
Depression and Anxiety Are Associated with Physical Performance in Patients Undergoing Cardiac Rehabilitation: A Retrospective Observational Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
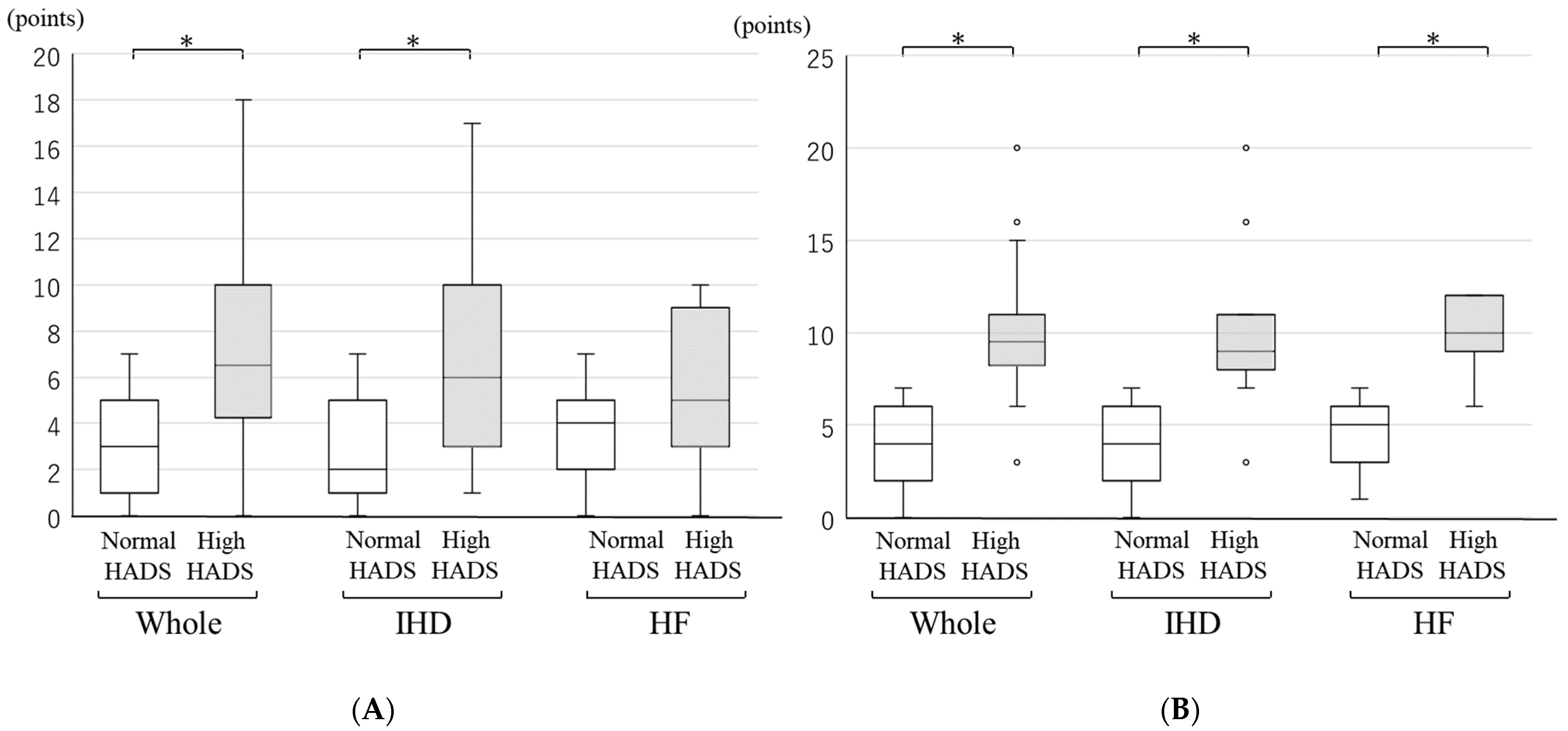
2.2. HADS
2.3. Body Composition
2.4. Physical Performance Tests
2.5. CPET
2.6. Statistical Analysis
3. Results
3.1. Patient Background
3.2. Body Composition
3.3. Physical Performances
3.4. CPET
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Gallagher, R.; Woolaston, A.; Tofler, G.; Bauman, A.; Zhao, E.; Jeon, Y.-H.; Neubeck, L.; Mitchell, J.-A.; Naismith, S.L. Cognitive impairment and psychological state in acute coronary syndrome patients: A prospective descriptive study at cardiac rehabilitation entry, completion and follow-up. Eur. J. Cardiovasc. Nurs. 2020, 20, 56–63. [Google Scholar] [CrossRef]
- Gostoli, S.; Roncuzzi, R.; Urbinati, S.; Rafanelli, C. Clinical and Subclinical Distress, Quality of Life, and Psychological Well-Being after Cardiac Rehabilitation. Appl. Psychol. Health Well Being 2017, 9, 349–369. [Google Scholar] [CrossRef] [PubMed]
- Szczepanska-Gieracha, J.; Morka, J.; Kowalska, J.; Kustrzycki, W.; Rymaszewska, J. The role of depressive and anxiety symptoms in the evaluation of cardiac rehabilitation efficacy after coronary artery bypass grafting surgery. Eur. J. Cardiothorac. Surg. 2012, 42, e108–e114. [Google Scholar] [CrossRef] [Green Version]
- Blumenthal, J.A.; Sherwood, A.; Smith, P.J.; Watkins, L.; Mabe, S.; Kraus, W.E.; Ingle, K.; Miller, P.; Hinderliter, A. Enhancing Cardiac Rehabilitation with Stress Management Training: A Randomized, Clinical Efficacy Trial. Circulation 2016, 133, 1341–1350. [Google Scholar] [CrossRef] [Green Version]
- Albus, C.; Herrmann-Lingen, C.; Jensen, K.; Hackbusch, M.; Munch, N.; Kuncewicz, C.; Grilli, M.; Schwaab, B.; Rauch, B. Additional effects of psychological interventions on subjective and objective outcomes compared with exercise-based cardiac rehabilitation alone in patients with cardiovascular disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2019, 26, 1035–1049. [Google Scholar] [CrossRef] [Green Version]
