
Healthy Lifestyle Behavior, Goal Setting, and Personality among Older Adults: A Synthesis of Literature Reviews and Interviews


Abstract
1. Highlights
- The current review highlights the relationship between healthy living practices, goal setting, and personality.
- Conscientiousness, neuroticism, and extraversion were shown to have significant effects on health-related behaviors as well as actual healthy lifestyle behaviors.
- Future research should focus on various types of HLB therapies that take into account personality and goal-setting processes.
2. Background
3. Objectives
4. Method
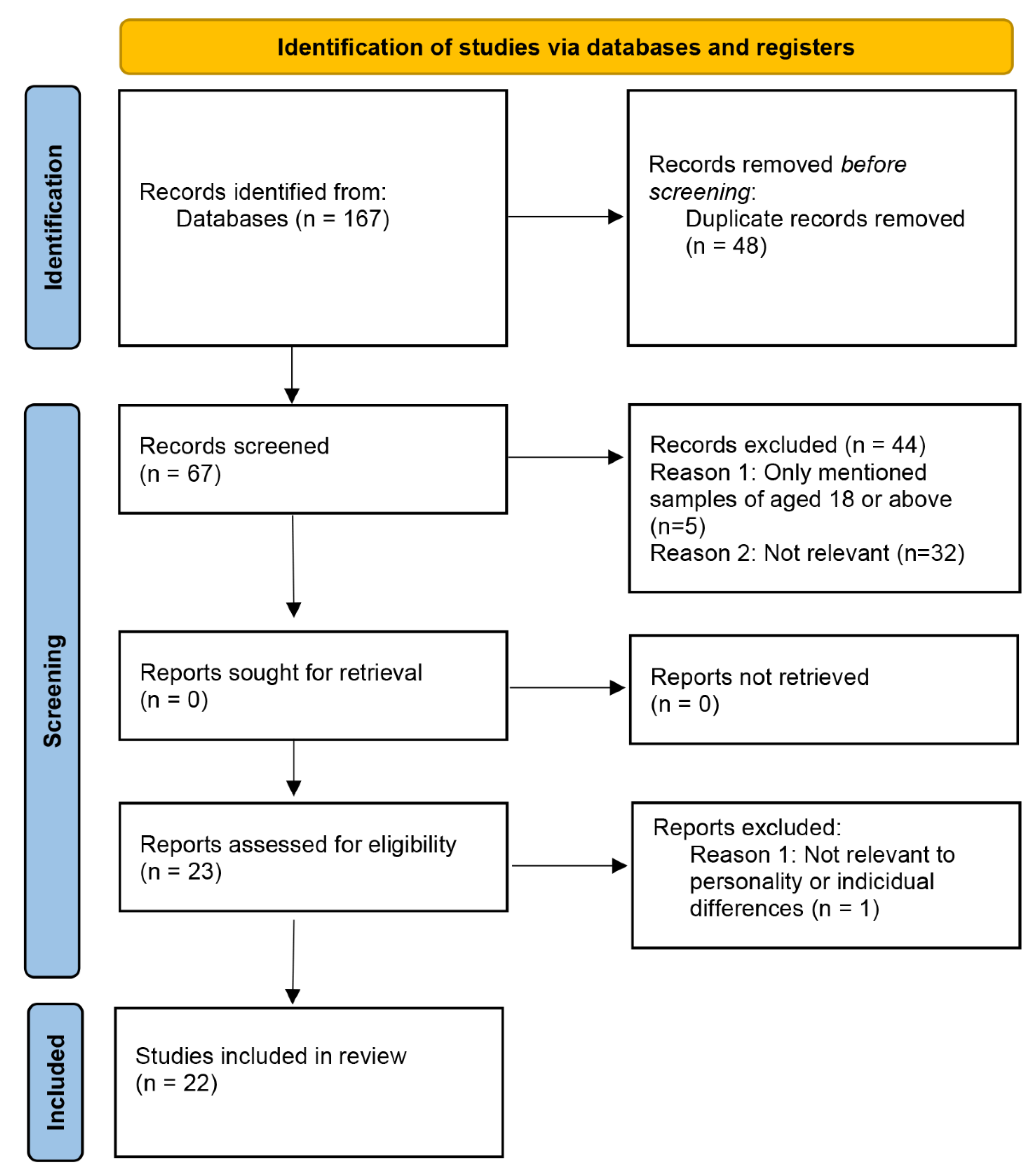
4.1. Literature Search
4.2. Interview
- 1. Did you set any goals for yourself before this program? What were they?
