
Efficacy and Safety of a Combined Aerobic, Strength and Flexibility Exercise Training Program in Patients with Implantable Cardiac Devices



 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
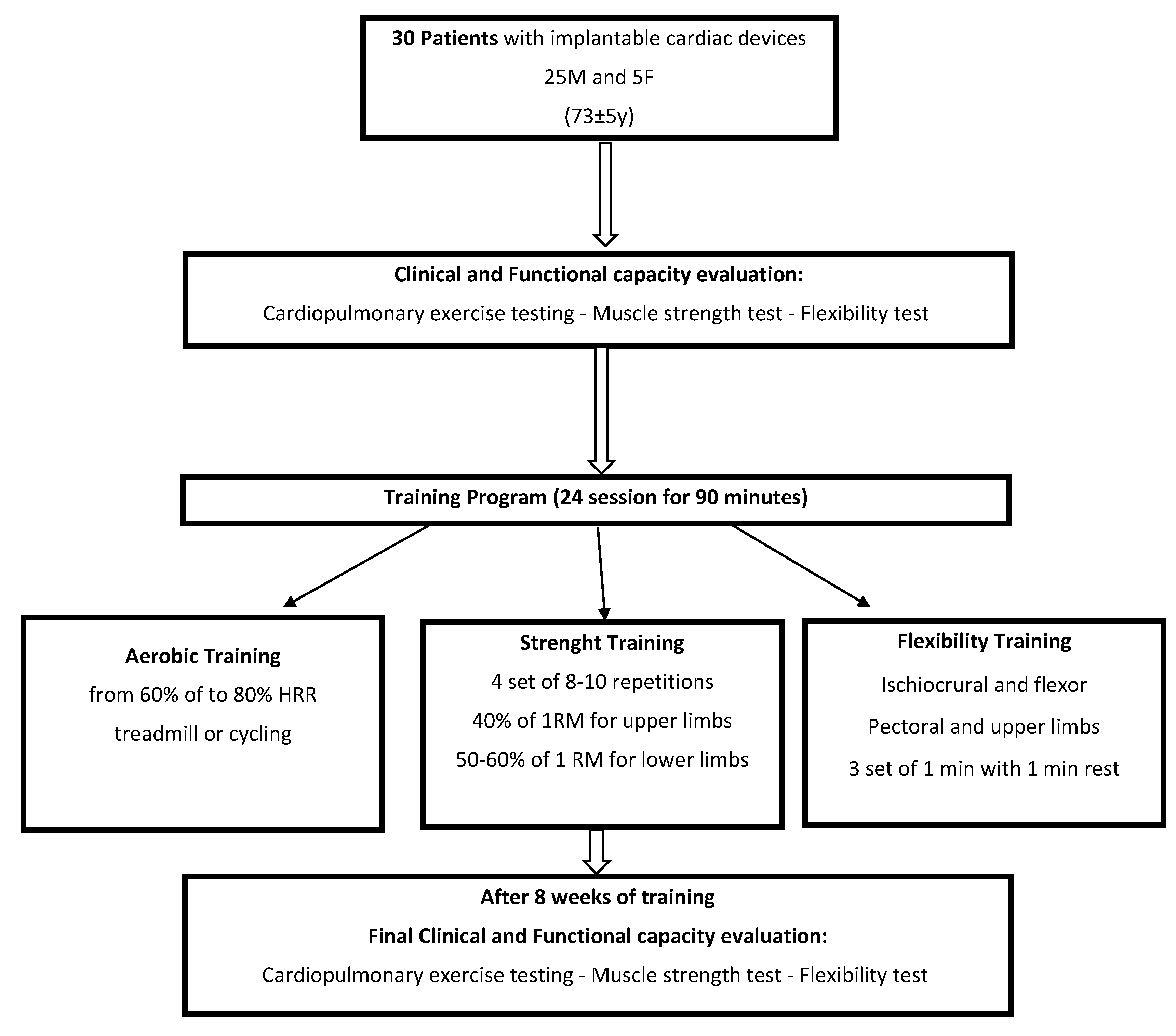
2.1. Study Group
2.2. Cardiovascular Rehabilitation Program
- Phase 1: Clinical and Functional Capacity Evaluation
- Phase 2: Training Program
- Phase 3: Assessment and Outcomes
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations of Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Proclemer, A.; Zecchin, M.; D’Onofrio, A.; Ricci, R.P.; Boriani, G.; Rebellato, L.; Ghidina, M.; Bianco, G.; Bernardelli, E.; Miconi, A.; et al. The Pacemaker and Implantable Cardioverter-Defibrillator Registry of the Italian Association of Arrhythmology and Cardiac Pacing—Annual report 2017. G. Ital. Cardiol. 2019, 20, 136–148. [Google Scholar]
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary Behavior, Exercise, and Cardiovascular Health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef] [PubMed]
- Kaminsky, L.A.; Arena, R.; Ellingsen, Ø.; Harber, M.P.; Myers, J.; Ozemek, C.; Ross, R. Cardiorespiratory fitness and cardiovascular disease—The past, present, and future. Prog. Cardiovasc. Dis. 2019, 62, 86–93. [Google Scholar] [CrossRef]
- Pepera, G.; Bromley, P.D.; Sandercock, G.R.H. A pilot study to investigate the safety of exercise training and testing in cardiac rehabilitation patients. Br. J. Cardiol. 2013, 20, 78. [Google Scholar] [CrossRef]
- Aoyama, D.; Miyazaki, S.; Hasegawa, K.; Nagao, M.; Kakehashi, S.; Mukai, M.; Sekihara, T.; Nodera, M.; Eguchi, T.; Aiki, T.; et al. Cardiac rehabilitation after catheter ablation of atrial fibrillation in patients with left ventricular dysfunction. Heart Vessels 2021, 36, 1542–1550. [Google Scholar] [CrossRef]
- Ambrosetti, M.; Abreu, A.; Corrà, U.; Davos, C.H.; Hansen, D.; Frederix, I.; Iliou, M.C.; Pedretti, R.F.; Schmid, J.-P.; Vigorito, C.; et al. Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2020, 28, 460–495. [Google Scholar] [CrossRef] [PubMed]
- Hansen, D.; Abreu, A.; Ambrosetti, M.; Cornelissen, V.; Gevaert, A.; Kemps, H.; Laukkanen, J.A.; Pedretti, R.; Simonenko, M.; Wilhelm, M.; et al. Exercise intensity assessment and prescription in cardiovascular rehabilitation and beyond: Why and how: A position statement from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2021, 29, 230–245. [Google Scholar] [CrossRef] [PubMed]
