
Visibility of Intracranial Perforating Arteries Using Ultra-High-Resolution Photon-Counting Detector Computed Tomography (CT) Angiography

Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Ethical Approval
2.3. CT Imaging
2.4. Subjective Analysis
2.5. Objective Analysis
2.6. Statistical Analysis
3. Results
3.1. Study Population
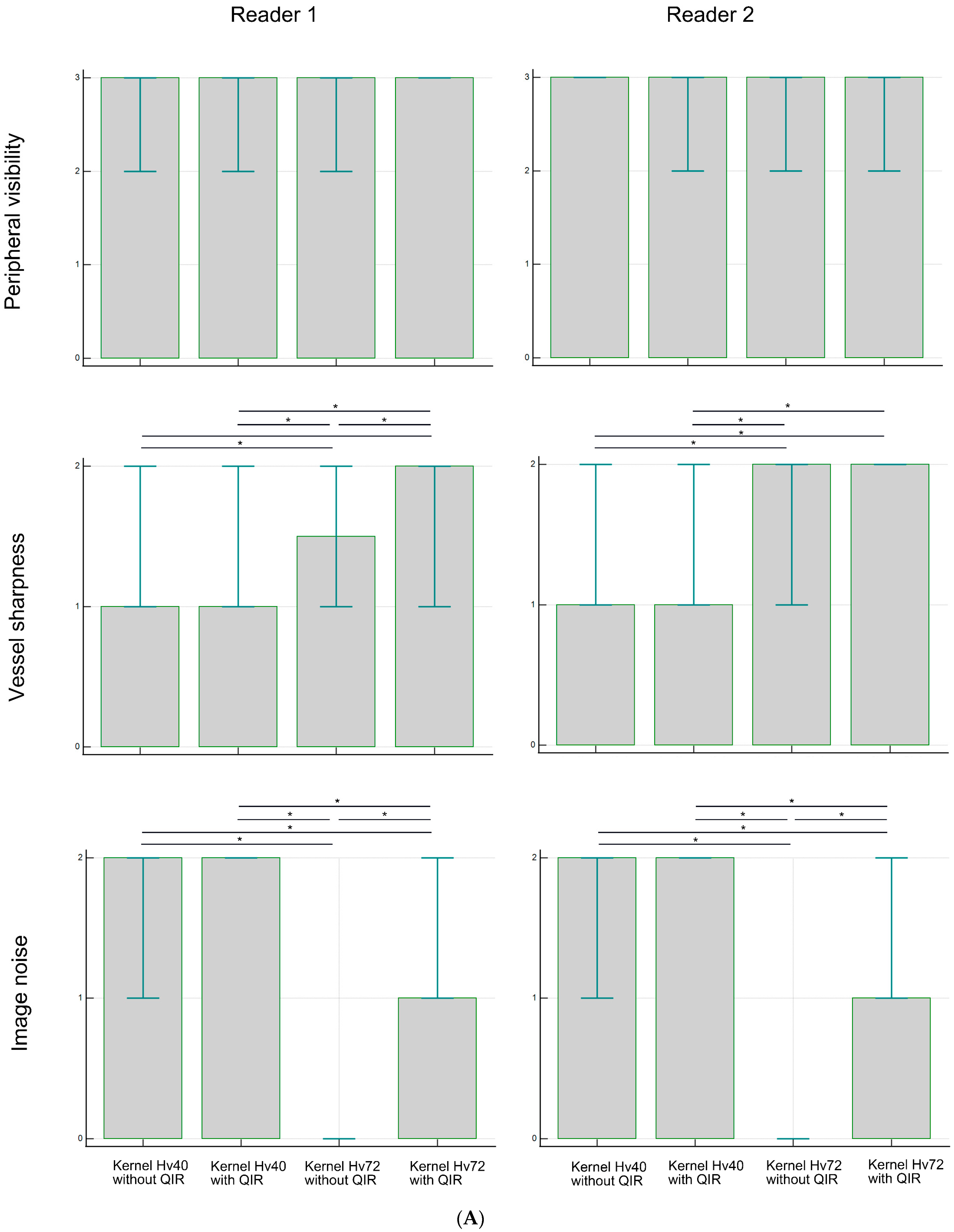
3.2. Subjective Analysis
3.3. Objective Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Campbell, B.C.V.; De Silva, D.A.; Macleod, M.R.; Coutts, S.B.; Schwamm, L.H.; Davis, S.M.; Donnan, G.A. Ischaemic stroke. Nat. Rev. Dis. Primers 2019, 5, 70. [Google Scholar] [CrossRef] [PubMed]
- Morotti, A.; Boulouis, G.; Dowlatshahi, D.; Li, Q.; Shamy, M.; Al-Shahi Salman, R.; Rosand, J.; Cordonnier, C.; Goldstein, J.N.; Charidimou, A. Intracerebral haemorrhage expansion: Definitions, predictors, and prevention. Lancet Neurol. 2023, 22, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Orrison, W.W., Jr.; Snyder, K.V.; Hopkins, L.N.; Roach, C.J.; Ringdahl, E.N.; Nazir, R.; Hanson, E.H. Whole-brain dynamic CT angiography and perfusion imaging. Clin. Radiol. 2011, 66, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S. Developmental anomalies of the distal vertebral artery and posterior inferior cerebellar artery: Diagnosis by CT angiography and literature review. Surg. Radiol. Anat. 2016, 38, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Wildberger, J.E.; Alkadhi, H. New horizons in vascular imaging with photon-counting detector CT. Investig. Radiol. 2023, 58, 499–504. [Google Scholar] [CrossRef]
- Esquivel, A.; Ferrero, A.; Mileto, A.; Baffour, F.; Horst, K.; Rajiah, P.S.; Inoue, A.; Leng, S.; McCollough, C.; Fletcher, J.G. Photon-counting detector CT: Key points radiologists should know. Korean J. Radiol. 2022, 23, 854–865. [Google Scholar] [CrossRef]
- Flohr, T.; Schmidt, B. Technical basics and clinical benefits of photon-counting CT. Investig. Radiol. 2023, 58, 441–450. [Google Scholar] [CrossRef]
- Leng, S.; Bruesewitz, M.; Tao, S.; Rajendran, K.; Halaweish, A.F.; Campeau, N.G.; Fletcher, J.G.; McCollough, C.H. Photon-counting detector CT: System design and clinical applications of an emerging technology. Radiographics 2019, 39, 729–743. [Google Scholar] [CrossRef]
- Flohr, T.; Petersilka, M.; Henning, A.; Ulzheimer, S.; Ferda, J.; Schmidt, B. Photon-counting CT review. Phys. Med. 2020, 79, 126–136. [Google Scholar] [CrossRef]