- 2. Think about your overall health and fitness and ability to get around and do the things you want to do. What are your wishes and hopes for that in the future?
- 2a. Do you think this program/participating in physical activity has facilitated you to do so, or at least achieve a certain extent of that?
- 3. Again, think about your health and fitness and ability to get around and do the things you want to do. What are your fears and worries about the future?
- 3a. Do you think this program/participating in physical activity could eliminate these fears or worries?
- 4. What kinds of goals do you tend to set for yourself, in terms of physical activity/health-related factors (e.g., diet, exercise)?
- 5. What kind of personality do you think you have?
- 5a. Do you think your personality affects your goals for physical activity and overall health? How?
- 6. Do you prefer having standardized static goals or personalized goals when participating in an exercise program with coach supervision?
- 7. Do you prefer having a single ultimate goal or integrated smaller goals (goal phrase) before achieving the ultimate goal?
- 8. To what extent could rewards prompt you to achieve your goals?
4.3. Data Analysis
5. Results
5.1. Literature Review and Interview Demographics
5.1.1. Types of Healthy Lifestyle Behavior
5.1.2. Personality Types and Healthy Lifestyle Behaviors
5.1.3. Healthy Lifestyle Behavior, Goals, and Personality Traits
5.1.4. Interaction between Personality, Goals, and Healthy Lifestyle Behaviors
5.2. Participant Interviews
5.2.1. Personality
5.2.2. Goals and Healthy Lifestyle Behavior
- Hoped-for possible self
- Fear of possible self
- Long term health-related goals
- Goal preference for intervention/program: generalized vs. personalized aims
- Goal preference for intervention/program: ultimate aim vs. progressive small aims
- Personality, goals, and healthy lifestyle behavior
5.3. Motivations and Intentions
- Theory-based program
- Exercise encouragement
- Perceived constraints on exercise
6. Discussion
7. Future Implications
8. Strengths and Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buchman, A.; Boyle, P.; Yu, L.; Shah, R.; Wilson, R.; Bennett, D. Total daily physical activity and the risk of AD and cognitive decline in older adults. Neurology 2012, 78, 1323–1329. [Google Scholar] [CrossRef]
- Martín-María, N.; Caballero, F.F.; Moreno-Agostino, D.; Olaya, B.; Haro, J.M.; Ayuso-Mateos, J.L.; Miret, M. Relationship between subjective well-being and healthy lifestyle behaviours in older adults: A longitudinal study. Aging Ment. Health 2020, 24, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Menichetti, J.; Cipresso, P.; Bussolin, D.; Graffigna, G. Engaging older people in healthy and active lifestyles: A systematic review. Ageing Soc. 2016, 36, 2036–2060. [Google Scholar] [CrossRef]
- Resnick, B.; Spellbring, A.M. Understanding what motivates older adults to exercise. J. Gerontol. Nurs. 2000, 26, 34–42. [Google Scholar] [CrossRef]
- Wrosch, C.; Scheier, M.F. Personality and quality of life: The importance of optimism and goal adjustment. Qual. Life Res. 2003, 12, 59–72. [Google Scholar] [CrossRef]
- Gomez, V.; Allemand, M.; Grob, A. Neuroticism, extraversion, goals, and subjective well-being: Exploring the relations in young, middle-aged, and older adults. J. Res. Personal. 2012, 46, 317–325. [Google Scholar] [CrossRef]
- Zapata-Lamana, R.; Poblete-Valderrama, F.; Cigarroa, I.; Parra-Rizo, M.A. The practice of vigorous physical activity is related to a higher educational level and income in older women. Int. J. Environ. Res. Public Health 2021, 18, 10815. [Google Scholar] [CrossRef]
