
Assessing the Risk of Hypertension in Chronic, Elderly Patients during the COVID-19 Pandemic: A Prospective Study
 , ,
, ,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Eligibility Criteria and Procedure
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Sample Description
3.2. Exploratory Analysis for Classification
3.2.1. Univariate Graphical Exploratory Analysis
3.2.2. Bivariate Graphical Exploratory Analysis
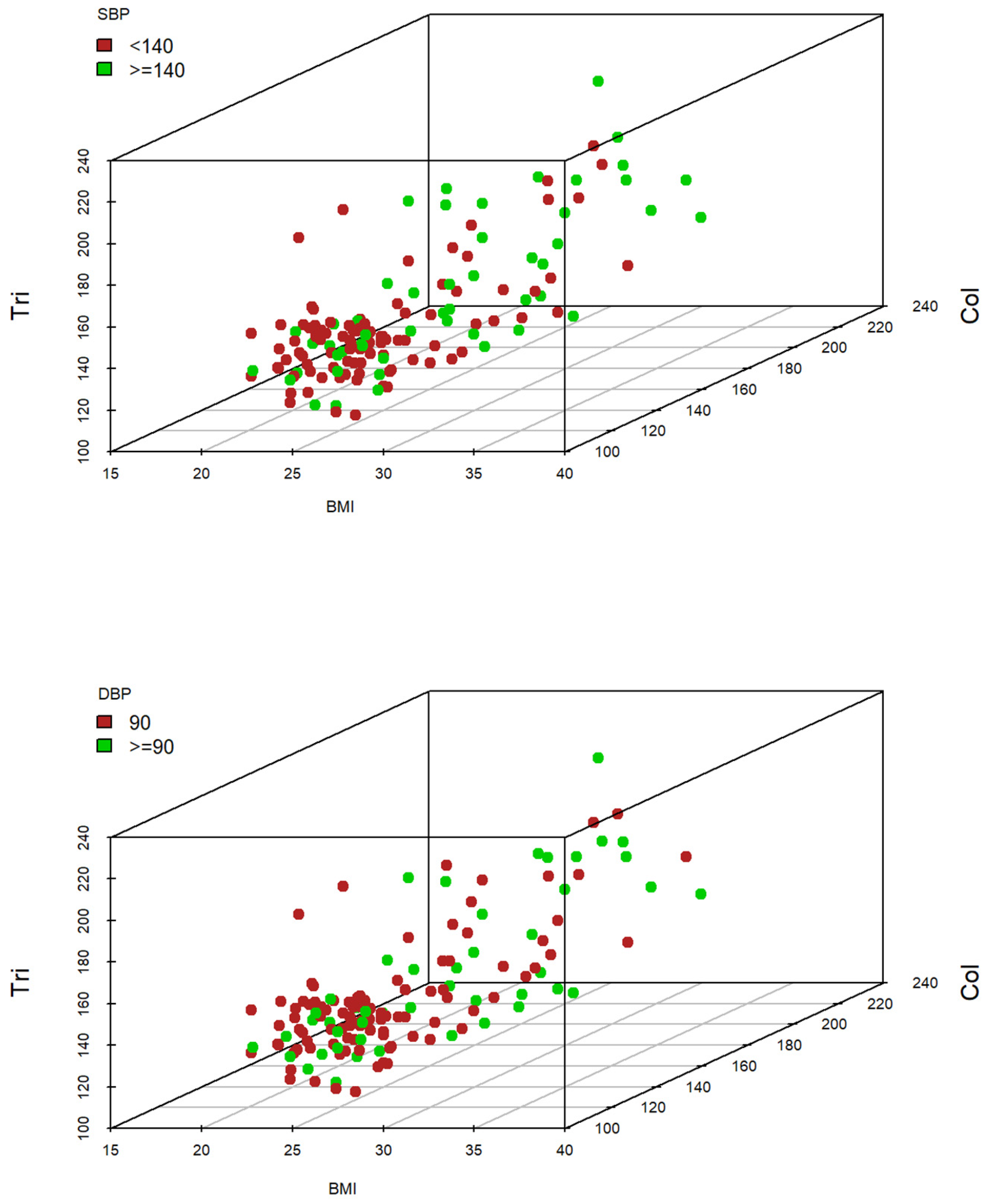
3.2.3. Three-Subscale Graphical Exploratory Analysis
3.3. Logit Model to Predict Systolic and Diastolic AHT Level at T2 Based on Sociodemographic and Clinical Variables at T1
3.4. Logit Model to Predict Systolic and Diastolic AHT Level at T3 Based on Sociodemographic and Clinical Variables at T2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mostaza, J.M.; Pintó, X.; Armario, P.; Masana, L.; Real, J.T.; Valdivielso, P.; Arrobas-Velilla, T.; Baeza-Trinidad, R.; Calmarza, P.; Cebollada, J.; et al. SEA 2022 Standards for Global Control of Cardiovascular Risk. Clin. Investig. Arterioscler. 2022, 34, 130–179. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596. [Google Scholar] [CrossRef] [PubMed]
- Gorostidi, M.; Gijón-Conde, T.; De la Sierra, A.; Rodilla, E.; Rubio, E.; Vinyoles, E.; Oliveras, A.; Santamaría, R.; Segura, J.; Molinero, A.; et al. Guía práctica sobre el diagnóstico y tratamiento de la hipertensión arterial en España, 2022. Sociedad Española de Hipertensión–Liga Española para la Lucha contra la Hipertensión Arterial (SEH-LELHA). Hipertens. Riesgo Vasc. 2022, 39, 174–194. [Google Scholar] [CrossRef] [PubMed]