- Sawall, S.; Amato, C.; Klein, L.; Wehrse, E.; Maier, J.; Kachelriess, M. Toward molecular imaging using spectral photon-counting computed tomography? Curr. Opin. Chem. Biol. 2021, 63, 163–170. [Google Scholar] [CrossRef]
- Tortora, M.; Gemini, L.; D’Iglio, I.; Ugga, L.; Spadarella, G.; Cuocolo, R. Spectral photon-counting computed tomography: A review on technical principles and clinical applications. J. Imaging 2022, 8, 112. [Google Scholar] [CrossRef] [PubMed]
- Abel, F.; Schubert, T.; Winklhofer, S. Advanced neuroimaging with photon-counting detector CT. Investig. Radiol. 2023, 58, 472–481. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H.; Rajendran, K.; Leng, S. Standardization and quantitative imaging with photon-counting detector CT. Investig. Radiol. 2023, 58, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Douek, P.C.; Boccalini, S.; Oei, E.H.G.; Cormode, D.P.; Pourmorteza, A.; Boussel, L.; Si-Mohamed, S.A.; Budde, R.P.J. Clinical applications of photon-counting CT: A review of pioneer studies and a glimpse into the future. Radiology 2023, 309, e222432. [Google Scholar] [CrossRef]
- Benson, J.C.; Campeau, N.G.; Diehn, F.E.; Lane, J.I.; Leng, S.; Moonis, G.; ASHNR Research Committee. Photon-counting CT in the head and neck: Current applications and future prospects. Am. J. Neuroradiol. 2024, 45, 1000–1005. [Google Scholar] [CrossRef]
- Hagen, F.; Soschynski, M.; Weis, M.; Hagar, M.T.; Krumm, P.; Ayx, I.; Taron, J.; Krauss, T.; Hein, M.; Ruile, P.; et al. Photon-counting computed tomography—Clinical application in oncological, cardiovascular, and pediatric radiology. RoFo 2024, 196, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Mergen, V.; Sartoretti, T.; Baer-Beck, M.; Schmidt, B.; Petersilka, M.; Wildberger, J.E.; Euler, A.; Eberhard, M.; Alkadhi, H. Ultra-high-resolution coronary CT angiography with photon-counting detector CT: Feasibility and image characterization. Investig. Radiol. 2022, 57, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Ucar, F.A.; Frenzel, M.; Kronfeld, A.; Altmann, S.; Sanner, A.P.; Mercado, M.A.A.; Uphaus, T.; Brockmann, M.A.; Othman, A.E. Improvement of neurovascular imaging using ultra-high-resolution computed tomography angiography. Clin. Neuroradiol. 2024, 34, 189–199. [Google Scholar] [CrossRef]
- Kwiatkowska, M.; Rzeplinski, R.; Ciszek, B. Anatomy of the pontine arteries and perforators of the basilar artery in humans. J. Anat. 2023, 243, 997–1006. [Google Scholar] [CrossRef]