- Isaksen, K.; Morken, I.M.; Munk, P.S.; Larsen, A.I. Exercise training and cardiac rehabilitation in patients with implantable cardioverter defibrillators: A review of current literature focusing on safety, effects of exercise training, and the psychological impact of programme participation. Eur. J. Prev. Cardiol. 2012, 19, 804–812. [Google Scholar] [CrossRef]
- Alswyan, A.H.; Liberato, A.C.S.; Dougherty, C.M. A Systematic Review of Exercise Training in Patients with Cardiac Implantable Devices. J. Cardiopulm. Rehabil. Prev. 2018, 38, 70–84. [Google Scholar] [CrossRef]
- Iliou, M.C.; Blanchard, J.C.; Lamar-Tanguy, A.; Cristofini, P.; Ledru, F. Cardiac rehabilitation in patients with pacemakers and implantable cardioverter defibrillators. Monaldi Arch. Chest Dis. 2016, 86, 756. [Google Scholar] [CrossRef]
- Belardinelli, R.; Capestro, F.; Misiani, A.; Scipione, P.; Georgiou, D. Moderate exercise training improves functional capacity, quality of life, and endothelium-dependent vasodilation in chronic heart failure patients with implantable cardioverter defibrillators and cardiac resynchronization therapy. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 818–825. [Google Scholar] [CrossRef]
- Vanhees, L.; Schepers, D.; Heidbüchel, H.; Defoor, J.; Fagard, R. Exercise performance and training in patients with implantable cardioverter-defibrillators and coronary heart disease. Am. J. Cardiol. 2001, 87, 712–715. [Google Scholar] [CrossRef]
- Allison, T.G. Changing medical culture to promote physical activity in secondary prevention of coronary artery disease. Eur. Heart J. 2013, 34, 3245–3247. [Google Scholar] [CrossRef][Green Version]
- Binder, R.K.; Wonisch, M.; Corra, U.; Cohen-Solal, A.; Vanhees, L.; Saner, H.; Schmid, J.-P. Methodological approach to the first and second lactate threshold in incremental cardiopulmonary exercise testing. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Bjarnason-Wehrens, B.; Mayer-Berger, W.; Meister, E.; Baum, K.; Hambrecht, R.; Gielen, S. German Federation for Cardiovascular Prevention and Rehabilitation. Recommendations for resistance exercise in cardiac rehabilitation. Recommendations of the German Federation for Cardiovascular Prevention and Rehabilitation. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 352–361. [Google Scholar] [CrossRef]
- Mazza, A.; Camera, F.; Maestri, A.; Longoni, F.; Patrignani, A.; Gualco, A.; Opasich, C.; Cobelli, F. Elderly patient-centered rehabilitation after cardiac surgery. Monaldi Arch. Chest Dis. 2007, 68, 36–43. [Google Scholar] [CrossRef]
- Steinhaus, D.A.; Lubitz, S.A.; Noseworthy, P.A.; Kramer, D.B. Exercise Interventions in Patients with Implantable Cardioverter-Defibrillators and Cardiac Resynchronization Therapy: A Systematic Review and Meta-Analysis. J. Cardiopulm. Rehabil Prev. 2019, 39, 308–317. [Google Scholar] [CrossRef]
