
Long-Term Survival in Patients with Post-Operative Atrial Fibrillation after Cardiac Surgery: Analysis from a Prospective Cohort Study


 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Overall Patient Population
3.2. POP AF Population
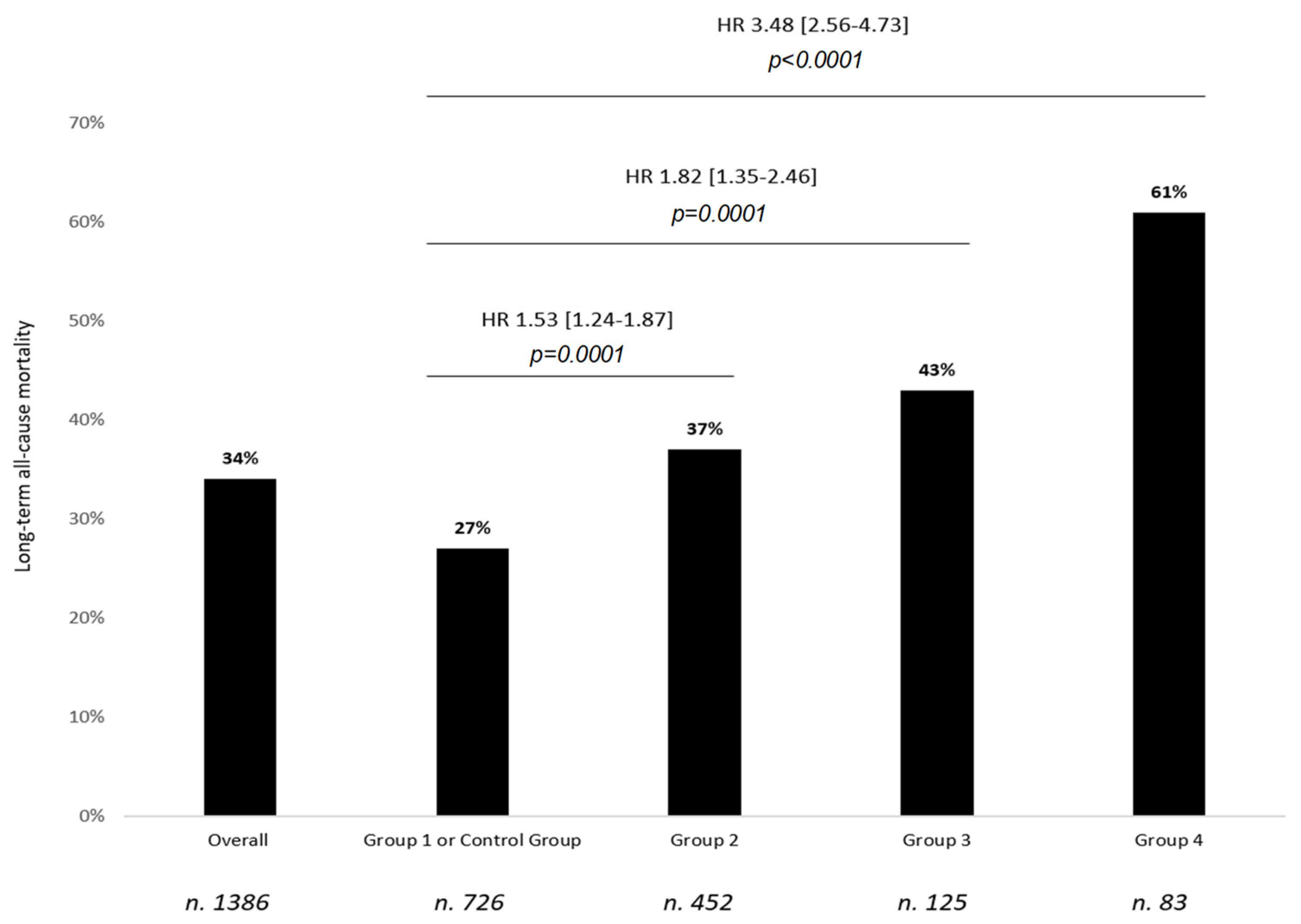
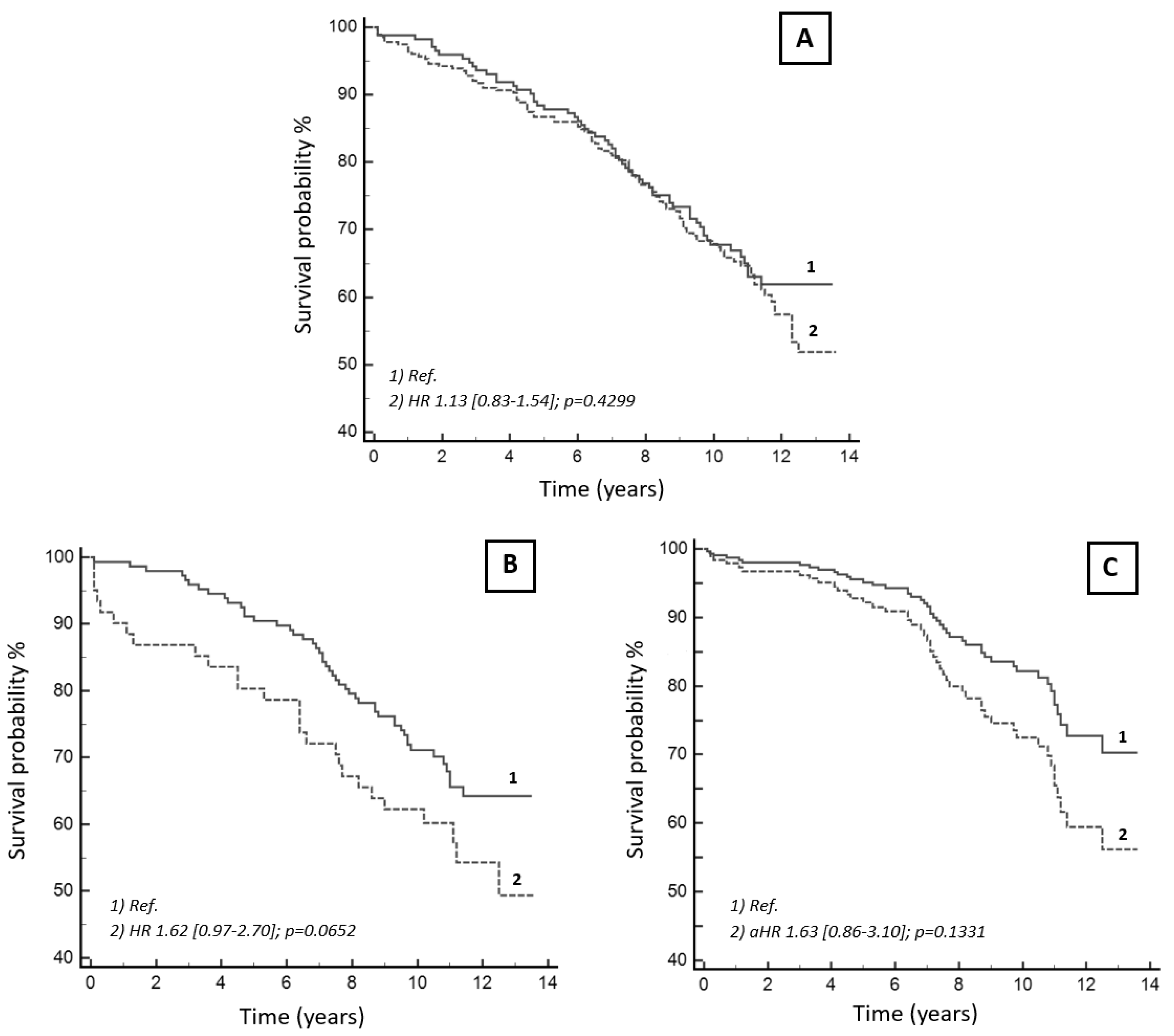
3.3. Univariable Analysis: The Long-Term Prognostic Impact of Atrial Fibrillation
3.4. Multivariable Analysis: Relationship between Atrial Fibrillation and Other Prognostic Variables over a Long-Term Follow-Up
3.5. Prognostic Impact of Oral Anticoagulation Administered at Discharge in Patients with New-Onset Post-Surgical Atrial Fibrillation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Woldendorp, K.; Farag, J.; Khadra, S.; Black, D.; Robinson, B.; Bannon, P. Postoperative atrial fibrillation after cardiac surgery: A meta-analysis. Ann. Thorac. Surg. 2021, 112, 2084–2093. [Google Scholar] [CrossRef] [PubMed]
- Kerwin, M.; Saado, J.; Pan, J.; Ailawadi, G.; Mazimba, S.; Salerno, M.; Mehta, N. New-onset atrial fibrillation and outcomes following isolated coronary artery bypass surgery: A systematic review and meta-analysis. Clin. Cardiol. 2020, 43, 928–934. [Google Scholar] [CrossRef] [PubMed]
- Taha, A.; Nielsen, S.J.; Bergfeldt, L.; Ahlsson, A.; Friberg, L.; Björck, S.; Franzén, S.; Jeppsson, A. New-onset atrial fibrillation after coronary artery bypass grafting and long-term outcome: A population-based nationwide study from the SWEDEHEART registry. J. Am. Heart Assoc. 2021, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Phan, K.; Ha, H.S.K.; Phan, S.; Medi, C.; Thomas, S.P.; Yan, T.D. New-onset atrial fibrillation following coronary bypass surgery predicts long-term mortality: A systematic review and meta-analysis. Eur. J. Cardio-Thorac. Surg. 2015, 48, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Verdecchia, P.; Reboldi, G.; Angeli, F. The 2020 International Society of Hypertension global hypertension practice guidelines-key messages and clinical considerations. Eur. J. Intern. Med. 2020, 82, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, E.D.