- Kang, H.S.; Han, M.H.; Kwon, B.J.; Kwon, O.K.; Kim, S.H.; Chang, K.H. Evaluation of the lenticulostriate arteries with rotational angiography and 3D reconstruction. Am. J. Neuroradiol. 2005, 26, 306–312. [Google Scholar]
- Sartoretti, T.; Racine, D.; Mergen, V.; Jungblut, L.; Monnin, P.; Flohr, T.G.; Martini, K.; Frauenfelder, T.; Alkadhi, H.; Euler, A. Quantum iterative reconstruction for low-dose ultra-high-resolution photon-counting detector CT of the lung. Diagnostics 2022, 12, 522. [Google Scholar] [CrossRef] [PubMed]
- Vecsey-Nagy, M.; Varga-Szemes, A.; Schoepf, U.J.; Tremamunno, G.; Fink, N.; Zsarnoczay, E.; Szilveszter, B.; Graafen, D.; Halfmann, M.C.; Vattay, B.; et al. Ultra-high resolution coronary CT angiography on photon-counting detector CT: Bi-centre study on the impact of quantum iterative reconstruction on image quality and accuracy of stenosis measurements. Eur. J. Radiol. 2024, 176, 111517. [Google Scholar] [CrossRef] [PubMed]
- Graafen, D.; Stoehr, F.; Halfmann, M.C.; Emrich, T.; Foerster, F.; Yang, Y.; Duber, C.; Muller, L.; Kloeckner, R. Quantum iterative reconstruction on a photon-counting detector CT improves the quality of hepatocellular carcinoma imaging. Cancer Imaging 2023, 23, 69. [Google Scholar] [CrossRef] [PubMed]
- Racine, D.; Mergen, V.; Viry, A.; Eberhard, M.; Becce, F.; Rotzinger, D.C.; Alkadhi, H.; Euler, A. Photon-counting detector CT with quantum iterative reconstruction: Impact on liver lesion detection and radiation dose reduction. Investig. Radiol. 2023, 58, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Sartoretti, T.; Landsmann, A.; Nakhostin, D.; Eberhard, M.; Roeren, C.; Mergen, V.; Higashigaito, K.; Raupach, R.; Alkadhi, H.; Euler, A. Quantum iterative reconstruction for abdominal photon-counting detector CT improves image quality. Radiology 2022, 303, 339–348. [Google Scholar] [CrossRef]
- Huflage, H.; Grunz, J.P.; Kunz, A.S.; Patzer, T.S.; Sauer, S.T.; Christner, S.A.; Petritsch, B.; Ergun, S.; Bley, T.A.; Luetkens, K.S. Potential of employing a quantum iterative reconstruction algorithm for ultra-high-resolution photon-counting detector CT of the hip. Radiography 2023, 29, 44–49. [Google Scholar] [CrossRef]
- White Paper NAEOTOM Alpha. Available online: https://marketing.webassets.siemens-healthineers.com/059a54d26d606b58/e7e8e6ebde2e/siemens-healthineers-DI-CT-NAEOTOM-Alpha-Whitepaper.pdf (accessed on 27 October 2024).
