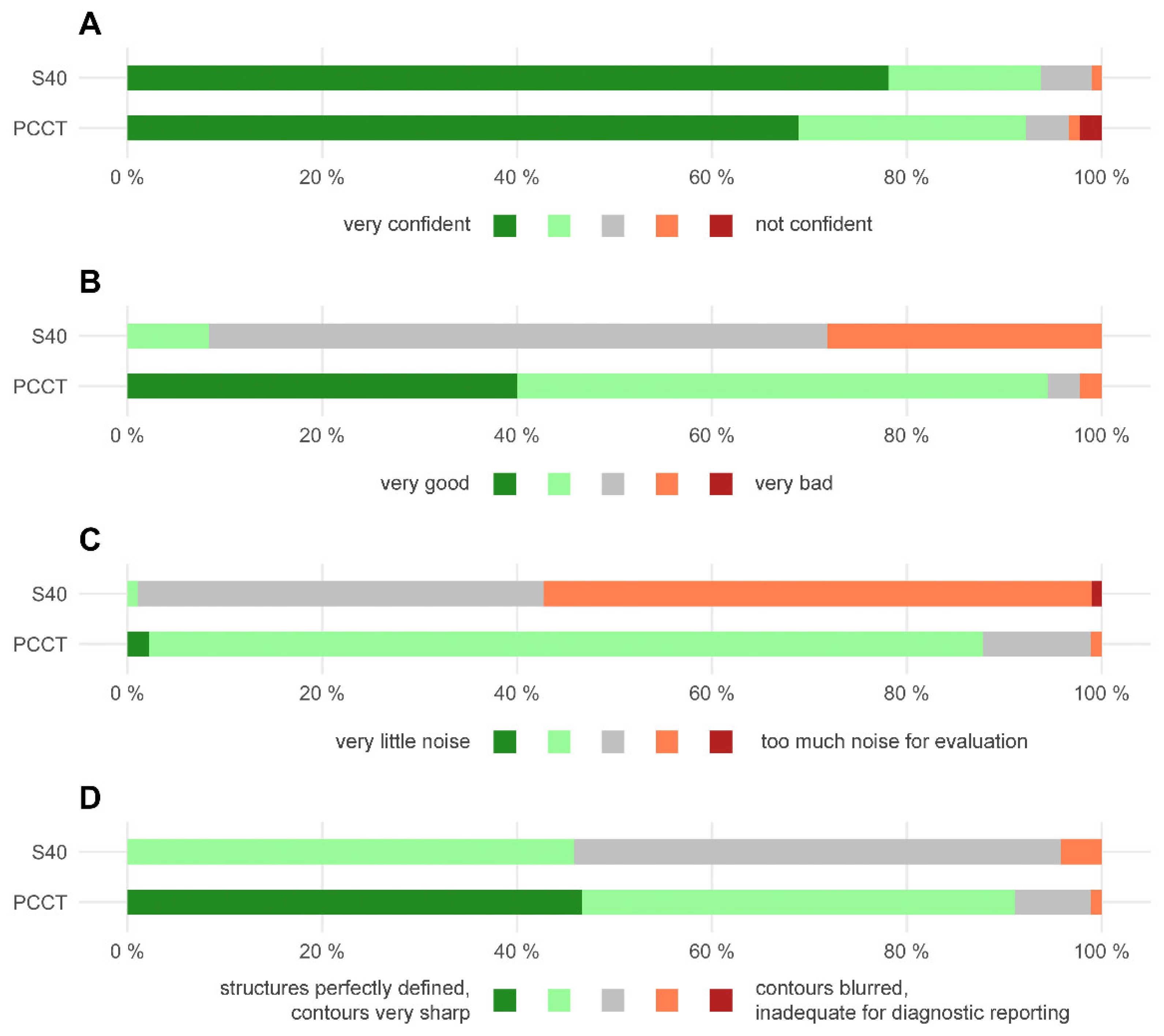
3.4. Qualitative Image Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ziemba, J.B.; Matlaga, B.R. Epidemiology and economics of nephrolithiasis. Investig. Clin. Urol. 2017, 58, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Scales, C.D., Jr.; Smith, A.C.; Hanley, J.M.; Saigal, C.S. Prevalence of kidney stones in the United States. Eur. Urol. 2012, 62, 160–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tundo, G.; Vollstedt, A.; Meeks, W.; Pais, V. Beyond Prevalence: Annual Cumulative Incidence of Kidney Stones in the United States. J. Urol. 2021, 205, 1707–1709. [Google Scholar] [CrossRef] [PubMed]
- Uribarri, J.; Oh, M.S.; Carroll, H.J. The first kidney stone. Ann. Intern. Med. 1989, 111, 1006–1009. [Google Scholar] [CrossRef]
- Brisbane, W.; Bailey, M.R.; Sorensen, M.D. An overview of kidney stone imaging techniques. Nat. Rev. Urol. 2016, 13, 654–662. [Google Scholar] [CrossRef] [Green Version]
- Fulgham, P.F.; Assimos, D.G.; Pearle, M.S.; Preminger, G.M. Clinical effectiveness protocols for imaging in the management of ureteral calculous disease: AUA technology assessment. J. Urol. 2013, 189, 1203–1213. [Google Scholar] [CrossRef]
- Poletti, P.-A.; Platon, A.; Rutschmann, O.T.; Schmidlin, F.R.; Iselin, C.E.; Becker, C.D. Low-Dose Versus Standard-Dose CT Protocol in Patients with Clinically Suspected Renal Colic. Am. J. Roentgenol. 2007, 188, 927–933. [Google Scholar] [CrossRef]
- Diel, J.; Perlmutter, S.; Venkataramanan, N.; Mueller, R.; Lane, M.J.; Katz, D.S. Unenhanced helical CT using increased pitch for suspected renal colic: An effective technique for radiation dose reduction? J. Comput. Assist. Tomogr. 2000, 24, 795–801. [Google Scholar] [CrossRef]
- Mozaffary, A.; Trabzonlu, T.A.; Kim, D.; Yaghmai, V. Comparison of Tin Filter–Based Spectral Shaping CT and Low-Dose Protocol for Detection of Urinary Calculi. Am. J. Roentgenol. 2019, 212, 808–814. [Google Scholar] [CrossRef]
- Hokamp, N.G.; Salem, J.; Hesse, A.; Holz, J.A.; Ritter, M.; Heidenreich, A.; Maintz, D.; Haneder, S. Low-Dose Characterization of Kidney Stones Using Spectral Detector Computed Tomography: An Ex Vivo Study. Investig. Radiol. 2018, 53, 457–462. [Google Scholar] [CrossRef]
- Hansmann, J.; Schoenberg, G.M.; Brix, G.; Henzler, T.; Meyer, M.; Attenberger, U.I.; Schoenberg, S.O.; Fink, C. CT of Urolithiasis: Comparison of Image Quality and Diagnostic Confidence Using Filtered Back Projection and Iterative Reconstruction Techniques. Acad. Radiol. 2013, 20, 1162–1167. [Google Scholar] [CrossRef] [PubMed]
- Reimer, R.P.; Klein, K.; Rinneburger, M.; Zopfs, D.; Lennartz, S.; Salem, J.; Heidenreich, A.; Maintz, D.; Haneder, S.; Hokamp, N.G. Manual kidney stone size measurements in computed tomography are most accurate using multiplanar image reformatations and bone window settings. Sci. Rep. 2021, 11, 16437. [Google Scholar] [CrossRef] [PubMed]
