
Common Arterial Trunk Associated with Functionally Univentricular Heart: Anatomical Study and Review of the Literature



Abstract
1. Introduction
2. Anatomical Definitions
2.1. Common Arterial Trunk
- CAT with aortic dominance and confluent pulmonary arteries (Type 1–2 of the modified Van Praagh classification).
- CAT with aortic dominance and discontinuous pulmonary arteries (Type 3 of the modified Van Praagh classification). One pulmonary artery originates from the CAT, the other is supplied by the arterial duct or collateral arteries.
- CAT with pulmonary dominance and interruption of the aortic arch (IAA, usually type B of Celoria and Patton [6], between the left carotid artery and the left subclavian artery), or coarctation of the aorta (Type 4 of the modified Van Praagh classification).
2.2. Functionally Univentricular Heart
3. Methods
3.1. Data Collection
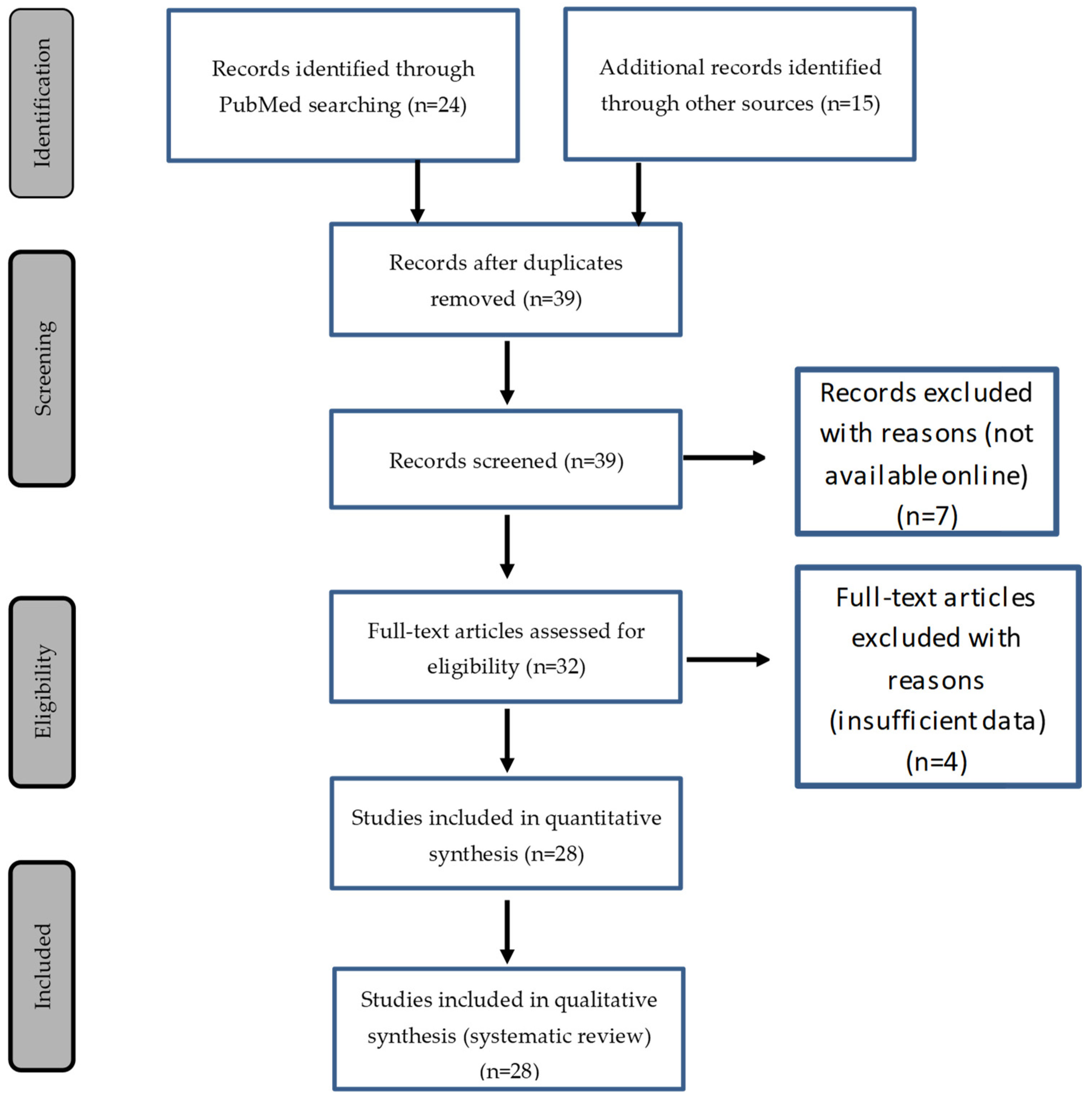
3.2. Literature Review
3.3. Heart Specimens
3.4. Fetal Echocardiography
3.5. Case Report
3.6. Statistical Analysis
4. Results
4.1. Tricuspid Atresia and Hypoplastic Right Ventricle
4.2. Mitral Atresia and Left Ventricle Hypoplasia
4.3. Double Inlet Left Ventricle:
4.4. Unbalanced Complete AVSD
4.5. Global RV and LV Hypoplasia
5. Discussion
5.1. Common Arterial Trunk Associated with Functionally Univentricular Heart has Specific Anatomic Characteristics Compared to Isolated CAT
5.2. The Phenotype of Functionally Univentricular Hearts Associated with CAT Is Different from Their Classical Forms Associated with Separate Ventriculo–Arterial Junctions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoffman, J.I.; Kaplan, S. The incidence of congenital heart disease. J. Am. Coll. Cardiol. 2002, 39, 1890–1900. [Google Scholar] [CrossRef]
- Van Praagh, R. Truncus Arteriosus: What Is It Really and How Should It Be Classified? Eur. J. Cardio-Thorac. Surg. 1987, 1, 65–70. [Google Scholar] [CrossRef]
- Jacobs, J.P.; Franklin, R.C.; Béland, M.J.; Spicer, D.E.; Colan, S.D.; Walters, H.L.; Bailliard, F.; Houyel, L.; Louis, J.D.S.; Lopez, L.; et al. Nomenclature for Pediatric and Congenital Cardiac Care: Unification of Clinical and Administrative Nomenclature—The 2021 International Paediatric and Congenital Cardiac Code (IPCCC) and the Eleventh Revision of the International Classification of Diseases (ICD-11). Cardiol. Young 2021, 31, 1057–1188. [Google Scholar]
- Jacobs, M.L. Congenital Heart Surgery Nomenclature and Database Project: Truncus Arteriosus. Ann. Thorac. Surg. 2000, 69, 50–55. [Google Scholar] [CrossRef]
- Russell, H.M.; Jacobs, M.L.; Anderson, R.H.; Mavroudis, C.; Spicer, D.; Corcrain, E.; Backer, C.L. A Simplified Categorization for Common Arterial Trunk. J. Thorac. Cardiovasc. Surg. 2011, 141, 645–653. [Google Scholar] [CrossRef]