- Fransson, V.; Mellander, H.; Ramgren, B.; Andersson, H.; Arena, F.; Ydstrom, K.; Ullberg, T.; Wasselius, J. Image quality of spectral brain computed tomography angiography using halved dose of iodine contrast medium. Neuroradiology 2023, 65, 1333–1342. [Google Scholar] [CrossRef]
- Tóth, A.; Chetta, J.A.; Yazdani, M.; Matheus, M.G.; O’Doherty, J.; Tipnis, S.V.; Spampinato, M.V. Neurovascular imaging with ultra-high-resolution photon-counting CT: Preliminary findings on image-quality evaluation. Am. J. Neuroradiol. 2024, 45, 1450–1457. [Google Scholar] [CrossRef]
- Wongpakaran, N.; Wongpakaran, T.; Wedding, D.; Gwet, K.L. A comparison of Cohen’s Kappa and Gwet’s AC1 when calculating inter-rater reliability coefficients: A study conducted with personality disorder samples. BMC Med. Res. Methodol. 2013, 13, 61. [Google Scholar] [CrossRef]
- Whatman, C.; Hing, W.; Hume, P. Physiotherapist agreement when visually rating movement quality during lower extremity functional screening tests. Phys. Ther. Sport 2012, 13, 87–96. [Google Scholar] [CrossRef]
- Takahashi, S. Neurovascular Imaging: MRI and Microangiography; Springer: London, UK, 2010; pp. 53–196. [Google Scholar]
- Djulejić, V.; Marinković, S.; Milić, V.; Georgievski, B.; Rašić, M.; Aksić, M.; Puškaš, L. Common features of the cerebral perforating arteries and their clinical significance. Acta Neurochir. 2015, 157, 743–754. [Google Scholar] [CrossRef] [PubMed]
