


Autonomic Nervous System Control in Male and Female Elite Soccer Players: Importance of Different Training Routines and Perceived Stress
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Evaluation
2.2. Study of the Cardiac Autonomic Control (CAR)
2.3. Evaluation of Stress Perception
2.4. Statistics
3. Results
3.1. Cardiac Autonomic Regulation (CAR) and Anthropometrics Data
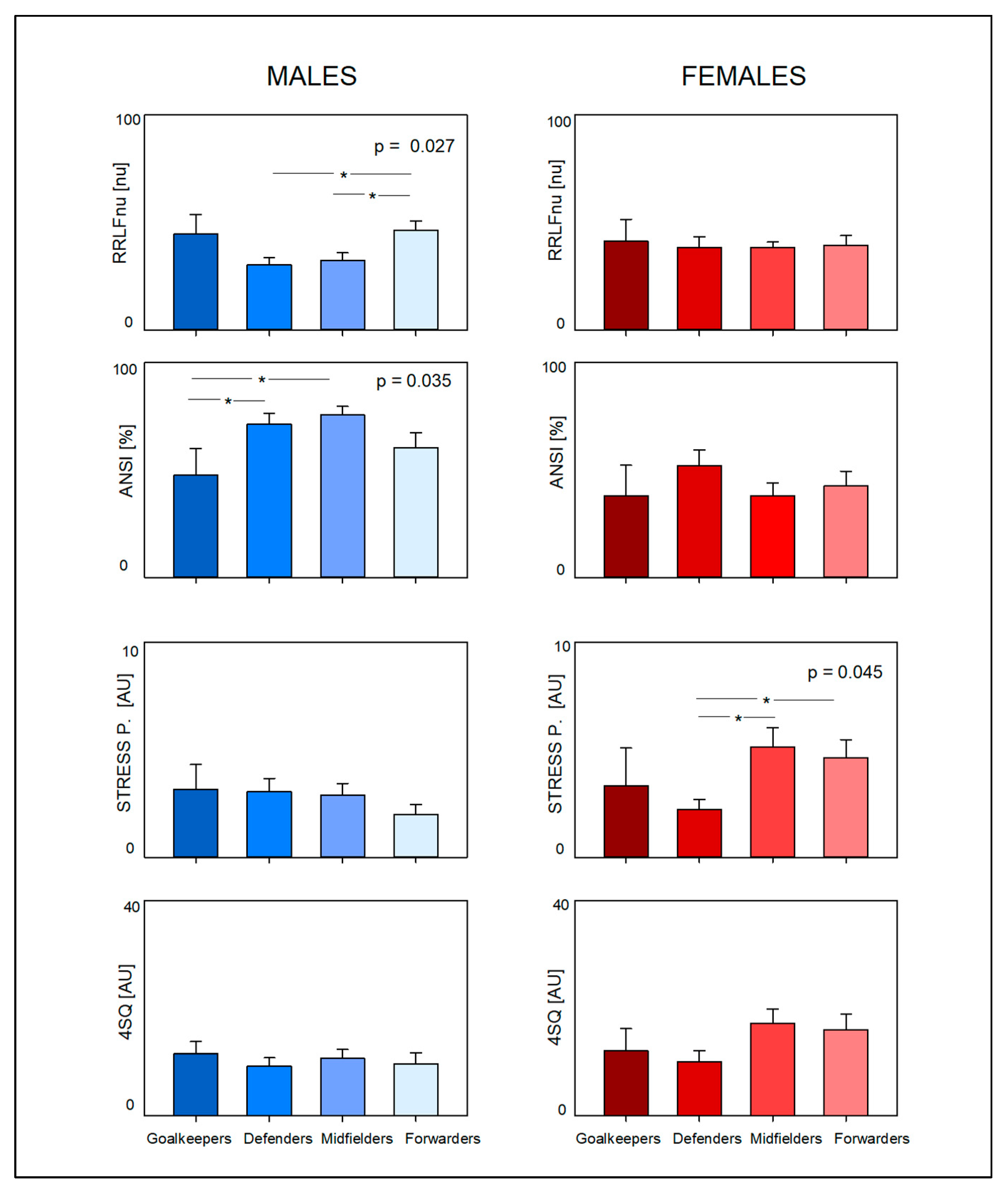
3.2. Stress and Somatic Symptoms Perception Data (See Table 1, Table 2, Table 3 and Table 4 and Figure 1)

{kind=link}
| Variable | Goalkeepers | Defenders | Midfielders | Forwards | p | |
|---|---|---|---|---|---|---|
| N | 3 | 14 | 15 | 11 | ||
| Age | [yrs] | 22.33 ± 5.13 | 20.64 ± 5.51 | 19.33 ± 4.40 | 20.82 ± 6.29 | 0.782 |
| Weight | [kg] | 63.67 ± 9.02 | 57.04 ± 5.37 | 54.70 ± 7.86 | 55.91 ± 8.34 | 0.288 |
| Height | [cm] | 171 ± 7 | 166 ± 5 | 163 ± 7 | 164 ± 5 | 0.152 |
| BMI | [kg/m2] | 25.49 ± 2.96 | 24.68 ± 1.49 | 24.70 ± 2.91 | 24.63 ± 2.69 | 0.928 |
| SAP | [mmHg] | 108.33 ± 14.43 | 109.14 ± 11.39 | 109.13 ± 10.60 | 108.55 ± 7.83 | 0.998 |
| DAP | [mmHg] | 68.33 ± 14.43 | 62.79 ± 9.17 | 63.80 ± 9.91 | 63.09 ± 8.38 | 0.832 |
| HR | [beat/min] | 61.43 ± 3.94 | 59.42 ± 7.92 | 63.14 ± 9.47 | 64.94 ± 10.10 | 0.472 |
| RR | [ms] | 979 ± 65 | 1027± 140 | 969 ± 136 | 942 ± 135 | 0.460 |
| RR VAR | [ms2] | 9611 ± 12,562 | 5982 ± 2744 | 7213 ± 5687 | 5604 ± 2795 | 0.572 |
| RR LFa | [ms2] | 2172 ± 2147 | 1699 ± 1516 | 1950 ± 1809 | 1474 ± 1018 | 0.844 |
| RR HFa | [ms2] | 4502 ± 6802 | 2408 ± 1769 | 2971 ± 2590 | 2142 ± 1697 | 0.510 |
| RR LFnu | [nu] | 41.34 ± 17.63 | 38.26 ± 18.67 | 38.40 ± 9.70 | 39.55 ± 14.72 | 0.986 |
| RR HFnu | [nu] | 46.46 ± 26.04 | 52.52 ± 19.27 | 52.95 ± 15.94 | 51.58 ± 15.60 | 0.949 |
| RR LF/HF | 1.55 ± 1.76 | 1.71 ± 3.81 | 0.89 ± 0.61 | 1.00 ± 0.95 | 0.780 | |
| ANSI | [%] | 38.18 ± 24.43 | 51.95 ± 27.12 | 37.95 ± 23.90 | 42.61 ± 22.83 | 0.479 |
| Stress P score | [AU] | 3.33 ± 3.06 | 2.21 ± 1.81 | 5.13 ± 3.48 * | 4.64 ± 2.77 * | 0.045 |
| Fatigue P score | [AU] | 4.00 ± 2.65 | 2.79 ± 1.93 | 4.53 ± 2.67 | 3.00 ± 2032 | 0.205 |
| 4SQ score | [AU] | 12.00 ± 7.21 | 10.00 ± 7.64 | 17.20 ± 10.25 | 16.00 ± 9.52 | 0.176 |
4. Discussion
4.1. Cardiac Autonomic Regulation (CAR)
4.2. Stress Perception
4.3. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CAR | Cardiac autonomic regulation |
