
Emerging Polymer Materials in Trackable Endovascular Embolization and Cell Delivery: From Hype to Hope



Abstract
1. Background
2. Endovascular Embolization
2.1. Clinical Applications

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Application | Polymer Embolics for Embolization | Treatment Outcome | Future Goal | Reference |
|---|---|---|---|---|
| Vascular malformations (Hemorrhage, Aneurysms, AVMs) | Liquid embolics (NBCA, PHILTM, Onyx®) |
|
| [24,30,31,37] |
| Hypervascular tumors (e.g., hepatocellular carcinoma or HCC) | Drug eluting beads/microspheres (e.g., calibrated PVA, gelatin sponge, crosslinked starch particles) |
|
| [40,41,42] |
| Uterine fibroids | Calibrated PVA microspheres |
|
| [43] |
2.2. Embolization Techniques
3. Polymer-Based Embolic Agents
3.1. Particulate Embolic Agents
3.1.1. Gelatin Sponge
3.1.2. Spherical and Nonspherical PVA
| Embolic Agents (Commercial) | Material Composition | Material Description | Therapeutic Loading | Degradability (In Vivo) | Reference |
|---|---|---|---|---|---|
| GelFoam® | Denatured collagen | Hemostatic gelatin sponge made of natural polymer | No | Yes | [11] |
| ContourTM | Poly(vinyl alcohol) | Irregular particles | No | No | [11] |
| DC Bead® LC Bead® Bead Block® | Poly(vinyl alcohol)-co-poly(2-acrylamido-2-methylpropane sulfonate) | Microsphere | Yes (Doxorubicin and Irinotecan) | No | [79,80] |
| HepaSphereTM QuadraSphereTM | Poly(vinyl acetate-co-sodium acrylate) | Microsphere | Yes (Doxorubicin) | No | [81,82] |
| Embosphere® EmboGold® | Tris-acyl gelatin | Microsphere EmboGold® has 2% gold incorporated into the sphere | No | No | [83] |
| Embozene® | Polyphosphazene-coated polymethylmethacrylate | Microsphere | Yes (Doxorubicin and Irinotecan) | No | [84] |
| EmboCept® | Crosslinked starch | Microsphere | No | Yes | [85] |
| Trufill® | Poly(N-butyl-cyanoacrylate) | Glue | No | No | [86,87] |
| PHILTM | Poly(lactide-co-glycolide) and Poly(hydroxyl ethyl methacrylate) | Precipitating liquid embolic | No | No | [88] |
| Onyx® | Poly(vinyl alcohol)-co-polyethylene | Precipitating liquid embolic | No | No | [89,90] |
3.1.3. HepaSphereTM/QuadraSphereTM
3.1.4. Embosphere®
3.1.5. Embozene®
3.1.6. Other Degradable Microspheres
3.2. Liquid Embolic Agents
3.2.1. N-Butyl Cyanoacrylate (NBCA)
3.2.2. Precipitating Hydrophobic Injectable Liquid (PHILTM)
3.2.3. Onyx®
3.3. Emerging Embolic Agents
3.3.1. Thermoresponsive Embolic Gels
3.3.2. pH-Responsive Gelling System
3.3.3. Self-Healing Embolic Gels
3.3.4. Shear-Thinning Hydrogels
3.3.5. Other Potential Polymeric Embolic Agents
3.4. Embolic Agents with Trackability
4. Injectable Polymers for Cell Delivery
5. Conclusions and Future Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ripoll, C.; Bañares, R.; Beceiro, I.; Menchén, P.; Catalina, M.V.; Echenagusia, A.; Turegano, F. Comparison of transcatheter arterial embolization and surgery for treatment of bleeding peptic ulcer after endoscopic treatment failure. J. Vasc. Interv. Radiol. 2004, 15, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Loffroy, R.; Rao, P.; Ota, S.; De Lin, M.; Kwak, B.K.; Geschwind, J.F. Embolization of acute nonvariceal upper gastrointestinal hemorrhage resistant to endoscopic treatment: Results and predictors of recurrent bleeding. Cardiovasc. Intervent. Radiol. 2010, 33, 1088–1100. [Google Scholar] [CrossRef] [PubMed]
- Seinstra, B.A.; van Delden, O.M.; van Erpecum, K.J.; van Hillegersberg, R.; Mali, W.P.T.M.; van den Bosch, M.A.A.J. Minimally invasive image-guided therapy for inoperable hepatocellular carcinoma: What is the evidence today? Insights Imaging 2010, 1, 167–181. [Google Scholar] [CrossRef][Green Version]
- Hu, J.; Albadawi, H.; Chong, B.W.; Deipolyi, A.R.; Sheth, R.A.; Khademhosseini, A.; Oklu, R. Advances in biomaterials and technologies for vascular embolization. Adv. Mater. 2019, 31, 1901071. [Google Scholar] [CrossRef] [PubMed]
- Wu, E.M.; El Ahmadieh, T.Y.; McDougall, C.M.; Aoun, S.G.; Mehta, N.; Neeley, O.J.; Plitt, A.; Ban, V.S.; Sillero, R.; White, J.A.; et al. Embolization of brain arteriovenous malformations with intent to cure: A systematic review. J. Neurosurg. 2019, 132, 388–399. [Google Scholar] [CrossRef]
- Pesapane, F.; Nezami, N.; Patella, F.; Geschwind, J.F. New concepts in embolotherapy of HCC. Med. Oncol. 2017, 34, 58. [Google Scholar] [CrossRef]
- Elmokadem, A.H.; Abdelsalam, H.; El-Morsy, A.; Elsabbagh, A. Trans-arterial embolization of malignant tumor-related gastrointestinal bleeding: Technical and clinical efficacy. Egypt. J. Radiol. Nucl. Med. 2019, 50, 45. [Google Scholar] [CrossRef]
- Shi, Z.X.; Yang, J.; Liang, H.W.; Cai, Z.H.; Bai, B. Emergency transcatheter arterial embolization for massive gastrointestinal arterial hemorrhage. Medicine 2017, 96, e9437. [Google Scholar] [CrossRef]
- Poursaid, A.; Jensen, M.M.; Huo, E.; Ghandehari, H. Polymeric materials for embolic and chemoembolic applications. J. Control. Release 2016, 240, 414–433. [Google Scholar] [CrossRef]
- SPEAKMAN, T.J. Internal Occlusion of a Carotid-Cavernous Fistula. J. Neurosurg. 1964, 21, 303–305. [Google Scholar] [CrossRef]
- Vaidya, S.; Tozer, K.R.; Chen, J. An overview of embolic agents. Semin. Intervent. Radiol. 2008, 25, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Martin, J. Embolization materials and principles. In Demystifying Interventional Radiology; Athreya, S., Ed.; Springer: Cham, Switzerland, 2016; pp. 57–60. [Google Scholar]
- Weng, L.; Rostamzadeh, P.; Nooryshokry, N.; Le, H.C.; Golzarian, J. In vitro and in vivo evaluation of biodegradable embolic microspheres with tunable anticancer drug release. Acta Biomater. 2013, 9, 6823–6833. [Google Scholar] [CrossRef] [PubMed]