- Celoria, G.C.; Patton, R.B. Congenital absence of the aortic arch. Am. Heart J. 1959, 58, 407–413. [Google Scholar] [CrossRef]
- Garcelon, N.; Neuraz, A.; Benoit, V.; Salomon, R.; Burgun, A. Improving a Full-Text Search Engine: The Importance of Negation Detection and Family History Context to Identify Cases in a Biomedical Data Warehouse. J. Am. Med. Inform. Assoc. 2017, 24, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, Y.; Tachi, M.; Suehiro, S.; Ito, M.; Oda, T. A Case of Staged Norwood Procedure for a Unique Form of Truncus Arteriosus, Interrupted Aortic Arch with Hypoplastic Tricuspid Valve and Right Ventricle and Anomalous Left Coronary Artery Orifice: First Reported Case. Gen. Thorac. Cardiovasc. Surg. 2017, 65, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Zeevi, B.; Dembo, L.; Berant, M. Rare Variant of Truncus Arteriosus with Intact Ventricular Septum and Hypoplastic Right Ventricle. Heart 1992, 68, 214–215. [Google Scholar] [CrossRef][Green Version]
- González-López, M.-T.; Crucean, A.; Seale, A.; McGuirk, S. Truncus Arteriosus, Tricuspid Atresia and Partial Anomalous Pulmonary Venous Drainage: A Unique Form of Univentricular Heart. Interact. Cardiovasc. Thorac. Surg. 2015, 21, 252–253. [Google Scholar] [CrossRef]
- Rao, P.S.; Levy, J.M.; Nikicicz, E.; Gilbert-Barness, E.F. Tricuspid Atresia: Association with Persistent Truncus Arteriosus. Am. Heart J. 1991, 122, 829–835. [Google Scholar] [CrossRef]
- Roldan, S.; Pieles, G.; Caputo, M.; Morgan, G.; Stoica, S.; Parry, A. Tricuspid Atresia with Truncus Arteriosus: Successful Surgical Treatment. Ann. Thorac. Surg. 2014, 98, 721–723. [Google Scholar] [CrossRef]
- Malec, E.; Mroczek, T.; Pajak, J.; Kordon, Z. Operative Treatment of Truncus Arteriosus Communis Coexisting with Tricuspid Atresia. Ann. Thorac. Surg. 2000, 69, 278–280. [Google Scholar] [CrossRef]
- Numata, S.; Uemura, H.; Kagisaki, K.; Yagihara, T. Tricuspid Atresia with Common Arterial Trunk: Successful Treatment Using Fontan Procedure. Interact. Cardiovasc. Thorac. Surg. 2004, 3, 161–162. [Google Scholar] [CrossRef]
- Sreeram, N.; Alvarado, O.; Peart, I. Tricuspid Atresia with Common Arterial Trunk: Surgical Palliation in a Neonate. Int. J. Cardiol. 1991, 32, 251–253. [Google Scholar] [CrossRef]
- Alva, C.; David, F.; Hernández, M.; Argüero, R.; Ortegón, J.; Martínez, A.; López, D.; Jiménez, S.; Sánchez, A. Tricuspid Atresia Associated with Common Arterial Trunk and 22q11 Chromosome Deletion. Arch. Cardiol. Mex. 2003, 73, 271–274. [Google Scholar] [PubMed]
- Areias, J.C.; Lopes, J.M. Common Arterial Trunk Associated with Absence of One Atrioventricular Connexion. Int. J. Cardiol. 1987, 17, 329–332. [Google Scholar] [CrossRef]