- Quesada-Caballero, M.; Carmona-García, A.; Chami-Peña, S.; Albendín-García, L.; Membrive-Jiménez, C.; Romero-Béjar, J.L.; la Fuente, G.A.C.-D. COVID-19 and the Use of Angiotensin II Receptor Blockers in Older Chronic Hypertensive Patients: Systematic Review and Meta-Analysis. Medicina 2023, 59, 1200. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-S.; Pei, Y.-H.; Gu, Y.-Y.; Zhu, J.-F.; Yu, P.; Chen, X.-H. Association between short-term exposure to ambient air pollution and heart failure: An updated systematic review and meta-analysis of more than 7 million participants. Front. Public Health 2023, 10, 948765. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J.; Miller, G.C.; Britt, H. What are chronic conditions that contribute to multimorbidity? Aust. J. Gen. Pract. 2018, 47, 21–22. [Google Scholar] [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Ott, C.; Schmieder, R.E. Diagnosis and treatment of arterial hypertension 2021. Kidney Int. 2022, 101, 36–46. [Google Scholar] [CrossRef]
- Adler, A.; Agodoa, L.; Algra, A.; Asselbergs, F.W.; Beckett, N.S.; Berge, E.; Black, H.; Brouwers, F.P.J.; Brown, M.; Bulpitt, C.J.; et al. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: An individual participant-level data meta-analysis. Lancet 2021, 397, 1625–1636. [Google Scholar] [CrossRef]
- Benetos, A.; Petrovic, M.; Strandberg, T. Hypertension Management in Older and Frail Older Patients. Circ. Res. 2019, 124, 1045–1060. [Google Scholar] [CrossRef]
- Carey, R.M.; Wright, J.T.; Taler, S.J.; Whelton, P.K. Guideline-Driven Management of Hypertension: An Evidence-Based Update. Circ. Res. 2021, 128, 827–846. [Google Scholar] [CrossRef] [PubMed]
- Ajabnoor, G.M.A.; Bahijri, S.; Alamoudi, A.A.; Al Raddadi, R.; Al-Ahmadi, J.; Jambi, H.; Borai, A.; Toumilehto, J. The association between hypertension and other cardiovascular risk factors among non-diabetic Saudis adults-A cross sectional study. PLoS ONE 2021, 16, e0246568. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- CDC. How to Protect Yourself and Others. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html (accessed on 22 October 2023).