| HRV | Heart rate variability |
| N | Number |
| BMI | Body mass index |
| RR | RR interval |
| HR | Heart rate |
| V | Variability |
| RR VAR | Total Power of RR interval variability (variance) |
| LF | Low-frequency component of RR variability |
| an | Absolute value |
| HF | High-frequency component of RR variability |
| nu | Normalized unit |
| SAP | Systolic arterial pressure |
| DAP | Diastolic arterial pressure |
| ANSI | Autonomic Nervous System Index |
| P | Perception |
| AU | Arbitrary units |
| 4SQ | Short somatic symptoms stress-related questionnaire |
References
- Kunz, M. Big Count: 265 Million Playing Football. FIFA Mag. 2007, 7, 11–15. [Google Scholar]
- Wragg, M. FIFA Magazine Nielsen Sport. 2018, pp. 10–13. Available online: https://nielsensports.com/wpcontent/uploads/2014/12/Nielsen_World-Football-2018-6.11.18.pdf (accessed on 17 January 2020).
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Joyner, M.J.; Green, D.J. Exercise Protects the Cardiovascular System: Effects beyond Traditional Risk Factors. J. Physiol. 2009, 587, 5551–5558. [Google Scholar] [CrossRef]
- Lucini, D.; Luconi, E.; Giovanelli, L.; Marano, G.; Bernardelli, G.; Guidetti, R.; Morello, E.; Cribellati, S.; Brambilla, M.M.; Biganzoli, E.M. Assessing Lifestyle in a Large Cohort of Undergraduate Students: Significance of Stress, Exercise and Nutrition. Nutrients 2024, 16, 4339. [Google Scholar] [CrossRef]
- Mitchell, J.J.; Bu, F.; Fancourt, D.; Steptoe, A.; Bone, J.K. Longitudinal Associations between Physical Activity and Other Health Behaviours during the COVID-19 Pandemic: A Fixed Effects Analysis. Sci. Rep. 2022, 12, 15956. [Google Scholar] [CrossRef]
- Douwes, R.; Metselaar, J.; Pijnenborg, G.H.M.; Boonstra, N. Well-Being of Students in Higher Education: The Importance of a Student Perspective. Cogent Educ. 2023, 10, 2190697. [Google Scholar] [CrossRef]
- Ligibel, J.A.; Bohlke, K.; May, A.M.; Clinton, S.K.; Demark-Wahnefried, W.; Gilchrist, S.C.; Irwin, M.L.; Late, M.; Mansfield, S.; Marshall, T.F.; et al. Exercise, Diet, and Weight Management during Cancer Treatment: ASCO Guideline. J. Clin. Oncol. 2022, 348, 2491–2507. [Google Scholar] [CrossRef]
- Linee Guida e Raccomandazioni. Available online: https://www.epicentro.iss.it/attivita_fisica/linee-indirizzo-2021 (accessed on 5 April 2025).
