

Three Decades of Experience with Aortic Prosthetic Valve Endocarditis

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Demography
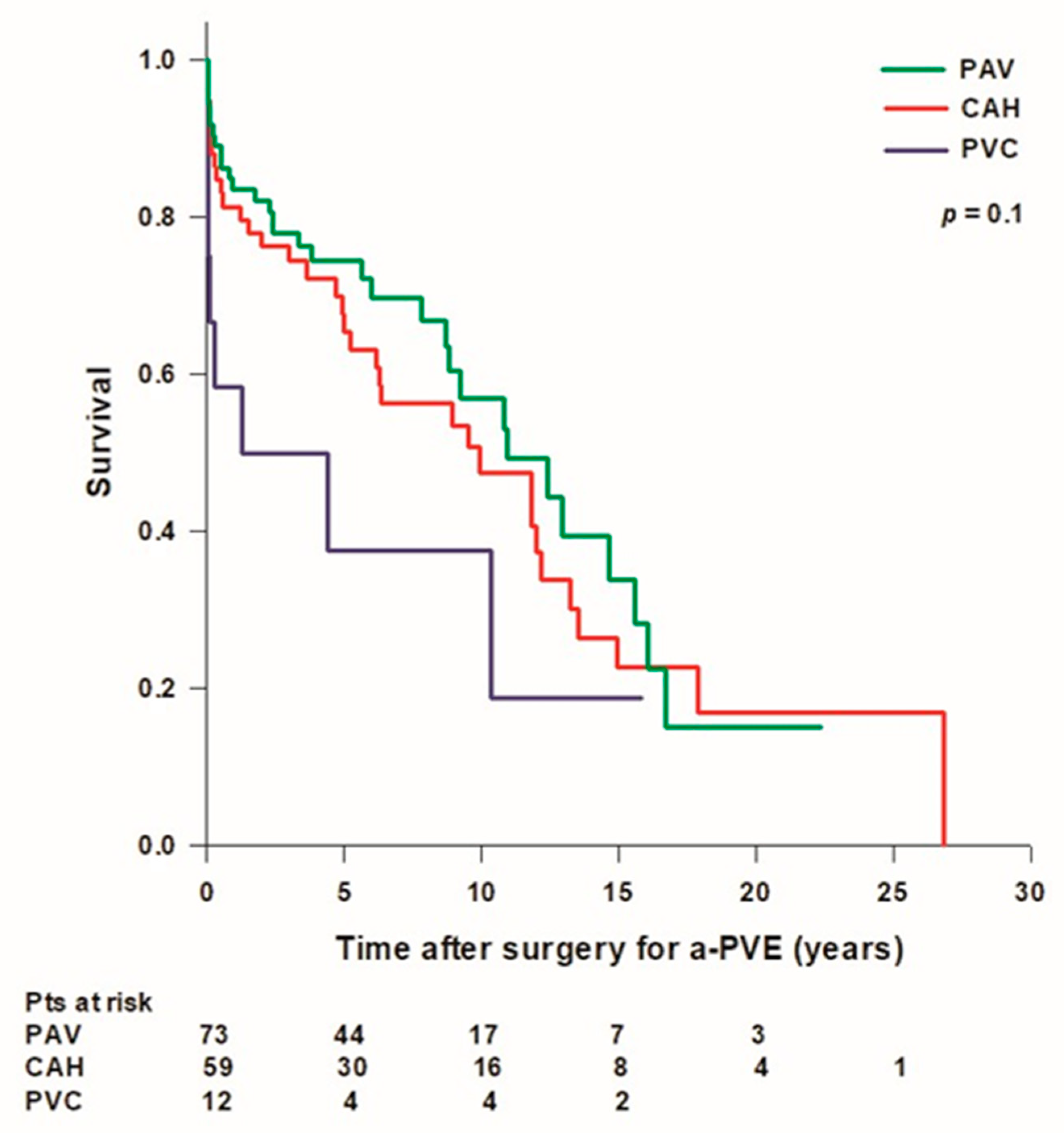
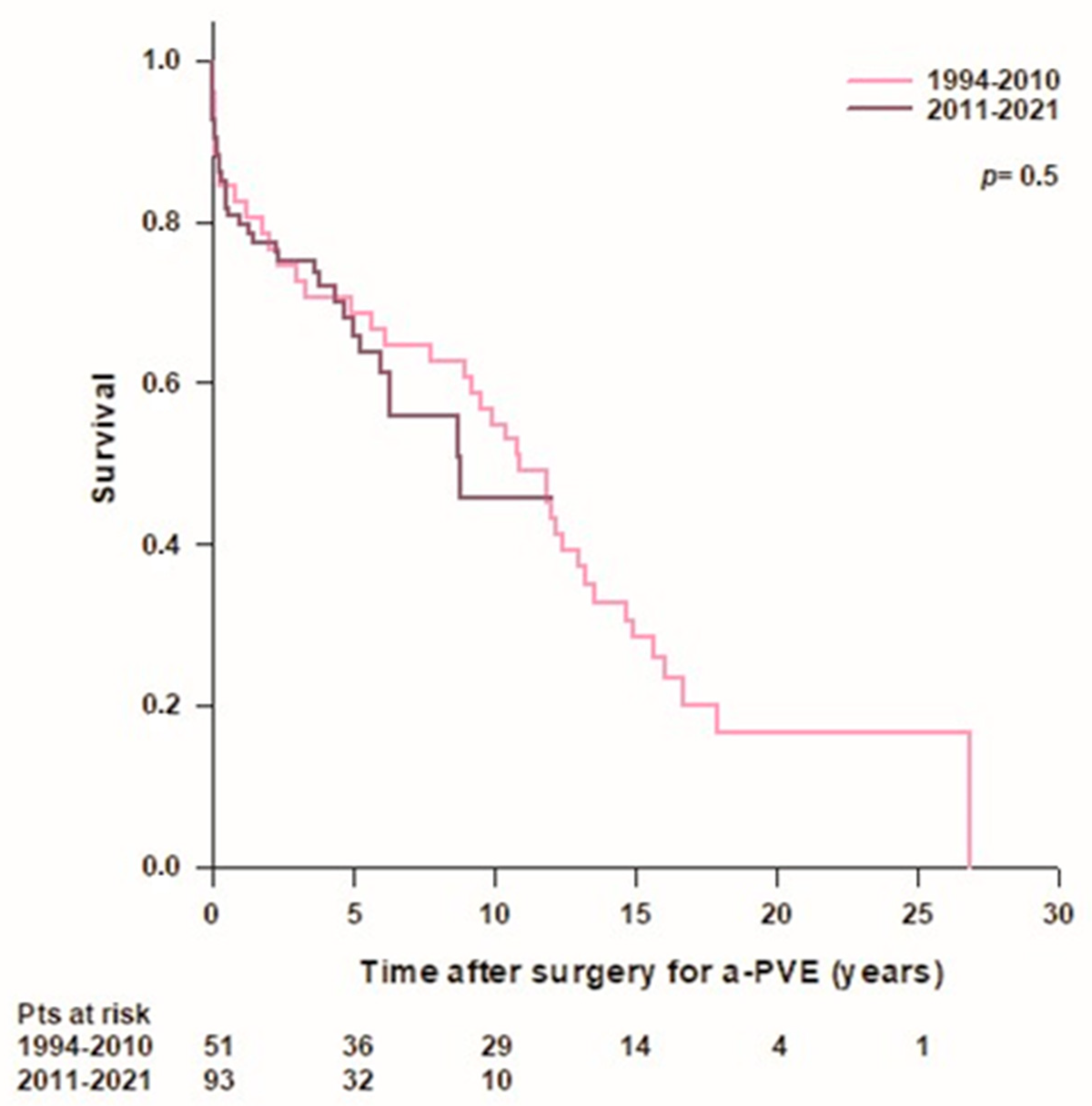
3.2. Survival
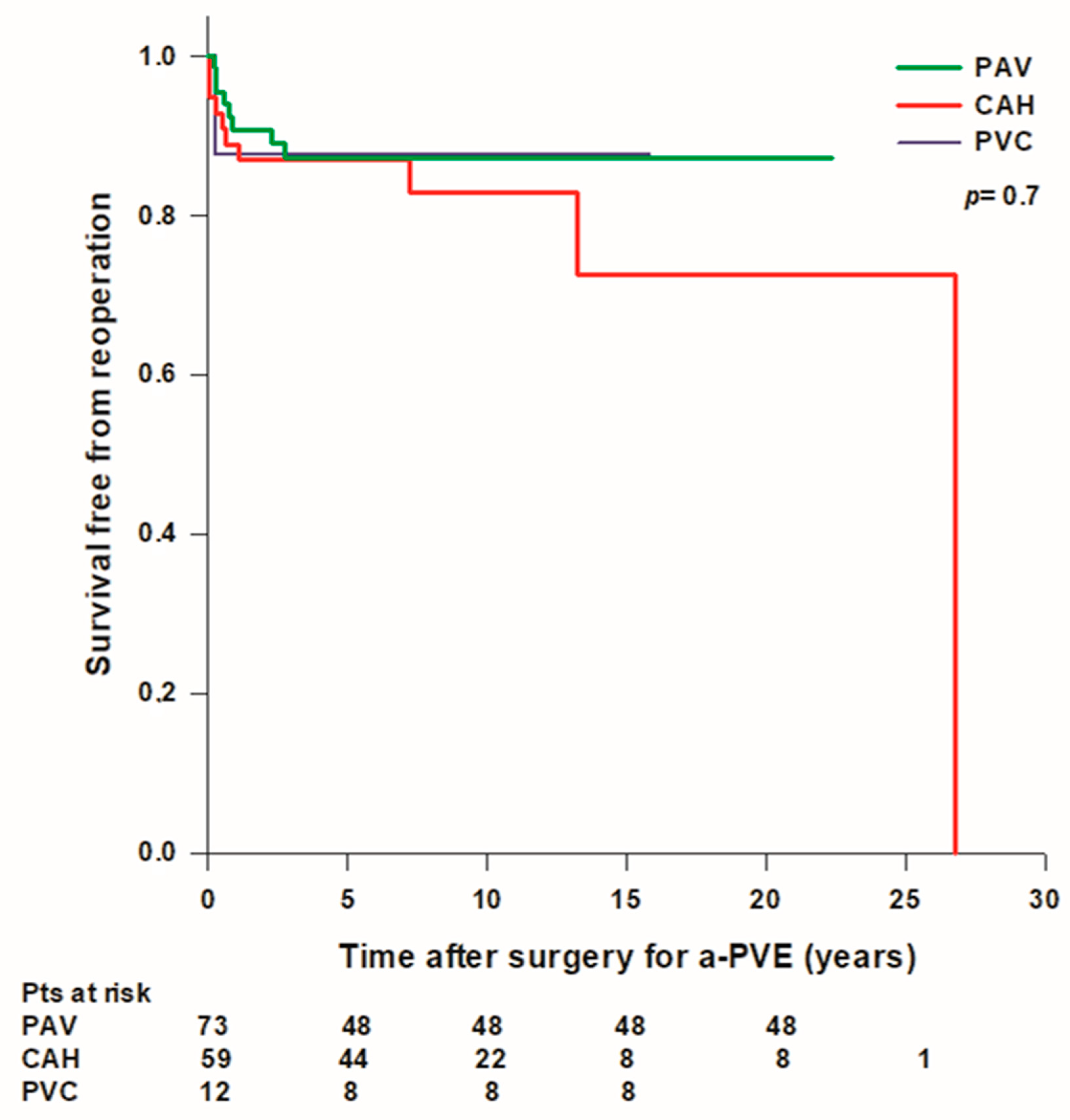
3.3. Reoperation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Habib, G.; Erba, P.A.; Iung, B.; Donal, E.; Cosyns, B.; Laroche, C.; Popescu, B.A.; Prendergast, B.; Tornos, P.; Sadeghpour, A.; et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: A prospective cohort study. Eur. Heart J. 2019, 40, 3222–3232. [Google Scholar] [CrossRef] [PubMed]
- Luehr, M.; Bauernschmitt, N.; Peterss, S.; Li, Y.; Heyn, O.; Dashkevich, A.; Oberbach, A.; Bagaev, E.; Pichlmaier, M.A.; Juchem, G.; et al. Incidence and Surgical Outcomes of Patients with Native and Prosthetic Aortic Valve Endocarditis. Ann. Thorac. Surg. 2020, 110, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Lalani, T.; Chu, V.H.; Park, L.P.; Cecchi, E.; Corey, G.R.; Durante-Mangoni, E.; Fowler, V.G., Jr.; Gordon, D.; Grossi, P.; Hannan, M.; et al. In-hospital and 1-year mortality in patients undergoing early surgery for prosthetic valve endocarditis. JAMA Intern. Med. 2013, 173, 1495–1504. [Google Scholar] [CrossRef]
- Leontyev, S.; Borger, M.A.; Modi, P.; Lehmann, S.; Seeburger, J.; Walther, T.; Mohr, F.W. Redo aortic valve surgery: Influence of prosthetic valve endocarditis on outcomes. J. Thorac. Cardiovasc. Surg. 2011, 142, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC guidelines for the management of infective endocarditis: The task force for the management of infective endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, V.G.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed Modifications to the Duke Criteria for the Diagnosis of Infective Endocarditis. Clin. Infect. Dis. 2000, 30, 633–638. [Google Scholar] [CrossRef]
