
Not Only Diagnostic Yield: Whole-Exome Sequencing in Infantile Cardiomyopathies Impacts on Clinical and Family Management


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Genetic Analyses
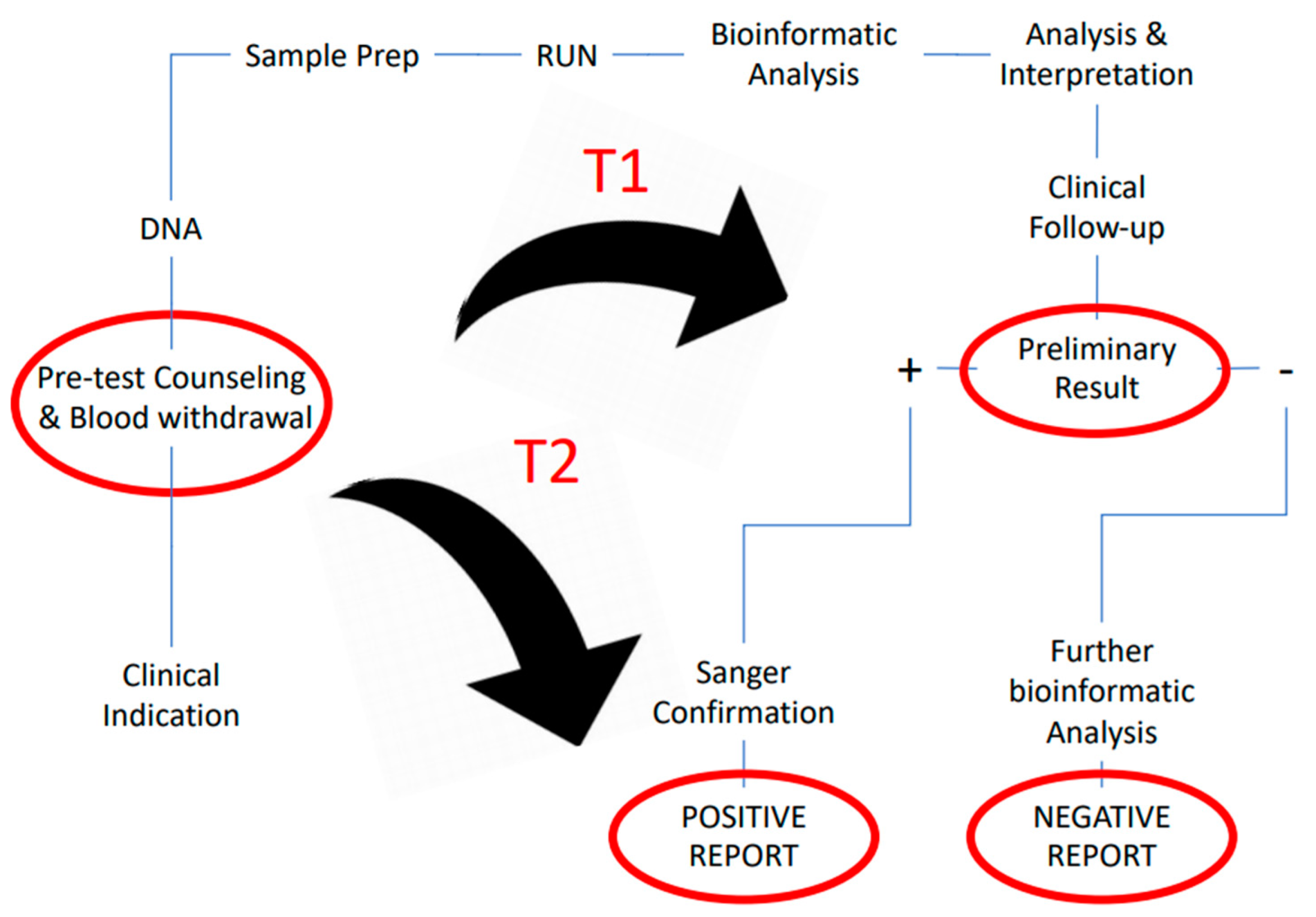
2.3. Turnaround Time and Clinical Utility Evaluation
3. Results
3.1. Overall Results
3.2. Results in Urgent Setting
3.3. Impact on Clinical Management, Diagnostic Yield and Genetic Diagnosis in Urgent vs. Non-Urgent Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kingsmore, S.F.; Cakici, J.A.; Clark, M.M.; Gaughran, M.; Feddock, M.; Batalov, S.; Bainbridge, M.N.; Carroll, J.; Caylor, S.A.; Clarke, C.; et al. A Randomized, Controlled Trial of the Analytic and Diagnostic Performance of Singleton and Trio, Rapid Genome and Exome Sequencing in Ill Infants. Am. J. Hum. Genet. 2019, 105, 719–733. [Google Scholar] [CrossRef]
- Clark, M.M.; Hildreth, A.; Batalov, S.; Ding, Y.; Chowdhury, S.; Watkins, K.; Ellsworth, K.; Camp, B.; Kint, C.I.; Yacoubian, C.; et al. Diagnosis of genetic diseases in seriously ill children by rapid whole-genome sequencing and automated phenotyping and interpretation. Sci. Transl. Med. 2019, 11, eaat6177. [Google Scholar] [CrossRef]
- Australian Genomics Health Alliance Acute Care Flagship; Lunke, S.; Eggers, S.; Wilson, M.; Patel, C.; Barnett, C.P.; Pinner, J.; Sandaradura, S.A.; Buckley, M.F.; Krzesinski, E.I.; et al. Feasibility of Ultra-Rapid Exome Sequencing in Critically Ill Infants and Children with Suspected Monogenic Conditions in the Australian Public Health Care System. JAMA 2020, 323, 2503–2511. [Google Scholar] [CrossRef]
- Dimmock, D.; Caylor, S.; Waldman, B.; Benson, W.; Ashburner, C.; Carmichael, J.L.; Carroll, J.; Cham, E.; Chowdhury, S.; Cleary, J.; et al. Project Baby Bear: Rapid precision care incorporating rWGS in 5 California children’s hospitals demonstrates improved clinical outcomes and reduced costs of care. Am. J. Hum. Genet. 2021, 108, 1231–1238. [Google Scholar] [CrossRef]