- Gielen, S.; Schuler, G.; Adams, V. Cardiovascular Effects of Exercise Training: Molecular Mechanisms. Circulation 2010, 122, 1221–1238. [Google Scholar] [CrossRef]
- Grassi, G.; Mark, A.; Esler, M. The Sympathetic Nervous System Alterations in Human Hypertension. Circ. Res. 2015, 116, 976–990. [Google Scholar] [CrossRef]
- El-Tahlawi, M. How Do You Prevent “Sudden Death” during Sports Activities? e-J. Cardiol. Pract. 2021, 19, 17–31. [Google Scholar]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on Sports Cardiology and Exercise in Patients with Cardiovascular Disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef]
- Fanous, Y.; Dorian, P. The Prevention and Management of Sudden Cardiac Arrest in Athletes. CMAJ 2019, 191, E787–E791. [Google Scholar] [CrossRef]
- Finocchiaro, G.; Westaby, J.; Sheppard, M.N.; Papadakis, M.; Sharma, S. Sudden Cardiac Death in Young Athletes: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2024, 83, 350–370. [Google Scholar] [CrossRef]
- Sala, R.; Malacarne, M.; Solaro, N.; Pagani, M.; Lucini, D. A Composite Autonomic Index as Unitary Metric for Heart Rate Variability: A Proof of Concept. Eur. J. Clin. Investig. 2017, 47, 241–249. [Google Scholar] [CrossRef]
- Lucini, D.; Marchetti, I.; Spataro, A.; Malacarne, M.; Benzi, M.; Tamorri, S.; Sala, R.; Pagani, M. Heart Rate Variability to Monitor Performance in Elite Athletes: Criticalities and Avoidable Pitfalls. Int. J. Cardiol. 2017, 240, 307–312. [Google Scholar] [CrossRef]
- Sala, R.; Malacarne, M.; Tosi, F.; Benzi, M.; Solaro, N.; Tamorri, S.; Spataro, A.; Pagani, M.; Lucini, D. May a Unitary Autonomic Index Help Assess Autonomic Cardiac Regulation in Elite Athletes? Preliminary Observations on the National Italian Olympic Committee Team. J. Sports Med. Phys. Fitness 2017, 57, 1702–1710. [Google Scholar] [CrossRef] [PubMed]
- Solaro, N.; Malacarne, M.; Pagani, M.; Lucini, D. Cardiac Baroreflex, HRV, and Statistics: An Interdisciplinary Approach in Hypertension. Front. Physiol. 2019, 10, 444572. [Google Scholar] [CrossRef] [PubMed]
- Lucini, D.; Malacarne, M.; Gatzemeier, W.; Pagani, M. A Simple Home-Based Lifestyle Intervention Program to Improve Cardiac Autonomic Regulation in Patients with Increased Cardiometabolic Risk. Sustainability 2020, 12, 7671. [Google Scholar] [CrossRef]
- Lucini, D.; Galiuto, L.; Malacarne, M.; Meucci, M.C.; Pagani, M. Cardiac Autonomic Effects of Yearly Athletic Retreats on Elite Basket Players: Usefulness of a Unitary Autonomic Nervous System Indicator. Sustainability 2021, 13, 2330. [Google Scholar] [CrossRef]
- Lucini, D.; Fallanca, A.; Malacarne, M.; Casasco, M.; Galiuto, L.; Pigozzi, F.; Galanti, G.; Pagani, M. Streamlining Analysis of RR Interval Variability in Elite Soccer Players: Preliminary Experience with a Composite Indicator of Cardiac Autonomic Regulation. Int. J. Environ. Res. Public Health 2020, 17, 1844. [Google Scholar] [CrossRef] [PubMed]
- Solaro, N.; Pagani, M.; Lucini, D. Altered Cardiac Autonomic Regulation in Overweight and Obese Subjects: The Role of Age-and-Gender-Adjusted Statistical Indicators of Heart Rate Variability and Cardiac Baroreflex. Front. Physiol. 2021, 11, 567312. [Google Scholar] [CrossRef] [PubMed]
- Lucini, D.; Spataro, A.; Giovanelli, L.; Malacarne, M.; Spada, R.; Parati, G.; Solaro, N.; Pagani, M. Relationship between Body Composition and Cardiac Autonomic Regulation in a Large Population of Italian Olympic Athletes. J. Pers. Med. 2022, 12, 1508. [Google Scholar] [CrossRef]
- Lucini, D.; Sala, R.; Spataro, A.; Malacarne, M.; Benzi, M.; Tamorri, S.; Pagani, M. Can the Use of a Single Integrated Unitary Autonomic Index Provide Early Clues for Eventual Eligibility for Olympic Games? Eur. J. Appl. Physiol. 2018, 118, 919–926. [Google Scholar] [CrossRef]
- McEwen, B.S.; Akil, H. Revisiting the Stress Concept: Implications for Affective Disorders. J. Neurosci. 2020, 40, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Henningsen, P.; Zipfel, S.; Herzog, W. Management of Functional Somatic Syndromes. Lancet 2007, 369, 946–955. [Google Scholar] [CrossRef]