- Guillem, F.C. Opportunities and threats for prevention and health promotion and the PAPPS in the context of the COVID-19 pandemic. Aten. Primaria 2020, 52, 449–451. [Google Scholar] [CrossRef]
- Quesada-Caballero, M.; Carmona-García, A.; Chami-Peña, S.; Caballero-Mateos, A.M.; Fernández-Martín, O.; Cañadas-De la Fuente, G.A.; Romero-Bejar, J.L. Telemedicine in Elderly Hypertensive and Patients with Chronic Diseases during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 6160. [Google Scholar] [CrossRef] [PubMed]
- Paice, J.A. Cancer pain during an epidemic and a pandemic. Curr. Opin. Support. Palliat. Care 2022, 16, 55–59. [Google Scholar] [CrossRef]
- García-Lara, R.A.; Suleiman-Martos, N.; Membrive-Jiménez, M.J.; García-Morales, V.; Quesada-Caballero, M.; Guisado-Requena, I.M.; Gómez-Urquiza, J.L. Prevalence of Depression and Related Factors among Patients with Chronic Disease during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 3094. [Google Scholar] [CrossRef] [PubMed]
- Agresti, A. Foundations of Linear and Generalized Linear Models; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2015; p. 473. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Chaput, J.-P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5–17 years: Summary of the evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef]
- Eckstrom, E.; Neukam, S.; Kalin, L.; Wright, J. Physical Activity and Healthy Aging. Clin. Geriatr. Med. 2020, 36, 671–683. [Google Scholar] [CrossRef]
- Bellettiere, J.; LaMonte, M.J.; Evenson, K.R.; Rillamas-Sun, E.; Kerr, J.; Lee, I.-M.; Di, C.; Rosenberg, D.E.; Stefanick, M.L.; Buchner, D.M.; et al. Sedentary Behavior and Cardiovascular Disease in Older Women: The OPACH Study. Circulation 2019, 139, 1036–1046. [Google Scholar] [CrossRef] [PubMed]
- Hermelink, R.; Leitzmann, M.F.; Markozannes, G.; Tsilidis, K.; Pukrop, T.; Berger, F.; Baurecht, H.; Jochem, C. Sedentary behavior and cancer–an umbrella review and meta-analysis. Eur. J. Epidemiol. 2022, 37, 447–460. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef] [PubMed]
- NHS. Physical Activity Guidelines for Older Adults. Available online: https://www.nhs.uk/live-well/exercise/exercise-guidelines/physical-activity-guidelines-older-adults/ (accessed on 22 October 2023).
- CDC. How Much Physical Activity do Older Adults Need? Physical Activity. Available online: https://www.cdc.gov/physicalactivity/basics/older_adults/index.htm (accessed on 22 October 2023).
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Gotanda, H.; Liyanage-Don, N.; Moran, A.E.; Krousel-Wood, M.; Green, J.B.; Zhang, Y.; Nuckols, T.K. Changes in Blood Pressure Outcomes Among Hypertensive Individuals During the COVID-19 Pandemic: A Time Series Analysis in Three US Healthcare Organizations. Hypertension 2022, 79, 2733–2742. [Google Scholar] [CrossRef]
- Nozato, Y.; Yamamoto, K.; Rakugi, H. Hypertension management before and under the COVID-19 pandemic: Lessons and future directions. Hypertens. Res. 2023, 46, 1471–1477. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Descriptive Analysis of Sociodemographic Information | ||||
|---|---|---|---|---|
| Variable | Levels | % (N) | ||
| Sex (N = 148) | (0) Male | 33.8 (50) | ||
| (1) Female | 66.2 (98) | |||
| Marital Status (N = 148) | (0) Married | 56.1 (83) | ||
| (1) Single | 18.2 (27) | |||
| (2) Widowed | 25.7 (38) | |||
| Variable | Mean (SD) | |||
| Age (N = 148) | 81.6 (9.65) | |||
| Descriptive Analysis of Clinical Information | ||||
| Variable | Mean (SD)-T1 | Mean (SD)-T2 | Mean (SD)-T3 | |
| Hb1Ac (N = 148) | 6.2 (1.54) | 6.2 (1.60) | 6.2 (1.64) | |
| AHT_SBP (N = 148) | 123.7 (17.42) | 127.3 (15.51) | 128.8 (18.33) | |