- Owen, M.J.; Niemi, A.-K.; Ding, Y.; Lenberg, J.; Chowdhury, S.; Hobbs, C.A.; Batalov, S.; Zhu, Z.; Nahas, S.A.; Gilmer, S.; et al. Rapid Sequencing-Based Diagnosis of Thiamine Metabolism Dysfunction Syndrome. N. Engl. J. Med. 2021, 384, 2159–2161. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Law, Y.M.; Colan, S.D.; Asante-Korang, A.; Austin, E.D.; Dipchand, A.I.; Everitt, M.D.; Hsu, D.T.; Lin, K.Y.; Price, J.F.; et al. Cardiomyopathy in Children: Classification and Diagnosis: A Scientific Statement from the American Heart Association. Circulation 2019, 140, e9–e68. [Google Scholar] [CrossRef]
- El-Hattab, A.W.; Scaglia, F. Mitochondrial Cardiomyopathies. Front. Cardiovasc. Med. 2016, 3, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massin, M.M.; Astadicko, I.; Dessy, H. Epidemiology of Heart Failure in a Tertiary Pediatric Center. Clin. Cardiol. 2008, 31, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Monda, E.; Rubino, M.; Lioncino, M.; Di Fraia, F.; Pacileo, R.; Verrillo, F.; Cirillo, A.; Caiazza, M.; Fusco, A.; Esposito, A.; et al. Hypertrophic Cardiomyopathy in Children: Pathophysiology, Diagnosis, and Treatment of Non-sarcomeric Causes. Front. Pediatr. 2021, 9, 94. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.M.; Hsu, D.T.; Kantor, P.; Towbin, J.A.; Ware, S.M.; Colan, S.D.; Chung, W.K.; Jefferies, J.L.; Rossano, J.W.; Castleberry, C.D.; et al. Pediatric Cardiomyopathies. Circ. Res. 2017, 121, 855–873. [Google Scholar] [CrossRef]
- Parker, L.E.; Landstrom, A.P. The clinical utility of pediatric cardiomyopathy genetic testing: From diagnosis to a precision medicine-based approach to care. Prog. Pediatr. Cardiol. 2021, 62, 101413. [Google Scholar] [CrossRef]
- A Marston, N.; Han, L.; Colan, S.D.; Rossano, J.W.; Wittekind, S.G.; Ware, J.S.; Saberi, S.; Helms, A.S.; Ho, C.Y.; Olivotto, I.; et al. Clinical characteristics and outcomes in childhood-onset hypertrophic cardiomyopathy. Eur. Heart J. 2021, 42, 1988–1996. [Google Scholar] [CrossRef]
- Grenier, M.; Osganian, S.K.; Cox, G.F.; Towbin, J.A.; Colan, S.D.; Lurie, P.R.; Sleeper, L.A.; Orav, E.; Lipshultz, S.E. Design and implementation of the North American Pediatric Cardiomyopathy Registry. Am. Heart J. 2000, 139, s86–s95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; Mahrholdt, H.; et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar] [CrossRef]
- Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; Kantor, P.; et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients with Hypertrophic Cardiomyopathy: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2020, 142, e558–e631. [Google Scholar] [PubMed]
- Rosenthal, D.; Chrisant, M.R.; Addonizio, L.; Beerman, L.; Berger, S.; Bernstein, D.; Blume, E.; Boucek, M.; Checchia, P.; Dipchand, A.; et al. International Society for Heart and Lung Transplantation: Practice guidelines for management of heart failure in children. J. Heart Lung Transplant. 2004, 23, 1313–1333. [Google Scholar] [CrossRef]
- Ross, R.D. The Ross Classification for Heart Failure in Children After 25 Years: A Review and an Age-Stratified Revision. Pediatr. Cardiol. 2012, 33, 1295–1300. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–423. [Google Scholar] [CrossRef] [PubMed]
- Nykamp, K.; Anderson, M.; Powers, M.; Garcia, J.; Herrera, B.; Ho, Y.-Y.; Kobayashi, Y.; Patil, N.; Thusberg, J.; Westbrook, M.; et al. Sherloc: A comprehensive refinement of the ACMG–AMP variant classification criteria. Genet. Med. 2017, 19, 1105–1117. [Google Scholar] [CrossRef] [Green Version]
- Robinson, J.T.; Thorvaldsdóttir, H.; Winckler, W.; Guttman, M.; Lander, E.S.; Getz, G.; Mesirov, J.P. Integrative genomics viewer. Nat. Biotechnol. 2011, 29, 24–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plagnol, V.; Curtis, J.; Kumararatne, D.; Doffinger, R.; Nejentsev, S.; Epstein, M.; Mok, K.; Stebbings, E.; Grigoriadou, S.; Wood, N.; et al. A robust model for read count data in exome sequencing experiments and implications for copy number variant calling. Bioinformatics 2012, 28, 2747–2754. [Google Scholar] [CrossRef] [Green Version]
- Riggs, E.R.; Andersen, E.F.; Cherry, A.M.; Kantarci, S.; Kearney, H.; Patel, A.; Raca, G.; Ritter, D.I.; South, S.T.; Thorland, E.C.; et al. Technical standards for the interpretation and reporting of constitutional copy-number variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics (ACMG) and the Clinical Genome Resource (ClinGen). Genet. Med. 2020, 22, 245–257. [Google Scholar] [CrossRef] [Green Version]
