

Reading Times of Common Musculoskeletal MRI Examinations: A Survey Study



Abstract
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Survey
2.3. Data Analysis
3. Results
3.1. Respondents
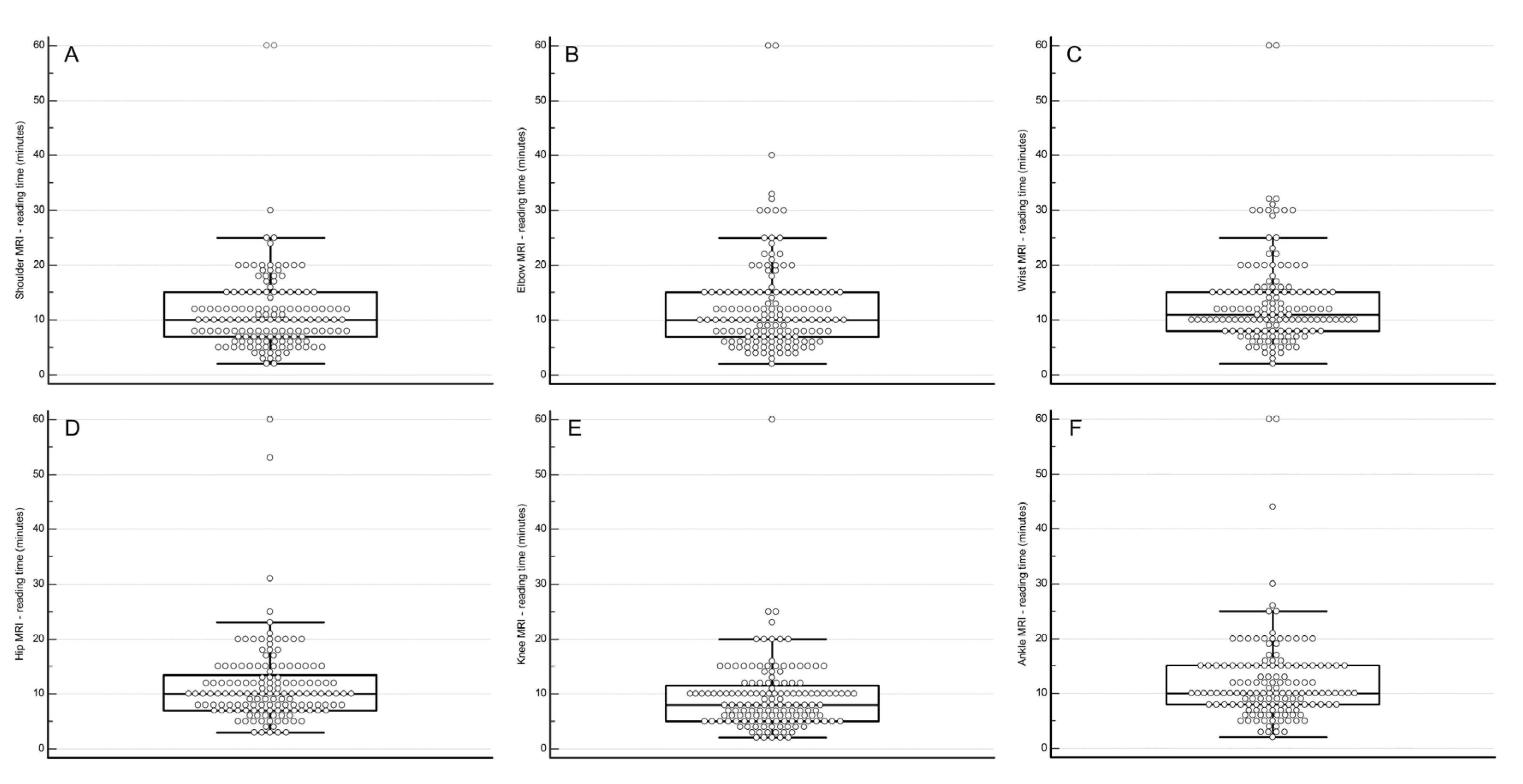
3.2. Reading Time of Common Musculoskeletal MRI Examinations
- Shoulder: median 10 min (interquartile range [IQR] 6–14, range 2–60).