- Chauvet-Gelinier, J.C.; Bonin, B. Stress, anxiety and depression in heart disease patients: A major challenge for cardiac rehabilitation. Ann. Phys. Rehabil. Med. 2017, 60, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Compare, A.; Mommersteeg, P.M.; Faletra, F.; Grossi, E.; Pasotti, E.; Moccetti, T.; Auricchio, A. Personality traits, cardiac risk factors, and their association with presence and severity of coronary artery plaque in people with no history of cardiovascular disease. J. Cardiovasc. Med. 2014, 15, 423–430. [Google Scholar] [CrossRef] [Green Version]
- Beekman, E.; Verhagen, A. Clinimetrics: Hospital Anxiety and Depression Scale. J. Physiother. 2018, 64, 198. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Reference values for the timed up and go test: A descriptive meta-analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Kear, B.M.; Guck, T.P.; McGaha, A.L. Timed Up and Go (TUG) Test: Normative Reference Values for Ages 20 to 59 Years and Relationships with Physical and Mental Health Risk Factors. J. Prim. Care Community Health 2017, 8, 9–13. [Google Scholar] [CrossRef] [Green Version]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Eto, M.; Miyauchi, S. Relationship between occlusal force and falls among community-dwelling elderly in Japan: A cross-sectional correlative study. BMC Geriatr. 2018, 18, 111. [Google Scholar] [CrossRef] [PubMed]
- Treacy, D.; Hassett, L. The Short Physical Performance Battery. J. Physiother. 2018, 64, 61. [Google Scholar] [CrossRef] [PubMed]
- Butland, R.J.; Pang, J.; Gross, E.R.; Woodcock, A.A.; Geddes, D.M. Two-, six-, and 12-minute walking tests in respiratory disease. Br. Med. J. 1982, 284, 1607–1608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, D.; Parsons, J.; Tran, D.; Jeng, B.; Gorczyca, B.; Newton, J.; Lo, V.; Dear, C.; Silaj, E.; Hawn, T. The two-minute walk test as a measure of functional capacity in cardiac surgery patients. Arch. Phys. Med. Rehabil. 2004, 85, 1525–1530. [Google Scholar] [CrossRef]
- Connelly, D.M.; Thomas, B.K.; Cliffe, S.J.; Perry, W.M.; Smith, R.E. Clinical utility of the 2-minute walk test for older adults living in long-term care. Physiother. Can. 2009, 61, 78–87. [Google Scholar] [CrossRef] [Green Version]
- JCS Joint Working Group. Guidelines for rehabilitation in patients with cardiovascular disease (JCS 2012). Circ. J. 2014, 78, 2022–2093. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, S.S.; Andersen, C.M.; Ahm, R.; Skovbakke, S.J.; Kok, R.; Helmark, C.; Wiil, U.K.; Schmidt, T.; Olsen, K.R.; Hjelmborg, J.; et al. Efficacy and cost-effectiveness of a therapist-assisted web-based intervention for depression and anxiety in patients with ischemic heart disease attending cardiac rehabilitation [eMindYourHeart trial]: A randomised controlled trial protocol. BMC Cardiovasc. Disord. 2021, 21, 20. [Google Scholar] [CrossRef]
