

The Role of [18F]FDG PET/CT in Predicting Toxicity in Patients with NHL Treated with CAR-T: A Systematic Review

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Methodological Quality Assessment
3. Results
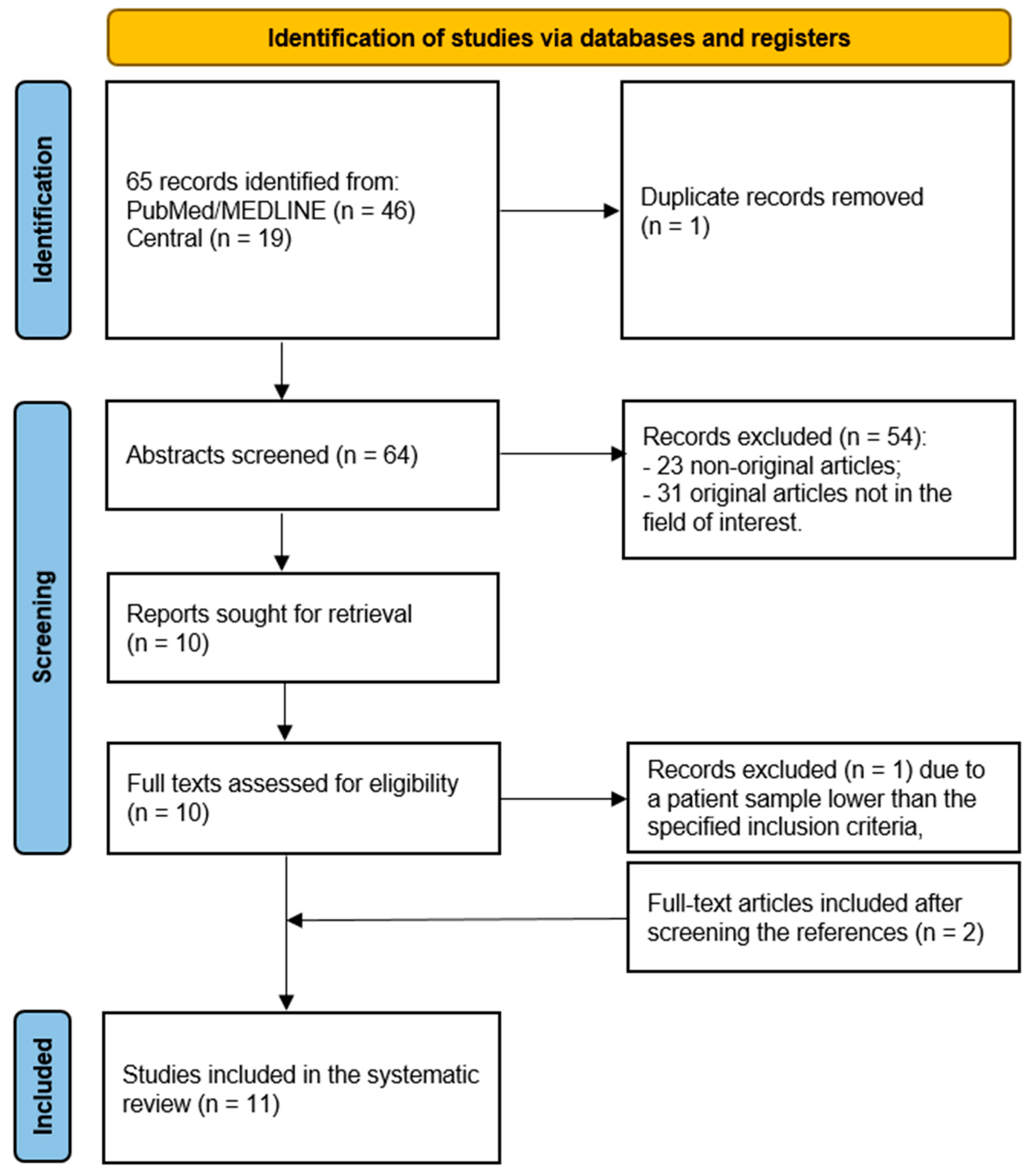
3.1. Literature Search and Eligibility Assessment
3.2. Methodological Quality of Included Studies
3.3. Systematic Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thandra, K.C.; Barsouk, A.; Saginala, K.; Padala, S.A.; Barsouk, A.; Rawla, P. Epidemiology of Non-Hodgkin’s lymphoma. Med. Sci. 2021, 9, 5. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.; Liu, Y.; Fang, X.; Jiang, Y.; Ding, M.; Ge, X.; Yuan, D.; Lu, K.; Li, P.; Li, Y.; et al. The epidemiological patterns of Non-Hodgkin lymphoma: Global estimates of disease burden, risk factors, and temporal trends. Front. Oncol. 2023, 13, 1059914. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, A. CAR-T cell therapy. Int. J. Mol. Sci. 2020, 21, 4303. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Liu, J.; Zhong, J.F.; Zhang, X. Engineering CAR-T cells. Biomark. Res. 2017, 5, 22. [Google Scholar] [CrossRef] [PubMed]
- Sterner, R.C.; Sterner, R.M. CAR-T cell therapy: Current limitations and potential strategies. Blood Cancer J. 2021, 11, 69. [Google Scholar] [CrossRef] [PubMed]
- Brudno, J.N.; Kochenderfer, J.N. Toxicities of chimeric antigen receptor T cells: Recognition and management. Blood 2016, 127, 3321–3330. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. Quadas-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Gui, J.; Li, M.; Xu, J.; Zhang, X.; Mei, H.; Lan, X. [18f]FDG PET/CT for prognosis and toxicity prediction of diffuse large B-cell lymphoma patients with chimeric antigen receptor T-cell therapy. Eur. J. Nucl. Med. Mol. Imaging 2024. [Google Scholar] [CrossRef] [PubMed]
- Leithner, D.; Flynn, J.R.; Devlin, S.M.; Mauguen, A.; Fei, T.; Zeng, S.; Zheng, J.; Imber, B.S.; Hubbeling, H.; Mayerhoefer, M.E.; et al. Conventional and novel [(18)f]FDG PET/CT features as predictors of CAR-T cell therapy outcome in large B-cell lymphoma. J. Hematol. Oncol. 2024, 17, 21. [Google Scholar] [CrossRef] [PubMed]
- Winkelmann, M.; Blumenberg, V.; Rejeski, K.; Quell, C.; Bücklein, V.L.; Ingenerf, M.; Unterrainer, M.; Schmidt, C.; Dekorsy, F.J.; Bartenstein, P.; et al. Predictive value of pre-infusion tumor growth rate for the occurrence and severity of CRS and ICANS in lymphoma under CAR T-cell therapy. Ann. Hematol. 2024, 103, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Ababneh, H.S.; Ng, A.K.; Abramson, J.S.; Soumerai, J.D.; Takvorian, R.W.; Frigault, M.J.; Patel, C.G. Metabolic parameters predict survival and toxicity in chimeric antigen receptor T-cell therapy-treated relapsed/refractory large B-cell lymphoma. Hematol. Oncol. 2024, 42, e3231. [Google Scholar] [CrossRef] [PubMed]
- Crombie, J.L.; Jacobson, C.A.; Redd, R.; Shouse, G.; Herrera, A.F.; Chow, V.A.; Gauthier, J.; Mullane, E.; Cahill, K.; Kline, J.; et al. Prognostic value of early positron emission tomography in patients with large B-cell lymphoma treated with anti-cd19 chimeric antigen receptor T-cell therapy. Haematologica 2023, 108, 3433–3437. [Google Scholar] [CrossRef] [PubMed]