- De Wert, G.; Dondorp, W.; Clarke, A.; Dequeker, E.M.C.; Cordier, C.; Deans, Z.; van El, C.G.; Fellmann, F.; Hastings, R.; Hentze, S.; et al. Opportunistic genomic screening. Recommendations of the European Society of Human Genetics. Eur. J. Hum. Genet. 2021, 29, 365–377. [Google Scholar] [CrossRef]
- Iascone, M.; Sana, M.E.; Ferrazzi, P.; Pezzoli, L.; Bianchi, P.; Marchetti, D.; Fasolini, G.; Sadou, Y.; Locatelli, A.; Fabiani, F.; et al. Extensive Arterial Tortuosity and Severe Aortic Dilation in a Newborn with an EFEMP2 Mutation. Circulation 2012, 126, 2764–2768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunning, A.C.; Strucinska, K.; Oreja, M.M.; Parrish, A.; Caswell, R.; Stals, K.L.; Durigon, R.; Durlacher-Betzer, K.; Cunningham, M.H.; Grochowski, C.M.; et al. Recurrent De Novo NAHR Reciprocal Duplications in the ATAD3 Gene Cluster Cause a Neurogenetic Trait with Perturbed Cholesterol and Mitochondrial Metabolism. Am. J. Hum. Genet. 2020, 106, 272–279. [Google Scholar] [CrossRef] [Green Version]
- Frazier, A.E.; Compton, A.G.; Kishita, Y.; Hock, D.H.; Welch, A.E.; Amarasekera, S.S.; Rius, R.; Formosa, L.E.; Imai-Okazaki, A.; Francis, D.; et al. Fatal Perinatal Mitochondrial Cardiac Failure Caused by Recurrent De Novo Duplications in the ATAD3 Locus. Med. N. Y. 2021, 2, 49–73. [Google Scholar] [CrossRef]
- Towbin, J.A.; Lowe, A.M.; Colan, S.D.; Sleeper, L.A.; Orav, E.J.; Clunie, S.; Messere, J.; Cox, G.F.; Lurie, P.R.; Hsu, D.; et al. Incidence, Causes, and Outcomes of Dilated Cardiomyopathy in Children. JAMA 2006, 296, 1867–1876. [Google Scholar] [CrossRef] [PubMed]
- Ritter, A.; Bedoukian, E.; Berger, J.H.; Copenheaver, D.; Gray, C.; Krantz, I.; Izumi, K.; Juusola, J.; Leonard, J.; Lin, K.; et al. Clinical utility of exome sequencing in infantile heart failure. Genet. Med. 2019, 22, 423–426. [Google Scholar] [CrossRef]