- Sharma, K.V.; Bascal, Z.; Kilpatrick, H.; Ashrafi, K.; Willis, S.L.; Dreher, M.R.; Lewis, A.L. Long-term biocompatibility, imaging appearance and tissue effects associated with delivery of a novel radiopaque embolization bead for image-guided therapy. Biomaterials 2016, 103, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Hu, H.; Min, N.; Wei, Y.; Li, X.; Li, X. Application and outlook of topical hemostatic materials: A narrative review. Ann. Transl. Med. 2021, 9, 577. [Google Scholar] [CrossRef]
- Ladage, D.; Turnbull, I.C.; Ishikawa, K.; Takewa, Y.; Rapti, K.; Morel, C.; Karakikes, I.; Hadri, L.; Müller-Ehmsen, J.; Costa, K.D.; et al. Delivery of gelfoam-enabled cells and vectors into the pericardial space using a percutaneous approach in a porcine model. Gene Ther. 2011, 18, 979–985. [Google Scholar] [CrossRef]
- Loffroy, R.; Favelier, S.; Pottecher, P.; Estivalet, L.; Genson, P.Y.; Gehin, S.; Cercueil, J.P.; Krausé, D. Transcatheter arterial embolization for acute nonvariceal upper gastrointestinal bleeding: Indications, techniques and outcomes. Diagn. Interv. Imaging 2015, 96, 731–744. [Google Scholar] [CrossRef]
- Yang, X.; Wang, S.; Zhang, X.; Ye, C.; Wang, S.; An, X. Development of PVA-based microsphere as a potential embolization agent. Mater. Sci. Eng. C 2022, 135, 112677. [Google Scholar] [CrossRef]
- Poursaid, A.; Price, R.; Tiede, A.; Olson, E.; Huo, E.; McGill, L.; Ghandehari, H.; Cappello, J. In situ gelling silk-elastinlike protein polymer for transarterial chemoembolization. Biomaterials 2015, 57, 142–152. [Google Scholar] [CrossRef]
- Kirmani, J.F.; Alkawi, A.; Ahmed, S.; Janjua, N.; Khatri, I.; Divani, A.A.; Qureshi, A.I. Endovascular treatment of subarachnoid hemorrhage. Neurol. Res. 2005, 27 (Suppl. 1), S103–S107. [Google Scholar] [CrossRef]
- Kauvar, D.S.; Wade, C.E. The epidemiology and modern management of traumatic hemorrhage: US and international perspectives. Crit. Care 2005, 9, S1. [Google Scholar] [CrossRef][Green Version]
- Kauvar, D.S.; Lefering, R.; Wade, C.E. Impact of hemorrhage on trauma outcome: An overview of epidemiology, clinical presentations, and therapeutic considerations. J. Trauma Inj. Infect. Crit. Care 2006, 60, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Irita, K. Risk and crisis management in intraoperative hemorrhage: Human factors in hemorrhagic critical events. Korean J. Anesthesiol. 2011, 60, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, L.G.; Ljungdahl, M.; Sundbom, M.; Nyman, R. Transcatheter Arterial Embolization versus Surgery in the Treatment of Upper Gastrointestinal Bleeding after Therapeutic Endoscopy Failure. J. Vasc. Interv. Radiol. 2008, 19, 1413–1418. [Google Scholar] [CrossRef] [PubMed]
- Poultsides, G.A.; Kim, C.J.; Orlando, R.; Peros, G.; Hallisey, M.J.; Vignati, P.V. Angiographic embolization for gastroduodenal hemorrhage: Safety, efficacy, and predictors of outcome. Arch. Surg. 2008, 143, 457–461. [Google Scholar] [CrossRef]
- Yetkin, E.; Ozturk, S. Dilating Vascular Diseases: Pathophysiology and Clinical Aspects. Int. J. Vasc. Med. 2018, 2018, 9024278. [Google Scholar] [CrossRef]
- Norman, P.E.; Powell, J.T. Site specificity of aneurysmal disease. Circulation 2010, 121, 560–568. [Google Scholar] [CrossRef]
- Juvela, S. Prevalence of and risk factors for intracranial aneurysms. Lancet Neurol. 2011, 10, 595–597. [Google Scholar] [CrossRef]
- Karhunen, V.; Bakker, M.K.; Ruigrok, Y.M.; Gill, D.; Larsson, S.C. Modifiable risk factors for intracranial aneurysm and aneurysmal subarachnoid hemorrhage: A mendelian randomization study. J. Am. Heart Assoc. 2021, 10, e022277. [Google Scholar] [CrossRef]
- Rodriguez, J.N.; Hwang, W.; Horn, J.; Landsman, T.L.; Boyle, A.; Wierzbicki, M.A.; Hasan, S.M.; Follmer, D.; Bryant, J.; Small, W.; et al. Design and biocompatibility of endovascular aneurysm filling devices. J. Biomed. Mater. Res. Part A 2015, 103, 1577–1594. [Google Scholar] [CrossRef]
- Fries, F.; Tomori, T.; Schulz-Schaeffer, W.J.; Jones, J.; Yilmaz, U.; Kettner, M.; Simgen, A.; Reith, W.; Mühl-Benninghaus, R. Treatment of experimental aneurysms with a GPX embolic agent prototype: Preliminary angiographic and histological results. J. Neurointerv. Surg. 2022, 14, 286–290. [Google Scholar] [CrossRef]
- Lubarsky, M.; Ray, C.E.; Funaki, B. Embolization Agents—Which One Should Be Used When? Part 1: Large-Vessel Embolization. Semin. Intervent. Radiol. 2009, 26, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Nasiri, S.; Khosravani, M.R. Progress and challenges in fabrication of wearable sensors for health monitoring. Sens. Actuators A Phys. 2020, 312, 112105. [Google Scholar] [CrossRef]
- Negussie, A.H.; de Ruiter, Q.M.B.; Britton, H.; Donahue, D.R.; Boffi, Q.; Kim, Y.S.; Pritchard, W.F.; Moonen, C.; Storm, G.; Lewis, A.L.; et al. Synthesis, characterization, and imaging of radiopaque bismuth beads for image-guided transarterial embolization. Sci. Rep. 2021, 11, 533. [Google Scholar] [CrossRef] [PubMed]
- Reinhold, H.A.; West, M.P. Nervous System. In Acute Care Handbook for Physical Therapists; Paz, J.C., West, M.P., Eds.; W.B. Saunders: Philadelphia, PA, USA, 2014; pp. 123–160. ISBN 9780323227551. [Google Scholar]
- Ajiboye, N.; Chalouhi, N.; Starke, R.M.; Zanaty, M.; Bell, R. Cerebral arteriovenous malformations: Evaluation and management. Sci. World J. 2014, 2014, 649036. [Google Scholar] [CrossRef] [PubMed]