- VARC-3 Writing Committee; Généreux, P.; Piazza, N.; Alu, M.C.; Nazif, T.; Hahn, R.T.; Pibarot, P.; Bax, J.J.; Leipsic, J.A.; Blanke, P.; et al. Valve Academic Research Consortium 3: Updated Endpoint Definitions for Aortic Valve Clinical Research. J. Am. Coll. Cardiol. 2021, 77, 2717–2746. [Google Scholar] [CrossRef]
- Shrestha, N.K.; Shah, S.Y.; Hussain, S.T.; Pettersson, G.B.; Griffin, B.P.; Nowacki, A.S.; Gordon, S.M. Association of Surgical Treatment with Survival in Patients with Prosthetic Valve Endocarditis. Ann. Thorac. Surg. 2020, 109, 1834–1843. [Google Scholar] [CrossRef]
- Mihos, C.G.; Capoulade, R.; Yucel, E.; Picard, M.H.; Santana, O. Surgical Versus Medical Therapy for Prosthetic Valve Endocarditis: A Meta-Analysis of 32 Studies. Ann. Thorac. Surg. 2017, 103, 991–1004. [Google Scholar] [CrossRef]
- Musci, M.; Hübler, M.; Amiri, A.; Stein, J.; Kosky, S.; Meyer, R.; Weng, Y.; Hetzer, R. Surgical treatment for active infective prosthetic valve endocarditis: 22-year single-centre experience. Eur. J. Cardiothorac. Surg. 2010, 38, 528–538. [Google Scholar] [CrossRef]
- Pettersson, G.B.; Coselli, J.S.; Hussain, S.T.; Griffin, B.; Blackstone, E.H.; Gordon, S.M.; LeMaire, S.A.; Woc-Colburn, L.E. 2016 The American Association for Thoracic Surgery (AATS) consensus guidelines: Surgical treatment of infective endocarditis: Executive summary. J. Thorac. Cardiovasc. Surg. 2017, 153, 1241–1258.e29. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.T.; Blackstone, E.H.; Pettersson, G.B. Allografts remain a cornerstone of surgical treatment of invasive and destructive aortic valve infective endocarditis: Surgeon and technique do matter! J. Thorac. Cardiovasc. Surg. 2017, 154, 1900–1901.e1. [Google Scholar] [CrossRef]
- Perrotta, S.; Jeppsson, A.; Fröjd, V.; Svensson, G. Surgical Treatment of Aortic Prosthetic Valve Endocarditis: A 20-Year Single-Center Experience. Ann. Thorac. Surg. 2016, 101, 1426–1432. [Google Scholar] [CrossRef] [PubMed]