- Reimer, R.P.; Salem, J.; Merkt, M.; Sonnabend, K.; Lennartz, S.; Zopfs, D.; Heidenreich, A.; Maintz, D.; Haneder, S.; Hokamp, N.G. Size and volume of kidney stones in computed tomography: Influence of acquisition techniques and image reconstruction parameters. Eur. J. Radiol. 2020, 132, 109267. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.-H.; Slebocki, K.; Khristenko, E.; Herden, J.; Salem, J.; Hokamp, N.G.; Mammadov, K.; Hellmich, M.; Kabbasch, C. Low-dose computed tomography of urolithiasis in obese patients: A feasibility study to evaluate image reconstruction algorithms. Diabetes. Metab. Syndr. Obes. 2019, 12, 439–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rob, S.; Bryant, T.; Wilson, I.; Somani, B. Ultra-low-dose, low-dose, and standard-dose CT of the kidney, ureters, and bladder: Is there a difference? Results from a systematic review of the literature. Clin. Radiol. 2017, 72, 11–15. [Google Scholar] [CrossRef]
- Weisenthal, K.; Karthik, P.; Shaw, M.; Sengupta, D.; Bhargavan-Chatfield, M.; Burleson, J.; Mustafa, A.; Kalra, M.; Moore, C. Evaluation of Kidney Stones with Reduced–Radiation Dose CT: Progress from 2011−2012 to 2015−2016—Not There Yet. Radiology 2017, 286, 581–589. [Google Scholar] [CrossRef]
- Willemink, M.J.; Persson, M.; Pourmorteza, A.; Pelc, N.J.; Fleischmann, D. Photon-counting CT: Technical Principles and Clinical Prospects. Radiology 2018, 289, 293–312. [Google Scholar] [CrossRef]
- Flohr, T.; Petersilka, M.; Henning, A.; Ulzheimer, S.; Ferda, J.; Schmidt, B. Photon-counting CT review. Phys. Med. 2020, 79, 126–136. [Google Scholar] [CrossRef]
- Svahn, T.M.; Gordon, R.; Ast, J.C.; Riffel, J.; Hartbauer, M. Comparison of Photon-Counting and Flat-Panel Digital Mammography for the Purpose of 3D Imaging Using a Novel Image Processing Method. Radiat. Prot. Dosim. 2021, 195, 454–461. [Google Scholar] [CrossRef]
- Kim, H.; Lee, M.; Kim, D.; Lee, D.; Kim, H.-J. Evaluation of photon-counting spectral mammography for classification of breast microcalcifications. Radiat. Phys. Chem. 2019, 162, 39–47. [Google Scholar] [CrossRef]
- Wallis, M.G.; Moa, E.; Zanca, F.; Leifland, K.; Danielsson, M. Two-view and Single-view Tomosynthesis versus Full-field Digital Mammography: High-resolution X-ray Imaging Observer Study. Radiology 2012, 262, 788–796. [Google Scholar] [CrossRef] [PubMed]
- Kappler, S.; Hannemann, T.; Kraft, E.; Kreisler, B.; Niederloehner, D.; Stierstorfer, K.; Flohr, T. First results from a hybrid prototype CT scanner for exploring benefits of quantum-counting in clinical CT. In Proceedings of the SPIE Medical Imaging, San Diego, CA, USA, 4–9 February 2012; Volume 8313. [Google Scholar] [CrossRef]