- Parra-Rizo, M.A.; Vásquez-Gómez, J.; Álvarez, C.; Diaz-Martínez, X.; Troncoso, C.; Leiva-Ordoñez, A.M.; Zapata-Lamana, R.; Cigarroa, I. Predictors of the Level of Physical Activity in Physically Active Older People. Behav. Sci. 2022, 12, 331. [Google Scholar] [CrossRef]
- Austin, J.T.; Vancouver, J.B. Goal constructs in psychology: Structure, process, and content. Psychol. Bull. 1996, 120, 338. [Google Scholar] [CrossRef]
- Kasser, T.; Ryan, R.M. Further examining the American dream: Differential correlates of intrinsic and extrinsic goals. Personal. Soc. Psychol. Bull. 1996, 22, 280–287. [Google Scholar] [CrossRef]
- Cantor, N. From thought to behavior: “Having” and “doing” in the study of personality and cognition. Am. Psychol. 1990, 45, 735. [Google Scholar] [CrossRef]
- Allport, G.W. Personality: A Psychological Interpretation. British Joural of Educational Psychology 1943, 13, 48–50. [Google Scholar]
- Ebner, N.C.; Freund, A.M. Personality theories of successful aging. In Handbook of Gerontology: Evidence-Based Approaches to Theory, Practice, and Policy; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2007. [Google Scholar]
- Hooker, K.; Choun, S.; Mejía, S.; Pham, T.; Metoyer, R. A microlongitudinal study of the linkages among personality traits, self-regulation, and stress in older adults. Res. Hum. Dev. 2013, 10, 26–46. [Google Scholar] [CrossRef]
- Cook, D.B.; Casillas, A.; Robbins, S.B.; Dougherty, L.M. Goal continuity and the “Big Five” as predictors of older adult marital adjustment. Personal. Individ. Differ. 2005, 38, 519–531. [Google Scholar] [CrossRef]
- Ouwehand, C.; de Ridder, D.T.; Bensing, J.M. Individual differences in the use of proactive coping strategies by middle-aged and older adults. Personal. Individ. Differ. 2008, 45, 28–33. [Google Scholar] [CrossRef][Green Version]
- Chung, P.-K.; Zhang, C.-Q.; Zhao, Y.; Wong, M.Y.C.; Hu, C. Effectiveness of resistance training on resilience in Hong Kong Chinese older adults: Study protocol for a randomized controlled trial. BMC Geriatr. 2021, 21, 250. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 105906. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, L.L.; Baumann, H.; Meixner, C.; Nixon, P.; Wollesen, B. App-tailoring requirements to increase stress management competencies within families: Cross-sectional survey study. J. Med. Internet Res. 2021, 23, e26376. [Google Scholar] [CrossRef]
- Davis, C.R.; Murphy, K.J.; Curtis, R.G.; Maher, C.A. A process evaluation examining the performance, adherence, and acceptability of a physical activity and diet artificial intelligence virtual health assistant. Int. J. Environ. Res. Public Health 2020, 17, 9137. [Google Scholar] [CrossRef]
- Briki, W. Why do exercisers with a higher trait self-control experience higher subjective well-being? The mediating effects of amount of leisure-time physical activity, perceived goal progress, and self-efficacy. Personal. Individ. Differ. 2018, 125, 62–67. [Google Scholar] [CrossRef]
- Kim, E.-J.; Nho, J.-H.; Kim, H.-Y.; Park, S.-K. The effects of lifestyle interventions on the health-promoting behavior, type D personality, cognitive function and body composition of low-income middle-aged Korean women. Int. J. Environ. Res. Public Health 2021, 18, 5637. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.; Williams, L.; O’donnell, C.; McKechnie, J. The influence of social-cognitive constructs and personality traits on physical activity in healthy adults. Int. J. Sport Exerc. Psychol. 2017, 15, 540–555. [Google Scholar] [CrossRef]