- Polo, M.C.; Thibault, D.; Jawitz, O.K.; Zwischenberger, B.A.; O’Brien, S.M.; Thourani, V.H.; Jacobs, J.P.; Hooker, R.L. Aortic Prosthetic Valve Endocarditis: Analysis of The Society of Thoracic Surgeons Database. Ann. Thorac. Surg. 2022, 114, 2140–2147. [Google Scholar] [CrossRef] [PubMed]
- Edlin, P.; Westling, K.; Sartipy, U. Long-term survival after operations for native and prosthetic valve endocarditis. Ann. Thorac. Surg. 2013, 95, 1551–1556. [Google Scholar] [CrossRef] [PubMed]
- Leontyev, S.; Davierwala, P.M.; Krögh, G.; Feder, S.; Oberbach, A.; Bakhtiary, F.; Misfeld, M.; Borger, M.A.; Mohr, F.W. Early and late outcomes of complex aortic root surgery in patients with aortic root abscesses. Eur. J. Cardiothorac. Surg. 2016, 49, 447–454. [Google Scholar] [CrossRef]
- Chen, G.J.; Lo, W.C.; Tseng, H.W.; Pan, S.C.; Chen, Y.S.; Chang, S.C. Outcome of surgical intervention for aortic root abscess: A meta-analysis. Eur. J. Cardiothorac. Surg. 2018, 53, 807–814. [Google Scholar] [CrossRef]
- Yang, B.; Caceres, J.; Farhat, L.; Le, T.; Brown, B.; St Pierre, E.; Wu, X.; Kim, K.M.; Patel, H.J.; Deeb, G.M. Root abscess in the setting of infectious endocarditis: Short- and long-term outcomes. J. Thorac. Cardiovasc. Surg. 2021, 162, 1049–1059. [Google Scholar] [CrossRef]
- Galeone, A.; Trojan, D.; Gardellini, J.; Di Gaetano, R.; Faggian, G.; Luciani, G.B. Cryopreserved aortic homografts for complex aortic valve or root endocarditis: A 28-year experience. Eur. J. Cardiothorac. Surg. 2022, 62, ezac193. [Google Scholar] [CrossRef]
- Byrne, J.G.; Rezai, K.; Sanchez, J.A.; Bernstein, R.A.; Okum, E.; Leacche, M.; Balaguer, J.M.; Prabhakaran, S.; Bridges, C.R.; Higgins, R.S. Surgical management of endocarditis: The society of thoracic surgeons clinical practice guideline. Ann. Thorac. Surg. 2011, 91, 2012–2019. [Google Scholar] [CrossRef]