- Decker, J.A.; Bette, S.; Lubina, N.; Rippel, K.; Braun, F.; Risch, F.; Woźnicki, P.; Wollny, C.; Scheurig-Muenkler, C.; Kroencke, T.J.; et al. Low-dose CT of the abdomen: Initial experience on a novel photon-counting detector CT and comparison with energy-integrating detector CT. Eur. J. Radiol. 2022, 148, 110181. [Google Scholar] [CrossRef] [PubMed]
- Michael, A.E.; Boriesosdick, J.; Schoenbeck, D.; Woeltjen, M.M.; Saeed, S.; Kroeger, J.R.; Horstmeier, S.; Lennartz, S.; Borggrefe, J.; Niehoff, J.H. Image-Quality Assessment of Polyenergetic and Virtual Monoenergetic Reconstructions of Unenhanced CT Scans of the Head: Initial Experiences with the First Photon-Counting CT Approved for Clinical Use. Diagnostics 2022, 12, 265. [Google Scholar] [CrossRef] [PubMed]
- Niehoff, J.H.; Woeltjen, M.M.; Saeed, S.; Michael, A.E.; Boriesosdick, J.; Borggrefe, J.; Kroeger, J.R. Assessment of hepatic steatosis based on virtual non-contrast computed tomography: Initial experiences with a photon counting scanner approved for clinical use. Eur. J. Radiol. 2022, 149, 110185. [Google Scholar] [CrossRef]
- Niehoff, J.H.; Woeltjen, M.M.; Laukamp, K.R.; Borggrefe, J.; Kroeger, J.R. Virtual Non-Contrast versus True Non-Contrast Computed Tomography: Initial Experiences with a Photon Counting Scanner Approved for Clinical Use. Diagnostics 2021, 11, 2377. [Google Scholar] [CrossRef]
- Sartoretti, T.; Racine, D.; Mergen, V.; Jungblut, L.; Monnin, P.; Flohr, T.G.; Martini, K.; Frauenfelder, T.; Alkadhi, H.; Euler, A. Quantum Iterative Reconstruction for Low-Dose Ultra-High-Resolution Photon-Counting Detector CT of the Lung. Diagnostics 2022, 12, 522. [Google Scholar] [CrossRef]
- Stamm, G.; Nagel, H.D. CT-expo: A novel program for dose evaluation in CT. Rofo 2002, 174, 1570–1576. [Google Scholar] [CrossRef]
- Nourian, A.; Ghiraldi, E.; Friedlander, J.I. Dual-Energy CT for Urinary Stone Evaluation. Curr. Urol. Rep. 2020, 22, 1. [Google Scholar] [CrossRef]
- Apfaltrer, G.; Dutschke, A.; Baltzer, P.A.T.; Schestak, C.; Özsoy, M.; Seitz, C.; Veser, J.; Petter, E.; Helbich, T.H.; Ringl, H.; et al. Substantial radiation dose reduction with consistent image quality using a novel low-dose stone composition protocol. World J. Urol. 2020, 38, 2971–2979. [Google Scholar] [CrossRef]
- Nestler, T.; Nestler, K.; Neisius, A.; Isbarn, H.; Netsch, C.; Waldeck, S.; Schmelz, H.U.; Ruf, C. Diagnostic accuracy of third-generation dual-source dual-energy CT: A prospective trial and protocol for clinical implementation. World J. Urol. 2019, 37, 735–741. [Google Scholar] [CrossRef]
- Rodger, F.; Roditi, G.; Aboumarzouk, O. Diagnostic Accuracy of Low and Ultra-Low Dose CT for Identification of Urinary Tract Stones: A Systematic Review. Urol. Int. 2018, 100, 375–385. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Score | Overall Image Quality | Image Noise | Image Sharpness |
|---|---|---|---|
| 5 | Very Good | Very little noise | Structures are perfectly defined, Contours are very sharp |