- Sharma, D.; Mehta, A.B.; Bharati, S.; Lev, M. Tricuspid Atresia with Persistent Truncus Arteriosus. Chest 1981, 79, 363–365. [Google Scholar] [CrossRef] [PubMed]
- Diógenes, T.C.; Atik, E.; Aiello, V.D. Common Arterial Trunk Associated with Absence of Right Atrioventricular Connexion. Int. J. Cardiol. 1990, 27, 385–388. [Google Scholar] [CrossRef]
- Hoashi, T.; Bove, E.L.; Ohye, R.G. Successful Staged Fontan Completion for Truncus Arteriosus with Hypoplastic Left Ventricle. Ann. Thorac. Surg. 2010, 89, 635–637. [Google Scholar] [CrossRef] [PubMed]
- Marathe, S.P.; Naganur, S.H.; Menon, S.; Orr, Y.; Cooper, S.G.; Winlaw, D.S. An Unusual Combination of Truncus Arteriosus, Interrupted Aortic Arch, and Hypoplastic Left Ventricle. World J. Pediatr. Congenit. Heart Surg. 2018, 9, 714–717. [Google Scholar] [CrossRef] [PubMed]
- Murdison, K.A.; McLean, D.A.; Carpenter, B.; Duncan, W.J. Truncus Arteriosus Communis Associated with Mitral Valve and Left Ventricular Hypoplasia without Ventricular Septal Defect: Unique Combination. Pediatr. Cardiol. 1996, 17, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Tsukuda, K.; Sakazaki, H.; Fujiwara, K. Persistent Truncus Arteriosus with Double Aortic Arch and Mitral Stenosis. Pediatr. Cardiol. 2013, 34, 2024–2026. [Google Scholar] [CrossRef]
- Michelfelder, E.C.; Zales, V.R.; Jacobs, M.L. Surgical Palliation of Truncus Arteriosus with Mitral Atresia and Hypoplastic Left Ventricle. Ann. Thorac. Surg. 1998, 65, 260–263. [Google Scholar] [CrossRef]
- Rice, M.J.; Andrilenas, K.; Reller, M.D.; McDonald, R.W. Truncus Arteriosus Associated with Mitral Atresia and a Hypoplastic Left Ventricle. Pediatr. Cardiol. 1991, 12, 128–130. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, M.L.; Pourmoghadam, K.K. Fontan Procedure for Truncus Arteriosus with Functionally Univentricular Heart. Ann. Thorac. Surg. 2010, 90, 1746. [Google Scholar] [CrossRef] [PubMed]
- Alves, P.M.; Ferrari, A.H. Common Arterial Trunk Arising Exclusively from the Right Ventricle with Hypoplastic Left Ventricle and Intact Ventricular Septum. Int. J. Cardiol. 1987, 16, 99–102. [Google Scholar] [CrossRef]
- Cree, I.C. Truncus Arteriosus and a Single Ventricle. Heart 1956, 18, 553–556. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Shaddy, R.E.; McGough, E.C. Successful Diagnosis and Surgical Treatment of Single Ventricle, Truncus Arteriosus. Ann. Thorac. Surg. 1989, 48, 298–300. [Google Scholar] [CrossRef]
- Paris, Y.M.; Bhan, I.; Marx, G.R.; Rhodes, J. Truncus Arteriosus with a Single Left Ventricle: Case Report of a Previously Unrecognized Entity. Am. Heart J. 1997, 133, 377–380. [Google Scholar] [CrossRef]