- Sousa, E.C.; Teixeira, M.J.; Piske, R.L.; Albuquerque, L.S.; Côrrea, S.; Benabou, S.; Welling, L.C.; de Sousa, L.M.; Figueiredo, E.G. The role of preradiosurgical embolization in the management of grades III, IV, and V arteriovenous malformations. Front. Surg. 2016, 3, 37. [Google Scholar] [CrossRef]
- Ellis, J.A.; Lavine, S.D. Role of Embolization for Cerebral Arteriovenous Malformations. Methodist Debakey Cardiovasc. J. 2014, 10, 234–239. [Google Scholar] [CrossRef]
- Vollherbst, D.F.; Chapot, R.; Bendszus, M.; Möhlenbruch, M.A. Glue, onyx, squid or PHIL? Liquid embolic agents for the embolization of cerebral arteriovenous malformations and dural arteriovenous fistulas. Clin. Neuroradiol. 2022, 32, 25–38. [Google Scholar] [CrossRef]
- Plasencia, A.R.; O’Higgins, T.V. Large parotid and cheek infantile hemangiomas refractory to medical treatment: Is there a role for embolization? Am. J. Interv. Radiol. 2020, 4, 21. [Google Scholar] [CrossRef]
- Idée, J.M.; Guiu, B. Use of Lipiodol as a drug-delivery system for transcatheter arterial chemoembolization of hepatocellular carcinoma: A review. Crit. Rev. Oncol. Hematol. 2013, 88, 530–549. [Google Scholar] [CrossRef]
- Wildgruber, M.; Sadick, M.; Müller-Wille, R.; Wohlgemuth, W.A. Vascular tumors in infants and adolescents. Insights Imaging 2019, 10, 30. [Google Scholar] [CrossRef]
- Mutiso, S.K.; Oindi, F.M.; Hacking, N.; Obura, T. Uterine necrosis after uterine artery embolization for symptomatic fibroids. Case Rep. Obstet. Gynecol. 2018, 2018, 9621741. [Google Scholar] [CrossRef]
- Nagy, J.A.; Chang, S.H.; Dvorak, A.M.; Dvorak, H.F. Why are tumour blood vessels abnormal and why is it important to know? Br. J. Cancer 2009, 100, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Tohme, S.; Simmons, R.L.; Tsung, A. Surgery for cancer: A trigger for metastases. Cancer Res. 2017, 77, 1548–1552. [Google Scholar] [CrossRef] [PubMed]
- Ghouri, Y.A.; Mian, I.; Rowe, J.H. Review of hepatocellular carcinoma: Epidemiology, etiology, and carcinogenesis. J. Carcinog. 2017, 16, 1. [Google Scholar] [CrossRef] [PubMed]
- Raza, A.; Sood, G.K. Hepatocellular carcinoma review: Current treatment, and evidence-based medicine. World J. Gastroenterol. 2014, 20, 4115–4127. [Google Scholar] [CrossRef] [PubMed]
- Rammohan, A.; Sathyanesan, J.; Ramaswami, S.; Lakshmanan, A.; Senthil-Kumar, P.; Srinivasan, U.P.; Ramasamy, R.; Ravichandran, P. Embolization of liver tumors: Past, present and future. World J. Radiol. 2012, 4, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Bulman, J.C.; Ascher, S.M.; Spies, J.B. Current concepts in uterine fibroid embolization. Radiographics 2012, 32, 1735–1750. [Google Scholar] [CrossRef]
- Khan, A.T.; Shehmar, M.; Gupta, J.K. Uterine fibroids: Current perspectives. Int. J. Women’s Health 2014, 6, 95–114. [Google Scholar] [CrossRef]
- Khurana, A.; Hangge, P.T.; Albadawi, H.; Knuttinen, M.G.; Alzubaidi, S.J.; Naidu, S.G.; Kriegshauser, J.S.; Oklu, R.; Chong, B.W. The use of transarterial approaches in peripheral arteriovenous malformations (AVMs). J. Clin. Med. 2018, 7, 109. [Google Scholar] [CrossRef]
- Powerski, M.; Meyer-Wilmes, P.; Omari, J.; Damm, R.; Seidensticker, M.; Friebe, B.; Fischbach, F.; Pech, M. Transcatheter arterial embolization of acute bleeding as 24/7 service: Predictors of outcome and mortality. Br. J. Radiol. 2018, 91, 20180516. [Google Scholar] [CrossRef]
- Fontana, F.; Piacentino, F.; Ossola, C.; Coppola, A.; Curti, M.; Macchi, E.; De Marchi, G.; Floridi, C.; Ierardi, A.M.; Carrafiello, G.; et al. Transcatheter arterial embolization in acute non-variceal gastrointestinal bleedings: A ten-year single-center experience in 91 patients and review of the literature. J. Clin. Med. 2021, 10, 4979. [Google Scholar] [CrossRef] [PubMed]
- Bolus, C.; Yamada, R.; Alshora, S.; Hannegan, C.; Anderson, B. Transarterial embolization of a hepatic arteriovenous malformation in an infant using Onyx: A case report and review of the differential diagnosis imaging findings. J. Radiol. Case Rep. 2014, 8, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Liu, F.Y.; Yuan, H.J.; Tian, X.M.; Tang, J.; Ye, T.; Ji, K. Therapeutic evaluation and management strategy of transarterial embolization for giant liver hemangiomas exceeding 10 cm in diameter. Cardiovasc. Intervent. Radiol. 2021, 44, 2005–2007. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Nowicki, K.W.; Gross, B.A.; Wagner, W.R. Injectable hydrogels for vascular embolization and cell delivery: The potential for advances in cerebral aneurysm treatment. Biomaterials 2021, 277, 121109. [Google Scholar] [CrossRef] [PubMed]
- Tam, K.Y.; Leung, K.C.F.; Wang, Y.X.J. Chemoembolization agents for cancer treatment. Eur. J. Pharm. Sci. 2011, 44, 1–10. [Google Scholar] [CrossRef]
- Chen, Y.P.; Zhang, J.L.; Zou, Y.; Wu, Y.L. Recent advances on polymeric beads or hydrogels as embolization agents for improved transcatheter arterial chemoembolization (TACE). Front. Chem. 2019, 7, 408. [Google Scholar] [CrossRef]
- Sieghart, W.; Hucke, F.; Peck-Radosavljevic, M. Transarterial chemoembolization: Modalities, indication, and patient selection. J. Hepatol. 2015, 62, 1187–1195. [Google Scholar] [CrossRef]
- Wiggermann, P.; Sieron, D.; Brosche, C.; Brauer, T.; Scheer, F.; Platzek, I.; Wawrzynek, W.; Stroszczynski, C. Transarterial Chemoembolization of Child-A hepatocellular carcinoma: Drug-eluting bead TACE (DEB TACE) vs. TACE with Cisplatin/Lipiodol (cTACE). Med. Sci. Monit. 2011, 17, CR189–CR195. [Google Scholar] [CrossRef]
- Luz, J.H.M.; Luz, P.M.; Martin, H.S.; Gouveia, H.R.; Levigard, R.B.; Nogueira, F.D.; Rodrigues, B.C.; De Miranda, T.N.; Mamede, M.H. DEB TACE for Intermediate and advanced HCC—Initial Experience in a Brazilian Cancer Center. Cancer Imaging 2017, 17, 5. [Google Scholar] [CrossRef]