- Schonfelder, M.; Oberreiter, H.; Egger, A.; Tschentscher, M.; Droese, S.; Niebauer, J. Effect of different endurance training protocols during cardiac rehabilitation on quality of life. Am. J. Med. 2020, 134, 805–811. [Google Scholar] [CrossRef]
- Wells, A.; Reeves, D.; Heal, C.; Fisher, P.; Davies, L.; Heagerty, A.; Doherty, P.; Capobianco, L. Establishing the Feasibility of Group Metacognitive Therapy for Anxiety and Depression in Cardiac Rehabilitation: A Single-Blind Randomized Pilot Study. Front. Psychiatry 2020, 11, 582. [Google Scholar] [CrossRef]
- Tulloch, H.; Heenan, A.; Cupper, L.; Pelletier, R.; O’Farrell, P.; Pipe, A. Depression and Anxiety Screening and Triage Protocol for Cardiac Rehabilitation Programs. J. Cardiopulm. Rehabil. Prev. 2018, 38, 159–162. [Google Scholar] [CrossRef]
- Messerli-Burgy, N.; Barth, J.; Berger, T. The InterHerz project—A web-based psychological treatment for cardiac patients with depression: Study protocol of a randomized controlled trial. Trials 2012, 13, 245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertolotti, G.; Moroni, L.; Burro, R.; Spanevello, A.; Pedretti, R.F.; Giorgetti, G. Shortened questionnaires to assess anxiety and depression during in-hospital rehabilitation: Clinical validation and cutoff scores. Neuropsychiatr. Dis. Treat. 2016, 12, 2627–2633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiringer, I.; Simon, A.; Herrfurth, D.; Suri, I.; Szalai, K.; Veress, A. Occurrence of anxiety and depression disorders after acute cardiac events during hospital rehabilitation. Appl. Hosp. Anxiety Depress. Scale A Screen. Instrument. Psychiatr. Hung 2008, 23, 430–443. [Google Scholar]
- Garcia, G.D.; Pompeo, D.A.; Eid, L.P.; Cesarino, C.B.; Pinto, M.H.; Goncalves, L.W.P. Relationship between anxiety, depressive symptoms and compulsive overeating disorder in patients with cardiovascular diseases. Rev. Lat. Am. Enfermagem. 2018, 26, e3040. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.J.; Freedland, K.E.; Clouse, R.E.; Lustman, P.J. The prevalence of comorbid depression in adults with diabetes: A meta-analysis. Diabetes Care 2001, 24, 1069–1078. [Google Scholar] [CrossRef] [Green Version]