- He, D.; Olivieri, L.J.; Jonas, R.A.; Sinha, P. Palliation of Truncus Arteriosus Associated with Complete Atrioventricular Canal—Results of Single Ventricle Palliation. World J. Pediatr. Congenit. Heart Surg. 2015, 6, 663–666. [Google Scholar] [CrossRef] [PubMed]
- Panwar, S.; Bradley, S.M.; Kavarana, M.N. Truncus Arteriosus and Unbalanced Complete Atrioventricular Septal Defect: Pulmonary Protection in the Neonate. Ann. Thorac. Surg. 2012, 94, e151–e153. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, R.R.; Sridhar, A.; Chidambaram, S. Unusual Combination of Hypoplastic Left Ventricle, Atrioventricular Septal Defect with Restrictive Ventricular Septal Defect, and Common Arterial Trunk. World J. Pediatr. Congenit. Heart Surg. 2012, 3, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Devi, A.; Ghosh, G. An Infant with Truncus Arteriosus with Situs Inversus with Single Atrium: A Case Report. J. Cardiol. Cases 2017, 15, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, S.R.; Ruckman, R.N.; Kapur, S.; Chandra, R.; Galioto, F.M.; Perry, L.W.; Scott, L.P. Single Ventricle with Truncus Arteriosus in Siblings. Am. Heart J. 1981, 102, 456–459. [Google Scholar] [CrossRef]
- Van Praagh, R.J.A.S. The Segmental Approach to Diagnosis in Congenital Heart Disease. Birth Defects Orig. Artic. Ser. 1972, 8, 4–23. [Google Scholar]
- Van Praagh, R. What Determines Whether the Great Arteries Are Normally or Abnormally Related? Am. J. Cardiol. 2016, 118, 1390–1398. [Google Scholar] [CrossRef]
- Houyel, L.; Bajolle, F.; Capderou, A.; Laux, D.; Parisot, P.; Bonnet, D. The Pattern of the Coronary Arterial Orifices in Hearts with Congenital Malformations of the Outflow Tracts: A Marker of Rotation of the Outflow Tract during Cardiac Development? J. Anat. 2013, 222, 349–357. [Google Scholar] [CrossRef]
- Mostefa-Kara, M.; Bonnet, D.; Belli, E.; Fadel, E.; Houyel, L. Anatomy of the Ventricular Septal Defect in Outflow Tract Defects: Similarities and Differences. J. Thorac. Cardiovasc. Surg. 2015, 149, 682–688.e1. [Google Scholar] [CrossRef]
- Kirby, M.L.; Gale, T.F.; Stewart, D.E. Neural crest cells contribute to normal aortopulmonary septation. Science 1983, 220, 1059–1061. [Google Scholar] [CrossRef] [PubMed]
- Gittenberger-de Groot, A.C.; Bartelings, M.M.; Bogers, A.J.J.C.; Boot, M.J.; Poelmann, R.E. The Embryology of the Common Arterial Trunk. Prog. Pediatr. Cardiol. 2002, 15, 1–8. [Google Scholar] [CrossRef]
- Yelbuz, T.M.; Waldo, K.L.; Kumiski, D.H.; Stadt, H.A.; Wolfe, R.R.; Leatherbury, L.; Kirby, M.L. Shortened outflow tract leads to altered cardiac looping after neural crest ablation. Circulation 2002, 106, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Waldo, K.L.; Hutson, M.R.; Ward, C.C.; Zdanowicz, M.; Stadt, H.A.; Kumiski, D.; Abu-Issa, R.; Kirby, M.L. Secondary Heart Field Contributes Myocardium and Smooth Muscle to the Arterial Pole of the Developing Heart. Dev. Biol. 2005, 281, 78–90. [Google Scholar] [CrossRef] [PubMed]
