
Pulmonary Vein Isolation in Obese Compared to Non-Obese Patients: Real-Life Experience from a Large Tertiary Center

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Methods
3. Results
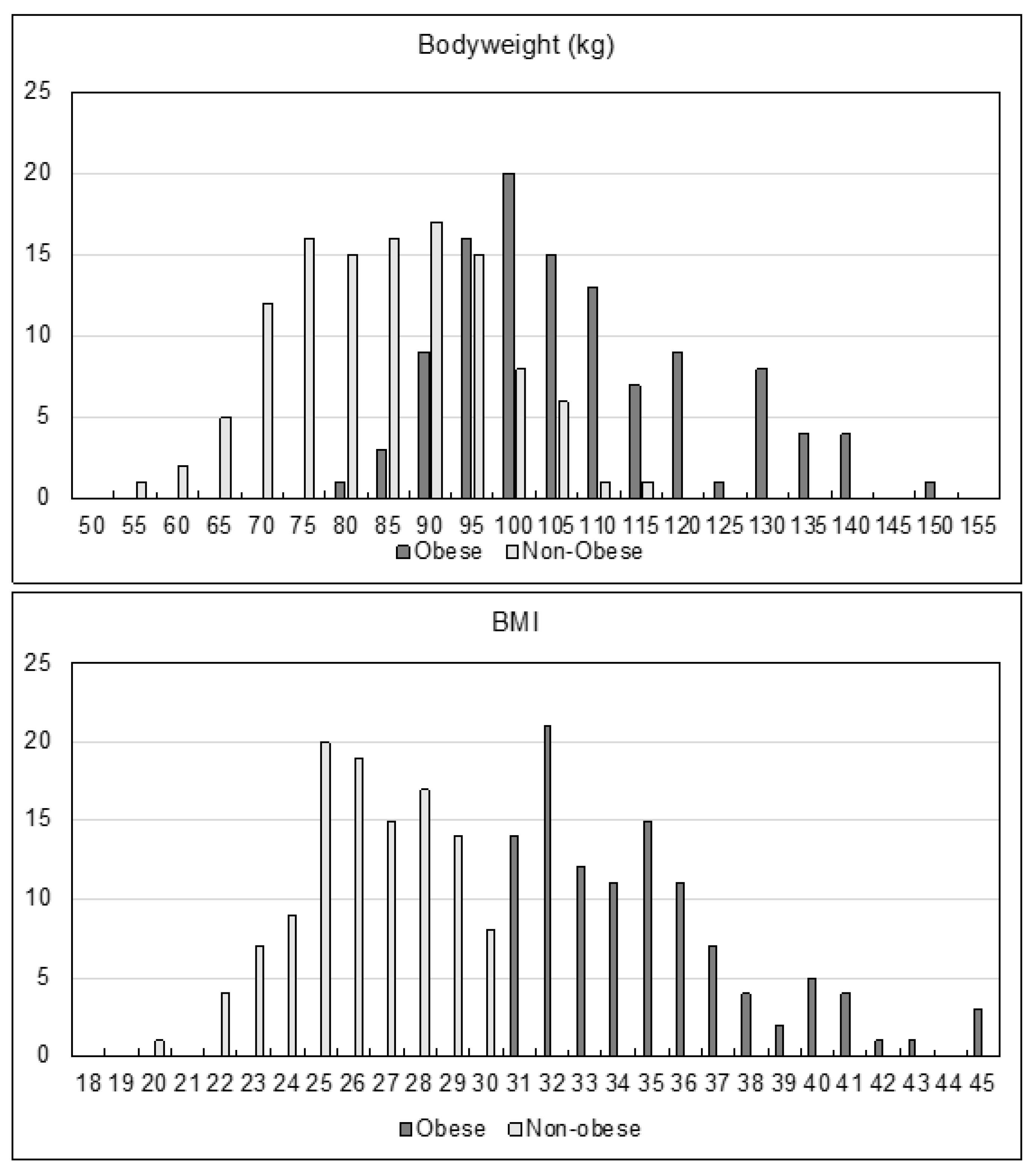
3.1. Patient Characteristics
3.2. Intrahospital Outcome
3.3. Long-Term Follow-Up
3.4. Risk Factors for AF Recurrence
4. Discussion
4.1. AF Recurrence Rates after PVI
4.2. Ablation Safety
4.3. Body Weight Development Following PVI
4.4. Risk Factors in Obese Patients
4.5. Antiarrhythmic Drugs in Obese Patients
4.6. Radiation and Operator Safety
5. Clinical Implications and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gaziano, J.M. Fifth phase of the epidemiologic transition: The age of obesity and inactivity. JAMA 2010, 303, 275–276. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Watkins, C.L. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Javed, S.; Gupta, D.; Lip, G.Y.H. Obesity and atrial fibrillation: Making inroads through fat. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Pandey, A.; Lau, D.H.; Alpert, M.A.; Sanders, P. Obesity and Atrial Fibrillation Prevalence, Pathogenesis, and Prognosis: Effects of Weight Loss and Exercise. J. Am. Coll. Cardiol. 2017, 70, 2022–2035. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. New Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.X.; Sullivan, T.; Sun, M.T.; Mahajan, R.; Pathak, R.K.; Middeldorp, M.; Sanders, P. Obesity and the Risk of Incident, Post-Operative, and Post-Ablation Atrial Fibrillation: A Meta-Analysis of 626,603 Individuals in 51 Studies. JACC Clin. Electrophysiol. 2015, 1, 139–152. [Google Scholar] [CrossRef] [PubMed]
- De Maat, G.E.; Mulder, B.; Berretty, W.L.; Al-Jazairi, M.I.; Tan, Y.E.; Wiesfeld, A.C.; Blaauw, Y. Obesity is associated with impaired long-term success of pulmonary vein isolation: A plea for risk factor management before ablation. Open Heart 2018, 5, e000771. [Google Scholar] [CrossRef] [PubMed]
- Sivasambu, B.; Balouch, M.A.; Zghaib, T.; Bajwa, R.J.; Chrispin, J.; Berger, R.D.; Ashikaga, H.; Nazarian, S.; Marine, J.E.; Calkins, H.; et al. Increased rates of atrial fibrillation recurrence following pulmonary vein isolation in overweight and obese patients. J. Cardiovasc. Electrophysiol. 2017, 29, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Winkle, R.A.; Mead, R.H.; Engel, G.; Kong, M.H.; Fleming, W.; Salcedo, J.; Patrawala, R.A. Impact of obesity on atrial fibrillation ablation: Patient characteristics, long-term outcomes, and complications. Heart Rhythm. 2017, 14, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Jongnarangsin, K.; Chugh, A.; Good, E.; Mukerji, S.; Dey, S.; Crawford, T.; Oral, H. Body mass index, obstructive sleep apnea, and outcomes of catheter ablation of atrial fibrillation. J. Cardiovasc. Electrophysiol. 2008, 19, 668–672. [Google Scholar] [CrossRef]