- Sirois, F.M.; Yang, S.; van Eerde, W. Development and validation of the General Procrastination Scale (GPS-9): A short and reliable measure of trait procrastination. Personal. Individ. Differ. 2019, 146, 26–33. [Google Scholar] [CrossRef]
- Briki, W.; Dagot, L. Conservatives are happier than liberals: The mediating role of perceived goal progress and flow experience—A pilot study. Curr. Psychol. 2020, 41, 1267–1278. [Google Scholar] [CrossRef]
- Churchill, S.; Jessop, D. Spontaneous implementation intentions and impulsivity: Can impulsivity moderate the effectiveness of planning strategies? Br. J. Health Psychol. 2010, 15, 529–541. [Google Scholar] [CrossRef]
- Gruenewald, T.L.; Mroczek, D.K.; Ryff, C.D.; Singer, B.H. Diverse pathways to positive and negative affect in adulthood and later life: An integrative approach using recursive partitioning. Dev. Psychol. 2008, 44, 330. [Google Scholar] [CrossRef] [PubMed]
- Javaras, K.N.; Williams, M.; Baskin-Sommers, A.R. Psychological interventions potentially useful for increasing conscientiousness. Personal. Disord. Theory Res. Treat. 2019, 10, 13. [Google Scholar] [CrossRef]
- Kahlbaugh, P.; Huffman, L. Personality, emotional qualities of leisure, and subjective well-being in the elderly. Int. J. Aging Hum. Dev. 2017, 85, 164–184. [Google Scholar] [CrossRef]
- Stieger, M.; Robinson, S.A.; Bisson, A.N.; Lachman, M.E. The relationship of personality and behavior change in a physical activity intervention: The role of conscientiousness and healthy neuroticism. Personal. Individ. Differ. 2020, 166, 110224. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, L.; Chakravarti, A. Not just for your health alone: Regular exercisers’ decision-making in unrelated domains. J. Exp. Psychol. Appl. 2022, 28, 379–398. [Google Scholar] [CrossRef]
- Rammstedt, B.; John, O.P. Measuring personality in one minute or less: A 10-item short version of the Big Five Inventory in English and German. J. Res. Personal. 2007, 41, 203–212. [Google Scholar] [CrossRef]
- Allen, H.L.; Gmelin, T.; Moored, K.D.; Boudreau, R.M.; Smagula, S.F.; Cohen, R.W.; Katz, R.; Stone, K.; Cauley, J.A.; Glynn, N.W. Relationship between Personality Measures and Perceived Mental Fatigability. J. Aging Health 2021, 34, 750–760. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, R.E.; Smith, N. Personality correlates of physical activity: A review and meta-analysis. Br. J. Sport. Med. 2006, 40, 958–965. [Google Scholar] [CrossRef]
- Lethbridge, J.; Watson, H.J.; Egan, S.J.; Street, H.; Nathan, P.R. The role of perfectionism, dichotomous thinking, shape and weight overvaluation, and conditional goal setting in eating disorders. Eat. Behav. 2011, 12, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Watson, H.J.; Raykos, B.C.; Street, H.; Fursland, A.; Nathan, P.R. Mediators between perfectionism and eating disorder psychopathology: Shape and weight overvaluation and conditional goal-setting. Int. J. Eat. Disord. 2011, 44, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Sherry, S.B.; Hewitt, P.L.; Besser, A.; McGee, B.J.; Flett, G.L. Self-oriented and socially prescribed perfectionism in the Eating Disorder Inventory Perfectionism subscale. Int. J. Eat. Disord. 2004, 35, 69–79. [Google Scholar] [CrossRef]
- Sirois, F.M. Procrastination and intentions to perform health behaviors: The role of self-efficacy and the consideration of future consequences. Personal. Individ. Differ. 2004, 37, 115–128. [Google Scholar] [CrossRef]