- Jia, G.; Van Valkenburgh, J.; Chen, A.Z.; Chen, Q.; Li, J.; Zuo, C.; Chen, K. Recent advances and applications of microspheres and nanoparticles in transarterial chemoembolization for hepatocellular carcinoma. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2022, 14, e1749. [Google Scholar] [CrossRef]
- Manyonda, I.; Belli, A.-M.; Lumsden, M.-A.; Moss, J.; McKinnon, W.; Middleton, L.J.; Cheed, V.; Wu, O.; Sirkeci, F.; Daniels, J.P.; et al. Uterine-artery embolization or myomectomy for uterine fibroids. N. Engl. J. Med. 2020, 383, 440–451. [Google Scholar] [CrossRef] [PubMed]
- Andersen, P.E.; Lund, N.; Justesen, P.; Munk, T.; Elle, B.; Floridon, C. Uterine artery embolization of symptomatic uterine fibroids: Initial success and short-term results. Acta Radiol. 2001, 42, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Pakiz, M.; But, I. Uterine artery embolization for symptomatic uterine fibroids. Int. J. Gynecol. Obstet. 2008, 101, 81–82. [Google Scholar] [CrossRef]
- Abramowitz, S.D.; Israel, G.M.; McCarthy, S.M.; Pollak, J.; White, R.L.; Tal, M.G. Comparison of four embolic materials at uterine artery artery embolization by using postprocedural MR imaging enhancement. Radiology 2009, 250, 482–487. [Google Scholar] [CrossRef]
- Siskin, G.P.; Beck, A.; Schuster, M.; Mandato, K.; Englander, M.; Herr, A. Leiomyoma infarction after uterine artery embolization: A prospective randomized study comparing tris-acryl gelatin microspheres versus polyvinyl alcohol microspheres. J. Vasc. Interv. Radiol. 2008, 19, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.C.H.; Lok, I.; Ho, S.S.Y.; Tong, M.M.B.; Hui, J.W.Y. Comparison of clinical outcomes of tris-acryl microspheres versus polyvinyl alcohol microspheres for uterine artery embolization for leiomyomas: Results of a randomized trial. J. Vasc. Interv. Radiol. 2011, 22, 1229–1235. [Google Scholar] [CrossRef] [PubMed]
- Vilos, G.A.; Vilos, E.C.; Romano, W.; Abu-Rafea, B. Temporary uterine artery occlusion for treatment of menorrhagia and uterine fibroids using an incisionless Doppler-guided transvaginal clamp: Case report. Hum. Reprod. 2006, 21, 269–271. [Google Scholar] [CrossRef]
- Istre, O.; Hald, K.; Qvigstad, E. Multiple Myomas treated with a temporary, noninvasive, doppler-directed, transvaginal uterine artery clamp. J. Am. Assoc. Gynecol. Laparosc. 2004, 11, 273–276. [Google Scholar] [CrossRef]
- Abada, H.T.; Golzarian, J. Gelatine sponge particles: Handling characteristics for endovascular use. Tech. Vasc. Interv. Radiol. 2007, 10, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Behrens, A.M.; Sikorski, M.J.; Kofinas, P. Hemostatic strategies for traumatic and surgical bleeding. J. Biomed. Mater. Res. Part A 2014, 102, 4182–4194. [Google Scholar] [CrossRef]
- Miyayama, S.; Yamakado, K.; Anai, H.; Abo, D.; Minami, T.; Takaki, H.; Kodama, T.; Yamanaka, T.; Nishiofuku, H.; Morimoto, K.; et al. Guidelines on the use of gelatin sponge particles in embolotherapy. Jpn. J. Radiol. 2014, 32, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Osuga, K.; Maeda, N.; Higashihara, H.; Hori, S.; Nakazawa, T.; Tanaka, K.; Nakamura, M.; Kishimoto, K.; Ono, Y.; Tomiyama, N. Current status of embolic agents for liver tumor embolization. Int. J. Clin. Oncol. 2012, 17, 306–315. [Google Scholar] [CrossRef]
- Makuuchi, M.; Sukigara, M.; Mori, T.; Kobayashi, J.; Yamazaki, S.; Hasegawa, H.; Moriyama, N.; Takayasu, K.; Hirohashi, S. Bile duct necrosis: Complication of transcatheter hepatic arterial embolization. Radiology 1985, 156, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Wáng, Y.X.J.; De Baere, T.; Idée, J.M.; Ballet, S. Transcatheter embolization therapy in liver cancer: An update of clinical evidences. Chin. J. Cancer Res. 2015, 27, 96–121. [Google Scholar] [CrossRef] [PubMed]
- Katsumori, T.; Kasahara, T.; Akazawa, K. Long-term outcomes of uterine artery embolization using gelatin sponge particles alone for symptomatic fibroids. Am. J. Roentgenol. 2012, 186, 848–854. [Google Scholar] [CrossRef]
- Tadavarthy, S.M.; Knight, L.; Ovitt, T.W.; Snyder, C.; Amplatz, K. Therapeutic transcatheter arterial embolization. Radiology 1974, 112, 13–16. [Google Scholar] [CrossRef]
- Caine, M.; Carugo, D.; Zhang, X.; Hill, M.; Dreher, M.R.; Lewis, A.L.; Caine, M.; Carugo, D.; Zhang, X.; Hill, M.; et al. Review of the development of methods for characterization of microspheres for use in embolotherapy: Translating bench to cathlab. Adv. Healthc. Mater. 2017, 6, 1601291. [Google Scholar] [CrossRef]
- Gadaleta, C.D.; Ranieri, G. Trans-arterial chemoembolization as a therapy for liver tumours: New clinical developments and suggestions for combination with angiogenesis inhibitors. Crit. Rev. Oncol. Hematol. 2011, 80, 40–53. [Google Scholar] [CrossRef] [PubMed]
- Lewis, A.L. Embolisation devices from biomedical polymers for intra-arterial occlusion and drug delivery in the treatment of cancer. Biomater. Cancer Ther. Diagn. Prev. Ther. 2013, 207–239. [Google Scholar] [CrossRef]
- Khankan, A.A.; Osuga, K.; Hori, S.; Morii, E.; Murakami, T.; Nakamura, H. Embolic effects of superabsorbent polymer microspheres in rabbit renal model: Comparison with tris-acryl gelatin microspheres and polyvinyl alcohol. Radiat. Med. 2004, 22, 384–390. [Google Scholar]
- Laurent, A.; Beaujeux, R.; Wassef, M.; Rüfenacht, D.; Boschetti, E.; Merland, J.J. Trisacryl gelatin microspheres for therapeutic embolization, I: Development and in vitro evaluation. Am. J. Neuroradiol. 1996, 17, 533–540. [Google Scholar] [PubMed]