- Weinmann, K.; Bothner, C.; Rattka, M.; Aktolga, D.; Teumer, Y.; Rottbauer, W.; Pott, A. Pulmonary vein isolation with the cryoballoon in obese atrial fibrillation patients—Does weight have an impact on procedural parameters and clinical outcome? Int. J. Cardiol. 2020, 316, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Malaspina, D.; Brasca, F.; Iacopino, S.; Arena, G.; Molon, G.; Pieragnoli, P.; Tondo, C.; Manfrin, M.; Rovaris, G.; Verlato, R.; et al. Cryoablation for pulmonary veins isolation in obese patients with atrial fibrillation compared to nonobese patients. Pacing Clin. Electrophysiol. 2020, 44, 306–317. [Google Scholar] [CrossRef] [PubMed]
- Pathak, R.K.; Middeldorp, M.E.; Lau, D.H.; Mehta, A.B.; Mahajan, R.; Twomey, D.; Sanders, P. Aggressive risk factor reduction study for atrial fibrillation and implications for the outcome of ablation: The ARREST-AF cohort study. J. Am. Coll. Cardiol. 2014, 64, 2222–2231. [Google Scholar] [CrossRef] [PubMed]
- Ector, J.; Dragusin, O.; Adriaenssens, B.; Huybrechts, W.; Willems, R.; Ector, H.; Heidbüchel, H. Obesity Is a Major Determinant of Radiation Dose in Patients Undergoing Pulmonary Vein Isolation for Atrial Fibrillation. J. Am. Coll. Cardiol. 2007, 50, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, N.; Sabir, A.; Kubo, T.; Lin, P.-J.P.; Clouse, M.E.; Hatabu, H. Correlation Between Image Noise and Body Weight in Coronary CTA with 16-row MDCT. Acad. Radiol. 2006, 13, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Cha, Y.-M.; Friedman, P.A.; Asirvatham, S.J.; Shen, W.-K.; Munger, T.M.; Rea, R.F.; Brady, P.A.; Jahangir, A.; Monahan, K.H.; Hodge, D.O.; et al. Catheter Ablation for Atrial Fibrillation in Patients With Obesity. Circulation 2008, 117, 2583–2590. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Baseline Characteristics | |||
|---|---|---|---|
| Obese (n = 111) | Non-Obese (n = 115) | p-Value | |
| Age | 61.0 ± 9 | 59.3 ± 12.9 | 0.071 |
| Female sex | 47 (42.3%) | 38 (33%) | 0.17 |
| Bodyweight (kg) | 106.7 ± 14.7 | 82.8 ± 11.9 | 0.01 |
| BMI (kg/m2) | 34.34 ± 3.4 | 25.9 ± 2.2 | 0.01 |
| Structural heart disease | 43 (38.7%) | 26 (22.6%) | 0.01 |
| Hypertension | 94 (84.7%) | 58 (50.4%) | 0.01 |
| Diabetes mellitus | 24 (21.6%) | 8 (7%) | 0.002 |
| OSAS | 17 (15.3%) | 4 (3.5%) | 0.002 |
| Coronary artery disease | 25 (22.5%) | 14 (12.2%) | 0.052 |
| LVEF | 57.5 ± 6.8 | 59 ± 5.3 | 0.085 |
| Smoking | 35 (31.5%) | 20 (17.4%) | 0.02 |
| Thyroid disorder | 22 (19.8%) | 25 (21.7%) | 0.746 |
| Persistent AF | 61 (55%) | 57 (49.6%) | 0.428 |
| Antiarrhythmic drugs before PVI | 60 (54.1%) | 46 (40%) | 0.045 |