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Mariscalco, G.; Klersy, C.; Zanobini, M.; Banach, M.; Ferrarese, S.; Borsani, P.; Cantore, C.; Biglioli, P.; Sala, A. Atrial Fibrillation After Isolated Coronary Surgery Affects Late Survival. Circulation 2008, 118, 1612–1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melduni, R.M.; Schaff, H.; Bailey, K.R.; Cha, S.S.; Ammash, N.M.; Seward, J.B.; Gersh, B.J. Implications of new-onset atrial fibrillation after cardiac surgery on long-term prognosis: A community-based study. Am. Heart J. 2015, 170, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, R.; Sanjanwala, R.; Le, M.-L.; Yamashita, M.H.; Arora, R.C. Postoperative Atrial Fibrillation After Cardiac Surgery: A Systematic Review and Meta-Analysis. Ann. Thorac. Surg. 2021, 111, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Schwann, T.A.; Al-Shaar, L.; Engoren, M.C.; Bonnell, M.R.; Goodwin, M.; Schwann, A.N.; Habib, R.H. Effect of new-onset atrial fibrillation on cause-specific late mortality after coronary artery bypass grafting surgery. Eur. J. Cardio-Thorac. Surg. 2018, 54, 294–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.-H.; Kang, D.R.; Uhm, J.-S.; Shim, J.; Sung, J.-H.; Kim, J.-Y.; Pak, H.-N.; Lee, M.-H.; Joung, B. New-onset atrial fibrillation predicts long-term newly developed atrial fibrillation after coronary artery bypass graft. Am. Heart J. 2014, 167, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Pillarisetti, J.; Patel, A.; Bommana, S.; Guda, R.; Falbe, J.; Zorn, G.T.; Muehlebach, G.; Vacek, J.; Lai, S.M.; Lakkireddy, D. Atrial fibrillation following open heart surgery: Long-term incidence and prognosis. J. Interv. Card. Electrophysiol. 2014, 39, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Thorén, E.; Wernroth, M.-L.; Christersson, C.; Grinnemo, K.-H.; Jidéus, L.; Ståhle, E. Compared with matched controls, patients with postoperative atrial fibrillation (POAF) have increased long-term AF after CABG, and POAF is further associated with increased ischemic stroke, heart failure and mortality even after adjustment for AF. Clin. Res. Cardiol. 