- Stampfl, U.; Stampfl, S.; Bellemann, N.; Sommer, C.M.; Lopez-Benitez, R.; Thierjung, H.; Radeleff, B.; Berger, I.; Richter, G.M. Experimental liver embolization with four different spherical embolic materials: Impact on inflammatory tissue and foreign body reaction. Cardiovasc. Intervent. Radiol. 2009, 32, 303–312. [Google Scholar] [CrossRef]
- Pieper, C.C.; Meyer, C.; Vollmar, B.; Hauenstein, K.; Schild, H.H.; Wilhelm, K.E. Temporary arterial embolization of liver parenchyma with degradable starch microspheres (EmboCept®S) in a swine model. Cardiovasc. Intervent. Radiol. 2015, 38, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Rabinov, J.D.; Yoo, A.J.; Ogilvy, C.S.; Carter, B.S.; Hirsch, J.A. ONYX versus n-BCA for embolization of cranial dural arteriovenous fistulas. J. Neurointerv. Surg. 2013, 5, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Kania, R.E.; Sauvaget, E.; Guichard, J.P.; Chapot, R.; Huy, P.T.B.; Herman, P. Early postoperative CT scanning for juvenile nasopharyngeal angiofibroma: Detection of residual disease. Am. J. Neuroradiol. 2005, 26, 82–88. [Google Scholar] [PubMed]
- Prashar, A.; Butt, S.; Shaida, N. Introducing PHIL (precipitating hydrophobic injectable liquid)—A new embolic agent for the body interventional radiologist. Diagn. Interv. Radiol. 2020, 26, 140–142. [Google Scholar] [CrossRef]
- Kolber, M.K.; Shukla, P.A.; Kumar, A.; Silberzweig, J.E. Ethylene Vinyl Alcohol Copolymer (Onyx) embolization for acute hemorrhage: A systematic review of peripheral applications. J. Vasc. Interv. Radiol. 2015, 26, 809–815. [Google Scholar] [CrossRef]
- Saeed Kilani, M.; Izaaryene, J.; Cohen, F.; Varoquaux, A.; Gaubert, J.Y.; Louis, G.; Jacquier, A.; Bartoli, J.M.; Moulin, G.; Vidal, V. Ethylene vinyl alcohol copolymer (Onyx®) in peripheral interventional radiology: Indications, advantages and limitations. Diagn. Interv. Imaging 2015, 96, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Osuga, K.; Khankan, A.A.; Hori, S.; Okada, A.; Sugiura, T.; Maeda, M.; Nagano, H.; Yamada, A.; Murakami, T.; Nakamura, H. Transarterial embolization for large hepatocellular carcinoma with use of superabsorbent polymer microspheres: Initial experience. J. Vasc. Interv. Radiol. 2002, 13, 929–934. [Google Scholar] [CrossRef]
- Osuga, K.; Hori, S.; Kitayoshi, H.; Khankan, A.A.; Okada, A.; Sugiura, T.; Murakami, T.; Hosokawa, K.; Nakamura, H. Embolization of high flow arteriovenous malformations: Experience with use of superabsorbent polymer microspheres. J. Vasc. Interv. Radiol. 2002, 13, 1125–1133. [Google Scholar] [CrossRef]
- Maeda, N.; Osuga, K.; Higashihara, H.; Mikami, K.; Tomoda, K.; Hori, S.; Nakazawa, T.; Nakamura, H. In Vitro Characterization of Cisplatin-loaded Superabsorbent Polymer Microspheres Designed for Chemoembolization. J. Vasc. Interv. Radiol. 2010, 21, 877–881. [Google Scholar] [CrossRef] [PubMed]
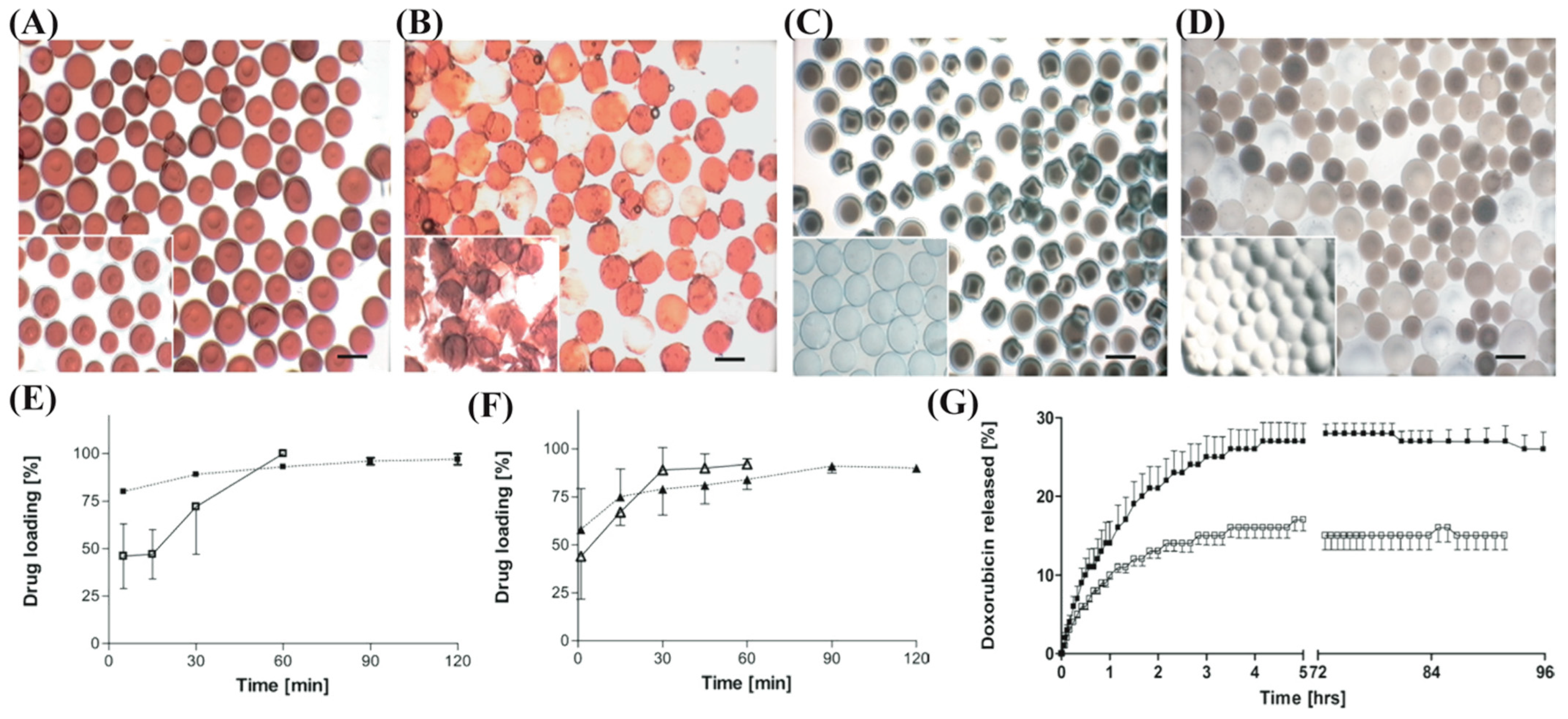
- Jordan, O.; Denys, A.; De Baere, T.; Boulens, N.; Doelker, E. Comparative study of chemoembolization loadable beads: In vitro drug release and physical properties of DC bead and hepasphere loaded with doxorubicin and irinotecan. J. Vasc. Interv. Radiol. 2010, 21, 1084–1090. [Google Scholar] [CrossRef] [PubMed]
- Laurent, A.; Wassef, M.; Chapot, R.; Houdart, E.; Merland, J.J. Location of vessel occlusion of calibrated tris-acryl gelatin microspheres for tumor and arteriovenous malformation embolization. J. Vasc. Interv. Radiol. 2004, 15, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Bates, M.C.; Yousaf, A.; Sun, L.; Barakat, M.; Kueller, A. Translational research and early favorable clinical results of a novel polyphosphazene (Polyzene-F) nanocoating. Regen. Eng. Transl. Med. 2019, 5, 341–353. [Google Scholar] [CrossRef]
- Poursaid, A. Design and Development of Silk-Elastinlike Protein Polymer Liquid Embolics for Treatment of Hepatocellular Carcinoma. Ph.D. Thesis, The University of Utah, Salt Lake City, UT, USA, 2016. [Google Scholar]
- Vogl, T.J.; Langenbach, M.C.; Hammerstingl, R.; Albrecht, M.H.; Chatterjee, A.R.; Gruber-Rouh, T. Evaluation of two different transarterial chemoembolization protocols using Lipiodol and degradable starch microspheres in therapy of hepatocellular carcinoma: A prospective trial. Hepatol. Int. 2021, 15, 685–694. [Google Scholar] [CrossRef]
- Ludwig, J.M.; Iezzi, R.; Theysohn, J.M.; Albrecht, T.; Posa, A.; Gross, A. European multicenter study on degradable starch microsphere TACE: The digestible way to conquer HCC in patients with high tumor burden. Cancers 2021, 13, 5122. [Google Scholar] [CrossRef]
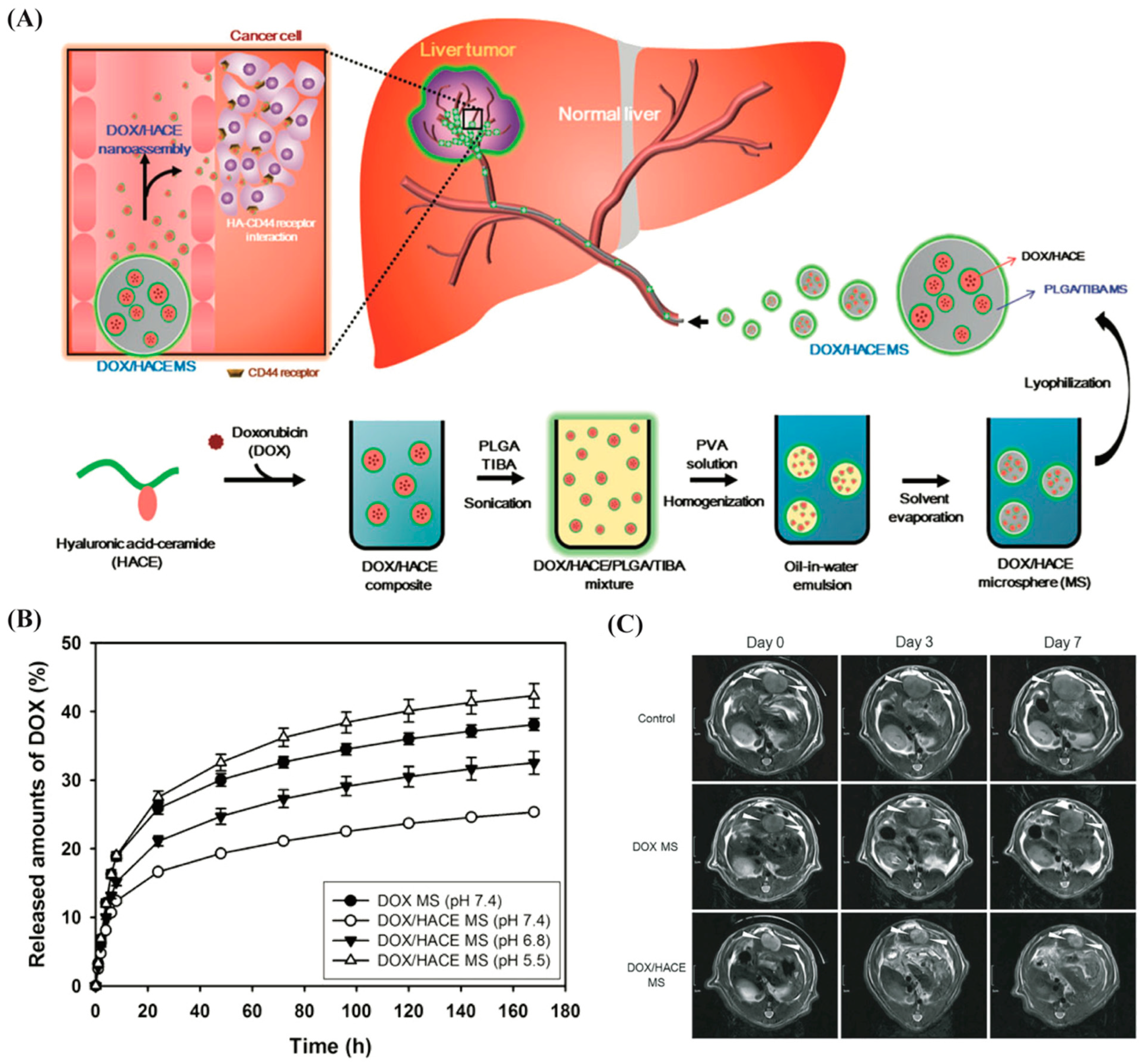
- Lee, S.Y.; Choi, J.W.; Lee, J.Y.; Kim, D.D.; Kim, H.C.; Cho, H.J. Hyaluronic acid/doxorubicin nanoassembly-releasing microspheres for the transarterial chemoembolization of a liver tumor. Drug Deliv. 2018, 25, 1472–1483. [Google Scholar] [CrossRef]
- Rosen, R.J.; Contractor, S. The use of cyanoacrylate adhesives in the management of congenital vascular malformations. Semin. Intervent. Radiol. 2004, 21, 59–66. [Google Scholar] [CrossRef]
- Razavi, M.K.; Murphy, K. Embolization of bronchial arteries with N-Butyl cyanoacrylate for management of massive hemoptysis: A technical review. Tech. Vasc. Interv. Radiol. 2007, 10, 276–282. [Google Scholar] [CrossRef]
- Yonemitsu, T.; Kawai, N.; Sato, M.; Sonomura, T.; Takasaka, I.; Nakai, M.; Minamiguchi, H.; Sahara, S.; Iwasaki, Y.; Naka, T.; et al. Comparison of hemostatic durability between N-butyl cyanoacrylate and gelatin sponge particles in transcatheter arterial embolization for acute arterial hemorrhage in a coagulopathic condition in a swine model. Cardiovasc. Intervent. Radiol. 2010, 33, 1192–1197. [Google Scholar] [CrossRef]