- Murayama, K.; Suzuki, S.; Nagata, H.; Oda, J.; Nakahara, I.; Katada, K.; Fujii, K.; Toyama, H. Visualization of lenticulostriate arteries on CT angiography using ultra-high-resolution CT compared with conventional-detector CT. Am. J. Neuroradiol. 2020, 41, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Fink, N.; Emrich, T.; Graafen, D.; Richter, R.; Bockius, S.; Wolf, E.V.; Laux, G.; Kavermann, L.; Muller, L.; et al. Optimization of kernel type and sharpness level improves objective and subjective image quality for high-pitch photon counting coronary CT angiography. Diagnostics 2023, 13, 1937. [Google Scholar] [CrossRef] [PubMed]
- Harteveld, A.A.; De Cocker, L.J.; Dieleman, N.; van der Kolk, A.G.; Zwanenburg, J.J.; Robe, P.A.; Luijten, P.R.; Hendrikse, J. High-resolution postcontrast time-of-flight MR angiography of intracranial perforators at 7.0 Tesla. PLoS ONE 2015, 10, e0121051. [Google Scholar] [CrossRef]
- Kang, C.K.; Park, C.A.; Kim, K.N.; Hong, S.M.; Park, C.W.; Kim, Y.B.; Cho, Z.H. Non-invasive visualization of basilar artery perforators with 7T MR angiography. J. Magn. Reson. Imaging 2010, 32, 544–550. [Google Scholar] [CrossRef]
- Shi, Z.; Zhao, X.; Zhu, S.; Miao, X.; Zhang, Y.; Han, S.; Wang, B.; Zhang, B.; Ye, X.; Dai, Y.; et al. Time-of-flight intracranial MRA at 3 T versus 5 T versus 7 T: Visualization of distal small cerebral arteries. Radiology 2023, 306, 207–217. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LSA | Kernel Hv40 Without QIR | Kernel Hv40 with QIR | Kernel Hv72 Without QIR | Kernel Hv72 with QIR | p |