2020, 109, 1232–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butt, J.H.; Xian, Y.; Peterson, E.D.; Olsen, P.S.; Rørth, R.; Gundlund, A.; Olesen, J.B.; Gislason, G.; Torp-Pedersen, C.; Køber, L.; et al. Long-term Thromboembolic Risk in Patients with Postoperative Atrial Fibrillation After Coronary Artery Bypass Graft Surgery and Patients with Nonvalvular Atrial Fibrillation. JAMA Cardiol. 2018, 3, 417–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butt, J.H.; Olesen, J.B.; Gundlund, A.; Kümler, T.; Olsen, P.S.; Havers-Borgersen, E.; Aagaard, D.T.; Gislason, G.H.; Torp-Pedersen, C.; Køber, L.; et al. Long-term Thromboembolic Risk in Patients with Postoperative Atrial Fibrillation After Left-Sided Heart Valve Surgery. JAMA Cardiol. 2019, 4, 1139–1147. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Overall | Survived | Deceased | p | Univariable Analysis HR [95% CI] | p | |
|---|---|---|---|---|---|---|
| No. of patients (n, %) | 1386 | 913 (66) | 473 (34) | |||
| Age (years) | 65 ± 12 | 62 ± 12 | 72 ± 9 | <0.0001 | 1.09 [1.08–1.10] | <0.0001 |
| Sex F (n, %) | 419 (30) | 257 (28) | 162 (34) | 0.0224 | 1.30 [1.07–1.57] | 0.0072 |
| BMI (kg/m2) | 25 ± 5 | 25 ± 4 | 25 ± 5 | 0.6044 | 0.99 [0.97–1.01] | 0.3792 |
| HTN (n, %) | 869 (65) | 533 (58) | 336 (71) | <0.0001 | 1.56 [1.28–1.90] | <0.0001 |
| Type II DM (n, %) | 290 (21) | 159 (17) | 131 (28) | <0.0001 | 1.66 [1.35–2.02] | <0.0001 |
| Prior history of CAD (n, %) | 894 (64) | 576 (63) | 318 (67) | 0.039 | 1.09 [0.90–1.32] | 0.3670 |
| Prior history of HF (n, %) | 116 (8) | 52 (6) | 64 (13) | <0.0001 | 2.21 [1.70–2.87] | <0.0001 |
| LVEF (%) | 54 ± 10 | 55 ± 10 | 51 ± 12 | <0.0001 | 0.97 [0.96–0.98] | <0.0001 |
| COPD | 91 (7) | 41 (4) | 50 (11) | <0.0001 | 2.11 [1.58–2.82] | <0.0001 |
| AF type before Cardiac Surgery: | ||||||
| Paroxysmal/Persistent AF | 125 (9) | 71 (8) | 54 (11) | <0.0001 | 1.82 [1.35–2.46] | 0.0001 |
| Permanent AF | 83 (6) | 32 (4) | 51 (11) | <0.0001 | 3.48 [2.56–4.73] | <0.0001 |
| Type of cardiac surgery (n, %): | <0.0001 | |||||
| CABG | 655 (47) | 457 (50) | 198 (42) | Ref | ||
| VHS | 495 (36) | 326 (36) | 169 (36) | 1.24 [1.0–1.52] | 0.0413 | |