- de Boer, J.W.; Pennings, E.R.A.; Kleinjan, A.; van Doesum, J.A.; Spanjaart, A.M.; Mutsaers, P.; Jak, M.; van der Poel, M.W.M.; Kuipers, M.T.; Adam, J.A.; et al. Inflammatory reactions mimic residual or recurrent lymphoma on [18f]FDG-PET/CT after cd19-directed CAR T-cell therapy. Blood Adv. 2023, 7, 6710–6716. [Google Scholar] [CrossRef] [PubMed]
- Marchal, E.; Palard-Novello, X.; Lhomme, F.; Meyer, M.E.; Manson, G.; Devillers, A.; Marolleau, J.P.; Houot, R.; Girard, A. Baseline [(18)f]FDG PET features are associated with survival and toxicity in patients treated with CAR T cells for large B cell lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2024, 51, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Morbelli, S.; Gambella, M.; Raiola, A.M.; Ghiggi, C.; Bauckneht, M.; Raimondo, T.D.; Lapucci, C.; Sambuceti, G.; Inglese, M.; Angelucci, E. Brain FDG-PET findings in chimeric antigen receptor T-cell therapy neurotoxicity for diffuse large B-cell lymphoma. J. Neuroimaging 2023, 33, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Derlin, T.; Schultze-Florey, C.; Werner, R.A.; Möhn, N.; Skripuletz, T.; David, S.; Beutel, G.; Eder, M.; Ross, T.L.; Bengel, F.M.; et al. (18)f-FDG PET/CT of off-target lymphoid organs in cd19-targeting chimeric antigen receptor T-cell therapy for relapsed or refractory diffuse large B-cell lymphoma. Ann. Nucl. Med. 2021, 35, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Hong, R.; Tan Su Yin, E.; Wang, L.; Zhao, X.; Zhou, L.; Wang, G.; Zhang, M.; Zhao, H.; Wei, G.; Wang, Y.; et al. Tumor burden measured by 18f-FDG PET/CT in predicting efficacy and adverse effects of chimeric antigen receptor T-cell therapy in Non-Hodgkin lymphoma. Front. Oncol. 2021, 11, 713577. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Hu, Y.; Yang, S.; Wei, G.; Zhao, X.; Wu, W.; Zhang, Y.; Zhang, Y.; Chen, D.; Wu, Z.; et al. Role of fluorodeoxyglucose positron emission tomography/computed tomography in predicting the adverse effects of chimeric antigen receptor T cell therapy in patients with Non-Hodgkin lymphoma. Biol. Blood Marrow Transplant. J. Am. Soc. Blood Marrow Transplant. 2019, 25, 1092–1098. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Authors | Year | Country | Journal | n. Patients | Sex | Age (Median; Range) in Years |
|---|---|---|---|---|---|---|
| Gui et al. [9] | 2024 | China | Eur. J. Nucl. Med. Mol. Imaging | 38 | 23 M, 15 F | 55 (29–74) |
| Leithner et al. [10] | 2024 | USA | J. Hematol. Oncol. | 180 | 121 M, 59 F | 66 |
| Winkelmann et al. [11] | 2024 | Germany | Ann. Hematol. | 62 | 37 M, 25 F | 62 |
| Ababneh et al. [12] | 2023 | USA | Hematol. Oncol. | 59 | 33 M, 23 F | 66 (35–90) |
| Crombie et al. [13] | 2023 | USA | Hematologica | 329 | 218 M, 111 F | 61 (19–83) |
| de Boer et al. [14] | 2023 | The Netherlands | Blood Adv. | 18 | SLR: 7 M, 4 F; HR: 7 M, 2 F | 60.5 (35–73) |