- Sirois, F.M. “I’ll look after my health, later”: A replication and extension of the procrastination–health model with community-dwelling adults. Personal. Individ. Differ. 2007, 43, 15–26. [Google Scholar] [CrossRef]
- Sirois, F.M. Is procrastination a vulnerability factor for hypertension and cardiovascular disease? Testing an extension of the procrastination–health model. J. Behav. Med. 2015, 38, 578–589. [Google Scholar] [CrossRef]
- Hankonen, N.; Vollmann, M.; Renner, B.; Absetz, P. What is setting the stage for abdominal obesity reduction? A comparison between personality and health-related social cognitions. J. Behav. Med. 2010, 33, 415–422. [Google Scholar] [CrossRef][Green Version]
- Palmer, B.W.; Martin, A.S.; Depp, C.A.; Glorioso, D.K.; Jeste, D.V. Wellness within illness: Happiness in schizophrenia. Schizophr. Res. 2014, 159, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Scheier, M.; Carver, C.; Bridges, M. Life Orientation Test-Revised (LOT-R). Diakses Pada Tanggal 1994, 11. Available online: https://fetzer.org/sites/default/files/images/stories/pdf/selfmeasures/Self_Measures_for_Love_and_Compassion_Research_OPTIMISM.pdf (accessed on 20 October 2022).
- Kim, E.S.; Park, N.; Peterson, C. Dispositional optimism protects older adults from stroke: The Health and Retirement Study. Stroke 2011, 42, 2855–2859. [Google Scholar] [CrossRef]
- Smagula, S.F.; Faulkner, K.; Scheier, M.F.; Tindle, H.A.; Cauley, J.A.; Osteoporotic Fractures in Men (MrOS) Study Group. Testing the independence of multiple personality factors in relation to health among community-dwelling older men. J. Aging Health 2016, 28, 571–586. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.R.; Nho, J.H.; Kim, J.Y.; Hur, J. Effects of a lifestyle intervention based on Type D personality in overweight and obese middle-aged women: A feasibility study. Worldviews Evid.-Based Nurs. 2020, 17, 393–403. [Google Scholar] [CrossRef]
- Rapkin, B.D.; Fischer, K. Personal goals of older adults: Issues in assessment and prediction. Psychol. Aging 1992, 7, 127. [Google Scholar] [CrossRef]
- Jarrahi, M.H.; Gafinowitz, N.; Shin, G. Activity trackers, prior motivation, and perceived informational and motivational affordances. Pers. Ubiquitous Comput. 2018, 22, 433–448. [Google Scholar] [CrossRef]
- Heckhausen, J. Agency and control striving across the life span. Handbook of Life-Span Development; Springer: Berlin/Heidelberg, Germany, 2011; pp. 183–212. [Google Scholar]
- Kappes, C.; Thomsen, T. Imitation of Goal Engagement and Disengagement Processes in Romantic Relationships. Eur. J. Personal. 2020, 34, 234–244. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F. Optimism, pessimism, and self-regulation. In Optimism & Pessimism: Implications for Theory, Research, and Practice; American Psychological Association: Washington, DC, USA, 2001. [Google Scholar]
- Egan, S.J.; Wade, T.D.; Shafran, R. Perfectionism as a transdiagnostic process: A clinical review. Clin. Psychol. Rev. 2011, 31, 203–212. [Google Scholar] [CrossRef]
- Hagger, M.S. The multiple pathways by which self-control predicts behavior. Front. Psychol. 2013, 4, 849. [Google Scholar] [CrossRef]
- Hagger, M.S. The multiple pathways by which trait self-control predicts health behavior. Ann. Behav. Med. 2014, 48, 282–283. [Google Scholar] [CrossRef]