| AHT_DBP (N = 148) | 77.7 (10.41) | 79.5 (11.83) | 77.7 (10.41) | |
| HR (N = 148) | 75.0 (11.35) | 75.4 (10.55) | 75.5 (11.09) | |
| BMI (N = 148) | 25.8 (3.44) | 25.8 (3.51) | 25.7 (3.56) | |
| Tri (N = 148) | 144.2 (23.16) | 148.7 (28.68) | 152.6 (26.96) | |
| Chol (N = 148) | 143.3 (24.86) | 140.2 (25.02) | 147.0 (27.76) | |
| LDL (N = 148) | 100.6 (25.08) | 108.5 (29.26) | 112.2 (33.07) | |
| HDL (N = 148) | 47.9 (10.92) | 48.4 (11.46) | 46.5 (11.07) | |
| AHT Variables after Segmentation and Coding | ||||
| Variable | Levels | % (N)-T1 | % (N)-T2 | % (N)-T3 |
| ATH_SBP (N = 148) | (0) <140 mmHg | 73.0 (108) | 64.2 (95) | 54.7 (81) |
| (1) ≥140 mmHg | 27.0 (40) | 35.8 (53) | 45.3 (67) | |
| ATH_DBP (N = 148) | (0) <90 mmHg | 82.4 (122) | 67.6 (100) | 58.8 (87) |
| (1) ≥90 mmHg | 17.6 (26) | 32.4 (48) | 41.2 (61) | |
| Prediction for Systolic AHT Level at T2 | |||||||
|---|---|---|---|---|---|---|---|
| Subscale | B | SD | Z | p | OR | CI for 95% OR | |
| Lower | Upper | ||||||
| Constant | −7.06 | 1.88 | −3.75 | <0.001 | |||
| 0.03 | 0.02 | 1.77 | 0.076 | 1.03 | 0.99 | 1.06 | |
| 0.16 | 0.05 | 2.96 | 0.003 | 1.17 | 1.05 | 1.31 | |
| Prediction for Diastolic AHT Level at T2 | |||||||
| Subscale | B | SD | Z | p | OR | CI for 95% OR | |
| Lower | Upper | ||||||
| Constant | −10.17 | 2.17 | −4.69 | <0.001 | |||
| −0.69 | 0.40 | −1.73 | 0.084 | 0.50 | 0.23 | 1.09 | |
| 0.06 | 0.02 | 3.24 | 0.001 | 1.06 | 1.02 | 1.11 | |
| 0.14 | 0.06 | 2.29 | 0.022 | 1.15 | 1.02 | 1.31 | |
| 0.01 | 0.01 | 1.56 | 0.118 | 1.01 | 1.00 | 1.03 | |
| Prediction for Systolic AHT Level at T3 | |||||||
|---|---|---|---|---|---|---|---|
| Subscale | B | SD | Z | p | OR | CI for 95% OR | |
| Lower | Upper | ||||||
| Constant | −7.35 | 1.94 | −3.79 | <0.001 | |||
| 0.03 | 0.02 | 1.53 | 0.127 | 1.03 | 0.99 | 1.06 | |
| 0.11 | 0.06 | 1.79 | 0.074 | 1.17 | 0.99 | 1.27 | |
| Tri | 0.02 | 0.01 | 2.00 | 0.045 | 1.02 | 1.00 | 1.03 |
| Prediction for Diastolic AHTLevel at T3 | |||||||
| Subscale | B | SD | Z | p | OR | CI for 95% OR | |
| Lower | Upper | ||||||
| Constant | −4.74 | 1.34 | −3.51 | <0.001 | |||
| 0.17 | 0.05 | 3.29 | 0.001 | 1.17 | 0.99 | 1.27 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quesada-Caballero, M.; Carmona-García, A.; García-Lara, R.A.; Caballero-Mateos, A.M.; Suleiman-Martos, N.; Cañadas-De la Fuente, G.A.; Romero-Béjar, J.L. Assessing the Risk of Hypertension in Chronic, Elderly Patients during the COVID-19 Pandemic: A Prospective Study. J. Cardiovasc. Dev. Dis. 2024, 11, 21. https://doi.org/10.3390/jcdd11010021
Quesada-Caballero M, Carmona-García A, García-Lara RA, Caballero-Mateos AM, Suleiman-Martos N, Cañadas-De la Fuente GA, Romero-Béjar JL. Assessing the Risk of Hypertension in Chronic, Elderly Patients during the COVID-19 Pandemic: A Prospective Study. Journal of Cardiovascular Development and Disease. 2024; 11(1):21. https://doi.org/10.3390/jcdd11010021
Chicago/Turabian StyleQuesada-Caballero, Miguel, Ana Carmona-García, Rubén A. García-Lara, Antonio M. Caballero-Mateos, Nora Suleiman-Martos, Guillermo A. Cañadas-De la Fuente, and José L. Romero-Béjar. 2024. "Assessing the Risk of Hypertension in Chronic, Elderly Patients during the COVID-19 Pandemic: A Prospective Study" Journal of Cardiovascular Development and Disease 11, no. 1: 21. https://doi.org/10.3390/jcdd11010021
APA StyleQuesada-Caballero, M., Carmona-García, A., García-Lara, R. A., Caballero-Mateos, A. M., Suleiman-Martos, N., Cañadas-De la Fuente, G. A., & Romero-Béjar, J. L. (2024). Assessing the Risk of Hypertension in Chronic, Elderly Patients during the COVID-19 Pandemic: A Prospective Study. Journal of Cardiovascular Development and Disease, 11(1), 21. https://doi.org/10.3390/jcdd11010021