- Yonemitsu, T.; Kawai, N.; Sato, M.; Tanihata, H.; Takasaka, I.; Nakai, M.; Minamiguchi, H.; Sahara, S.; Iwasaki, Y.; Shima, Y.; et al. Evaluation of transcatheter arterial embolization with gelatin sponge particles, microcoils, and N-butyl cyanoacrylate for acute arterial bleeding in a coagulopathic condition. J. Vasc. Interv. Radiol. 2009, 20, 1176–1187. [Google Scholar] [CrossRef] [PubMed]
- Niimi, Y.; Berenstein, A.; Setton, A. Complications and their management during NBCA embolization of craniospinal lesions. Interv. Neuroradiol. 2003, 9, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Moohan, J.; Stewart, S.A.; Espinosa, E.; Rosal, A.; Rodríguez, A.; Larrañeta, E.; Donnelly, R.F.; Domínguez-Robles, J. Cellulose nanofibers and other biopolymers for biomedical applications. A review. Appl. Sci. 2020, 10, 65. [Google Scholar] [CrossRef]
- Lamin, S.; Chew, H.S.; Chavda, S.; Thomas, A.; Piano, M.; Quilici, L.; Pero, G.; Holtmannspolter, M.; Cronqvist, M.E.; Casasco, A.; et al. Embolization of intracranial dural arteriovenous fistulas using PHIL liquid embolic agent in 26 patients: A multicenter study. Am. J. Neuroradiol. 2017, 38, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Samaniego, E.A.; Kalousek, V.; Abdo, G.; Ortega-Gutierrez, S. Preliminary experience with Precipitating Hydrophobic Injectable Liquid (PHIL) in treating cerebral AVMs. J. Neurointerv. Surg. 2016, 8, 1253–1255. [Google Scholar] [CrossRef] [PubMed]
- Weber, W.; Kis, B.; Siekmann, R.; Kuehne, D. Endovascular treatment of intracranial arteriovenous malformations with onyx: Technical aspects. Am. J. Neuroradiol. 2007, 28, 371–377. [Google Scholar]
- Bass, D.I.; Young, C.C.; Sen, R.D.; Levitt, M.R. Transarterial embolization. In Cerebral Dural Arteriovenous Fistulas; Gross, B.A., Albuquerque, F.C., Jankowitz, B.T., McDougall, C.G., Eds.; Academic Press: Cambridge, MA, USA, 2021; pp. 45–62. [Google Scholar]
- Né, R.; Chevallier, O.; Falvo, N.; Facy, O.; Berthod, P.E.; Galland, C.; Gehin, S.; Midulla, M.; Loffroy, R. Embolization with ethylene vinyl alcohol copolymer (Onyx®) for peripheral hemostatic and non-hemostatic applications: A feasibility and safety study. Quant. Imaging Med. Surg. 2018, 8, 280–290. [Google Scholar] [CrossRef]
- Natarajan, S.K.; Born, D.; Ghodke, B.; Britz, G.W.; Sekhar, L.N. Histopathological changes in brain arteriovenous malformations after embolization using Onyx or N-butyl cyanoacrylate: Laboratory investigation. J. Neurosurg. 2009, 111, 105–113. [Google Scholar] [CrossRef]
- Won, Y.; Lee, S.L.; Kim, Y.; Ku, Y.M. Clinical efficacy of transcatheter embolization of visceral artery pseudoaneurysms using N-butyl cyanoacrylate (NBCA). Diagn. Interv. Imaging 2015, 96, 563–569. [Google Scholar] [CrossRef]
- Jahan, R.; Murayama, Y.; Gobin, Y.P.; Duckwiler, G.R.; Vinters, H.V.; Viñuela, F. Embolization of arteriovenous malformations with Onyx: Clinicopathological experience in 23 patients. Neurosurgery 2001, 48, 984–997. [Google Scholar] [CrossRef]
- Koçer, N.; Hanımoğlu, H.; Batur, Ş.; Kandemirli, S.G.; Kızılkılıç, O.; Sanus, Z.; Öz, B.; Işlak, C.; Kaynar, M.Y. Preliminary experience with precipitating hydrophobic injectable liquid in brain arteriovenous malformations. Diagn. Interv. Radiol. 2016, 22, 184–189. [Google Scholar] [CrossRef]
- Lee, B.H.; West, B.; McLemore, R.; Pauken, C.; Vernon, B.L. In-situ injectable physically and chemically gelling NIPAAm-based copolymer system for embolization. Biomacromolecules 2006, 7, 2059–2064. [Google Scholar] [CrossRef] [PubMed]
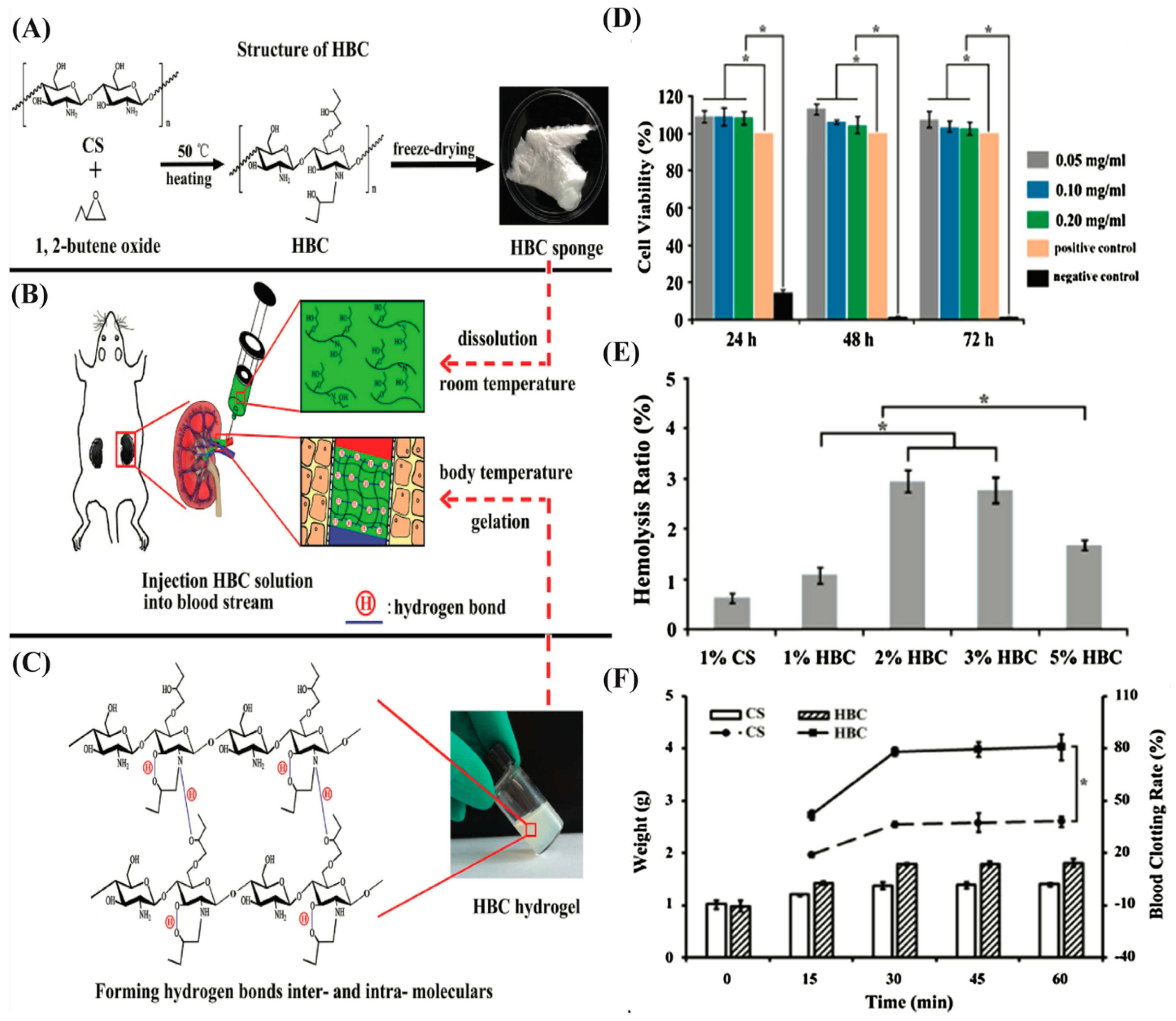
- Sun, G.; Feng, C.; Jiang, C.; Zhang, T.; Bao, Z.; Zuo, Y.; Kong, M.; Cheng, X.; Liu, Y.; Chen, X. Thermo-responsive hydroxybutyl chitosan hydrogel as artery intervention embolic agent for hemorrhage control. Int. J. Biol. Macromol. 2017, 105, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Liu, W.; Ye, G.; Zhang, B.; Zhu, D.; Yao, K.; Liu, Z.; Sheng, X. Thermosensitive N-isopropylacrylamide–N–propylacrylamide-vinyl pyrrolidone terpolymers: Synthesis, characterization and preliminary application as embolic agents. Biomaterials 2005, 26, 7002–7011. [Google Scholar] [CrossRef] [PubMed]
- Coutu, J.M.; Fatimi, A.; Berrahmoune, S.; Soulez, G.; Lerouge, S. A new radiopaque embolizing agent for the treatment of endoleaks after endovascular repair: Influence of contrast agent on chitosan thermogel properties. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101B, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xu, N.; Luo, Q.; Li, Y.; Sun, L.; Wang, H.; Xu, K.; Wang, B.; Zhen, Y. In vivo assessment of chitosan/β-glycerophosphate as a new liquid embolic agent. Interv. Neuroradiol. 2011, 17, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Fatimi, A.; Zehtabi, F.; Lerouge, S. Optimization and characterization of injectable chitosan-iodixanol-based hydrogels for the embolization of blood vessels. J. Biomed. Mater. Res. Part B Appl. Biomater. 2016, 104, 1551–1562. [Google Scholar] [CrossRef]
- Raymond, J.; Metcalfe, A.; Salazkin, I.; Schwarz, A. Temporary vascular occlusion with poloxamer 407. Biomaterials 2004, 25, 3983–3989. [Google Scholar] [CrossRef]
- Huang, L.; Shen, M.; Li, R.; Zhang, X.; Sun, Y.; Gao, P.; Fu, H.; Liu, H.; He, Y.; Du, Y.; et al. Thermo-sensitive composite hydrogels based on poloxamer 407 and alginate and their therapeutic effect in embolization in rabbit VX2 liver tumors. Oncotarget 2016, 7, 73280–73291. [Google Scholar] [CrossRef]