- Merritt, J.L.; McLean, T.J.; Erickson, R.P.; Offord, K.P. Measurement of trunk flexibility in normal subjects: Reproducibility of three clinical methods. Mayo Clin. Proc. 1986, 61, 192–197. [Google Scholar] [CrossRef]
- Piccini, J.P.; Hellkamp, A.S.; Whellan, D.J.; Ellis, S.J.; Keteyian, S.J.; Kraus, W.E.; Hernandez, A.F.; Daubert, J.P.; Piña, L.; O’Connor, C.M. HF-ACTION Investigators. Exercise training and implantable cardioverter-defibrillator shocks in patients with heart failure: Results from HF-ACTION (Heart Failure and A Controlled Trial Investigating Outcomes of Exercise TraiNing). JACC Heart Fail. 2013, 1, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Parashar, A.; Moore, C.; Ngo, C.; Salahuddin, U.; Bhargava, M.; Kumbhani, D.J.; Piccini, J.P.; Fonarow, G.C.; Berry, J.D. Safety and Efficacy of Exercise Training in Patients with an Implantable Cardioverter-Defibrillator: A Meta-Analysis. JACC Clin. Electrophysiol. 2017, 3, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Sandercock, G.R.; Cardoso, F.; Almodhy, M.; Pepera, G. Cardiorespiratory fitness changes in patients receiving comprehensive outpatient cardiac rehabilitation in the UK: A multicentre study. Heart 2013, 99, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Pryzbek, M.; MacDonald, M.; Stratford, P.; Richardson, J.; McQuarrie, A.; McKelvie, R.; Tang, A. Long-Term Enrollment in Cardiac Rehabilitation Benefits of Cardiorespiratory Fitness and Skeletal Muscle Strength in Females with Cardiovascular Disease. Womens Health Rep. 2021, 2, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Stefanakis, M.; Batalik, L.; Papathanasiou, J.; Dipla, L.; Antoniou, V.; Pepera, G. Exercise-based cardiac rehabilitation programs in the era of COVID-19: A critical review. Rev. Cardiovasc. Med. 2021, 22, 1143–1155. [Google Scholar] [CrossRef]
- Perrone, M.A.; Donatucci, B.; Salvati, A.; Gualtieri, P.; De Lorenzo, A.; Romeo, F.; Bernardini, S. Inflammation, oxidative stress and gene expression: The postprandial approach in professional soccer players to reduce the risk of muscle injuries and early atherosclerosis. Med. Sport 2019, 72, 234–243. [Google Scholar] [CrossRef]
- Tutor, A.; Lavie, C.J.; Kachur, S.; Dinshaw, H.; Milani, R.V. Impact of cardiorespiratory fitness on outcomes in cardiac rehabilitation. Prog. Cardiovasc. Dis. 2022, 70, 2–7. [Google Scholar] [CrossRef]
- Guidelines for Exercise Testing and Prescription, 11th edition 2021. The American College of Sports Medicine (ACSM). Available online: https://www.acsm.org/read-research/books (accessed on 25 January 2022).