- Kivimäki, M.; Pentti, J.; Ferrie, J.E.; Batty, G.D.; Nyberg, S.T.; Jokela, M.; Virtanen, M.; Alfredsson, L.; Dragano, N.; Fransson, E.I.; et al. Work Stress and Risk of Death in Men and Women with and without Cardiometabolic Disease: A Multicohort Study. Lancet Diabetes Endocrinol. 2018, 6, 705–713. [Google Scholar] [CrossRef]
- Bart, R.; Ishak, W.W.; Ganjian, S.; Jaffer, K.Y.; Abdelmesseh, M.; Hanna, S.; Gohar, Y.; Azar, G.; Vanle, B.; Dang, J.; et al. The Assessment and Measurement of Wellness in the Clinical Medical Setting: A Systematic Review. Innov. Clin. Neurosci. 2018, 15, 14. [Google Scholar]
- Herbert, C. Enhancing Mental Health, Well-Being and Active Lifestyles of University Students by Means of Physical Activity and Exercise Research Programs. Front. Public Health 2022, 10, 849093. [Google Scholar] [CrossRef]
- Lazarus, R.S. How Emotions Influence Performance in Competitive Sports. Sport. Psychol. 2000, 14, 229–252. [Google Scholar] [CrossRef]
- Song, Z.; Baicker, K. Effect of a Workplace Wellness Program on Employee Health and Economic Outcomes: A Randomized Clinical Trial. JAMA 2019, 321, 1491–1501. [Google Scholar] [CrossRef]
- Schnermann, M.E.; Schulz, C.A.; Ludwig, C.; Alexy, U.; Nöthlings, U. A Lifestyle Score in Childhood and Adolescence Was Positively Associated with Subsequently Measured Fluid Intelligence in the DONALD Cohort Study. Eur. J. Nutr. 2022, 61, 3719–3729. [Google Scholar] [CrossRef]
- Bosquet, L.; Merkari, S.; Arvisais, D.; Aubert, A.E. Is Heart Rate a Convenient Tool to Monitor Over-Reaching? A Systematic Review of the Literature. Br. J. Sports Med. 2008, 42, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Krishna Bandi, H.; Keerthi, S.G.; Reddy, M.N.; Singh, M.S.B. Spectral Analysis of Short Term Heart Rate Variability in Healthy Volunteers: The Role of Gender. Int. J. Sci. Res. Publ. 2012, 2, 399. [Google Scholar]
- Lucini, D.; Solaro, N.; Lesma, A.; Gillet, V.B.; Pagani, M. Health Promotion in the Workplace: Assessing Stress and Lifestyle with an Intranet Tool. J. Med. Internet Res. 2011, 13, e88. [Google Scholar] [CrossRef]
- Lucini, D.; Riva, S.; Pizzinelli, P.; Pagani, M. Stress Management at the Worksite: Reversal of Symptoms Profile and Cardiovascular Dysregulation. Hypertension 2007, 49, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect Size Estimates: Current Use, Calculations, and Interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef]
- Coote, J.H. Myths and Realities of the Cardiac Vagus. J. Physiol. 2013, 591, 4073–4085. [Google Scholar] [CrossRef]
- Plews, D.J.; Laursen, P.B.; Stanley, J.; Kilding, A.E.; Buchheit, M. Training Adaptation and Heart Rate Variability in Elite Endurance Athletes: Opening the Door to Effective Monitoring. Sports Med. 2013, 43, 773–781. [Google Scholar] [CrossRef]
- White, D.W.; Raven, P.B. Autonomic Neural Control of Heart Rate during Dynamic Exercise: Revisited. J. Physiol. 2014, 592, 2491–2500. [Google Scholar] [CrossRef]
- Smith, D.L.; Horn, G.P.; Petruzzello, S.J.; Freund, G.G.; Bloom, S.I.; Fernhall, B. Hemostatic Responses to Multiple Bouts of Firefighting Activity: Female vs. Male Differences in a High Demand, High Performance Occupation. Int. J. Environ. Res. Public Health 2022, 19, 2124. [Google Scholar] [CrossRef] [PubMed]
- Strath, S.J.; Kaminsky, L.A.; Ainsworth, B.E.; Ekelund, U.; Freedson, P.S.; Gary, R.A.; Richardson, C.R.; Smith, D.T.; Swartz, A.M. Guide to the Assessment of Physical Activity: Clinical and Research Applications: A Scientific Statement from the American Heart Association. Circulation 2013, 128, 2259–2279. [Google Scholar] [CrossRef]
- Manzi, V.; Iellamo, F.; Impellizzeri, F.; D’Ottavio, S.; Castagna, C. Relation between Individualized Training Impulses and Performance in Distance Runners. Med. Sci. Sports Exerc. 2009, 41, 2090–2096. [Google Scholar] [CrossRef] [PubMed]