- Dimatteo, R.; Darling, N.J.; Segura, T. In situ forming injectable hydrogels for drug delivery and wound repair. Adv. Drug Deliv. Rev. 2018, 127, 167–184. [Google Scholar] [CrossRef]
- Askari, E.; Seyfoori, A.; Amereh, M.; Gharaie, S.S.; Ghazali, H.S.; Ghazali, Z.S.; Khunjush, B.; Akbari, M. Stimuli-responsive hydrogels for local post-surgical drug delivery. Gels 2020, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Q.V.; Lee, M.S.; Lym, J.S.; Kim, Y.I.; Jae, H.J.; Lee, D.S. pH-Sensitive sulfamethazine-based hydrogels as potential embolic agents for transcatheter vascular embolization. J. Mater. Chem. B 2016, 4, 6524–6533. [Google Scholar] [CrossRef] [PubMed]
- Lym, J.S.; Nguyen, Q.V.; Ahn, D.W.; Huynh, C.T.; Jae, H.J.; Kim, Y.I.; Lee, D.S. Sulfamethazine-based pH-sensitive hydrogels with potential application for transcatheter arterial chemoembolization therapy. Acta Biomater. 2016, 41, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Q.V.; Lym, J.S.; Huynh, C.T.; Kim, B.S.; Jae, H.J.; Kim, Y.I.; Lee, D.S. A novel sulfamethazine-based pH-sensitive copolymer for injectable radiopaque embolic hydrogels with potential application in hepatocellular carcinoma therapy. Polym. Chem. 2016, 7, 5805–5818. [Google Scholar] [CrossRef]
- Lu, D.; Wang, J.; Li, Y.; Zhang, Y.; Yu, L.; Xu, T.; Guo, H.; Zhang, Y.; Wang, X.; Wang, X.; et al. Tumor noninvasive and target embolization therapy platform by intravenous injection based on acidic microenvironment-responsive hyperbranched poly (amino acid)s. ACS Cent. Sci. 2020, 6, 1977–1986. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Li, Y.; Chen, S.; Fu, Y.-n.; Wang, S.; Li, G.; Tao, L.; Wei, Y.; Wang, X.; Liang, J.F. Dynamic agent of an injectable and self-healing drug-loaded hydrogel for embolization therapy. Colloids Surf. B Biointerfaces 2018, 172, 601–607. [Google Scholar] [CrossRef]
- Loebel, C.; Rodell, C.B.; Chen, M.H.; Burdick, J.A. Shear-thinning and self-healing hydrogels as injectable therapeutics and for 3D-printing. Nat. Protoc. 2017, 12, 1521–1541. [Google Scholar] [CrossRef]
- Gaharwar, A.K.; Avery, R.K.; Assmann, A.; Paul, A.; McKinley, G.H.; Khademhosseini, A.; Olsen, B.D. Shear-thinning nanocomposite hydrogels for the treatment of hemorrhage. ACS Nano 2014, 8, 9833–9842. [Google Scholar] [CrossRef]
- Avery, R.K.; Albadawi, H.; Akbari, M.; Zhang, Y.S.; Duggan, M.J.; Sahani, D.V.; Olsen, B.D.; Khademhosseini, A.; Oklu, R. An injectable shear-thinning biomaterial for endovascular embolization. Sci. Transl. Med. 2016, 8, 365ra156. [Google Scholar] [CrossRef]
- Riley, C.M.; McLemore, R.; Preul, M.C.; Vernon, B.L. Gelling process differences in reverse emulsion, in situ gelling polymeric materials for intracranial aneurysm embolization, formulated with injectable contrast agents. J. Biomed. Mater. Res. Part B Appl. Biomater. 2011, 96, 47–56. [Google Scholar] [CrossRef]
- Brennecka, C.R.; Preul, M.C.; Vernon, B.L. In vitro delivery, cytotoxicity, swelling, and degradation behavior of a liquid-to-solid gelling polymer system for cerebral aneurysm embolization. J. Biomed. Mater. Res. Part B Appl. Biomater. 2012, 100, 1298–1309. [Google Scholar] [CrossRef] [PubMed]
- Huynh, C.T.; Nguyen, Q.V.; Lym, J.S.; Kim, B.S.; Huynh, D.P.; Jae, H.J.; Kim, Y.I.; Lee, D.S. Intraarterial gelation of injectable cationic pH/temperature-sensitive radiopaque embolic hydrogels in a rabbit hepatic tumor model and their potential application for liver cancer treatment. RSC Adv. 2016, 6, 47687–47697. [Google Scholar] [CrossRef]
- Aldenhoff, Y.B.J.; Kruft, M.A.B.; Paul Pijpers, A.; Van Der Veen, F.H.; Bulstra, S.K.; Kuijer, R.; Koole, L.H. Stability of radiopaque iodine-containing biomaterials. Biomaterials 2002, 23, 881–886. [Google Scholar] [CrossRef]
- Sharma, K.V.; Dreher, M.R.; Tang, Y.; Pritchard, W.; Chiesa, O.A.; Karanian, J.; Peregoy, J.; Orandi, B.; Woods, D.; Donahue, D.; et al. Development of “imageable” beads for transcatheter embolotherapy. J. Vasc. Interv. Radiol. 2010, 21, 865–876. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Zheng, C.; Wang, Q.; Fang, J.; Zhou, G.; Zhao, H.; Yang, Y.; Xu, H.; Feng, G.; Yang, X. Permanent and peripheral embolization: Temperature-sensitive p (N-Isopropylacrylamide-co-butyl methylacrylate) nanogel as a novel blood-vessel-embolic material in the interventional therapy of liver tumors. Adv. Funct. Mater. 2011, 21, 2035–2042. [Google Scholar] [CrossRef]
- Ma, Y.; Wan, J.; Qian, K.; Geng, S.; He, N.; Zhou, G.; Zhao, Y.; Yang, X. The studies on highly concentrated complex dispersions of gold nanoparticles and temperature-sensitive nanogels and their application as new blood-vessel-embolic materials with high-resolution angiography. J. Mater. Chem. B 2014, 2, 6044–6053. [Google Scholar] [CrossRef]
- Horák, D.; Metalová, M.; Švec, F.; Drobník, J.; Kálal, J.; Borovička, M.; Adamyan, A.A.; Voronkova, O.S.; Gumargalieva, K.Z. Hydrogels in endovascular embolization. III. Radiopaque spherical particles, their preparation and properties. Biomaterials 1987, 8, 142–145. [Google Scholar] [CrossRef]
- Levy, E.B.; Krishnasamy, V.P.; Lewis, A.L.; Willis, S.; Macfarlane, C.; Anderson, V.; van der Bom, I.M.J.; Radaelli, A.; Dreher, M.R.; Sharma, K.V.; et al. First human experience with directly image-able iodinated embolization microbeads. Cardiovasc. Intervent. Radiol. 2016, 39, 1177–1186. [Google Scholar] [CrossRef]
- Aliberti, C.; Carandina, R.; Sarti, D.; Pizzirani, E.; Ramondo, G.; Cillo, U.; Guadagni, S.; Fiorentini, G. Transarterial chemoembolization with DC Bead LUMITM radiopaque beads for primary liver cancer treatment: Preliminary experience. Future Oncol. 2017, 13, 2243–2252. [Google Scholar] [CrossRef]