- Geske, J.B.; Gersh, B.J. The hypertrophic cardiomyopathy paradox: Better with age. Eur. Hear. J. 2019, 40, 994–996. [Google Scholar] [CrossRef]
- Saettini, F.; Poli, C.; Vengoechea, J.; Bonanomi, S.; Orellana, J.C.; Fazio, G.; Rodriguez, I.F.H.; Noguera, L.P.; A Booth, C.; Jarur-Chamy, V.; et al. Absent B cells, agammaglobulinemia, and hypertrophic cardiomyopathy in folliculin-interacting protein 1 deficiency. Blood 2021, 137, 493–499. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Urgent | Non Urgent | |
|---|---|---|---|
| Patients n | 42 | 24 | 18 |
| Gender | |||
| Male n (%) | 26 (61.9%) | 12 (50%) | 14 (77.8%) |
| Female n (%) | 16 (38.1%) | 12 (50%) | 4 (22.2%) |
| Mean age (median) in months | 4.0 (3.0) | 4.3 (3.0) | 3.7 (3.0) |
| CM type | |||
| HCM n (%) | 30 (71.4%) | 19 (79.2%) | 11 (61.1%) |
| DCM n (%) | 12 (28.6%) | 5 (20.8%) | 7 (38.9%) |
| CM classification | |||
| Isolated n (%) | 12 (28.6%) | 5 (20.8%) | 7 (38.8%) |
| Complex n (%) | 30 (71.4%) | 19 (79.2%) | 11 (61.2%) |
| Positive family history n (%) | 5 (11.9%) | 3 (12.5%) | 2 (11.1%) |
| Prenatal diagnosis of CM n (%) | 9 (21.4%) | 5 (20.8%) | 4 (22.2%) |
| ID# | Urgent | Age (Months) | Sex | Type of CM * | Disease | Gene | Genomic Position (hg19) | cDNA | Protein | Zygosity | Inheritance | ACMG Classification |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 | no | 7 | M | iDCM | Cardiomyopathy, dilated | ACTC1 | Chr15:g.35085595T>C | NM_005159.4:c.305A>G | p.(Glu102Gly) | hetero | father | Likely pathogenic |
| 3 | no | 3 | F | iDCM | Cardiomyopathy, dilated | TNNT2 | Chr1:g.201331116C>T | NM_001001430.2:c.614G>A | p.(Arg205Gln) | hetero | de novo | Pathogenic |
| 5 | yes | 1 | M | iHCM | Noonan syndrome | PTPN11 | Chr12:g.112888202C>T | NM_002834.4:c.218C>T | p.(Thr73Ile) | hetero | de novo | Pathogenic |
| 6 | no | 1 | M | sHCM | Noonan syndrome | RAF1 | Chr3:g.12645682_12645684del | NM_001354689.1:c.785_787del | p.(Asn262_ Val263delinsIle) | hetero | de novo | Pathogenic |
| 7 | yes | 1 | M | sHCM | Glycogen storage disease of heart, lethal congenital | PRKAG2 | Chr7:g.151257696C>T | NM_016203.4:c.1592G>A | p.(Arg531Gln) | hetero | de novo | Pathogenic |