- Momma, K. Cardiovascular anomalies associated with chromosome 22q11.2 deletion syndrome. Am. J. Cardiol. 2010, 105, 1617–1624. [Google Scholar] [CrossRef]
- Freedom, R.M. Unusual forms of common arterial trunk. Prog. Pediatr. Cardiol. 2002, 15, 19–22. [Google Scholar] [CrossRef]
- Adachi, I.; Ho, S.Y.; Bartelings, M.M.; McCarthy, K.P.; Seale, A.; Uemura, H. Common arterial trunk with atrioventricular septal defect: New observations pertinent to repair. Ann. Thorac. Surg. 2009, 87, 1495–1499. [Google Scholar] [CrossRef]
- Bajolle, F.; Zaffran, S.; Losay, J.; Ou, P.; Buckingham, M.; Bonnet, D. Conotruncal defects associated with anomalous pulmonary venous connections. Arch. Cardiovasc. Dis. 2009, 102, 105–110. [Google Scholar] [CrossRef]
- Calder, L.; Van Praagh, R.; Van Praagh, S.; Sears, W.P.; Corwin, R.; Levy, A.; Keith, J.D.; Paul, M.H. Truncus arteriosus communis. Clinical, angiocardiographic, and pathologic findings in 100 patients. Am. Heart J. 1976, 92, 23–38. [Google Scholar] [CrossRef]
- Van Praagh, S.; Davidoff, A.; Chin, A.; Shiel, F.S.; Reynolds, J.; Vanpraagh, R. Double Outlet Right Ventricle: Anatomic Types and Developmental Implications Based on a Study of 101 Autopsied Cases. Coeur 1982, 13, 389–440. [Google Scholar]
- Tandon, R.; Edwards, J.E. Tricuspid atresia: A re-evaluation and classification. J. Thorac. Cardiovasc. Surg. 1974, 67, 530. [Google Scholar] [CrossRef]
- Rao, P.S. A unified classification for tricuspid atresia. Am. Heart J. 1980, 99, 799–804. [Google Scholar] [CrossRef]
- Anderson, R.H.; Spicer, D.E.; Mohun, T.J.; Hikspoors, J.P.; Lamers, W.H. Remodeling of the embryonic interventricular communication in regard to the description and classification of ventricular septal defects. Anat. Rec. 2019, 302, 19–31. [Google Scholar] [CrossRef]
- Burnicka-Turek, O.; Steimle, J.; Huang, W.; Felker, L.; Kamp, A.; Kweon, J.; Peterson, M.; Reeves, R.H.; Maslen, C.L.; Gruber, P.J.; et al. Cilia gene mutations cause atrioventricular septal defects by multiple mechanisms. Hum. Mol. Genet. 2016, 25, 3011–3028. [Google Scholar] [CrossRef]
- Burns, T.; Yang, Y.; Hiriart, E.; Wessels, A. The dorsal mesenchymal protrusion and the pathogenesis of atrioventricular septal defects. J. Cardiovasc. Dev. Dis. 2016, 3, 29. [Google Scholar] [CrossRef] [PubMed]