| Marchal et al. [15] | 2023 | France | Eur. J. Nucl. Med. Mol. Imaging | 56 | 36 M, 20 F | Mean: 60.2 (±11.5) |
| Morbelli et al. [16] | 2023 | Italy | J. Neuroimaging | 21 | 11 M, 10 F | Mean: 55.8 (±11.8) |
| Derlin et al. [17] | 2021 | Germany | Ann. Nucl. Med. | 10 | 6 M, 4 F | 59 (31–74) |
| Hong et al. [18] | 2021 | China | Front. Oncol. | 41 | 24, 17 F | 2 groups: CR: 44 (25–71); Non-CR: 55 (22–70) |
| Wang et al. [19] | 2019 | China | Biol. Blood Marrow Transplant | 19 | 12 M, 7 F | 43 (22–67) |
| Study | Risk of Bias | Applicability Concerns | |||||
|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference Standard | Flow and Timing | Patient Selection | Index Test | Reference Standard | |
| Ababneh et al. [12] | ☺ | ☹ | ☺ | ☺ | ☺ | ☹ | ☺ |
| Gui et al. [9] | ☺ | ☺ | ☺ | ☹ | ☺ | ☺ | ☺ |
| Lethner et al. [10] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ |
| Winkelmann et al. [11] | ☺ | ☹ | ☺ | ☺ | ☺ | ☹ | ☺ |
| Crombie et al. [13] | ☺ | ? | ☺ | ☺ | ☹ | ☹ | ☹ |
| de Boer et al. [14] | ☹ | ☹ | ☺ | ☹ | ☹ | ☹ | ☺ |
| Marchal et al. [15] | ☺ | ☹ | ☺ | ☹ | ☹ | ☺ | ☺ |
| Morbelli et al. [16] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ |
| Derlin et al. [17] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ |
| Hong et al. [18] | ☺ | ☹ | ☺ | ? | ☺ | ☹ | ☺ |
| Wang et al. [19] | ☹ | ☺ | ☺ | ☺ | ☹ | ☺ | ☺ |
| Study | Type of Toxicity | Main PET Findings |
|---|---|---|
| Ababneh et al. [12] | CRS, ICANS | CRS was linked with high pre-CAR-T TLG. ICANS was linked with high pre-CAR-T MTV. Elevated pre-CAR-T SUVmax was linked to neurological episodes of grade 3–4. |
| Crombie et al. [13] | CRS | Elevated baseline lactate dehydrogenase levels, the presence of grade 3 or higher cytokine release syndrome, and a Deauville score of 4 or 5 on the 1-month PET scan were all associated with an increased risk of disease progression, according to a univariable Cox regression analysis. |
| De Boer et al. [14] | SLR, HR | SLR: symmetric bilateral hilar and mediastinal lymphadenopathy, as well as lymphadenopathy in other areas, accompanied by increased [18F]FDG uptake. In the biopsy, there was no sign of lymphoma and only noncaseating epithelioid cell granulomatous inflammation. HR: increased [18F]FDG uptake at the site of the initial tumor shortly after CAR-T injection (about one month). A biopsy revealed necrotic lymphoma cells lacking granulomatous processes surrounded by sheets of foamy histiocytic cells. |
| Derlin et al. [14] | CRS, neurotoxicity | Four patients had CRS and four developed neurotoxicity. Neurotoxicity was linked to higher baseline SUVmax. A decrease in metabolic activity in lymphoid organs was associated with less favorable results, but an early metabolic response was required for remission. |
| Gui et al. [9] | CRS | Strong direct correlation between pre-infusion SUVmax and the grade of CRS. Moderate direct correlation between pre-infusion TLG and the CRS grade. Pre-infusion SUVmax and CRS risk: higher pre-infusion SUVmax values were linked to an increased risk of developing a higher grade of CRS. |