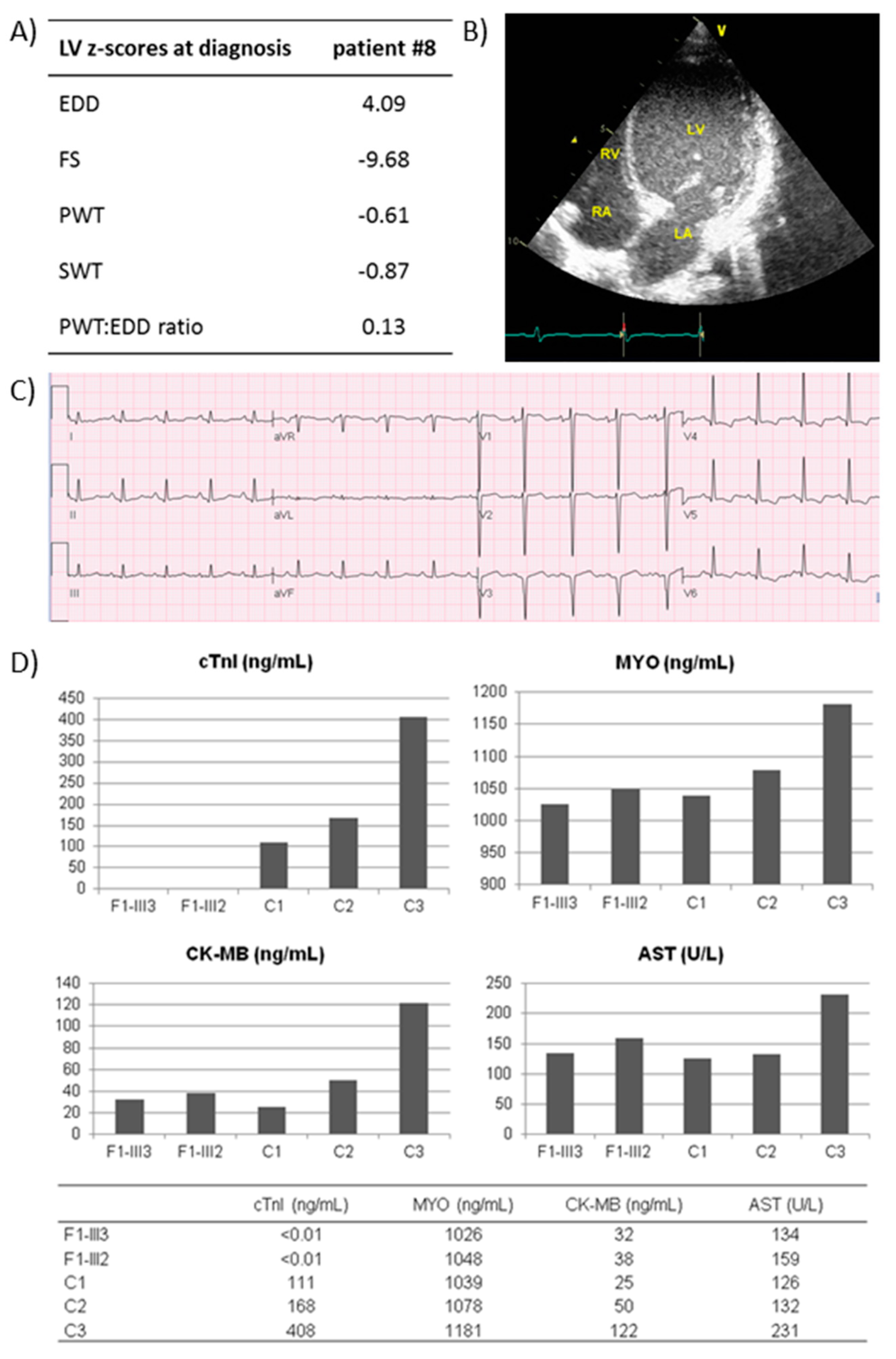
| 8 | yes | 12 | F | iDCM | Cardiomyopathy, dilated | TNNI3 | Chr19:g.55668662A>T | NM_000363.4:c.24+2T>A | skip of exon 2 | homo | both | Likely pathogenic |
| 12 | yes | 4 | F | mHCM | Trifunctional protein deficiency | HADHB | Chr2:g.26502860A>G | NM_000183.3:c.812-2A>G | skip of exon 10 | homo | both | Likely pathogenic |
| 13 | yes | 6 | F | iHCM | Glycogen storage disease II | GAA | Chr17:g.78078910del | NM_000152.5:c.525del | p.(Glu176fs*45) | hetero | father | Pathogenic |
| Chr17:g.78090909G>A | NM_000152.5:c.2331+1G>A | skip of exon 16 | hetero | mother | Pathogenic | |||||||
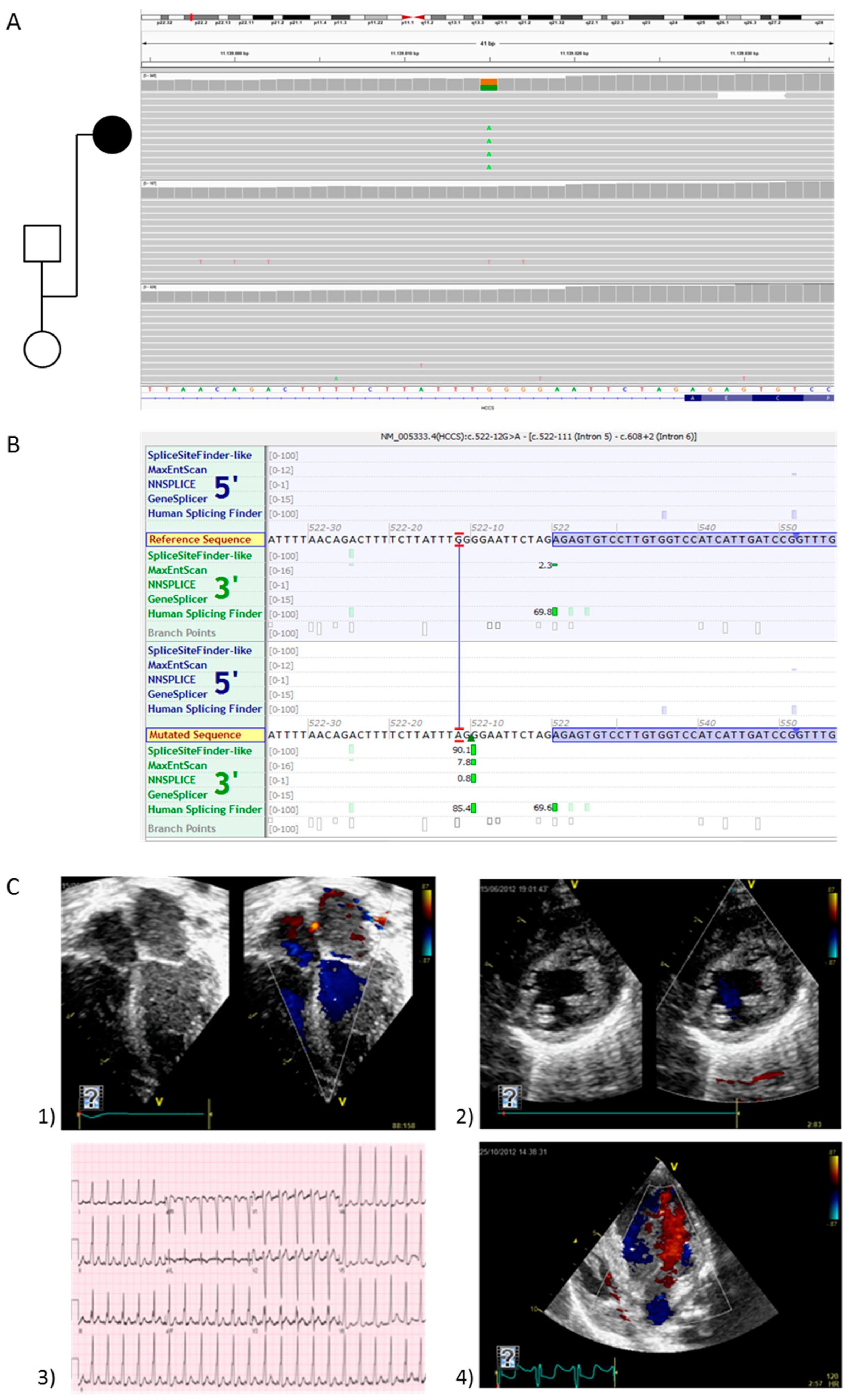
| 14 | yes | 3 | F | sHCM | Linear skin defects with multiple congenital anomalies | HCCS | ChrX:g.11139015G>A | NM_005333.4:c.522-12G>A | p.(Ala174fs*2) | hetero | de novo | Likely pathogenic |
| 17 | no | 1 | F | sHCM | Noonan syndrome | PTPN11 | Chr12:g.112926270C>T | NM_002834.4:c.1403C>T | p.(Thr468Met) | hetero | de novo | Pathogenic |
| 18 | no | 0 | M | sHCM | Noonan syndrome | RAF1 | Chr3:g.12645699G>A | NM_001354689.1:c.770C>T | p.(Ser257Leu) | hetero | de novo | Pathogenic |
| 19 | yes | 3 | M | mHCM | Tyrosinemia, type I | FAH | Chr15:g.80450512G>T | NM_000137.3:c.192G>T | p.(Gln64His) | homo | both | Pathogenic |
| 20 | yes | 10 | F | mHCM | Glycogen storage disease II | GAA | Chr17:g.78078910del | NM_000152.5:c.525del | p.(Glu176fs*45) | hetero | father | Pathogenic |
| Chr17:g.78079671C>T | NM_000152.5:c.670C>T | p.(Arg224Trp) | hetero | mother | Pathogenic | |||||||
| 21 | yes | 1 | F | mHCM | Trifunctional protein deficiency | HADHB | Chr2:g.26505741del | NM_000183.3:c.962del | p.(Met321fs*17) | hetero | mother | Likely pathogenic |
| Chr2:g.26502860A>G | NM_000183.3:c.812-2A>G | skip of exon 10 | hetero | father | Likely pathogenic | |||||||
| 22 | yes | 9 | M | mDCM | Barth syndrome | TAZ | ChrX:g.153640263_153640266del | NM_000116.3:c.83_86del | p.(Val28Alafs*11) | hemi | mother | Likely pathogenic |