| Peripheral visibility | |||||
| Reader 1 | 3 (2–3) | 3 (2–3) | 3 (2–3) | 3 (3–3) | 0.293 |
| Reader 2 | 3 (3–3) | 3 (2–3) | 3 (2–3) | 3 (2–3) | 0.109 |
| Vessel sharpness | |||||
| Reader 1 | 1 (1–2) | 1 (1–2) | 1.5 (1–2) | 2 (1–2) | <0.00001 |
| Reader 2 | 1 (1–2) | 1 (1–2) | 2 (1–2) | 2 (2–2) | <0.00001 |
| Noise | |||||
| Reader 1 | 2 (1–2) | 2 (2–2) | 0 (0–0) | 1 (1–1) | <0.00001 |
| Reader 2 | 2 (1–2) | 2 (2–2) | 0 (0–0) | 1 (1–2) | <0.00001 |
| PA | Kernel Hv40 Without QIR | Kernel Hv40 with QIR | Kernel Hv72 Without QIR | Kernel Hv72 with QIR | p |
| Peripheral visibility | |||||
| Reader 1 | 2 (1–3) | 2 (1–3) | 2 (1–2) | 2 (1–3) | 0.257 |
| Reader 2 | 2 (1–3) | 2 (1–3) | 2 (1–2) | 2 (1–3) | 0.00007 |
| Vessel sharpness | |||||
| Reader 1 | 1 (1–2) | 1 (1–2) | 1 (1–2) | 2 (1–2) | <0.00001 |
| Reader 2 | 1 (1–2) | 1 (1–2) | 2 (1–2) | 2 (1–2) | <0.00001 |
| Noise | |||||
| Reader 1 | 2 (1–2) | 2 (2–2) | 0 (0–0) | 1 (1–2) | <0.00001 |
| Reader 2 | 2 (1–2) | 2 (2–2) | 0 (0–1) | 1 (1–1) | <0.00001 |
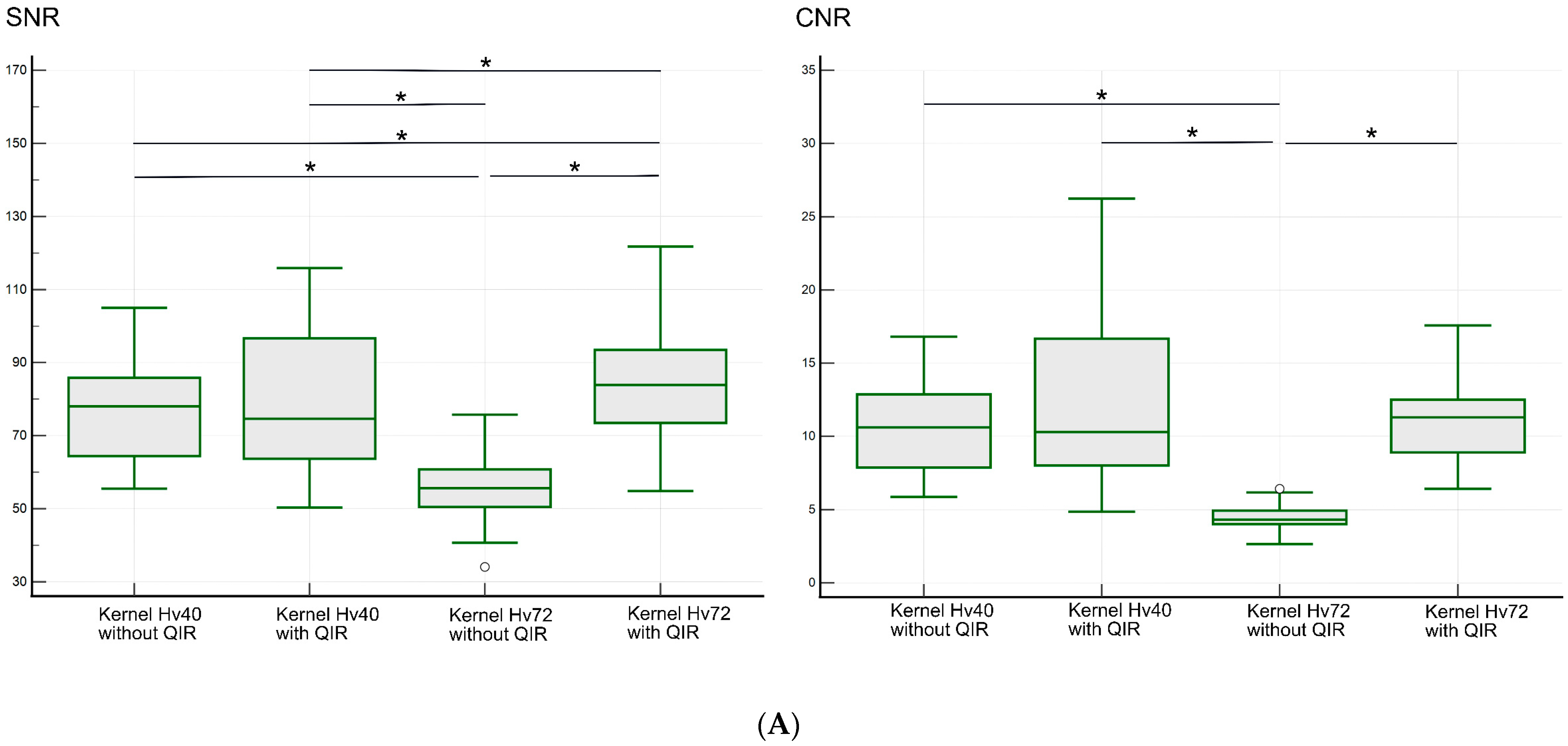
| Kernel Hv40 Without QIR | Kernel Hv40 with QIR | Kernel Hv72 Without QIR | Kernel Hv72 with QIR | p | |
|---|---|---|---|---|---|
| LSA region | |||||
| SNR | 78.0 (55.5–105.0) | 76.6 (50.3–115.9) | 55.7 (34.1–75.8) | 85.4 (54.9–121.8) | <0.00001 |
| CNR | 10.6 (5.9–16.8) | 10.3 (4.9–26.2) | 4.3 (2.6–6.4) | 11.3 (6.4–17.6) | <0.00001 |