| Hong et al. [18] | CRS, coagulation abnormalities (elevated D-dimer levels and prolonged clotting times) | CRS incidence, cytokine levels were considerably higher in patients with higher PET/CT parameters at baseline. Increased D-dimer levels and longer clotting times, two coagulation disorders that might result in bleeding issues, are connected with greater baseline PET/CT parameters. |
| Leithner et al. [10] | CRS | Grade ≥ 2 CRS was correlated with pre-infusion MTV (odds ratio [OR] for a 100 mL increase: 1.08 [95% confidence interval (CI), 1.01–1.20], p = 0.031). |
| Marchal et al. [15] | CRS, ICANS | Overall survival and progression-free survival were independently predicted by sDmax and TMTV, respectively. Grades 2 through 4 ICANS were associated with greater spleen SUVmean levels, while grades 2 through 4 CRS were linked to higher levels of C-reactive protein and liver SUVmean. |
| Morbelli et al. [16] | CRS, ICANS | Five of the eleven patients who had CRS went on to develop ICANS. Whereas ICANS was associated with a more widespread hypometabolic pattern in the frontal cortex, CRS without ICANS revealed hypometabolism in bilateral medial and lateral temporal lobes, posterior parietal lobes, and other regions. |
| Wang et al. [19] | CRS, pseudoprogression | Lower MTV and TLG were associated with mild to moderate CRS, whereas greater MTV and TLG were linked to severe CRS. There appears to be a connection between a higher baseline disease burden and more severe CRS, as evidenced by pseudoprogression and local immune activation. |
| Winkelmann et al. [11] | CRS, ICANS | The calculated pre-infusion TGR had minimal relationships with the severity of CRS and ICANS, indicating that it might not have a substantial effect on treatment planning or outcome prediction. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quartuccio, N.; Ialuna, S.; Pulizzi, S.; D’Oppido, D.; Nicolosi, S.; Moreci, A.M. The Role of [18F]FDG PET/CT in Predicting Toxicity in Patients with NHL Treated with CAR-T: A Systematic Review. Tomography 2024, 10, 869-879. https://doi.org/10.3390/tomography10060066
Quartuccio N, Ialuna S, Pulizzi S, D’Oppido D, Nicolosi S, Moreci AM. The Role of [18F]FDG PET/CT in Predicting Toxicity in Patients with NHL Treated with CAR-T: A Systematic Review. Tomography. 2024; 10(6):869-879. https://doi.org/10.3390/tomography10060066
Chicago/Turabian StyleQuartuccio, Natale, Salvatore Ialuna, Sabina Pulizzi, Dante D’Oppido, Stefania Nicolosi, and Antonino Maria Moreci. 2024. "The Role of [18F]FDG PET/CT in Predicting Toxicity in Patients with NHL Treated with CAR-T: A Systematic Review" Tomography 10, no. 6: 869-879. https://doi.org/10.3390/tomography10060066
APA StyleQuartuccio, N., Ialuna, S., Pulizzi, S., D’Oppido, D., Nicolosi, S., & Moreci, A. M. (2024). The Role of [18F]FDG PET/CT in Predicting Toxicity in Patients with NHL Treated with CAR-T: A Systematic Review. Tomography, 10(6), 869-879. https://doi.org/10.3390/tomography10060066