- Goddeeris, M.M.; Rho, S.; Petiet, A.; Davenport, C.L.; Johnson, G.A.; Meyers, E.N.; Klingensmith, J. Intracardiac septation requires hedgehog-dependant cellular contributions from outside the heart. Development 2008, 135, 1887–1895. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.E.; Krikov, S.; Riehle-Colarusso, T.; Frías, J.L.; Belmont, J.; Anderka, M.; Geva, T.; Getz, K.D.; Botto, L.D.; National Birth Defects Prevention Study. Laterality defects in the national birth defects prevention study (1998–2007): Birth prevalence and descriptive epidemiology. Am. J. Med. Genet. Part A 2014, 164, 2581–2591. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, J.; Desai, M.; Kinare, S. Persistent truncus arteriosus—An autopsy study of 16 cases. Int. J. Cardiol. 1992, 37, 395–399. [Google Scholar] [CrossRef]
- Gumbiner, C.H.; McManus, B.M.; Latson, L.A. Associated occurrence of persistent truncus arteriosus and asplenia. Pediatr. Cardiol. 1991, 12, 192–195. [Google Scholar] [CrossRef]
- Franco, D.; Campione, M. The role of Pitx2 during cardiac development. Linking left–right Signaling and congenital heart diseases. Trends Cardiovasc. Med. 2003, 13, 157–163. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors Case Number | Chromosomal Abnormality | FUVH Type | VSD | CAT Type/ Origin | Truncal Valve Nb Leaflets | Aortic Arch | Anomalies |
|---|---|---|---|---|---|---|---|
| Fujimoto et al. [9] Case 1 | Hypoplastic RV | Large outlet | 4 | 4 | Left | IAA type B, left coronary ostium from right sinus | |
| Zeevi et al. [10] Case 2 | Hypoplastic RV | No VSD | 1 from LV | 2 | Left | No ASD, mitral stenosis, atretic right coronary ostium with retrograde sinusoid filling | |
| Gonzalez-Lopez et al. [11] Case 3 | Tricuspid atresia | Outlet | 1 from RV | 3 | Left | LUPV in retro aortic innominate vein | |
| Rao et al. [12] Case 4 | Tricuspid atresia | Outlet | 1 | 3 | Left | Hypoplastic thymus, right thumb and hemivertebrae, narrow PA branches | |
| Roldan et al. [13] Case 5 | Tricuspid atresia | Large outlet | 2 | US | US | ||
| Malec et al. [14] Case 6 | Tricuspid atresia | Outlet | 1 | US | Left | Restrictive ASD | |
| Numata et al. [15] Case 7 | Tricuspid atresia | Outlet | 1 | US | US | ||
| Sreeram et al. [16] Case 8 | Tricuspid atresia | Outlet | 1 | US | Left | ||
| Alva et al. [17] Case 9 | Di George | Tricuspid atresia | Outlet | 1 from LV | US | Right | |
| Areias et al. [18] Case 10 | Tricuspid atresia | Outlet | 3 | 3 | Right | LPA from left-sided duct | |
| Sharma et al. [19] Case 11 | Tricuspid atresia | Large outlet | 1 from LV | 3 | Right | Two OS ASD | |
| Diogenes et al. [20] Case 12 | Tricuspid atresia | Large outlet | 2 | 2 | Left | Large ASD, L-JAA | |
| Hoashi et al. [21] Case 13 | Hypoplastic LV | Large outlet | 2 | 4 | Right | RUPLV in right SCV | |
| Marathe et al. [22] Case 14 | Hypoplastic LV | No VSD | 4 from RV | 3 | Left | IAA type B | |
| Murdison et al. [23] Case 15 | Hypoplastic LV | No VSD | 1 From RV | 3 | Left | Subarterial conus, only 2 brachiocephalic arteries, RCA origin from posterior cusp | |