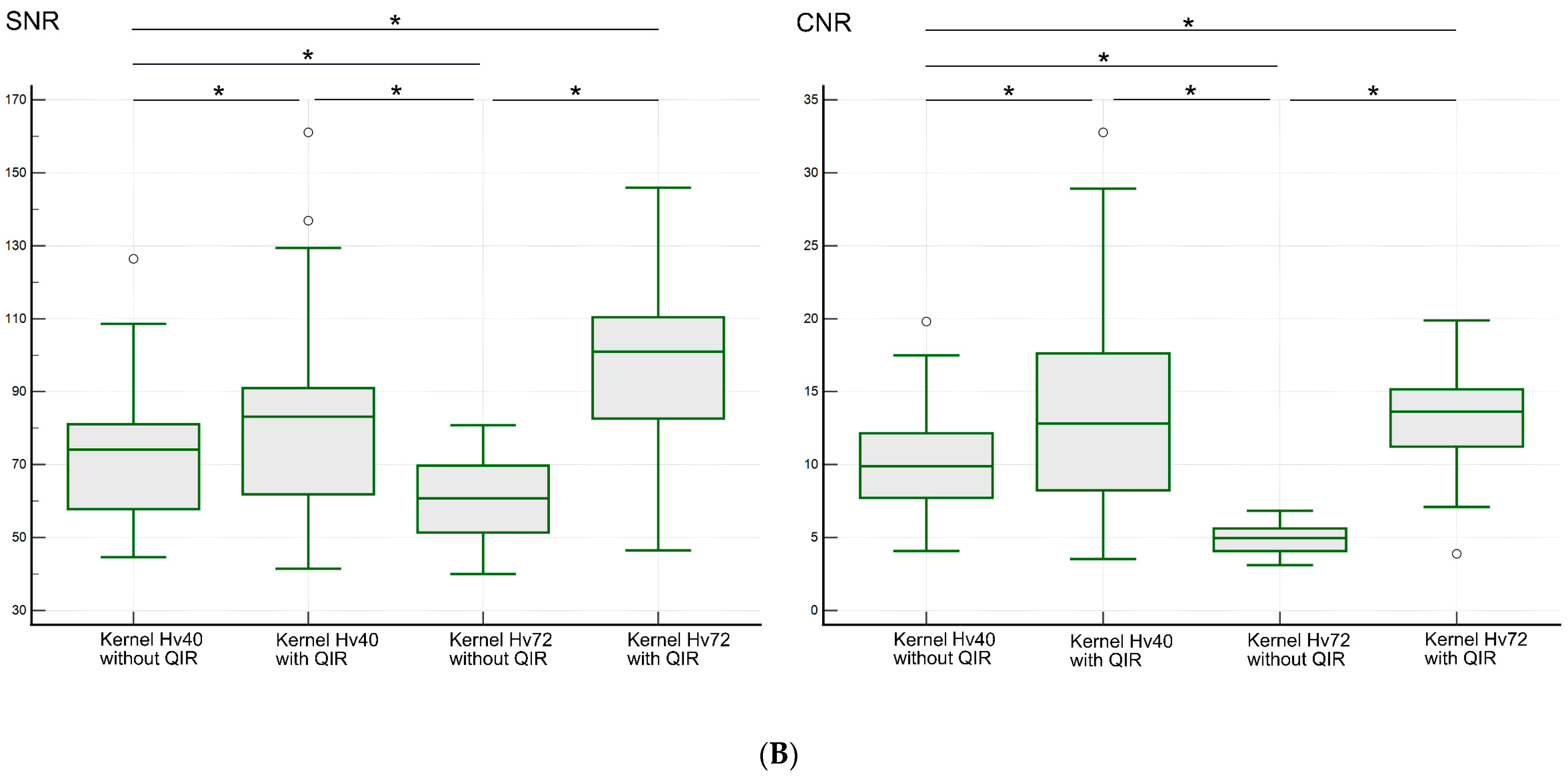
| PA region | |||||
| SNR | 74.1 (44.6–126.4) | 83.2 (41.5–161.1) | 60.7 (40.0–80.8) | 101.0 (46.5–145.9) | <0.00001 |
| CNR | 9.9 (4.1–19.8) | 12.8 (3.5–32.8) | 5.0 (3.1–6.8) | 13.6 (3.9–19.9) | <0.00001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okazaki, T.; Niwa, T.; Yoshida, R.; Sorimachi, T.; Hashimoto, J. Visibility of Intracranial Perforating Arteries Using Ultra-High-Resolution Photon-Counting Detector Computed Tomography (CT) Angiography. Tomography 2024, 10, 1867-1880. https://doi.org/10.3390/tomography10120136
Okazaki T, Niwa T, Yoshida R, Sorimachi T, Hashimoto J. Visibility of Intracranial Perforating Arteries Using Ultra-High-Resolution Photon-Counting Detector Computed Tomography (CT) Angiography. Tomography. 2024; 10(12):1867-1880. https://doi.org/10.3390/tomography10120136
Chicago/Turabian StyleOkazaki, Takashi, Tetsu Niwa, Ryoichi Yoshida, Takatoshi Sorimachi, and Jun Hashimoto. 2024. "Visibility of Intracranial Perforating Arteries Using Ultra-High-Resolution Photon-Counting Detector Computed Tomography (CT) Angiography" Tomography 10, no. 12: 1867-1880. https://doi.org/10.3390/tomography10120136
APA StyleOkazaki, T., Niwa, T., Yoshida, R., Sorimachi, T., & Hashimoto, J. (2024). Visibility of Intracranial Perforating Arteries Using Ultra-High-Resolution Photon-Counting Detector Computed Tomography (CT) Angiography. Tomography, 10(12), 1867-1880. https://doi.org/10.3390/tomography10120136