- Masaoka, Y.; Homma, I. Anxiety and respiratory patterns: Their relationship during mental stress and physical load. Int. J. Psychophysiol. 1997, 27, 153–159. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Whole Patients | p Value | IHD Patients | p Value | HF Patients | p Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Normal HADS | High HADS | Normal HADS | High HADS | Normal HADS | High HADS | ||||
| n = 68 | n = 32 | n = 23 | n = 15 | n = 27 | n = 7 | ||||
| Age, years | 70.2 (10.2) | 71.1 (8.5) | 0.56 | 68.7 (11.9) | 70.1 (8.0) | 0.71 | 70.9 (8.7) | 70.6 (10.0) | 0.42 |
| Male, n(%) | 48 (70.6) | 25 (78.1) | 0.43 | 21 (91.3) | 15 (80.0) | 0.31 | 13 (48.1) | 4 (57.1) | 0.67 |
| BMI, kg/m2 | 23.2 (21.4–25.8) | 23.7 (22.1–27.9) | 0.14 | 23.3 (21.8–24.7) | 23.9 (22.7–28.8) | 0.07 | 23.4 (20.6–26.7) | 22.4 (21.4–29.7) | 0.68 |
| LVEF, % | 58.8 (50.4–67.2) | 63.6 (43.8–69.0) | 0.73 | 57.9 (53.2–66.1) | 63.3 (46.9–70.2) | 0.80 | 56.9 (44.5–67.1) | 68.8 (36.7–73.6) | 0.74 |
| Frequency of CR, n(%) | 1 (1–2) | 1 (1–2) | 0.24 | 1 (1–2) | 1 (1–2) | 0.06 | 2 (1–2) | 1 (1–2) | 0.11 |
| Hypertension, n(%) | 52 (76.5) | 29 (90.6) | 0.09 | 19 (82.6) | 14 (93.3) | 0.34 | 20 (74.1) | 6 (85.7) | 0.52 |
| Diabetes mellitus, n(%) | 22 (32.4) | 18 (56.3) | 0.02 | 10 (43.5) | 9 (60.0) | 0.32 | 7 (25.9) | 1 (14.3) | 0.52 |
| Dyslipidemia, n(%) | 54 (79.4) | 31 (96.9) | 0.02 | 22 (95.7) | 15 (100) | 0.41 | 15 (55.6) | 6 (85.7) | 0.14 |
| CKD, n(%) | 42 (61.8) | 22 (68.8) | 0.50 | 9 (39.1) | 10 (66.7) | 0.10 | 22 (81.5) | 2 (28.6) | 0.01 |
| COPD, n(%) | 2 (2.9) | 1 (3.1) | 0.96 | 0 | 0 | 2 (7.4) | 0 | 0.46 | |
| The other pulmonary disease, n(%) | 5 (7.4) | 3 (9.4) | 0.73 | 1 (4.3) | 1 (6.7) | 0.75 | 4 (14.8) | 0 | 0.28 |
| Psychiatric disorder, n(%) | 2 (2.9) | 3 (9.4) | 0.17 | 1 (4.3) | 2 (13.3) | 0.32 | 1 (3.7) | 0 | 0.61 |
| Cardiovascular disease | |||||||||
| IHD, n(%) | 35 (51.5) | 23 (71.9) | 0.05 | 23 (100) | 15 (100) | 0 | 0 | ||
| Heart failure, n(%) | 39 (57.4) | 15 (46.9) | 0.33 | 0 | 0 | 27 (100) | 7 (100) | ||
| Valvular disease, n(%) | 14 (20.6) | 3 (9.4) | 0.16 | 2 (8.7) | 0 | 0.24 | 8 (29.6) | 2 (28.6) | 0.96 |
| Cardiomyopathy, n(%) | 13 (19.1) | 2 (6.3) | 0.09 | 0 | 0 | 12 (44.4) | 1 (14.3) | 0.14 | |
| Vascular disease, n(%) | 7 (10.3) | 2 (6.3) | 0.51 | 1 (4.3) | 0 | 0.41 | 4 (14.8) | 0 | 0.28 |
| Treatment | |||||||||