| Cardiac Transplantation | 31 (2) | 27 (3) | 4 (1) | 0.45 [0.17–1.19] | 0.1097 | |
| PCI plus CABG | 12 (1) | 10 (1) | 2 (0) | 0.51 [0.13–2.05] | 0.3466 | |
| CABG plus VHS | 173 (12) | 82 (9) | 91 (19) | 2.06 [1.61–2.64] | <0.0001 | |
| Others | 20 (2) | 11 (1) | 9 (2) | 1.80 [0.92–3.50] | 0.0852 | |
| POP AF | 539 (39) | 331 (36) | 208 (44) | 0.0001 | 1.53 [1.26–1.85] | <0.0001 |
| New-onset POP AF | 452 (33) | 283 (31) | 169 (36) | <0.0001 | 1.53 [1.24–1.87] | 0.0001 |
| POP complications: | ||||||
| Stroke | 35 (3) | 18 (2) | 17 (4) | 0.1000 | 1.64 [1.01–2.66] | 0.0447 |
| Myocardial Infarction | 31 (2) | 22 (2) | 9 (2) | 0.6792 | 0.87 [0.45–1.68] | 0.6849 |
| Acute HF | 50 (4) | 28 (3) | 22 (5) | 0.1777 | 1.65 [1.07-2.52] | 0.0223 |
| Acute Respiratory Failure | 131 (9) | 85 (9) | 46 (10) | 0.8779 | 1.10 [0.81–1.49] | 0.5367 |
| Acute renal failure | 158 (11) | 101 (11) | 57 (12) | <0.0001 | 2.97 [2.38–3.71] | <0.0001 |
| Infections | 472 (34) | 287 (31) | 185 (39) | 0.0051 | 1.35 [1.12–1.62] | 0.0015 |
| DVT | 158 (11) | 88 (10) | 70 (15) | 0.0055 | 1.43 [1.11–1.84] | 0.0056 |
| Blood tests at admission (rehabilitation program): | ||||||
| POP Creatinine (mg/dL) | 1.26 ± 0.61 | 1.14 ± 0.44 | 1.49 ± 0.81 | <0.0001 | 1.56 [1.45–1.68] | <0.0001 |
| POP Hemoglobin (g/dL) | 11.8 ± 1.19 | 11.9 ± 1.19 | 11.7 ± 1.19 | 0.0417 | 0.91 [0.84–0.98] | 0.0131 |
| POP C-reactive protein (mg/L) | 5.2 ± 4.2 | 4.9 ± 3.9 | 5.7 ± 4.7 | 0.0292 | 1.04 [1.02–1.07] | 0.0014 |
| In-hospital stay (days) | 21 ± 7 | 20 ± 7 | 22 ± 8 | <0.0001 | 1.03 [1.02–1.04] | <0.0001 |
| 6-MWT at discharge (meters) | 426 ± 113 | 727 ± 102 | 340 ± 110 | <0.0001 | 0.99 [0.98–0.99] | <0.0001 |
| Medications after discharge: | ||||||
| VKA oral anticoagulants | 757 (55) | 459 (50) | 298 (63) | <0.0001 | 1.59 [1.32–1.91] | <0.0001 |
| ACE-I | 739 (53) | 458 | 281 | 0.0013 | 1.36 [1.13–1.63] | 0.0010 |
| ARB | 136 (10) | 80 | 56 | 0.0847 | 1.28 [0.97–1.69] | 0.0849 |
| Beta-blockers | 1010 (73) | 685 | 325 | 0.0145 | 0.76 [0.63–0.92] | 0.0055 |
| Antiarrhythmic medications | 353 (25) | 220 | 133 | 0.1177 | 1.21 [0.99–1.48] | 0.0609 |
| Digoxin | 26 (2) | 17 | 9 | 0.8762 | 1.05 [0.55–2.03] | 0.8814 |