- Iellamo, F.; Legramante, J.M.; Pigozzi, F.; Spataro, A.; Norbiato, G.; Lucini, D.; Pagani, M. Conversion from Vagal to Sympathetic Predominance with Strenuous Training in High-Performance World Class Athletes. Circulation 2002, 105, 2719–2724. [Google Scholar] [CrossRef]
- Kivimäki, M.; Steptoe, A. Effects of Stress on the Development and Progression of Cardiovascular Disease. Nat. Rev. Cardiol. 2018, 15, 215–229. [Google Scholar] [CrossRef] [PubMed]
- Purvis, D.; Gonsalves, S.; Deuster, P.A. Physiological and Psychological Fatigue in Extreme Conditions: Overtraining and Elite Athletes. Phys. Med. Rehabil. 2010, 2, 442–450. [Google Scholar] [CrossRef]
- Mirto, M.; Filipas, L.; Altini, M.; Codella, R.; Meloni, A. Heart Rate Variability in Professional and Semiprofessional Soccer: A Scoping Review. Scand. J. Med. Sci. Sports 2024, 34, e14673. [Google Scholar] [CrossRef]
- Hayano, J.; Yuda, E. Pitfalls of Assessment of Autonomic Function by Heart Rate Variability. J. Physiol. Anthropol. 2019, 38, 3. [Google Scholar] [CrossRef]
- Beissner, F.; Meissner, K.; Bär, K.J.; Napadow, V. The Autonomic Brain: An Activation Likelihood Estimation Meta-Analysis for Central Processing of Autonomic Function. J. Neurosci. 2013, 33, 10503–10511. [Google Scholar] [CrossRef]
- Pagani, M.; Lombardi, F.; Guzzetti, S.; Rimoldi, O.; Furlan, R.; Pizzinelli, P.; Sandrone, G.; Malfatto, G.; Dell’Orto, S.; Piccaluga, E. Power Spectral Analysis of Heart Rate and Arterial Pressure Variabilities as a Marker of Sympatho-Vagal Interaction in Man and Conscious Dog. Circ. Res. 1986, 59, 178–193. [Google Scholar] [CrossRef]
- Hess, W.R. Nobel Lecture. In Nobel Lectures, Physiology or Medicine (1942–1962); Elsevier: Amsterdam, The Netherlands, 1949. [Google Scholar]
- Malik, M.; Camm, A.J.; Bigger, J.T.; Breithardt, G.; Cerutti, S.; Cohen, R.J.; Coumel, P.; Fallen, E.L.; Kennedy, H.L.; Kleiger, R.E.; et al. Heart Rate Variability. Standards of Measurement, Physiological Interpretation, and Clinical Use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef]
- Saleem, S.H.M. Gender Differences of Heart Rate Variability in Healthy Volunteers. J. Pak. Med. Assoc. 2012, 62, 422–425. [Google Scholar]
- Reimann, M.; Friedrich, C.; Gasch, J.; Reichmann, H.; Rüdiger, H.; Ziemssen, T. Trigonometric Regressive Spectral Analysis Reliably Maps Dynamic Changes in Baroreflex Sensitivity and Autonomic Tone: The Effect of Gender and Age. PLoS ONE 2010, 5, e12187. [Google Scholar] [CrossRef]
- Fu, Q. Sex Differences in Autonomic Function. In Primer on the Autonomic Nervous System, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2023; pp. 267–272. [Google Scholar] [CrossRef]
- McQuilliam, S.J.; Clark, D.R.; Erskine, R.M.; Brownlee, T.E. Mind the Gap! A Survey Comparing Current Strength Training Methods Used in Men’s versus Women’s First Team and Academy Soccer. Sci. Med. Footb. 2022, 6, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, C.; Hoppe, M.W.; Freiwald, J. Different Endurance Characteristics of Female and Male German Soccer Players. Biol. Sport. 2014, 31, 227–232. [Google Scholar] [CrossRef] [PubMed]
- McFadden, B.A.; Walker, A.J.; Bozzini, B.N.; Sanders, D.J.; Arent, S.M. Comparison of Internal and External Training Loads in Male and Female Collegiate Soccer Players During Practices vs. Games. J. Strength. Cond. Res. 2020, 34, 969–974. [Google Scholar] [CrossRef]
- Burfeind, K.; Hong, J.; Stavrianeas, S. Gender Differences in the Neuromuscular Fitness Profiles of NCAA Division III Soccer Players. Isokinet. Exerc. Sci. 2012, 20, 115–120. [Google Scholar] [CrossRef]
- Nunome, H.; Drust, B.; Dawson, B. Science and Football VII: The Proceedings of the Seventh World Congress on Science and Football. In Science and Football VII: The Proceedings of the Seventh World Congress on Science and Football; Routledge: London, UK, 2013; pp. 1–432. [Google Scholar] [CrossRef]