| PCI, n(%) | 30 (44.1) | 19 (59.4) | 0.15 | 20 (87.0) | 13 (86.7) | 0.98 | 0 | 0 | |
| CABG, n(%) | 4 (5.9) | 5 (15.6) | 0.11 | 3 (13.0) | 3 (20.0) | 0.57 | 0 | 0 | |
| Valve Operation, n(%) | 11 (16.2) | 2 (6.3) | 0.17 | 1 (4.3) | 0 | 0.41 | 7 (25.9) | 1 (14.3) | 0.52 |
| ICD/CRT, n(%) | 6 (8.8) | 3 (9.4) | 0.93 | 0 | 1 (6.7) | 0.21 | 6 (22.2) | 1 (14.3) | 0.64 |
| Whole Patients | p Value | IHD Patients | p Value | HF Patients | p Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Normal HADS | High HADS | Normal HADS | High HADS | Normal HADS | High HADS | ||||
| n = 68 | n = 32 | n = 23 | n = 15 | n = 27 | n = 7 | ||||
| Body weight, kg | 63.3 (55.2–67.1) | 62.9 (56.2–71.4) | 0.29 | 64.9 (57.8–67.5) | 66.9 (62.5–76.6) | 0.21 | 60.4 (12.6) | 59.8 (14.6) | 0.92 |
| Lean body mass, kg | 49.3 (39.6–52.3) | 46.5 (40.8–51.3) | 0.47 | 47.4 (42.4–51.2) | 48.1 (37.5–49.1) | 0.37 | 39.6 (8.7) | 39.9 (7.5) | 0.95 |
| Body fat mass, kg | 14.8 (11.7–17.6) | 15.8 (13.2–23.8) | 0.15 | 14.5 (11.7–17.5) | 19.3 (15.0–24.8) | 0.003 | 14.6 (11.2–20.1) | 13.7 (9.7–15.0) | 0.30 |
| Percent body fat, % | 24.4 (7.5) | 27.7 (8.6) | 0.07 | 22.2 (6.8) | 30.5 (7.3) | 0.001 | 27.2 (8.1) | 22.8 (8.5) | 0.34 |
| Dry lean mass, kg | 44.3 (7.2) | 44.8 (10.8) | 0.83 | 50.0 (44.7–54.0) | 50.2 (39.6–51.4) | 0.24 | 41.8 (9.2) | 42.1 (7.9) | 0.98 |
| Total body water, L | 32.7 (5.1) | 32.3 (6.2) | 0.75 | 34.1 (4.6) | 33.1 (7.1) | 0.61 | 29.9 (6.1) | 29.3 (4.9) | 0.85 |
| Estimated bone mass, kg | 2.60 (2.23–2.73) | 2.45 (2.15–2.70) | 0.30 | 2.60 (2.40–2.90) | 2.65 (2.10–2.70) | 0.20 | 2.20 (1.90–2.70) | 2.35 (1.90–2.55) | 0.82 |
| Basal metabolic rate, kcal | 1282 (187) | 1256 (200) | 0.56 | 1339 (161) | 1292 (211) | 0.45 | 1169 (230) | 1139 (186) | 0.82 |
| Trunk lean mass, kg | 25.5 (22.2–27.1) | 24.8 (21.8–26.2) | 0.19 | 25.9 (24.0–28.3) | 25.5 (19.3–26.5) | 0.09 | 20.4 (19.2–25.5) | 24.2 (19.9–25.7) | 0.75 |
| Right arm lean mass, kg | 2.25 (0.47) | 2.28 (0.48) | 0.76 | 2.46 (0.40) | 2.38 (0.53) | 0.62 | 1.70 (1.50–2.40) | 2.25 (1.75–2.30) | 0.98 |
| Left arm lean mass, kg | 2.30 (1.83–2.53) | 2.15 (2.00–2.55) | 0.95 | 2.37 (0.38) | 2.30 (0.47) | 0.60 | 1.90 (0.57) | 1.98 (0.46) | 0.81 |
| Right leg lean mass, kg | 7.70 (1.58) | 7.67 (1.71) | 0.95 | 8.17 (1.25) | 8.02 (1.76) | 0.77 | 6.88 (1.93) | 6.68 (1.36) | 0.85 |
| Left leg lean mass, kg | 7.54 (1.55) | 7.55 (1.72) | 0.98 | 7.94 (1.26) | 7.88 (1.78) | 0.85 | 6.75 (1.92) | 6.55 (1.25) | 0.85 |