- Sabik, J.F.; Lytle, B.W.; Blackstone, E.H.; Marullo, A.G.; Pettersson, G.B.; Cosgrove, D.M. Aortic root replacement with cryopreserved allograft for prosthetic valve endocarditis. Ann. Thorac. Surg. 2002, 74, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Svensson, L.G.; Pillai, S.T.; Rajeswaran, J.; Desai, M.Y.; Griffin, B.; Grimm, R.; Hammer, D.F.; Thamilarasan, M.; Roselli, E.E.; Pettersson, G.B.; et al. Long-term survival, valve durability, and reoperation for 4 aortic root procedures combined with ascending aorta replacement. J. Thorac. Cardiovasc. Surg. 2016, 151, 764–774. [Google Scholar] [CrossRef] [PubMed]
- Solari, S.; Mastrobuoni, S.; de Kerchove, L.; Navarra, E.; Astarci, P.; Noirhomme, P.; Poncelet, A.; Jashari, R.; Rubay, J.; El Khoury, G. Over 20 years experience with aortic homograft in aortic valve replacement during acute infective endocarditis. Eur. J. Cardiothorac. Surg. 2016, 50, 1158–1164. [Google Scholar] [CrossRef]
- Musci, M.; Weng, Y.; Hübler, M.; Amiri, A.; Pasic, M.; Kosky, S.; Stein, J.; Siniawski, H.; Hetzer, R. Homograft aortic root replacement in native or prosthetic active infective endocarditis: Twenty-year single-center experience. J. Thorac. Cardiovasc. Surg. 2010, 139, 665–673. [Google Scholar] [CrossRef]
- Perrotta, S.; Aljassim, O.; Jeppsson, A.; Bech-Hanssen, O.; Svensson, G. Survival and quality of life after aortic root replacement with homografts in acute endocarditis. Ann. Thorac. Surg. 2010, 90, 1862–1867. [Google Scholar] [CrossRef] [PubMed]
- Yazdchi, F.; Harloff, M.; Hirji, S.; Percy, E.; McGurk, S.; Cherkasky, O.; Malarczyk, A.; Newell, P.; Rinewalt, D.; Mallidi, H.R.; et al. Long-term Outcomes of Aortic Valve Replacement with Aortic Homograft: 27 Years Experience. Ann. Thorac. Surg. 2021, 112, 1929–1938. [Google Scholar] [CrossRef]