- Khadanga, S.; Savage, P.D.; Ades, P.A. Resistance Training for Older Adults in Cardiac Rehabilitation. Clin. Geriatr. Med. 2019, 35, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Zhang, X.; Guo, J.; Roberts, C.K.; McKenzie, S.; Wu, W.C.; Liu, S.; Song, Y. Effects of Exercise Training on Cardiorespiratory Fitness and Biomarkers of Cardiometabolic Health: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2015, 4, e002014. [Google Scholar] [CrossRef]
- Williams, M.A.; Haskell, W.L.; Ades, P.A.; Amsterdam, E.A.; Bittner, V.; Franklin, B.A.; Gulanick, M.; Laing, S.T.; Stewart, K.J.; American Heart Association Council on Clinical Cardiology; et al. Resistance exercise in individuals with and without cardiovascular disease: 2007 update: A scientific statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation 2007, 116, 572–584. [Google Scholar] [CrossRef]
- Perrone, M.A.; Feola, A.; Pieri, M.; Donatucci, B.; Salimei, C.; Lombardo, M.; Perrone, A.; Parisi, A. The Effects of Reduced Physical Activity on the Lipid Profile in Patients with High Cardiovascular Risk during COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 8858. [Google Scholar] [CrossRef]
- Fealy, C.E.; Nieuwoudt, S.; Foucher, J.A.; Scelsi, A.R.; Malin, S.K.; Pagadala, M.; Cruz, L.A.; Li, M.; Rocco, M.; Burguera, B.; et al. Functional high-intensity exercise training ameliorates insulin resistance and cardiometabolic risk factors in type 2 diabetes. Exp. Physiol. 2018, 103, 985–994. [Google Scholar] [CrossRef]
- Marzolini, S.; Oh, P.; Brooks, D. Effect of combined aerobic and resistance training versus aerobic training alone in individuals with coronary artery disease: A meta-analysis. Eur. J. Prev. Cardiol. 2012, 19, 81–94. [Google Scholar] [CrossRef] [PubMed]
- Caminiti, G.; Iellamo, F.; Perrone, M.A.; D’Antoni, V.; Catena, M.; Manzi, V.; Morsella, V.; Franchini, A.; Volterrani, M. Central Hemodynamic Adjustments during Post-Exercise Hypotension in Hypertensive Patients with Ischemic Heart Disease: Concurrent Circuit Exercise versus High-Intensity Interval Exercise. A Preliminary Study. J. Clin. Med. 2021, 10, 5881. [Google Scholar] [CrossRef] [PubMed]
- Caminiti, G.; Perrone, M.A.; Iellamo, F.; D’Antoni, V.; Catena, M.; Franchini, A.; Volterrani, M. Acute Left Atrial Response to Different Eccentric Resistance Exercise Loads in Patients with Heart Failure with Middle Range Ejection Fraction: A Pilot Study. J. Pers. Med. 2022, 12, 689. [Google Scholar] [CrossRef]
- Hotta, K.; Kamiya, K.; Shimizu, R.; Yokoyama, M.; Nakamura-Ogura, M.; Tabata, M.; Kamekawa, D.; Akiyama, A.; Kato, M.; Noda, C.; et al. Stretching exercises enhance vascular endothelial function and improve peripheral circulation in patients with acute myocardial infarction. Int. Heart J. 2013, 54, 59–63. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Clinical and Demographic Characteristics | ||
|---|---|---|
| Age | N= | % |
| 40–60 | 4 | 13 |
| 61–80 | 15 | 50 |
| 81–95 | 11 | 37 |
| CV risk factors | ||
| Hypertension | 9 | 30 |
| Obesity | 5 | 17 |
| Diabetes Mellitus | 4 | 13 |
| Dyslipidemia | 6 | 20 |
| Smoking | 3 | 10 |
| ICD or PM indication | ||
| Atrial fibrillation/atrial flutter | 11 | 37 |
| Complete atrium-ventricular block | 6 | 20 |
| Sick sinus syndrome | 6 | 20 |
| Post-ischemic dilated cardiomyopathy | 5 | 17 |
| Hypertrophic cardiomyopathy | 1 | 3 |