| Previous cardioversion | 65 (58.6%) | 48 (41.7%) | 0.016 |
| LA-dilatation | 64 (57.5%) | 36 (31.3%) | 0.000093 |
| Repeat ablation | 24 (21.6%) | 24 (20.9%) | 0.872 |
| Procedural and Intrahospital Characteristics | |||
|---|---|---|---|
| Obese (n = 111) | Non-Obese (n = 115) | p-Value | |
| RF-ablation | 25 (22.5%) | 18 (15.7%) | 0.477 |
| Cryoballoon | 56 (50.5%) | 67 (58.3%) | 0.23 |
| PVAC | 30 (27%) | 30 (26.1%) | 0.881 |
| Repeat ablation | 24 (21.6%) | 24 (20.9%) | 0.872 |
| EP duration (min) | 117.4 ± 47.7 | 108.5 ± 43.9 | 0.146 |
| Impulses | 10.3 ± 11.2 | 10.5 ± 8.2 | 0.891 |
| Flouroscopy time (min) | 18.3 ± 7.9 | 16.1 ± 7.8 | 0.04 |
| DAP-Value (cGy/cm2) | 2360.83 ± 1759.6 | 989.75 ± 756.2 | 0 |
| Complete isolation | 106 (95.5%) | 112 (97.4%) | 0.493 |
| Death | 0 | 0 | 1 |
| Pericardial effusion | 3 (2.7%) | 6 (5.2%) | 0.5 |
| Pericardial tamponade | 1 (0.9%) | 1 (0.9%) | 1 |
| Embolism | 0 | 0 | 1 |
| Phrenic palsy | 2 (1.8%) | 1 (0.9%) | 0.617 |
| Femoral bleeding | 5 (4.5%) | 2 (1.7%) | 0.276 |
| Intrahospital AF recurrence | 19 (17.1%) | 17 (14.8%) | 0.717 |
| Antiarrhythmic drugs after PVI | 88 (79.3%) | 73 (63.5%) | 0.012 |
| Hospital stay (nights) | 3.05 ± 1.77 | 2.77 ± 1.39 | 0.199 |
| Intraprocedural Details | ||||
|---|---|---|---|---|
| Obese | ||||
| n | EP Duration (min) | Flouroscopy Time (min) | DAP-Value (cGy/cm2) | |
| RF-ablation | 25 | 175.2 ± 52.71 | 24.16 ± 21.95 | 3327.67 ± 1800.14 |
| PVAC | 30 | 109.47 ± 25.3 | 16.04 ± 5.49 | 2148.4 ± 1595.73 |
| Cryoballoon | 56 | 95.81 ± 30.72 | 15.85 ± 5.79 | 2026.94 ± 1708.85 |
| Non-obese | ||||
| n | EP Duration (min) | Flouroscopy Time (min) | DAP-Value (cGy/cm2) | |
| RF-ablation | 18 | 169.44 ± 46.49 | 22.21 ± 9.79 | 907.75 ± 673.83 |
| PVAC | 30 | 118.63 ± 40.81 | 17.67 ± 9.71 | 1261.73 ± 935.13 |
| Cryoballoon | 67 | 87.57 ± 23.3 | 13.78 ± 4.83 | 901.14 ± 677.71 |
| Long Term Follow-Up | |||
|---|---|---|---|
| Obese (n = 79) | Non-Obese (n = 87) | p-Value | |
| AF recurrence | 31 (39.2%) | 38 (43.7%) | 0.637 |
| Stroke | 1 (1.3%) | 1 (1.1%) | 1 |
| Confidence with ablation | 69 (87.3%) | 82 (94.2%) | 0.175 |
| Electrical cardioversion during follow-up | 6 (7.6%) | 3 (3.4%) | 0.312 |
| Repeat ablation during follow-up | 18 (22.8%) | 23 (26.4%) | 0.595 |
| Actual bodyweight | 100 ± 16,2 | 83.9 ± 11.9 | <0.001 |
| Bodyweight compared to procedure date | –4.8 ± 8.8 | 0.9 ± 6.3 | <0.001 |
| Riskfactors of AF Recurrence | ||||||
|---|---|---|---|---|---|---|
| All | Obese | Non-Obese | ||||
| Variable | Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value |
| Obesity | –0.117 | 0.474 | ||||
| Bodyweight | 0.002 | 0.726 | −0.002 | 0.749 | 0.004 | 0.755 |
| BMI | –0.003 | 0.871 | 0.017 | 0.535 | –0.029 | 0.508 |