- Kim, J.B.; Ejiofor, J.I.; Yammine, M.; Camuso, J.M.; Walsh, C.W.; Ando, M.; Melnitchouk, S.I.; Rawn, J.D.; Leacche, M.; MacGillivray, T.E.; et al. Are homografts superior to conventional prosthetic valves in the setting of infective endocarditis involving the aortic valve? J. Thorac. Cardiovasc. Surg. 2016, 151, 1239–1246. [Google Scholar] [CrossRef]
- Jassar, A.S.; Bavaria, J.E.; Szeto, W.Y.; Moeller, P.J.; Maniaci, J.; Milewski, R.K.; Gorman, J.H., 3rd; Desai, N.D.; Gorman, R.C.; Pochettino, A. Graft selection for aortic root replacement in complex active endocarditis: Does it matter? Ann. Thorac. Surg. 2012, 3, 480–487. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Isolated Microorganism | ALL (n = 144) | PAV (n = 73) | PVC (n = 12) | CAH (n = 59) | p |
|---|---|---|---|---|---|
| GRAM+ | 95 (66%) | 51 (70%) | 7 (58%) | 37 (63%) | 0.2 |
| Staphylococcus aureus | 14 (10%) | 8 (11%) | 1 (8%) | 5 (8%) | 0.8 |
| Coagulase negative staphylococcus | 38 (26%) | 18 (25%) | 4 (33%) | 16 (27%) | 0.7 |
| Enterococcus spp. | 21 (15%) | 12 (16%) | 1 (8%) | 8 (14%) | 0.5 |
| Streptococcus spp. | 14 (10%) | 8 (11%) | 1 (8%) | 5 (8%) | 0.8 |
| Other GRAM+ | 8 (6%) | 5 (7%) | 0 | 3 (5%) | - |
| GRAM− | 6 (4%) | 2 (3%) | 0 | 4 (7%) | - |
| Fungi | 4 (3%) | 3 (4%) | 1 (8%) | 0 | - |
| Negative blood tests | 16 (11%) | 5 (7%) | 3 (25%) | 8 (14%) | 0.1 |
| Unknown | 23 (16%) | 12 (16%) | 1 (8%) | 10 (17%) | 0.2 |
| Preoperative Characteristics | ALL (n = 144) | PAV (n = 73) | PVC (n = 12) | CAH (n = 59) | p |
|---|---|---|---|---|---|
| Male sex | 115 (80%) | 60 (82%) | 10 (83%) | 45 (76%) | 0.51 |
| Age, years | 70 [61–75] | 70 [61–75] | 65 [54–76] | 71 [62–76] | 0.3 |
| BMI | 26 [23–29] | 26 [23–30] | 26 [23–28] | 26 [24–28] | 0.9 |
| BSA | 1.9 [1.8–2] | 1.9 [1.7–2.1] | 1.9 [1.8–2.1] | 1.9 [1.7-2] | 0.9 |
| Early PVE | 47 (33%) | 19 (26%) | 5 (42%) | 23 (39%) | 0.1 |
| Indication for prior surgery | |||||
| AS | 75 (52%) | 38 (53%) | 4 (33%) | 33 (56%) | 0.8 |
| AR | 13 (9%) | 9 (13%) | 1 (8%) | 3 (5%) | 0.6 |
| AAA and AS | 14 (10%) | 8 (11%) | 4 (33%) | 2 (3%) | 0.4 |