| 24 | yes | 11 | M | mHCM | Mucopolysaccharidosis-plus syndrome | VPS33A | Chr12:g.122717464G>A | NM_022916.6:c.1492C>T | p.(Arg498Trp) | homo | both | Pathogenic |
| 26 | yes | 3 | M | mHCM | Pituitary hormone deficiency | POU1F1 | Chr3:g.87310439G>A | NM_000306.3:c.649C>T | p.(Arg217*) | homo | both | Likely pathogenic |
| 27 | yes | 0 | M | sHCM | Noonan syndrome | PTPN11 | Chr12:g.112926908C>G | NM_002834.4:c.1528C>G | p.(Gln510Glu) | hetero | de novo | Pathogenic |
| 28 | yes | 0 | M | sHCM | Costello syndrome | HRAS | Chr11:g.534288C>T | NM_005343.4:c.35G>A | p.(Gly12Asp) | hetero | de novo | Pathogenic |
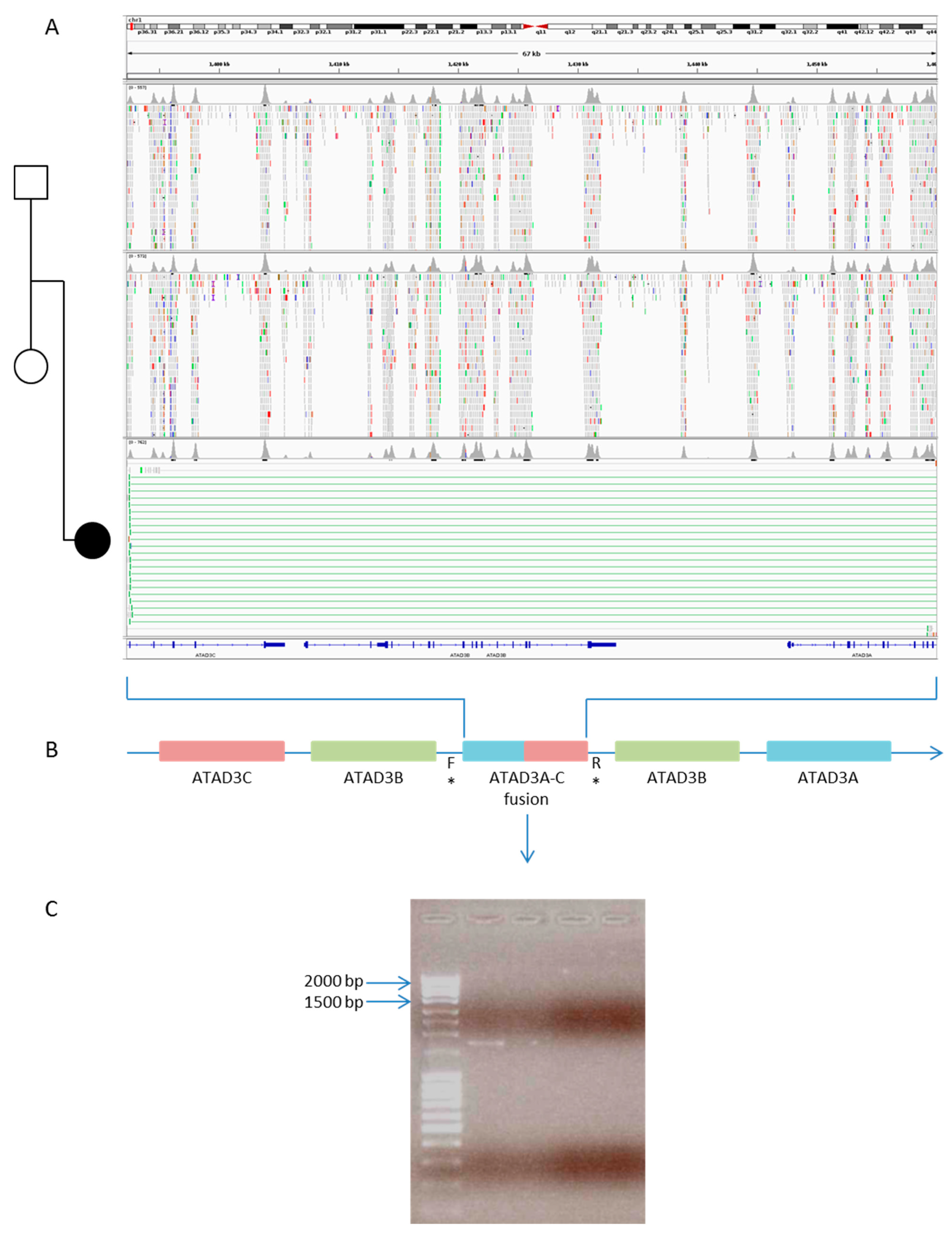
| 30 | yes | 1 | F | mHCM | Chromosome 1p36.33 duplication syndrome | ATAD3A | Chr1:1392270_1460317dup | Fusion gene ATAD3A-ATAD3C | hetero | de novo | Pathogenic | |
| 32 | no | 0 | M | iHCM | Cardiomyopathy, hypertrophic | MYL2 | Chr12:111356937C>T | NM_000432.3:c.64G>A | p.(Glu22Lys) | hetero | mother | Pathogenic |
| Cardiomyopathy, hypertrophic | MYH7 | Chr14:g.23887522C>T | NM_000257.3:c.4066G>A | p.(Glu1356Lys) | hetero | father | Pathogenic | |||||
| 33 | no | 5 | M | sHCM | Noonan syndrome | PTPN11 | Chr12:g.112910827A>G | NM_002834.4:c.836A>G | p.(Tyr279Cys) | hetero | de novo | Pathogenic |
| 35 | no | 2 | M | iDCM | Cardiomyopathy, dilated | MYH7 | Chr14:g.23886789C>T | NM_000257.3:c.4276G>A | p.(Glu1426Lys) | hetero | mother | Likely pathogenic |
| 36 | no | 12 | M | iHCM | Cardiomyopathy, hypertrophic | MYH7 | Chr14:g.23886717C>T | NM_000257.3:c.4348G>A | p.(Asp1450Asn) | hetero | de novo | Likely pathogenic |
| 37 | no | 7 | M | iDCM | Cardiomyopathy, dilated | MYH7 | Chr14:g.23887513G>A | NM_000257.3:c.4075C>T | p.(Arg1359Cys) | hetero | father | Likely pathogenic |
| 38 | no | 8 | F | sHCM | Noonan syndrome | PTPN11 | Chr12:g.112910827A>G | NM_002834.4:c.836A>G | p.(Tyr279Cys) | hetero | de novo | Pathogenic |
| 40 | no | 3 | M | sDCM | Intellectual developmental disorder, X-linked syndromic | NONO | ChrX:g.70514185C>T | NM_001145408.1:c.457C>T | p.(Arg153*) | hemi | mother | Pathogenic |
| 41 § | yes | 9 | F | iDCM | Cardiomyopathy, dilated | TNNI3 | Chr19:g.55667648del | NM_000363.4:c.204del | p.(Arg69fs*8) | homo | both | Likely pathogenic |