- Fan, L.; Duan, M.; Xie, Z.; Pan, K.; Wang, X.; Sun, X.; Wang, Q.; Rao, W.; Liu, J. Injectable and radiopaque liquid metal/calcium alginate hydrogels for endovascular embolization and tumor embolotherapy. Small 2020, 16, 1903421. [Google Scholar] [CrossRef]
- Liang, S.; Wang, Z.; Zhou, Z.; Liang, G.; Zhang, Y. Polymeric carbon nitride-based materials: Rising stars in bioimaging. Biosens. Bioelectron. 2022, 211, 114370. [Google Scholar] [CrossRef] [PubMed]
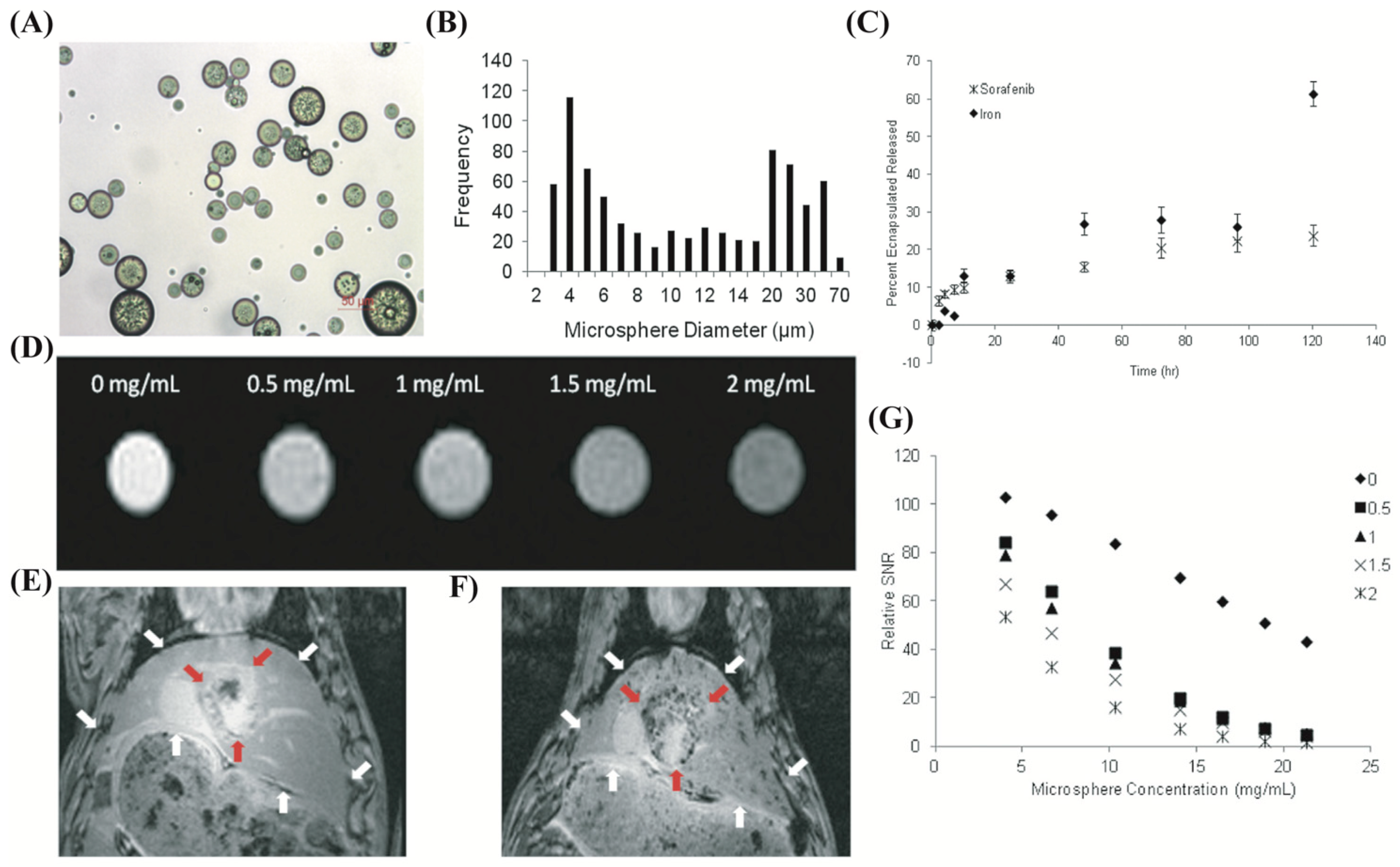
- Chen, J.; White, S.B.; Harris, K.R.; Li, W.; Yap, J.W.T.; Kim, D.H.; Lewandowski, R.J.; Shea, L.D.; Larson, A.C. Poly (lactide-co-glycolide) microspheres for MRI-monitored delivery of sorafenib in a rabbit VX2 model. Biomaterials 2015, 61, 299–306. [Google Scholar] [CrossRef]
- Thanoo, B.C.; Sunny, M.C.; Jayakrishnan, A. Preparation and properties of barium sulphate and methyl iothalamate loaded poly (vinyl alcohol) microspheres as radiopaque particulate emboli. J. Appl. Biomater. 1991, 2, 67–72. [Google Scholar] [CrossRef]
- Horák, D.; Červinka, M.; Půža, V. Radiopaque poly (2-hydroxyethyl methacrylate) particles containing silver iodide complexes tested on cell culture. Biomaterials 1998, 19, 1303–1307. [Google Scholar] [CrossRef]
- Wang, Q.; Qian, K.; Liu, S.; Yang, Y.; Liang, B.; Zheng, C.; Yang, X.; Xu, H.; Shen, A.Q. X-ray visible and uniform alginate microspheres loaded with in situ synthesized BaSO4 nanoparticles for in vivo transcatheter arterial embolization. Biomacromolecules 2015, 16, 1240–1246. [Google Scholar] [CrossRef]
- Thanoo, B.C.; Sunny, M.C.; Jayakrisnnan, A. Tantalum-loaded polyurethane microspheres for particulate embolization: Preparation and properties. Biomaterials 1991, 12, 525–528. [Google Scholar] [CrossRef]
- Adibi, A.; Sen, A.; Mitha, A.P. Cell Therapy for Intracranial Aneurysms: A Review. World Neurosurg. 2016, 86, 390–398. [Google Scholar] [CrossRef]
- Rocca, A.; Tafuri, D.; Paccone, M.; Giuliani, A.; Zamboli, A.G.I.; Surfaro, G.; Paccone, A.; Compagna, R.; Amato, M.; Serra, R.; et al. Cell based therapeutic approach in vascular surgery: Application and review. Open Med. 2017, 12, 308–322. [Google Scholar] [CrossRef] [PubMed]
- Sagaradze, G.D.; Basalova, N.A.; Efimenko, A.Y.; Tkachuk, V.A. Mesenchymal stromal cells as critical contributors to tissue regeneration. Front. Cell Dev. Biol. 2020, 8, 576176. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Sun, Q.; Li, Q.; Kawazoe, N.; Chen, G. Functional hydrogels with tunable structures and properties for tissue engineering applications. Front. Chem. 2018, 6, 499. [Google Scholar] [CrossRef] [PubMed]
- Foster, A.A.; Marquardt, L.M.; Heilshorn, S.C. The diverse roles of hydrogel mechanics in injectable stem cell transplantation. Curr. Opin. Chem. Eng. 2017, 15, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Aamodt, J.M.; Grainger, D.W. Extracellular matrix-based biomaterial scaffolds and the host response. Biomaterials 2016, 86, 68–82. [Google Scholar] [CrossRef] [PubMed]
- Loh, Q.L.; Choong, C. Three-dimensional scaffolds for tissue engineering applications: Role of porosity and pore size. Tissue Eng. Part B Rev. 2013, 19, 485–502. [Google Scholar] [CrossRef]
- Griffin, D.R.; Weaver, W.M.; Scumpia, P.O.; Di Carlo, D.; Segura, T. Accelerated wound healing by injectable microporous gel scaffolds assembled from annealed building blocks. Nat. Mater. 2015, 14, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Grosskopf, A.K.; Roth, G.A.; Smith, A.A.A.; Gale, E.C.; Hernandez, H.L.; Appel, E.A. Injectable supramolecular polymer–nanoparticle hydrogels enhance human mesenchymal stem cell delivery. Bioeng. Transl. Med. 2020, 5, e10147. [Google Scholar] [CrossRef]
- Kusuma, G.D.; Carthew, J.; Lim, R.; Frith, J.E. Effect of the microenvironment on mesenchymal stem cell paracrine signaling: Opportunities to engineer the therapeutic effect. Stem Cells Dev. 2017, 26, 617–631. [Google Scholar] [CrossRef]
- Marx, W.F.; Cloft, H.J.; Helm, G.A.; Short, J.G.; Do, H.M.; Jensen, M.E.; Kallmes, D.F. Endovascular treatment of experimental aneurysms by use of biologically modified embolic devices: Coil-mediated intraaneurysmal delivery of fibroblast tissue allografts. Am. J. Neuroradiol. 2001, 22, 323–333. [Google Scholar] [PubMed]
- Rouchaud, A.; Brinjikji, W.; Dai, D.; Ding, Y.H.; Gunderson, T.; Schroeder, D.; Spelle, L.; Kallmes, D.F.; Kadirvel, R. Autologous adipose-derived mesenchymal stem cells improve healing of coiled experimental saccular aneurysms: An angiographic and histopathological study. J. Neurointerv. Surg. 2018, 10, 60–65. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rana, M.M.; Melancon, M.P. Emerging Polymer Materials in Trackable Endovascular Embolization and Cell Delivery: From Hype to Hope. Biomimetics 2022, 7, 77. https://doi.org/10.3390/biomimetics7020077
Rana MM, Melancon MP. Emerging Polymer Materials in Trackable Endovascular Embolization and Cell Delivery: From Hype to Hope. Biomimetics. 2022; 7(2):77. https://doi.org/10.3390/biomimetics7020077
Chicago/Turabian StyleRana, Md Mohosin, and Marites P. Melancon. 2022. "Emerging Polymer Materials in Trackable Endovascular Embolization and Cell Delivery: From Hype to Hope" Biomimetics 7, no. 2: 77. https://doi.org/10.3390/biomimetics7020077
APA StyleRana, M. M., & Melancon, M. P. (2022). Emerging Polymer Materials in Trackable Endovascular Embolization and Cell Delivery: From Hype to Hope. Biomimetics, 7(2), 77. https://doi.org/10.3390/biomimetics7020077