- Hunter, S.K.; Angadi, S.S.; Bhargava, A.; Harper, J.; Hirschberg, A.L.; Levine, B.D.; Moreau, K.L.; Nokoff, N.J.; Stachenfeld, N.S.; Bermon, S. The Biological Basis of Sex Differences in Athletic Performance: Consensus Statement for the American College of Sports Medicine. Med. Sci. Sports Exerc. 2023, 55, 2328–2360. [Google Scholar] [CrossRef]
- Mujika, I.; Santisteban, J.; Impellizzeri, F.M.; Castagna, C. Fitness Determinants of Success in Men’s and Women’s Football. J. Sports Sci. 2009, 27, 107–114. [Google Scholar] [CrossRef]
- J Helgerud, J.H.U.W. Gender Differences in Strength and Endurance of Elite Soccer Players. In Science and Football IV; Routledge: London, UK, 2013. [Google Scholar]
- Gioldasis, A. Technical Skills According to Playing Position of Male and Female Soccer Players. Int. J. Sci. Cult. Sport 2017, 5, 293–301. [Google Scholar] [CrossRef]
- Garnica-Caparrós, M.; Memmert, D. Understanding Gender Differences in Professional European Football through Machine Learning Interpretability and Match Actions Data. Sci. Rep. 2021, 11, 10805. [Google Scholar] [CrossRef]
- Pappalardo, L.; Rossi, A.; Natilli, M.; Cintia, P. Explaining the Difference between Men’s and Women’s Football. PLoS ONE 2021, 16, e0255407. [Google Scholar] [CrossRef] [PubMed]
- Gullett, N.; Zajkowska, Z.; Walsh, A.; Harper, R.; Mondelli, V. Heart Rate Variability (HRV) as a Way to Understand Associations between the Autonomic Nervous System (ANS) and Affective States: A Critical Review of the Literature. Int. J. Psychophysiol. 2023, 192, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Pelliccia, A. The Heart of Trained Athletes: Cardiac Remodeling and the Risks of Sports, Including Sudden Death. Circulation 2006, 114, 1633–1644. [Google Scholar] [CrossRef] [PubMed]
- Lochbaum, M.; Stoner, E.; Hefner, T.; Cooper, S.; Lane, A.M.; Terry, P.C. Sport Psychology and Performance Meta-Analyses: A Systematic Review of the Literature. PLoS ONE 2022, 17, e0263408. [Google Scholar] [CrossRef]
- Leblanc, V.R. The Effects of Acute Stress on Performance: Implications for Health Professions Education. Acad. Med. 2009, 84, S25–S33. [Google Scholar] [CrossRef]
- La Rovere, M.T.; Gorini, A.; Schwartz, P.J. Stress, the Autonomic Nervous System, and Sudden Death. Auton. Neurosci. 2022, 237, 102921. [Google Scholar] [CrossRef]
- Sheppard, M.N. Aetiology of Sudden Cardiac Death in Sport: A Histopathologist’s Perspective. Br. J. Sports Med. 2012, 46 (Suppl. S1), i15–i21. [Google Scholar] [CrossRef]
- Putukian, M. The Psychological Response to Injury in Student Athletes: A Narrative Review with a Focus on Mental Health. Br. J. Sports Med. 2016, 50, 145–148. [Google Scholar] [CrossRef]
- Gustafsson, H.; Sagar, S.S.; Stenling, A. Fear of Failure, Psychological Stress, and Burnout among Adolescent Athletes Competing in High Level Sport. Scand. J. Med. Sci. Sports 2017, 27, 2091–2102. [Google Scholar] [CrossRef]
- Nicholls, A.R.; Gustafsson, H.; Gerber, M.; Nixdorf, I.; Beckmann, J.; Nixdorf, R. Psychological Predictors for Depression and Burnout Among German Junior Elite Athletes. Front. Psychol. 2020, 11, 601. [Google Scholar] [CrossRef]
- Kim, H.G.; Cheon, E.J.; Bai, D.S.; Lee, Y.H.; Koo, B.H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Pagani, E.; Gavazzoni, N.; Bernardelli, G.; Malacarne, M.; Solaro, N.; Giusti, E.; Castelnuovo, G.; Volpi, P.; Carimati, G.; Lucini, D. Psychological Intervention Based on Mental Relaxation to Manage Stress in Female Junior Elite Soccer Team: Improvement in Cardiac Autonomic Control, Perception of Stress and Overall Health. Int. J. Environ. Res. Public Health 2023, 20, 942. [Google Scholar] [CrossRef] [PubMed]
- Krygier, J.R.; Heathers, J.A.J.; Shahrestani, S.; Abbott, M.; Gross, J.J.; Kemp, A.H. Mindfulness Meditation, Well-Being, and Heart Rate Variability: A Preliminary Investigation into the Impact of Intensive Vipassana Meditation. Int. J. Psychophysiol. 2013, 89, 305–313. [Google Scholar] [CrossRef]