- Elbow: median 10 min (IQR 6–14, range 2–60).
- Wrist: median 11 min (IQR 7.5–14.5, range 2–60).
- Hip: median 10 min (IQR 6.6–13.4, range 3–60).
- Knee: median 8 min (IQR 4.6–11.4, range 2–60).
- Ankle: median 10 min (IQR 6.5–13.5, range 2–60).
3.3. Determinants of Reading Time
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chung, C.B.; Pathria, M.N.; Resnick, D. MRI in MSK: Is it the ultimate examination? Skelet. Radiol. 2024, 53, 1727–1735. [Google Scholar] [CrossRef] [PubMed]
- Del Grande, F.; Guggenberger, R.; Fritz, J. Rapid Musculoskeletal MRI in 2021: Value and Optimized Use of Widely Accessible Techniques. Am. J. Roentgenol. 2021, 216, 704–717. [Google Scholar] [CrossRef] [PubMed]
- Subhas, N. Establishing a New Normal: The 5-Minute MRI. Radiology 2021, 299, 647–648. [Google Scholar] [CrossRef] [PubMed]
- Alexander, R.; Waite, S.; Bruno, M.A.; Krupinski, E.A.; Berlin, L.; Macknik, S.; Martinez-Conde, S. Mandating Limits on Workload, Duty, and Speed in Radiology. Radiology 2022, 304, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Henderson, M. Radiology Facing a Global Shortage. RSNA News. 10 May 2022. Available online: https://www.rsna.org/news/2022/may/global-radiologist-shortage (accessed on 12 July 2024).
- Chew, F.S.; Mulcahy, M.J.; Porrino, J.A.; Mulcahy, H.; Relyea-Chew, A. Prevalence of burnout among musculoskeletal radiologists. Skelet. Radiol. 2017, 46, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Sebro, R. Leveraging the electronic health record to evaluate the validity of the current RVU system for radiologists. Clin. Imaging 2021, 78, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Sokolovskaya, E.; Shinde, T.; Ruchman, R.B.; Kwak, A.J.; Lu, S.; Shariff, Y.K.; Wiggins, E.F.; Talangbayan, L. The Effect of Faster Reporting Speed for Imaging Studies on the Number of Misses and Interpretation Errors: A Pilot Study. J. Am. Coll. Radiol. 2015, 12, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Hanna, T.N.; Lamoureux, C.; Krupinski, E.A.; Weber, S.; Johnson, J.O. Effect of Shift, Schedule, and Volume on Interpretive Accuracy: A Retrospective Analysis of 2.9 Million Radiologic Examinations. Radiology 2018, 287, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Ivanovic, V.; Paydar, A.; Chang, Y.M.; Broadhead, K.; Smullen, D.; Klein, A.; Hacein-Bey, L. Impact of Shift Volume on Neuroradiology Diagnostic Errors at a Large Tertiary Academic Center. Acad. Radiol. 2023, 30, 1584–1588. [Google Scholar] [CrossRef] [PubMed]
- Kasalak, Ö.; Alnahwi, H.; Toxopeus, R.; Pennings, J.P.; Yakar, D.; Kwee, T.C. Work overload and diagnostic errors in radiology. Eur. J. Radiol. 2023, 167, 111032. [Google Scholar] [CrossRef] [PubMed]
- Wintermark, M.; Gupta, V.; Hess, C.; Lee, R.; Maldjian, J.; Mukherjee, S.; Mukherji, S.; Seidenwurm, D.; Kennedy, T. Realistic Productivity in Academic Neuroradiology: A National Survey of Neuroradiology Division Chiefs. Am. J. Neuroradiol. 2023, 44, 759–761. [Google Scholar] [CrossRef] [PubMed]