| 42 § | yes | 10 | F | iDCM | Cardiomyopathy, dilated | TNNI3 | Chr19:g.55667648del | NM_000363.4:c.204del | p.(Arg69fs*8) | homo | both | Likely pathogenic |
| Treatment | n. |
|---|---|
| Non-contraindication to heart transplantation | 11 * |
| ERT/diet/specific therapy | 6 |
| Palliative care | 4 |
| Specific follow-up for extra-cardiac manifestations | 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pezzoli, L.; Pezzani, L.; Bonanomi, E.; Marrone, C.; Scatigno, A.; Cereda, A.; Bedeschi, M.F.; Selicorni, A.; Gasperini, S.; Bini, P.; et al. Not Only Diagnostic Yield: Whole-Exome Sequencing in Infantile Cardiomyopathies Impacts on Clinical and Family Management. J. Cardiovasc. Dev. Dis. 2022, 9, 2. https://doi.org/10.3390/jcdd9010002
Pezzoli L, Pezzani L, Bonanomi E, Marrone C, Scatigno A, Cereda A, Bedeschi MF, Selicorni A, Gasperini S, Bini P, et al. Not Only Diagnostic Yield: Whole-Exome Sequencing in Infantile Cardiomyopathies Impacts on Clinical and Family Management. Journal of Cardiovascular Development and Disease. 2022; 9(1):2. https://doi.org/10.3390/jcdd9010002
Chicago/Turabian StylePezzoli, Laura, Lidia Pezzani, Ezio Bonanomi, Chiara Marrone, Agnese Scatigno, Anna Cereda, Maria Francesca Bedeschi, Angelo Selicorni, Serena Gasperini, Paolo Bini, and et al. 2022. "Not Only Diagnostic Yield: Whole-Exome Sequencing in Infantile Cardiomyopathies Impacts on Clinical and Family Management" Journal of Cardiovascular Development and Disease 9, no. 1: 2. https://doi.org/10.3390/jcdd9010002
APA StylePezzoli, L., Pezzani, L., Bonanomi, E., Marrone, C., Scatigno, A., Cereda, A., Bedeschi, M. F., Selicorni, A., Gasperini, S., Bini, P., Maitz, S., Maccioni, C., Pedron, C., Colombo, L., Marchetti, D., Bellini, M., Lincesso, A. R., Perego, L., Pingue, M., ... Iascone, M. (2022). Not Only Diagnostic Yield: Whole-Exome Sequencing in Infantile Cardiomyopathies Impacts on Clinical and Family Management. Journal of Cardiovascular Development and Disease, 9(1), 2. https://doi.org/10.3390/jcdd9010002