- Kalbaugh, C.A.; Kucharska-Newton, A.; Wruck, L.; Lund, J.L.; Selvin, E.; Matsushita, K.; Bengtson, L.G.; Heiss, G.; Loehr, L. Peripheral artery disease prevalence and incidence estimated from both outpatient and inpatient settings among medicare fee-for-service beneficiaries in the atherosclerosis risk in communities (ARIC) study. J. Am. Heart Assoc. 2017, 6, e003796. [Google Scholar] [CrossRef] [PubMed]
- Resnick, B.; Orwig, D.; Wehren, L.; Zimmerman, S.; Simpson, M.; Magaziner, J. The Exercise Plus Program for older women post hip fracture: Participant perspectives. Gerontol. 2005, 45, 539–544. [Google Scholar] [CrossRef]
- Myers, I.B. The Myers-Briggs Type Indicator: Manual (1962); Consulting Psychologists Press: Palo Alto, CA, USA, 1962. [Google Scholar]
- Carlyn, M. An assessment of the Myers-Briggs type indicator. J. Personal. Assess. 1977, 41, 461–473. [Google Scholar] [CrossRef] [PubMed]
- Furnham, A. The big five versus the big four: The relationship between the Myers-Briggs Type Indicator (MBTI) and NEO-PI five factor model of personality. Personal. Individ. Differ. 1996, 21, 303–307. [Google Scholar] [CrossRef]
- Furnham, A.; Moutafi, J.; Crump, J. The relationship between the revised NEO-personality inventory and the Myers-Briggs type indicator. Soc. Behav. Personal. Int. J. 2003, 31, 577–584. [Google Scholar] [CrossRef]
- Conner, M.; Abraham, C. Conscientiousness and the theory of planned behavior: Toward a more complete model of the antecedents of intentions and behavior. Personal. Soc. Psychol. Bull. 2001, 27, 1547–1561. [Google Scholar] [CrossRef]
- Bogg, T.; Roberts, B.W. The case for conscientiousness: Evidence and implications for a personality trait marker of health and longevity. Ann. Behav. Med. 2013, 45, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Kristén, L.; Ring, M. SwingPingis—An innovative and norm critical physical activity aid for everyone, everywhere. Eur. J. Adapt. Phys. Act. 2019, 12. [Google Scholar] [CrossRef]
- Roberts, B.W.; Walton, K.E.; Viechtbauer, W. Patterns of mean-level change in personality traits across the life course: A meta-analysis of longitudinal studies. Psychol. Bull. 2006, 132, 1. [Google Scholar] [CrossRef]
- Moffitt, T.E.; Arseneault, L.; Belsky, D.; Dickson, N.; Hancox, R.J.; Harrington, H.; Houts, R.; Poulton, R.; Roberts, B.W.; Ross, S. A gradient of childhood self-control predicts health, wealth, and public safety. Proc. Natl. Acad. Sci. USA 2011, 108, 2693–2698. [Google Scholar] [CrossRef] [PubMed]
- Welch, D.; Poulton, R. Personality influences on change in smoking behavior. Health Psychol. 2009, 28, 292. [Google Scholar] [CrossRef]
- Littlefield, A.K.; Sher, K.J.; Wood, P.K. A personality-based description of maturing out of alcohol problems: Extension with a five-factor model and robustness to modeling challenges. Addict. Behav. 2010, 35, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Roberts, B.W.; Bogg, T. A longitudinal study of the relationships between conscientiousness and the social-environmental factors and substance-use behaviors that influence health. J. Personal. 2004, 72, 325–354. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Year | Age | Population | F (%) | M (%) | Study Design | Purpose |
|---|---|---|---|---|---|---|---|
| Rapkin and Fischer | 1992 | mean = 73.3 | n = 179 | 23.20% | 76.80% | Cross-sectional study/scale | Examined how individual differences among elders influence goals in key life domains |
| Resnick, Orwig et al. | 2005 | mean = 80.9 | n = 70 | 100% | N/A | Naturalistic or constructivist inquiry with single open-ended interview | Investigated how older women with hip fractures reacted to a motivational intervention designed to increase adherence to exercise |