| Female sex | 0.152 | 0.220 | 0.015 | 0.930 | 0.192 | 0.480 |
| Age | 0.005 | 0.355 | 0.007 | 0.551 | 0.005 | 0.527 |
| Persistent AF | 0.100 | 0.347 | –0.030 | 0.863 | 0.291 | 0.162 |
| AF duration | –0.005 | 0.574 | –0.015 | 0.439 | –0.008 | 0.571 |
| Previous cardioversion | 0.030 | 0.776 | 0.026 | 0.874 | 0.201 | 0.289 |
| Structural heart disease | –0.097 | 0.397 | 0.021 | 0.892 | 0.014 | 0.951 |
| Hypertension | 0.224 | 0.063 | 0.361 | 0.103 | 0.089 | 0.634 |
| Diabetes mellitus | –0.195 | 0.270 | –0.271 | 0.208 | –0.041 | 0.923 |
| OSAS | 0.044 | 0.768 | 0.115 | 0.624 | –0.358 | 0.366 |
| Coronary artery disease | 0.075 | 0.597 | 0.195 | 0.278 | –0.303 | 0.346 |
| Thyroid disorder | 0.342 | 0.003 | 0.542 | 0.006 | 0.032 | 0.882 |
| Smoking | 0.231 | 0.044 | 0.092 | 0.571 | 0.431 | 0.047 |
| Repeat ablation | –0.055 | 0.663 | –0.205 | 0.291 | 0.071 | 0.754 |
| Cryoballoon | –0.310 | 0.015 | –0.356 | 0.215 | –0.329 | 0.138 |
| RF ablation | 0.177 | 0.323 | 0.270 | 0.299 | 0.110 | 0.748 |
| PVAC | 0.191 | 0.130 | 0.135 | 0.533 | 0.220 | 0.335 |
| AAD before PVI | 0.147 | 0.167 | 0.242 | 0.142 | –0.083 | 0.641 |
| AAD after PVI | 0.073 | 0.518 | 0.325 | 0.142 | –0.011 | 0.948 |
| Intrahospital AF recurrence | 0.287 | 0.013 | 0.340 | 0.062 | 0.231 | 0.255 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolfes, J.; Hoppe, D.; Ellermann, C.; Willy, K.; Rath, B.; Leitz, P.; Güner, F.; Köbe, J.; Lange, P.S.; Eckardt, L.; et al. Pulmonary Vein Isolation in Obese Compared to Non-Obese Patients: Real-Life Experience from a Large Tertiary Center. J. Cardiovasc. Dev. Dis. 2022, 9, 275. https://doi.org/10.3390/jcdd9080275
Wolfes J, Hoppe D, Ellermann C, Willy K, Rath B, Leitz P, Güner F, Köbe J, Lange PS, Eckardt L, et al. Pulmonary Vein Isolation in Obese Compared to Non-Obese Patients: Real-Life Experience from a Large Tertiary Center. Journal of Cardiovascular Development and Disease. 2022; 9(8):275. https://doi.org/10.3390/jcdd9080275
Chicago/Turabian StyleWolfes, Julian, Daniel Hoppe, Christian Ellermann, Kevin Willy, Benjamin Rath, Patrick Leitz, Fatih Güner, Julia Köbe, Philipp S. Lange, Lars Eckardt, and et al. 2022. "Pulmonary Vein Isolation in Obese Compared to Non-Obese Patients: Real-Life Experience from a Large Tertiary Center" Journal of Cardiovascular Development and Disease 9, no. 8: 275. https://doi.org/10.3390/jcdd9080275
APA StyleWolfes, J., Hoppe, D., Ellermann, C., Willy, K., Rath, B., Leitz, P., Güner, F., Köbe, J., Lange, P. S., Eckardt, L., & Frommeyer, G. (2022). Pulmonary Vein Isolation in Obese Compared to Non-Obese Patients: Real-Life Experience from a Large Tertiary Center. Journal of Cardiovascular Development and Disease, 9(8), 275. https://doi.org/10.3390/jcdd9080275