| AAA and AR | 19 (13%) | 7 (10%) | 2 (17%) | 10 (17%) | 0.5 |
| Infective endocarditis | 10 (7%) | 3 (4%) | 0 | 7 (12%) | 0.6 |
| Rheumatic disease | 8 (6%) | 6 (7%) | 0 | 2 (3%) | 0.7 |
| Aortic dissection | 3 (2%) | 2 (3%) | 1 (8%) | 0 | - |
| Structural valve dysfunction | 2 (1%) | 0 | 0 | 2 (3%) | - |
| Previous surgery | |||||
| AVR | 81 (56%) | 39 (53%) | 4 (42%) | 38 (64%) | 0.1 |
| AVR + AAR | 18 (13%) | 12 (15%) | 2 (8%) | 4 (7%) | 0.2 |
| AVR + CABG | 17 (12%) | 12 (16%) | 1 (8%) | 4 (7%) | 0.2 |
| Bentall procedure | 13 (9%) | 4 (5%) | 5 (42%) | 4 (7%) | <0.001 |
| AVR + MVR | 7 (5%) | 5 (7%) | 0 | 2 (3%) | - |
| AVR + AAR + CABG | 4 (3%) | 1 (1%) | 0 | 3 (5%) | - |
| AVR + AAR + MVR | 2 (1%) | 0 | 0 | 2 (3%) | - |
| AVR + PVM + CABG | 2 (1%) | 0 | 0 | 2 (3%) | - |
| Redo ≥ 2 | 10 (7%) | 4 (6%) | 1 (8%) | 5 (8%) | 0.8 |
| Intra and perioperative characteristics | |||||
| Vegetations | 66 (46%) | 34 (72%) | 3 (25%) | 28 (47%) | 0.2 |
| Circumferential annular abscess | 37 (26%) | 6 (8%) | 6 (50%) | 25 (42%) | 0.001 |
| Aorto-mitral discontinuity | 40 (28%) | 16 (22%) | 1 (8%) | 23 (39%) | 0.05 |
| Prosthetic valve dehiscence | 78 (55%) | 32 (44%) | 6 (50%) | 40 (68%) | 0.09 |
| Prosthetic valve perforation | 14 (10%) | 10 (14%) | 1 (8%) | 3 (5%) | 0.1 |
| MV endocarditis | 17 (12%) | 7 (10%) | 1 (8%) | 9 (15%) | 0.2 |
| TV endocarditis | 11 (8%) | 1 (1%) | 0 | 10 (17%) | 0.002 |
| Gerbode defect | 8 (6%) | 0 | 0 | 8 (14%) | - |
| IV septum defect | 7 (5%) | 2 (3%) | 0 | 5 (8%) | 0.8 |
| Aortic-left atrium fistula | 3 (2%) | 2 (3%) | 0 | 1 (2%) | |
| Urgent/emergency procedure | 53 (37%) | 21 (29%) | 5 (42%) | 27 (46%) | 0.1 |
| Indication for surgery | |||||
| Haemodynamic | 44 (31%) | 17 (23%) | 4 (33%) | 23 (39%) | 0.1 |
| Infectious | 62 43%) | 35 (48%) | 5 (42%) | 22 (37%) | 0.2 |
| Embolic | 38 (26%) | 21 (29%) | 3 (25%) | 14 (24%) | 0.7 |