| Churchill and Jessop | 2010 | mean = 33.05 | n = 256 | 79.36% | 20.64% | Prospective study | Investigated whether impulsivity moderated any effects of self-initiated implementation on avoiding snacking |
| Hankonen, Vollmann et al. | 2010 | 50–65 | n = 385 | 74% | 26% | Longitudinal study | Studied whether modifiable and domain-specific social cognition, relatively stable and broad personality traits are the best predictors of waist circumference changes |
| Lethbridge, Watson et al. | 2011 | mean = 26.02 mean = 31.42 | E: n = 238 C: n = 248 | 100% | N/A | Case–control study | Studied role of perfectionism, shape and weight overvaluation, dichotomous thinking, and conditional goals in psychopathology of eating disorders |
| Watson, Raykos et al. | 2011 | mean = 26.33 | n = 201 | 100% | N/A | Cross-sectional study | Examined mediators of relationship between perfectionism and eating disorder psychopathology in a clinical sample |
| Palmer, Martin et al. | 2014 | S: mean = 50.1 H: mean = 50.7 (SD: 11.6) | Schizophrenia: n = 72 Healthy: n = 64 | S:54.2% H:62.5% | S:45.8 H:37.5 | Case–control study, interviews, and review of available medical records with SAPS/SANS/CES-D/BSI-A scale | Studied happiness in 72 outpatients with non-remitted chronic schizophrenia with a mean duration of 10 years |
| Smagula, Faulkner et al. | 2016 | mean = 81.4 (SD: 5.04) | n = 613 | N/A | 100% | Cross-sectional study | Evaluated relationships between specific personality factors and health |
| Kahlbaugh and Huffman | 2017 | 65–97 | n = 49 | 65.31% | 34.69% | Cross-sectional study/scale | Examined personality traits of older adults and their emotional experiences associated with engaging in specific leisure activities |
| Smith, Williams et al. | 2017 | 21–65 | n = 94 | 68.08% | 31.92% | Cross-sectional study | (i) Determined if Big Five personality traits are associated with physical activity over two weeks; (ii) assessed whether social-cognitive constructs predict physical activity; (iii) compared participants at various activity levels regarding differences in social-cognitive constructs and personality factors; (iv) examined the impact of personality and social cognitions on physical activity behavior |
| Briki | 2018 | 18–65 | n = 501 | 58.70% | 41.30% | Cross-sectional study | Investigated relationships between personality, LTPA, and feelings |
| Jarrahi, Gafinowitz et al. | 2018 | NA | n = 29 | 65.52% | 34.48% | Cross-sectional study | Explored how different types of pre-existing motivation shape people’s perception and adoption of the device |
| Javaras, Williams et al. | 2019 | N/A | N/A | N/A | N/A | Systematic review | Overview of existing cognitive behavioral, metacognitive, and cognitive remediation interventions to influence conscientiousness, providing several suggestions |
| Briki and Dagot | 2020 | mean = 33.63 | n = 418 | 66.70% | 33.30% | Pilot study: 10-item Flow Short Scale/ questionnaire | Presumed that conservatives are happier than liberals because they develop better mental adjustment especially under contextual threat |
| Davis, Murphy et al. | 2020 | 45–75 | n = 28 | N/A | N/A | Pre-post pilot study | Evaluated pilot 12-week physical activity and diet program delivered by virtual assistant |
| Kappes and Thomsen | 2020 | Study 1: mean = 32.65 Study 2: mean = 25.9 | Study 1: n = 67 Study 2: n = 60 * n-couples | N/A | N/A | Cross-sectional study | Analyzed whether viewing a partner’s regulatory technique would encourage imitation when faced with similar problems pursuing a goal and translated to overcoming challenges in a different setting; also evaluated impact of boundary conditions on imitation of goal regulatory processes |