- Pitman, A.; Cowan, I.A.; Floyd, R.A.; Munro, P.L. Measuring radiologist workload: Progressing from RVUs to study ascribable times. J. Med. Imaging Radiat. Oncol. 2018, 62, 605–618. [Google Scholar] [CrossRef] [PubMed]
- Guermazi, A.; Omoumi, P.; Tordjman, M.; Fritz, J.; Kijowski, R.; Regnard, N.E.; Carrino, J.; Kahn, C.E., Jr.; Knoll, F.; Rueckert, D.; et al. How AI May Transform Musculoskeletal Imaging. Radiology 2024, 310, e230764. [Google Scholar] [CrossRef] [PubMed]
- Gitto, S.; Serpi, F.; Albano, D.; Risoleo, G.; Fusco, S.; Messina, C.; Sconfienza, L.M. AI applications in musculoskeletal imaging: A narrative review. Eur. Radiol. Exp. 2024, 8, 22. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.; Kim, S.; Lee, Y.H. AI musculoskeletal clinical applications: How can AI increase my day-to-day efficiency? Skelet. Radiol. 2022, 51, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Fritz, J.; Kijowski, R.; Recht, M.P. Artificial intelligence in musculoskeletal imaging: A perspective on value propositions, clinical use, and obstacles. Skelet. Radiolology 2022, 51, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Streit, U.; Uhlig, J.; Lotz, J.; Panahi, B.; Seif Amir Hosseini, A. Qualitative and Quantitative Workplace Analysis of Staff Requirement in an Academic Radiology Department. RoFo 2021, 193, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- Stec, N.; Arje, D.; Moody, A.R.; Krupinski, E.A.; Tyrrell, P.N. A Systematic Review of Fatigue in Radiology: Is It a Problem? Am. J. Roentgenol. 2018, 210, 799–806. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Category | Number and % | |
|---|---|---|
| Age distribution | 25–34 years | n = 5 (3.5%) |
| 35–44 years | n = 39 (27.1%) | |
| 45–54 years | n = 48 (33.3%) | |
| 55–64 years | n = 39 (27.1%) | |
| >65 years | n = 13 (9.0%) | |
| Gender | Male | n = 108 (75.0%) |
| Female | n = 35 (24.3%) | |
| Other | n = 1 (0.7%) | |
| Continent | Europe | n = 66 (45.8%) |
| North America | n = 48 (33.3%) | |
| Asia | n = 19 (13.2%) | |
| South America | n = 5 (3.5%) | |
| Australia | n = 5 (3.5%) | |
| Africa | n = 1 (0.7%) | |
| Working in an academic/teaching hospital | Yes | n = 118 (81.9%) |
| No | n = 26 (18.1%) | |
| Fellowship-trained musculoskeletal radiologist | Yes | n = 119 (82.6%) |
| No | n = 25 (17.4%) | |
| Post-residency experience in interpreting and reporting musculoskeletal MRI examinations | <5 years | n = 13 (9.0%) |
| 5–10 years | n = 24 (16.7%) | |
| >10 years | n = 107 (74.3%) | |
| Currently using an AI-based tool to help with interpretation of musculoskeletal MRI examinations | Yes | n = 9 (6.3%) |
| No | n = 135 (93.8%) |
| Variable | Category | Shoulder | Elbow | Wrist | Hip | Knee | Ankle |
|---|---|---|---|---|---|---|---|