| Imai et al. [24] Case 16 | Hypoplastic LV | US | 2 | US | Double | LSVC | |
| Michelfelder et al. [25] Case 17 | Di George | Mitral atresia | No VSD | 1 From RV | 3 | Left | Restrictive ASD, Subarterial conus |
| Rice et al. [26] Case 18 | Mitral atresia | Outlet | 1 From RV | 4 | Left | LSCV to CS, Subarterial conus | |
| Jacobs et al. [27] Case 19 | Mitral atresia | Tiny outlet | 1 | US | US | ||
| Alves et al. [28] Case 20 | Mitral atresia | No VSD | 4 from RV | 3 | Left | Subarterial conus, IAA Type A, LCA ostium supracommissural | |
| Cree et al. [29] Case 21 | Mitral atresia | No VSD | 2 from RV | 3 | Subarterial conus, single coronary artery from inominate artery | ||
| Shaddy et al. [30] Case 22 | Double inlet LV | US | 1 | US | Left | Situs Solitus {SDD}, LSCV to LA, L-JAA | |
| Paris et al. [31] Case 23 | Double inlet LV | Large outlet | 2 | 3 | Left | Situs Solitus {SDD}, dextrocardia, L-JAA | |
| He et al. [32] Cases 24 and 25 | Di George | uAVSD (hypo LV) | Large inlet extending to outlet | 2 | 3 | Right | LSCV |
| Di George | uAVSD (hypo LV) | Large inlet extending to muscular septum | 2 | 4 | Right | ||
| Panwar et al. [33] Cases 26 and 27 | uAVSD (hypoLV) | Restrictive inlet | 1 from RV | US | US | ||
| uAVSD (hypoLV) | Restrictive inlet | 1 from RV | US | Right | |||
| Tripathi et al. [34] Cases 28 and 29 | uAVSD (hypoLV) | Restrictive inlet | 1 from RV | 3 | Right | ||
| uAVSD (hypoLV) | Restrictive inlet with muscular extension | 1 from RV | US | Left | LSCV | ||
| Kumar et al. [35] Case 30 | uAVSD (hypoLV) | Inlet | 2 from RV | 3 | Right | Situs inversus, dextrocardia, common atrium | |
| Shapiro et al. [36] Cases 31 and 32 | uAVSD (hypoRV) | Muscular (BVF) | 1 | US | Left | PA trunk stenosis | |
| uAVSD (hypoRV) | Muscular (BVF) | 1 from LV | 4 | Left |
| Case Number | FUVH Type | VSD | CAT Type/ Origin | Truncal Valve Nb Leaflets | Aortic Arch | Anomalies |
|---|---|---|---|---|---|---|
| 33 (HS) | Hypoplastic RV | Outlet VSD | 1 from RV | 4 | Left | Subarterial conus |
| 34 (HS) | Hypoplastic RV | Outlet VSD | 1 | 3 | Left | Very large ASD |
| 35 (HS) | Mitral atresia | No VSD | 2 from RV | 3 | Left | Subarterial conus, supra commissural RCA ostium, narrow LCA ostium |
| 36 (HS) | Mitral hypoplasia | Large muscular VSD | 4 from RV | 3 | Left | Subarterial conus, narrow LCA ostium, LCSV to CS, Hypoplastic horizontal Ao |
| 37 (HS) | Hypoplastic LV | No VSD | 4 from RV | 3 | Left | Subarterial conus, Type A IAA, LSCV to CS, TAPVR in CS |
| 38 (fetus) | Hypoplastic RV | Outlet | 1 from LV | US | US | |
| 39 (patient) | Tricuspid atresia | Large outlet | 1 | 3 | Left | LSCV to CS |