| Surgical technique | |||||
| Biological prosthetic AVR | 67 (47%) | 67 (92%) | |||
| Mechanical prosthetic AVR | 6 (4%) | 6 (8%) | |||
| Biological Bentall procedure | 10 (7%) | 10 (83%) | |||
| Mechanical Bentall procedure | 2 (1%) | 2 (17%) | |||
| CAH Free-hand sub-coronary technique | 27 (19%) | 27 (46%) | |||
| CAH Full root replacement | 28 (20%) | 28 (47%) | |||
| CAH Intraluminal cylinder technique | 4 (3%) | 4 (7%) | |||
| Concomitant procedure | |||||
| Pericardial patch use | 37 (26%) | 20 (28%) | 5 (42%) | 12 (20%) | |
| MV replacement | 11 (8%) | 7 (10%) | 1 (8%) | 3 (5%) | 0.6 |
| MV repair | 10 (7%) | 2 (4%) | 1 (8%) | 7 (12%) | 0.4 |
| TV repair | 7 (5%) | 2 (3%) | 0 | 5 (7%) | 0.5 |
| AA replacement | 9 (6%) | 7 (10%) | 0 | 2 (3%) | 0.6 |
| CABG | 4 (3%) | 3 (4%) | 1 (8%) | 0 | |
| CPB time, min | 184 [131–236] | 150 [110–190] | 279 [225–386] | 214 [178–278] | <0.001 |
| Aortic cross-clamping time, min | 138 [99–181] | 104 [75–134] | 179 [150–263] | 167 [140–203] | <0.001 |
| IABP | 8 (6%) | 4 (6%) | 2 (17%) | 2 (3%) | 0.8 |
| ECMO | 5 (3%) | 2 (3%) | 0 | 3 (5%) | 0.8 |
| Re-exploration for bleeding | 12 (8%) | 3 (4%) | 1 (8%) | 8 (14%) | 0.07 |
| Pacemaker implantation | 26 (18%) | 6 (8%) | 1 (8%) | 19 (32%) | <0.001 |
| CVA | 7 (5%) | 4 (6%) | 0 | 3 (5%) | 0.9 |
| CRRT | 5 (3%) | 4 (6%) | 0 | 1 (2%) | 0.8 |
| Mediastinitis | 3 (2%) | 0 | 0 | 3 (5%) | |
| Periprocedural mortality | 17 (12%) | 6 (8%) | 4 (33%) | 7 (12%) | |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p | Hazard Ratio (95% CI) | p | |
| Patient’s age > 65 years | 1.36 (0.82–2.25) | 0.2 | ||
| Female sex | 1.15 (0.64–2.07) | 0.62 | ||
| Circumferential abscess | 1.47 (0.9–2.4) | 0.12 | ||
| MV endocarditis | 1.95 (1.06–3.58) | 0.03 | 2.27 (1.22–4.23) | 0.01 |
| TV endocarditis | 1.83 (0.83–4) | 0.13 | ||
| AVR with PAV | 0.76 (0.48–1.2) | 0.25 | ||
| ARR with PVC | 2.1 (1–4.4) | 0.05 | 2.37 (1.08–5.19) | 0.03 |