| Age 1 | 35–44 years | −3.412 (−6.676 to −0.147) p = 0.041 | −2.120 (−6.016 to 1.775) p = 0.284 | −1.857 (−5.595 to 1.882) p = 0.328 | −3.596 (−6.693 to −0.499) p = 0.023 | −3.541 (−6.312 to −0.770 p = 0.013 | −3.276 (−6.874 to 0.322) p = 0.074 |
| 55–64 years | −0.850 (−3.919 to 2.219) p = 0.585 | −0.859 (−4.522 to 2.803) p = 0.643 | 0.041 (−3.474 to 3.556) p = 0.981 | −1.495 (−4.407 to 1.416) p = 0.312 | −1.370 (−3.975 to 1.225) p = 0.300 | −0.917 (−4.299 to 2.466) p = 0.593 | |
| >65 years | 0.644 (−3.855 to 5.143) p = 0.778 | −1.010 (−6.378 to 4.358) p = 0.710 | −0.405 (−5.557 to 4.747) p = 0.877 | 0.144 (−4.124 to 4.412) p = 0.947 | −0.188 (−4.006 to 3.630) p = 0.923 | 0.223 (−4.735 to 5.181) p = 0.929 | |
| Gender 2 | Female | 5.186 (2.365 to 8.007) p < 0.001 | 4.229 (0.863 to 7.595) p = 0.014 | 3.980 (0.749 to 7.210) p = 0.016 | 3.704 (1.028 to 6.381) p = 0.007 | 2.592 (0.198 to 4.986) p = 0.034 | 3.329 (0.220 to 6.438) p = 0.036 |
| Working in an academic/teaching hospital 3 | No | −3.232 (−6.550 to 0.085) p = 0.056 | −4.086 (−8.045 to −0.127) p = 0.043 | −3.722 (−7.522 to 0.077) p = 0.055 | −3.611 (−6.759 to −0.464) p = 0.025 | −3.038 (−5.854 to −0.222) p = 0.035 | −2.753 (−6.410 to 0.904) p = 0.139 |
| Fellowship-trained musculoskeletal radiologist 4 | No | 4.604 (1.441 to 7.766) p = 0.005 | 3.989 (0.215 to 7.763) p = 0.038 | 4.543 (0.921 to 8.165) p = 0.014 | 2.380 (−0.621 to 5.380) p = 0.119 | 1.447 (−1.238 to 4.131) p = 0.288 | 2.821 (−0.665 to 6.306) p = 0.112 |
| Post-residency experience in interpreting and reporting musculoskeletal MRI examinations 5 | <5 years | 5.837 (1.216 to 10.458) p = 0.014 | 5.639 (0.125 to 11.153) p = 0.045 | 7.214 (1.922 to 12.506) p = 0.008 | 6.948 (2.564 to 11.332) p = 0.002 | 5.355 (1.433 to 9.277) p = 0.008 | 6.162 (1.069 to 11.254) p = 0.018 |
| 5–10 years | 3.022 (−0.750 to 6.794) p = 0.115 | 2.172 (−2.329 to 6.673) p = 0.342 | 2.578 (−1.742 to 6.897) p = 0.240 | 3.660 (0.082 to 7.238) p = 0.045 | 2.159 (−1.042 to 5.360) p = 0.184 | 3.788 (−0.369 to 7.945) p = 0.074 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwee, R.M.; Amasha, A.A.H.; Kwee, T.C. Reading Times of Common Musculoskeletal MRI Examinations: A Survey Study. Tomography 2024, 10, 1527-1533. https://doi.org/10.3390/tomography10090112
Kwee RM, Amasha AAH, Kwee TC. Reading Times of Common Musculoskeletal MRI Examinations: A Survey Study. Tomography. 2024; 10(9):1527-1533. https://doi.org/10.3390/tomography10090112
Chicago/Turabian StyleKwee, Robert M., Asaad A. H. Amasha, and Thomas C. Kwee. 2024. "Reading Times of Common Musculoskeletal MRI Examinations: A Survey Study" Tomography 10, no. 9: 1527-1533. https://doi.org/10.3390/tomography10090112
APA StyleKwee, R. M., Amasha, A. A. H., & Kwee, T. C. (2024). Reading Times of Common Musculoskeletal MRI Examinations: A Survey Study. Tomography, 10(9), 1527-1533. https://doi.org/10.3390/tomography10090112