| Recurrent syncope | 1 | 3 |
| Type of device | ||
| (PM) dual chamber | 17 | 57 |
| (PM) single chamber | 8 | 27 |
| ICD | 5 | 16 |
| Medications | ||
| Diuretics | 26 | 87 |
| Antiarrhytmics | 15 | 50 |
| Angiotensin II receptor blockers | 10 | 33 |
| Betablockers | 9 | 30 |
| Vitamin K antagonists | 8 | 27 |
| Calcium antagonists | 8 | 27 |
| ACE inhibitors | 7 | 23 |
| Statins | 6 | 20 |
| Direct oral anticoagulants | 5 | 17 |
| Aspirin | 4 | 13 |
| Digitalis | 4 | 13 |
| Clopidogrel | 2 | 7 |
| Alfa-blockers | 2 | 7 |
| Nitroglycerin | 1 | 3 |
| Aerobic Fitness | Muscle Strength (kg) | Flexibility (cm) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | PRE | POST | p | Parameter | PRE | POST | p | Parameter | PRE | POST | p |
| Basal HR (bpm) | 69 ± 6 | 69 ± 7 | 0.4 | Quadriceps | 21 ± 18 | 29 ± 16 | 0.000003 | Sit and reach | −19 ± 11.7 | −15 ± 11.7 | 0.003 |
| Basal SBP (mmHg) | 122 ± 72 | 121 ± 12 | 0.3 | Biceps brachii | 11 ± 5 | 15 ± 9 | 0.02 | Back scratch R | −19 ± 11.6 | −15 ± 10.0 | 0.02 |
| Basal DBP (mmHg) | 74 ± 7 | 74 ± 11 | 0.2 | Triceps brachii | 7 ± 3 | 9 ± 4 | 0.003 | Back scratch L | −21 ± 17.7 | −18 ± 13.5 | 0.3 |
| Peak power (watt) | 87 ± 30.7 | 108 ± 37.0 | 0.001 | Deltoid | 6 ± 2 | 7 ± 3 | 0.01 | Lateral R | −44 ± 1.4 | −43 ± 9.5 | 0.1 |
| Peak HR (bpm) | 96 ± 19.5 | 106 ± 22.6 | 0.008 | Lateral L | −43 ± 6.0 | −45 ± 8.7 | 0.2 | ||||
| V ̇O2peak (mL/kg/min) | 15 ± 3.8 | 17 ± 4.1 | 0.001 | ||||||||
| V ̇O2peak (mL/min) | 1232 ± 386.9 | 1413 ± 494 | 0.02 | ||||||||
| LT V ̇O2 (mL/kg/min) | 10 ± 2.2 | 11 ± 2.1 | 0.4 | ||||||||
| Peak SBP (mm Hg) | 156 ± 19.8 | 156 ± 23.5 | 0.4 | ||||||||
| Peak DBP (mm Hg) | 77 ± 10.7 | 72 ± 11.1 | 0.009 | ||||||||
| V ̇O2/HR average value | 13 ± 3.9 | 12 ± 5 | 0.73 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Squeo, M.R.; Di Giacinto, B.; Perrone, M.A.; Santini, M.; Sette, M.L.; Fabrizi, E.; Vaquer, A.; Parisi, A.; Spataro, A.; Biffi, A. Efficacy and Safety of a Combined Aerobic, Strength and Flexibility Exercise Training Program in Patients with Implantable Cardiac Devices. J. Cardiovasc. Dev. Dis. 2022, 9, 182. https://doi.org/10.3390/jcdd9060182
Squeo MR, Di Giacinto B, Perrone MA, Santini M, Sette ML, Fabrizi E, Vaquer A, Parisi A, Spataro A, Biffi A. Efficacy and Safety of a Combined Aerobic, Strength and Flexibility Exercise Training Program in Patients with Implantable Cardiac Devices. Journal of Cardiovascular Development and Disease. 2022; 9(6):182. https://doi.org/10.3390/jcdd9060182
Chicago/Turabian StyleSqueo, Maria Rosaria, Barbara Di Giacinto, Marco Alfonso Perrone, Massimo Santini, Maria Luisa Sette, Emanuele Fabrizi, Antonia Vaquer, Attilio Parisi, Antonio Spataro, and Alessandro Biffi. 2022. "Efficacy and Safety of a Combined Aerobic, Strength and Flexibility Exercise Training Program in Patients with Implantable Cardiac Devices" Journal of Cardiovascular Development and Disease 9, no. 6: 182. https://doi.org/10.3390/jcdd9060182
APA StyleSqueo, M. R., Di Giacinto, B., Perrone, M. A., Santini, M., Sette, M. L., Fabrizi, E., Vaquer, A., Parisi, A., Spataro, A., & Biffi, A. (2022). Efficacy and Safety of a Combined Aerobic, Strength and Flexibility Exercise Training Program in Patients with Implantable Cardiac Devices. Journal of Cardiovascular Development and Disease, 9(6), 182. https://doi.org/10.3390/jcdd9060182