| Stieger, Robinson et al. | 2020 | 35–69 | n = 52 | 71.20% | 28.80% | Cross-sectional study | Examined whether personality traits predict the extent to which people increase their number of daily steps over 35 days |
| Bischoff, Baumann et al. | 2021 | mean = 47.7 | n = 1008 | 59% | 41% | Web-based survey | Identified requirements for a tailored app to reduce stress in a cohort of highly stressed families |
| Kim, Nho et al. | 2021 | 40–60 | E: n = 31 C: n = 32 | 100% | N/A | Randomized control group pretest–post-test | Examined lifestyle changes for low-income middle-aged women to actively manage risk factors |
| Sirois | 2021 | mean = 34.03 | n = 191 | 67.50% | 32.50% | Prospective cohort study | Investigated association between procrastination and self-regulatory processes as reflected in efficacy |
| Allen, Gmelin et al. | 2022 | mean = 84.3 | n = 1670 | N/A | 100% | Cross-sectional study | Examined association between personality measures and perceived mental fatigability |
| Zimmermann and Chakravarti | 2022 | 35–44 | n = 281 | 44% | 56% | Dilution effect studies | Investigated whether people who are physically active on a regular basis make different decisions than people who are not |
| mean = 36 | n = 289 | 52% | 48% | ||||
| mean = 38 | n = 120 | 61% | 39% | ||||
| 45–49 | n = 268 | 49% | 51% | ||||
| mean = 34 | n = 257 | 47% | 53% |
| Category | Source | Subcategories | Detailed Information |
|---|---|---|---|
| Healthy lifestyle behaviors | Literature and interviews | Physical exercise (using electronic devices) | “Planned, structured, repeated and with maintenance” [21], with intention and beliefs |
| Literature | Healthy eating habits | Weight control and nutrition management | |
| Engaging in social activities | / | ||
| Goal setting | Literature | Types of goals | Achievement, maintenance, disengagement/engagement, and compensation goals [47]; preventative and personalized goals for “hoped-for” possible self and “feared-for” possible self |
| Interviews | Types of goals | Personalized, generalized, ultimate, and progressive goals | |
| Personality | Literature | Big Five personality traits | Openness, conscientiousness, extraversion, agreeableness, neuroticism |
| Interviews | Optimism | Likes to make friends, engage in social activities | |
| Introversion | Curious, anxious, and impatient but open-minded |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, M.Y.C.; Ou, K.-l.; Chung, P.K. Healthy Lifestyle Behavior, Goal Setting, and Personality among Older Adults: A Synthesis of Literature Reviews and Interviews. Geriatrics 2022, 7, 131. https://doi.org/10.3390/geriatrics7060131
Wong MYC, Ou K-l, Chung PK. Healthy Lifestyle Behavior, Goal Setting, and Personality among Older Adults: A Synthesis of Literature Reviews and Interviews. Geriatrics. 2022; 7(6):131. https://doi.org/10.3390/geriatrics7060131
Chicago/Turabian StyleWong, Ming Yu Claudia, Kai-ling Ou, and Pak Kwong Chung. 2022. "Healthy Lifestyle Behavior, Goal Setting, and Personality among Older Adults: A Synthesis of Literature Reviews and Interviews" Geriatrics 7, no. 6: 131. https://doi.org/10.3390/geriatrics7060131
APA StyleWong, M. Y. C., Ou, K.-l., & Chung, P. K. (2022). Healthy Lifestyle Behavior, Goal Setting, and Personality among Older Adults: A Synthesis of Literature Reviews and Interviews. Geriatrics, 7(6), 131. https://doi.org/10.3390/geriatrics7060131