| Trunk fat mass, kg | 9.00 (6.20–10.48) | 9.35 (8.05–12.95) | 0.15 | 8.70 (6.30–10.30) | 11.65 (8.70–15.60) | 0.005 | 8.70 (5.90–10.70) | 8.20 (5.80–8.70) | 0.39 |
| Right arm fat mass, kg | 0.60 (0.45–0.75) | 0.65 (0.50–0.90) | 0.21 | 0.60 (0.40–0.70) | 0.80 (0.60–1.00) | 0.003 | 0.60 (0.40–0.80) | 0.55 (0.35–0.65) | 0.44 |
| Left arm fat mass, kg | 0.60 (0.45–0.75) | 0.70 (0.55–0.90) | 0.10 | 0.60 (0.50–0.80) | 0.80 (0.70–1.10) | 0.002 | 0.60 (0.50–0.80) | 0.55 (0.40–0.65) | 0.41 |
| Right leg fat mass, kg | 2.45 (1.88–2.95) | 2.65 (2.05–3.50) | 0.20 | 2.40 (1.80–2.80) | 3.00 (2.70–4.30) | 0.002 | 2.50 (2.30–3.40) | 2.30 (1.65–2.55) | 0.23 |
| Left leg fat mass, kg | 2.45 (1.90–2.93) | 2.65 (2.10–3.45) | 0.13 | 2.50 (1.80–2.90) | 3.10 (2.60–4.30) | 0.001 | 2.50 (2.30–3.30) | 2.30 (1.70–2.55) | 0.26 |
| Whole Patients | p Value | IHD Patients | p Value | HF Patients | p Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Normal HADS | High HADS | Normal HADS | High HADS | Normal HADS | High HADS | ||||
| n = 68 | n = 32 | n = 23 | n = 15 | n = 27 | n = 7 | ||||
| Timed Up and Go Test, sec | 6.75 (5.95–7.70) | 7.52 (6.64–9.09) | 0.01 | 6.25 (6.00–7.60) | 7.20 (6.60–9.00) | 0.07 | 6.90 (6.00–8.50) | 6.90 (6.00–9.60) | 0.77 |
| Right-legged ST test, sec | 35.9 (18.4–60.0) | 26.5 (11.2–60.0) | 0.12 | 60.0 (23.4–60.0) | 39.2 (7.9–60.0) | 0.33 | 27.4 (14.1–60.0) | 18.6 (12.3–47.2) | 0.51 |
| Left-legged ST test, sec | 30.8 (10.6–60.0) | 28.4 (6.0–60.0) | 0.27 | 47.1 (10.6–60.0) | 43.5 (11.2–60.0) | 0.65 | 26.3 (7.7–60.0) | 21.8 (6.0–53.3) | 0.75 |
| SPPB, points | 12.0 (12.0–12.0) | 12.0 (11.5–12.0) | 0.61 | 12.0 (12.0–12.0) | 12.0 (12.0–12.0) | 0.83 | 12.0 (12.0–12.0) | 12.0 (10.0–12.0) | 0.55 |
| Whole Patients | p Value | IHD Patients | p Value | HF Patients | p Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Normal HADS | High HADS | Normal HADS | High HADS | Normal HADS | High HADS | ||||
| n = 68 | n = 32 | n = 23 | n = 15 | n = 27 | n = 7 | ||||
| Distance, m | 202 (185–216) | 186 (162–208) | 0.01 | 211 (200–238) | 194 (178–210) | 0.05 | 191 (26) | 189 (24) | 0.83 |
| RPE, points | |||||||||
| Baseline | 11 (9–12) | 11 (11–11) | 0.96 | 11 (8–11) | 11 (10–11) | 0.97 | 11 (11–12) | 11 (11–12) | 0.63 |
| After 1 min | 11 (11–13) | 13 (12–14) | 0.26 | 11 (11–12) | 11 (11–12) | 0.68 | 12 (11–13) | 13 (11–16) | 0.22 |