- Brown, L.; Rando, A.A.; Eichel, K.; Van Dam, N.T.; Celano, C.M.; Huffman, J.C.; Morris, M.E. The Effects of Mindfulness and Meditation on Vagally Mediated Heart Rate Variability: A Meta-Analysis. Psychosom. Med. 2021, 83, 631–640. [Google Scholar] [CrossRef]
- Russo, M.A.; Santarelli, D.M.; O’Rourke, D. The Physiological Effects of Slow Breathing in the Healthy Human. Breathe 2017, 13, 298–309. [Google Scholar] [CrossRef]
- Kirk, U.; Axelsen, J.L. Heart Rate Variability Is Enhanced during Mindfulness Practice: A Randomized Controlled Trial Involving a 10-Day Online-Based Mindfulness Intervention. PLoS ONE 2020, 15, e0243488. [Google Scholar] [CrossRef]
- Bernardi, L.; Sleight, P.; Bandinelli, G.; Cencetti, S.; Fattorini, L.; Wdowczyc-Szulc, J.; Lagi, A. Effect of Rosary Prayer and Yoga Mantras on Autonomic Cardiovascular Rhythms: Comparative Study. BMJ 2001, 323, 1446–1449. [Google Scholar] [CrossRef]
- Iellamo, D.; Pigozzi, F.; Spataro, A. Autonomic and Psychological Adaptations in Olympic Rowers. J. Sports Med. Phys. Fit. 2006, 46, 598–604. [Google Scholar]
- Button, K.S.; Ioannidis, J.P.A.; Mokrysz, C.; Nosek, B.A.; Flint, J.; Robinson, E.S.J.; Munafò, M.R. Power Failure: Why Small Sample Size Undermines the Reliability of Neuroscience. Nat. Rev. Neurosci. 2013, 14, 365–376. [Google Scholar] [CrossRef]
| Variable | All | Males | Females | p | Cohen’s d | |
|---|---|---|---|---|---|---|
| N | 117 | 74 | 43 | |||
| Age | [yrs] | 20.54 ± 4.36 | 20.65 ± 3.81 | 20.35 ± 5.22 | 0.74 | −0.07 |
| Weight | [kg] | 68.63 ± 11.54 | 75.74 ± 6.39 | 56.40 ± 7.41 * | 0.00 | −2.85 |
| Height | [cm] | 175 ± 0.11 | 182 ± 0.07 | 165 ± 50.06 * | 0.00 | −2.63 |
| BMI | [Kg/m2] | 25.23 ± 2.08 | 25.52 ± 1.84 | 24.73 ± 2.39 * | 0.03 | 0.48 |
| SAP | [mmHg] | 119.65 ± 15.99 | 125.88 ± 15.5 | 108.93 ± 10.11 * | 0.00 | −1.23 |
| DAP | [mmHg] | 67.91 ± 9.08 | 70.41 ± 7.97 | 63.60 ± 9.34 * | 0.00 | −0.8 |
| HR | [beat/min] | 56.41 ± 10.33 | 53.00 ± 9.59 | 62.27 ± 8.90 * | 0.00 | 0.99 |
| RR | [ms] | 1098 ± 198 | 1166 ± 198 | 981 ± 134 * | 0.00 | −1.04 |
| RR VAR | [ms2] | 8839 ± 12,474 | 10,159 ± 15,128 | 6568 ± 4864 | 0.06 | −0.29 |
| RR LFa | [ms2] | 1975 ± 2138 | 2098 ± 2427 | 1762 ± 1522 | 0.36 | −0.16 |
| RR HFa | [ms2] | 4078 ± 8187 | 4889 ± 10,049 | 2682 ± 2542 | 0.08 | −0.27 |
| RR LFnu | [nu] | 36.88 ± 17.56 | 35.74 ± 19.17 | 38.85 ± 14.37 | 0.32 | 0.18 |
| RR HFnu | [nu] | 57.39 ± 19.41 | 60.53 ± 20.08 | 52.01 ± 17.10 * | 0.02 | −0.45 |
| RR LF/HF | 1.04 ± 1.70 | 0.93 ± 1.70 | 1.23 ± 2.26 | 0.43 | 0.18 | |
| ANSI | [%] | 59.34 ± 27.97 | 68.42 ± 25.81 | 43.71 ± 24.65 * | 0.00 | −0.97 |
| Stress P score | [AU] | 3.31 ± 2.70 | 2.82 ± 2.36 | 3.93 ± 3.00 * | 0.05 | 0.42 |
| Fatigue P score | [AU] | 3.37 ± 2.11 | 3.24 ± 1.87 | 3.53 ± 2.40 | 0.50 | 0.14 |
| 4SQ score | [AU] | 11.89 ± 8.19 | 10.09 ± 6.71 | 14.19 ± 9.35 * | 0.02 | 0.51 |
| Variable | Goalkeepers | Defenders | Midfielders | Forwards | p | |
|---|---|---|---|---|---|---|
| N | 10 | 39 | 42 | 26 | ||
| Age | [yrs] | 19.57 ± 4.04 | 19.22 ± 3.85 | 21.30 ± 5.14 | 20.20 ± 3.59 | 0.651 |
| Weight | [kg] | 78.10 ± 11.28 | 70.32 ± 11.50 | 66.17 ± 10.51 * | 66.42 ± 11.60 * | 0.014 |
| Height | [cm] | 184 ± 0.10 | 177 ± 0.11 * | 173 ± 0.10 * | 174 ± 0.11 * | 0.019 |
| BMI | [kg/m2] | 25.20 ± 1.87 | 25.35 ± 1.89 | 25.37 ± 2.26 | 24.81 ± 2.20 | 0.824 |
| SAP | [mmHg] | 117.50 ± 14.19 | 119.99 ± 15.10 | 121.52 ± 18.66 | 117.08 ± 13.44 | 0.701 |
| DAP | [mmHg] | 68.60 ± 9.70 | 66.74 ± 9.25 | 68.76 ± 9.07 | 68.00 ± 8.95 | 0.788 |
| HR | [beat/min] | 60.21 ± 10.67 | 55.78 ± 10.27 | 54.74 ± 10.25 | 58.59 ± 10.25 | 0.291 |
| RR | [ms] | 1026 ± 191 | 1110 ± 201 | 1132 ± 205 | 1054 ± 181 | 0.258 |
| RR VAR | [ms2] | 5759 ± 6806 | 8511 ± 7488 | 9110 ± 8422 | 10,078 ± 22,319 | 0.826 |
| RR LFa | [ms2] | 1315 ± 1284 | 1896 ± 1802 | 2035 ± 1779 | 2247 ± 3197 | 0.697 |
| RR HFa | [ms2] | 2352 ± 3640 | 3864 ± 4990 | 4296 ± 5692 | 4709 ± 14,611 | 0.887 |