| Tricuspid Atresia and HypoRV N = 16 | Mitral Atresia and HypoLV N = 12 | DILV N = 2 | Unbalanced AVSD N = 9 | Hypoplastic RV, Global N = 20 | Hypoplastic LV, Global N = 19 | p | |
|---|---|---|---|---|---|---|---|
| Systemic venous return | |||||||
| LSCV to CS | 1 | 3 | 0 | 0 | 1 | 3 | |
| LSCV to LA | 0 | 0 | 1 | 0 | 1 | 0 | |
| LSCV (unspecified) | 0 | 1 | 0 | 2 | 0 | 3 | |
| Pulmonary venous return | |||||||
| PAPVR | 1 | 1 | 0 | 0 | 1 | 1 | |
| TAPVR | 0 | 1 | 0 | 0 | 0 | 1 | |
| Ventricular septal defect | |||||||
| No VSD | 1 | 7 | 0 | 0 | 1 (5%) | 7 (37%) | <0.02 |
| Outlet | 15 | 3 | 1 | 0 | 16 (89%) | 3 (27%) | <0.002 |
| Inlet | 0 | 0 | 0 | 7 | 0 | 7 | |
| Muscular | 0 | 1 | 0 | 2 | 2 | 1 | |
| Unspecified | 0 | 1 | 1 | 0 | 1 | 1 | |
| Type CAT | |||||||
| 1 | 12 | 4 | 1 | 6 | 15 | 8 | |
| 2 | 2 | 4 | 1 | 3 | 3 | 7 | |
| 3 | 1 | 0 | 0 | 0 | 1 | 0 | |
| 4 | 1 | 4 | 0 | 0 | 1 | 4 | |
| From RV | 2 | 9 | 0 | 5 | 2 (10%) | 14 (74%) | 0.0001 |
| From LV | 3 | 0 | 0 | 1 | 3 | 1 | |
| Truncal valve | |||||||
| Bicuspid | 2 | 0 | 0 | 0 | 2 | 0 | |
| Tricuspid | 6 | 8 | 1 | 3 | 7 | 11 | |
| Quadricuspid | 2 | 2 | 0 | 2 | 3 | 3 | |
| Unspecified | 6 | 2 | 1 | 4 | 7 | 6 | |
| Subarterial conus | 1 (tiny) | 8 | 0 | 0 | 1 (5%) | 8 (42%) | <0.01 |
| Coronary artery anomalies | 2 | 5 | 0 | 0 | 2 | 5 | |
| Aortic arch | |||||||
| Left | 10 | 9 | 2 | 3 | 14 | 12 | |
| Right | 3 | 1 | 0 | 5 | 3 | 6 | |
| IAA type A | 0 | 2 | 0 | 0 | 0 | 2 | |
| IAA type B | 1 | 1 | 0 | 0 | 1 | 1 | |
| AoA hypoplasia | 0 | 1 | 0 | 0 | 0 | 1 | |
| Double AoA | 0 | 1 | 0 | 0 | 0 | 1 | |
| Unspecified | 3 | 1 | 0 | 1 | 2 | 2 | |
| L-JAA | 1 | 0 | 2 | 0 | 3 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chatila, S.; Houyel, L.; Hily, M.; Bonnet, D. Common Arterial Trunk Associated with Functionally Univentricular Heart: Anatomical Study and Review of the Literature. J. Cardiovasc. Dev. Dis. 2021, 8, 175. https://doi.org/10.3390/jcdd8120175
Chatila S, Houyel L, Hily M, Bonnet D. Common Arterial Trunk Associated with Functionally Univentricular Heart: Anatomical Study and Review of the Literature. Journal of Cardiovascular Development and Disease. 2021; 8(12):175. https://doi.org/10.3390/jcdd8120175
Chicago/Turabian StyleChatila, Sami, Lucile Houyel, Manon Hily, and Damien Bonnet. 2021. "Common Arterial Trunk Associated with Functionally Univentricular Heart: Anatomical Study and Review of the Literature" Journal of Cardiovascular Development and Disease 8, no. 12: 175. https://doi.org/10.3390/jcdd8120175
APA StyleChatila, S., Houyel, L., Hily, M., & Bonnet, D. (2021). Common Arterial Trunk Associated with Functionally Univentricular Heart: Anatomical Study and Review of the Literature. Journal of Cardiovascular Development and Disease, 8(12), 175. https://doi.org/10.3390/jcdd8120175