| Follow-up: | ||||||
| Average follow-up (years) | 10 ± 3 | 11 ± 1 | 7 ± 3 | <0.0001 | ||
| Follow-up < 1 year (n, %) | 29 (2) | 0 (0) | 29 (6) | <0.0001 |
| POP AF | p | ||
|---|---|---|---|
| No (N = 726) | Yes (N = 539) | ||
| Age (years) | 62 ± 12 | 69 ± 9 | <0.0001 |
| Sex F (n, %) | 172 (23) | 193 (36) | <0.0001 |
| BMI (kg/m2) | 25 ± 5 | 25 ± 5 | 0.3693 |
| HTN (n, %) | 428 (59) | 367 (68) | 0.0009 |
| Type II DM (n, %) | 157 (22) | 113 (21) | 0.7768 |
| Prior history of CAD (n, %) | 515 (71) | 333 (62) | 0.0006 |
| Prior history of HF (n, %) | 45 (6) | 51 (9) | 0.0303 |
| LVEF (%) | 55 ± 10 | 53 ± 11 | 0.0035 |
| COPD | 27 (4) | 52 (10) | <0.0001 |
| Type of cardiac surgery (n, %): | <0.0001 | ||
| CABG | 421 (56) | 217 (40) | |
| VHS | 203 (28) | 209 (39) | |
| Cardiac Transplantation | 27 (4) | 0 (0) | |
| PCI plus CABG | 6 (1) | 4 (1) | |
| CABG plus VHS | 61 (8) | 97 (20) | |
| Others | 8 (1) | 12 (2) | |
| POP complications: | |||
| Stroke | 12 (2) | 20 (4) | 0.0212 |
| Myocardial Infarction | 23 (3) | 7 (1) | 0.0308 |
| Acute HF | 24 (3) | 15 (3) | 0.1777 |
| Acute Respiratory Failure | 66 (9) | 52 (10) | 0.7365 |
| Acute renal failure | 59 (8) | 79 (15) | 0.0002 |
| Infections | 235 (32) | 197 (36) | 0.1212 |
| DVT | 71 (10) | 78 (15) | 0.0105 |
| Blood tests at admission | |||
| POP Creatinine (mg/dL) | 1.20 ± 0.59 | 1.34 ± 0.62 | <0.0001 |
| POP Hemoglobin (g/dL) | 12.0 ± 1.20 | 11.8 ± 1.16 | 0.0313 |
| POP C-reactive protein (mg/L) | 4.9 ± 4.1 | 5.7 ± 4.5 | 0.0043 |
| In-hospital stay (days) | 20 ± 7 | 22 ± 7 | <0.0001 |
| 6-MWT at discharge (meters) | 451 ± 107 | 403 ± 109 | <0.0001 |
| Medications after discharge: | |||
| VKA oral anticoagulants | 285 (39) | 360 (67) | <0.0001 |
| ACE-I | 374 (51) | 297 (55) | 0.2064 |
| ARB | 62 (9) | 61 (11) | 0.1010 |
| Beta-blockers | 563 (78) | 382 (71) | 0.0069 |
| Antiarrhythmic medications | 37 (5) | 294 (54) | <0.0001 |
| Digoxin | 1 (0) | 11 (2) | 0.0006 |
| Follow-up: | |||
| Average follow-up (years) | 10 ± 3 | 9 ± 3 | <0.0001 |
| Follow-up <1 year (n, %) | 15 (2) | 9 (2) | 0.6095 |
| Covariates | Comparison | HR [95% CI] | p |