| RR LFnu | [nu] | 43.67 ± 21.42 | 33.21 ± 17.91 | 34.59 ± 15.93 | 43.49 ± 16.36 | 0.053 |
| RR HFnu | [nu] | 50.28 ± 22.53 | 60.58 ± 19.91 | 60.56 ± 18.33 | 50.24 ± 17.46 | 0.068 |
| RR LF/HF | 1.61 ± 1.95 | 1.01 ± 2.34 | 0.78 ± 0.85 | 1.27 ± 1.48 | 0.470 | |
| ANSI | [%] | 44.77 ± 29.51 | 64.37 ± 27.09 | 62.15 ± 28.33 | 52.87 ± 26.53 | 0.121 |
| Stress P score | [AU] | 3.22 ± 2.68 | 2.69 ± 2.28 | 3.83 ± 3.08 | 3.38 ± 2.58 | 0.384 |
| Fatigue P score | [AU] | 4.56 ± 2.01 | 2.78 ± 1.93 * | 3.83 ± 2.26 | 2.95 ± 1.88 | 0.046 |
| 4SQ score | [AU] | 11.67 ± 5.66 | 9.56 ± 7.02 | 13.39 ± 9.15 | 12.95 ± 8.69 | 0.247 |
| Variable | Goalkeepers | Defenders | Midfielders | Forwards | p | |
|---|---|---|---|---|---|---|
| N | 7 | 25 | 27 | 15 | ||
| Age | [yrs] | 22.14 ± 5.6 | 20.00 ± 3.4 | 21.11 ± 3.87 | 20.20 ± 3.59 | 0.501 |
| Weight | [kg] | 84.29 ± 3.86 | 77.76 ± 5.78 * | 72.54 ± 4.79 +* | 74.13 ± 6.35 +* | 0.000 |
| Height | [cm] | 190 ± 0.03 | 183 ± 0.08 * | 179 ± 0.05 +* | 182 ± 0.07 * | 0.001 |
| BMI | [kg/m2] | 25.08 ± 1.52 | 25.73 ± 2.01 | 25.75 ± 1.76 | 24.93 ± 1.85 | 0.369 |
| SAP | [mmHg] | 121.43 ± 13.14 | 125.92 ± 13.62 | 128.41 ± 18.73 | 123.33 ± 13.40 | 0.646 |
| DAP | [mmHg] | 68.71 ± 8.46 | 68.96 ± 8.71 | 71.52 ± 7.40 | 71.60 ± 7.75 | 0.581 |
| HR | [beat/min] | 59.69 ± 12.83 | 53.74 ± 11.00 | 50.07 ± 7.36 | 53.93 ± 7.73 | 0.099 |
| RR | [ms] | 1046 ± 227 | 1158 ± 216 | 1223 ± 179 | 1135 ± 170 | 0.156 |
| RR VAR | [ms2] | 4107 ± 2507 | 9927 ± 8881 | 10,164 ± 9550 | 13,360 ± 29,269 | 0.624 |
| RR LFa | [ms2] | 948 ± 643 | 2006 ± 1966 | 2083 ± 1795 | 2814 ± 4086 | 0.411 |
| RR HFa | [ms2] | 1430 ± 1073 | 4860 ± 5983 | 5033 ± 6775 | 6592 ± 19,241 | 0.743 |
| RR LFnu | [nu] | 44.68 ± 24.10 | 30.38 ± 17.19 | 32.48 ± 18.35 | 46.38 ± 17.38 +# | 0.027 |
| RR HFnu | [nu] | 51.92 ± 22.92 | 65.10 ± 19.16 | 64.78 ± 18.47 | 49.25 ± 19.18 +# | 0.033 |
| RR LF/HF | 1.63 ± 2.15 | 0.63 ± 0.61 | 0.72 ± 0.96 | 1.47 ± 1.78 | 0.068 | |
| ANSI | [%] | 47.60 ± 32.80 | 71.33 ± 24.95 * | 75.19 ± 20.80 * | 60.40 ± 27.22 | 0.035 |
| Stress P score | [AU] | 3.17 ± 2.79 | 3.06 ± 2.58 | 2.90 ± 2.45 | 2.00 ± 1.49 | 0.683 |
| Fatigue P score | [AU] | 4.83 ± 1.83 | 2.78 ± 1.99 | 3.33 ± 1.83 | 2.90 ± 1.37 | 0.115 |
| 4SQ score | [AU] | 11.50 ± 5.5 | 9.22 ± 6.71 | 10.67 ± 7.37 | 9.60 ± 6.59 | 0.863 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oggionni, G.; Pagani, E.; Rizzardini, J.; Rigillo, M.; Giovanelli, L.; Malacarne, M.; Loureiro, N.; Ribeiro, J.M.; Volpi, P.; Pagani, M.; et al. Autonomic Nervous System Control in Male and Female Elite Soccer Players: Importance of Different Training Routines and Perceived Stress. J. Cardiovasc. Dev. Dis. 2025, 12, 150. https://doi.org/10.3390/jcdd12040150
Oggionni G, Pagani E, Rizzardini J, Rigillo M, Giovanelli L, Malacarne M, Loureiro N, Ribeiro JM, Volpi P, Pagani M, et al. Autonomic Nervous System Control in Male and Female Elite Soccer Players: Importance of Different Training Routines and Perceived Stress. Journal of Cardiovascular Development and Disease. 2025; 12(4):150. https://doi.org/10.3390/jcdd12040150
Chicago/Turabian StyleOggionni, Gianluigi, Eleonora Pagani, Jacopo Rizzardini, Margherita Rigillo, Luca Giovanelli, Mara Malacarne, Nuno Loureiro, Júlia Machado Ribeiro, Piero Volpi, Massimo Pagani, and et al. 2025. "Autonomic Nervous System Control in Male and Female Elite Soccer Players: Importance of Different Training Routines and Perceived Stress" Journal of Cardiovascular Development and Disease 12, no. 4: 150. https://doi.org/10.3390/jcdd12040150
APA StyleOggionni, G., Pagani, E., Rizzardini, J., Rigillo, M., Giovanelli, L., Malacarne, M., Loureiro, N., Ribeiro, J. M., Volpi, P., Pagani, M., & Lucini, D. (2025). Autonomic Nervous System Control in Male and Female Elite Soccer Players: Importance of Different Training Routines and Perceived Stress. Journal of Cardiovascular Development and Disease, 12(4), 150. https://doi.org/10.3390/jcdd12040150