| After 2 min | 13 (11–13) | 13 (12–14) | 0.22 | 13 (11–13) | 13 (12–13) | 0.92 | 13 (11–14) | 13 (12–17) | 0.38 |
| SpO2, % | |||||||||
| Baseline | 97 (97–98) | 97 (96–98) | 0.28 | 97 (97–98) | 97 (96–98) | 0.53 | 97 (97–98) | 96 (96–98) | 0.52 |
| After 1 min | 97 (96–97) | 96 (96–97) | 0.15 | 97 (95–97) | 97 (96–97) | 0.75 | 97 (96–98) | 96 (94–97) | 0.09 |
| After 2 min | 96 (95–97) | 96 (94–96) | 0.09 | 96 (94–97) | 96 (94–97) | 0.53 | 96 (95–97) | 94 (92–95) | 0.01 |
| HR, /min | |||||||||
| Baseline | 76 (69–86) | 82 (70–96) | 0.38 | 80.2 (13.7) | 81.5 (16.7) | 0.80 | 73.3 (11.8) | 81.1 (17.1) | 0.16 |
| After 1 min | 91.0 (16.5) | 91.5 (14.5) | 0.92 | 94.6 (17.3) | 92.5 (16.6) | 0.71 | 85.1 (16.1) | 91.4 (9.7) | 0.33 |
| After 2 min | 98.0 (17.1) | 96.2 (14.8) | 0.56 | 102.9 (18.3) | 96.8 (16.3) | 0.31 | 93.2 (17.3) | 95.0 (9.8) | 0.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakamoto, M.; Suematsu, Y.; Yano, Y.; Kaino, K.; Teshima, R.; Matsuda, T.; Fujita, M.; Tazawa, R.; Fujimi, K.; Miura, S.-i. Depression and Anxiety Are Associated with Physical Performance in Patients Undergoing Cardiac Rehabilitation: A Retrospective Observational Study. J. Cardiovasc. Dev. Dis. 2022, 9, 21. https://doi.org/10.3390/jcdd9010021
Sakamoto M, Suematsu Y, Yano Y, Kaino K, Teshima R, Matsuda T, Fujita M, Tazawa R, Fujimi K, Miura S-i. Depression and Anxiety Are Associated with Physical Performance in Patients Undergoing Cardiac Rehabilitation: A Retrospective Observational Study. Journal of Cardiovascular Development and Disease. 2022; 9(1):21. https://doi.org/10.3390/jcdd9010021
Chicago/Turabian StyleSakamoto, Maaya, Yasunori Suematsu, Yuiko Yano, Koji Kaino, Reiko Teshima, Takuro Matsuda, Masaomi Fujita, Rie Tazawa, Kanta Fujimi, and Shin-ichiro Miura. 2022. "Depression and Anxiety Are Associated with Physical Performance in Patients Undergoing Cardiac Rehabilitation: A Retrospective Observational Study" Journal of Cardiovascular Development and Disease 9, no. 1: 21. https://doi.org/10.3390/jcdd9010021
APA StyleSakamoto, M., Suematsu, Y., Yano, Y., Kaino, K., Teshima, R., Matsuda, T., Fujita, M., Tazawa, R., Fujimi, K., & Miura, S.-i. (2022). Depression and Anxiety Are Associated with Physical Performance in Patients Undergoing Cardiac Rehabilitation: A Retrospective Observational Study. Journal of Cardiovascular Development and Disease, 9(1), 21. https://doi.org/10.3390/jcdd9010021