| AVR or ARR with CAH | 1.05 (0.66–1.67) | 0.8 | ||
| Postoperative IABP | 2.82 (1.11–7.15) | 0.02 | 1.3 (0.35–4.76) | 0.68 |
| Postoperative ECMO | 4.53 (1.61–12.7) | 0.004 | 5.52 (1.08–28.2) | 0.04 |
| Reintervention | 1.29 (0.72–2.29) | 0.38 | ||
| Reintervention | ALL (n = 144) | PAV (n = 73) | PVC (n = 12) | CAH (n = 59) | p |
|---|---|---|---|---|---|
| Early reintervention | 3 (2%) | 0 | 0 | 3 (5%) | |
| SVD | 1 (1%) | 0 | 0 | 1 (2%) | |
| NSVD | 2 (2%) | 0 | 0 | 2 (3%) | |
| Late reintervention | 16 (11%) | 8 (11%) | 1 (8%) | 7 (12%) | |
| IE | 7 (5%) | 4 (5%) | 0 | 3 (5%) | 0.9 |
| SVD | 2 (2%) | 0 | 0 | 2 (3%) | 0.9 |
| NSVD | 6 (4%) | 3 (5%) | 1 (8%) | 2 (3%) | |
| MV regurgitation | 1(1%) | 0 | 0 | 1 (2%) | 0.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galeone, A.; Gardellini, J.; Trojan, D.; Di Nicola, V.; Di Gaetano, R.; Faggian, G.; Luciani, G.B. Three Decades of Experience with Aortic Prosthetic Valve Endocarditis. J. Cardiovasc. Dev. Dis. 2023, 10, 338. https://doi.org/10.3390/jcdd10080338
Galeone A, Gardellini J, Trojan D, Di Nicola V, Di Gaetano R, Faggian G, Luciani GB. Three Decades of Experience with Aortic Prosthetic Valve Endocarditis. Journal of Cardiovascular Development and Disease. 2023; 10(8):338. https://doi.org/10.3390/jcdd10080338
Chicago/Turabian StyleGaleone, Antonella, Jacopo Gardellini, Diletta Trojan, Venanzio Di Nicola, Renato Di Gaetano, Giuseppe Faggian, and Giovanni Battista Luciani. 2023. "Three Decades of Experience with Aortic Prosthetic Valve Endocarditis" Journal of Cardiovascular Development and Disease 10, no. 8: 338. https://doi.org/10.3390/jcdd10080338
APA StyleGaleone, A., Gardellini, J., Trojan, D., Di Nicola, V., Di Gaetano, R., Faggian, G., & Luciani, G. B. (2023). Three Decades of Experience with Aortic Prosthetic Valve Endocarditis. Journal of Cardiovascular Development and Disease, 10(8), 338. https://doi.org/10.3390/jcdd10080338