|---|---|---|---|
| Age | 1-year increase | 1.08 [1.05–1.10] | <0.0001 |
| COPD | Yes vs. No | 1.72 [1.05–2.82] | 0.0309 |
| History of HF | Yes vs. No | 1.79 [1.10–2.93] | 0.0194 |
| LVEF | 1% increase | 0.98 [0.97–0.99] | 0.0448 |
| Serum creatinine at admission | 1 mg/dL increase | 1.43 [1.13–1.80] | 0.0026 |
| 6-MWT at discharge | 1 m increase | 0.98 [0.97–0.99] | 0.0031 |
| Atrial fibrillation groups (Group 1 as reference) | |||
| Group 2 | Group 1 | 1.31 [0.90–1.89] | 0.1609 |
| Group 3 | Group 1 | 1.33 [0.71–2.49] | 0.3736 |
| Group 4 | Group 1 | 1.55 [0.82–2.95] | 0.1803 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marazzato, J.; Masnaghetti, S.; De Ponti, R.; Verdecchia, P.; Blasi, F.; Ferrarese, S.; Trapasso, M.; Spanevello, A.; Angeli, F. Long-Term Survival in Patients with Post-Operative Atrial Fibrillation after Cardiac Surgery: Analysis from a Prospective Cohort Study. J. Cardiovasc. Dev. Dis. 2021, 8, 169. https://doi.org/10.3390/jcdd8120169
Marazzato J, Masnaghetti S, De Ponti R, Verdecchia P, Blasi F, Ferrarese S, Trapasso M, Spanevello A, Angeli F. Long-Term Survival in Patients with Post-Operative Atrial Fibrillation after Cardiac Surgery: Analysis from a Prospective Cohort Study. Journal of Cardiovascular Development and Disease. 2021; 8(12):169. https://doi.org/10.3390/jcdd8120169
Chicago/Turabian StyleMarazzato, Jacopo, Sergio Masnaghetti, Roberto De Ponti, Paolo Verdecchia, Federico Blasi, Sandro Ferrarese, Monica Trapasso, Antonio Spanevello, and Fabio Angeli. 2021. "Long-Term Survival in Patients with Post-Operative Atrial Fibrillation after Cardiac Surgery: Analysis from a Prospective Cohort Study" Journal of Cardiovascular Development and Disease 8, no. 12: 169. https://doi.org/10.3390/jcdd8120169
APA StyleMarazzato, J., Masnaghetti, S., De Ponti, R., Verdecchia, P., Blasi, F., Ferrarese, S., Trapasso, M., Spanevello, A., & Angeli, F. (2021). Long-Term Survival in Patients with Post-Operative Atrial Fibrillation after Cardiac Surgery: Analysis from a Prospective Cohort Study. Journal of Cardiovascular Development and Disease, 8(12), 169. https://doi.org/10.3390/jcdd8120169