| 4 | Good | Appropriate noise | Structures are well defined, Contours are sharp |
| 3 | Sufficient | Noisy, evaluation is possible | Structures are defined, Contours are not fully sharp |
| 2 | Bad | Very noisy, evaluation is difficult | Structures can be seen, Contours are barely sharp enough |
| 1 | Very bad | Too much noise for evaluation | Contours are blurred, images are inadequate for diagnostic reporting |
| n | BMI (kg/m2) | ||||
|---|---|---|---|---|---|
| PCCT | S40 | PCCT | S40 | p | |
| Total | 31 | 32 | 27.5 ± 5.1 | 29.0 ± 5.4 | 0.268 |
| Total, BMI < 30 | 23 | 21 | 25.1 ± 3.2 | 26.0 ± 2.8 | 0.353 |
| Male | 15 | 21 | 27.4 ± 4.5 | 29.5 ± 4.3 | 0.191 |
| Female | 16 | 11 | 27.6 ± 5.7 | 28.0 ± 7.2 | 0.981 |
| CTDIvol (mGy) | DLP (mGy*cm) | Eff. Dose (mSv) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| PCCT | S40 | p | PCCT | S40 | p | PCCT | S40 | p | |
| Total | 3.8 ± 1.2 | 5.2 ± 1.5 | <0.001 | 158.2 ± 58.0 | 232.5 ± 67.6 | <0.001 | 2.4 ± 1.0 | 3.4 ± 1.0 | <0.001 |
| Total, BMI < 30 | 3.4 ± 0.8 | 4.5 ± 1.1 | <0.001 | 138.3 ± 33.7 | 203.9 ± 62.5 | <0.001 | 2.1 ± 0.6 | 3.1 ± 1.0 | <0.001 |
| Male | 3.5 ± 0.7 | 5.1 ± 1.3 | <0.001 | 144.7 ± 37.8 | 231.2 ± 55.8 | <0.001 | 2.0 ± 0.5 | 3.3 ± 0.8 | <0.001 |
| Female | 4.1 ± 1.5 | 5.3 ± 1.8 | 0.080 | 170.8 ± 71.0 | 235.0 ± 89.0 | 0.030 | 2.8 ± 1.2 | 3.8 ± 1.4 | 0.034 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niehoff, J.H.; Carmichael, A.F.; Woeltjen, M.M.; Boriesosdick, J.; Lopez Schmidt, I.; Michael, A.E.; Große Hokamp, N.; Piechota, H.; Borggrefe, J.; Kroeger, J.R. Clinical Low Dose Photon Counting CT for the Detection of Urolithiasis: Evaluation of Image Quality and Radiation Dose. Tomography 2022, 8, 1666-1675. https://doi.org/10.3390/tomography8040138
Niehoff JH, Carmichael AF, Woeltjen MM, Boriesosdick J, Lopez Schmidt I, Michael AE, Große Hokamp N, Piechota H, Borggrefe J, Kroeger JR. Clinical Low Dose Photon Counting CT for the Detection of Urolithiasis: Evaluation of Image Quality and Radiation Dose. Tomography. 2022; 8(4):1666-1675. https://doi.org/10.3390/tomography8040138
Chicago/Turabian StyleNiehoff, Julius Henning, Alexandra Fiona Carmichael, Matthias Michael Woeltjen, Jan Boriesosdick, Ingo Lopez Schmidt, Arwed Elias Michael, Nils Große Hokamp, Hansjuergen Piechota, Jan Borggrefe, and Jan Robert Kroeger. 2022. "Clinical Low Dose Photon Counting CT for the Detection of Urolithiasis: Evaluation of Image Quality and Radiation Dose" Tomography 8, no. 4: 1666-1675. https://doi.org/10.3390/tomography8040138
APA StyleNiehoff, J. H., Carmichael, A. F., Woeltjen, M. M., Boriesosdick, J., Lopez Schmidt, I., Michael, A. E., Große Hokamp, N., Piechota, H., Borggrefe, J., & Kroeger, J. R. (2022). Clinical Low Dose Photon Counting CT for the Detection of Urolithiasis: Evaluation of Image Quality and Radiation Dose. Tomography, 8(4), 1666-1675. https://doi.org/10.3390/tomography8040138