
Informal Caregivers’ Perceptions of Self-Efficacy and Subjective Well-Being When Using Telecare in the Home Environment: A Qualitative Study


Abstract
:1. Introduction
1.1. Background
1.1.1. The Concepts of IC Subjective Well-Being and Self-Efficacy
1.1.2. ICs’ SWB and SE in the Context of Telecare Use
2. Materials and Methods
2.1. Study Design and Recruitment
2.2. Apparatus
2.3. Participants
2.4. Analysis
2.5. Ethical Review
3. Results
3.1. Characteristics of Study Participants
3.2. Emergency Interventions and Use of Telecare Solutions during the Intervention
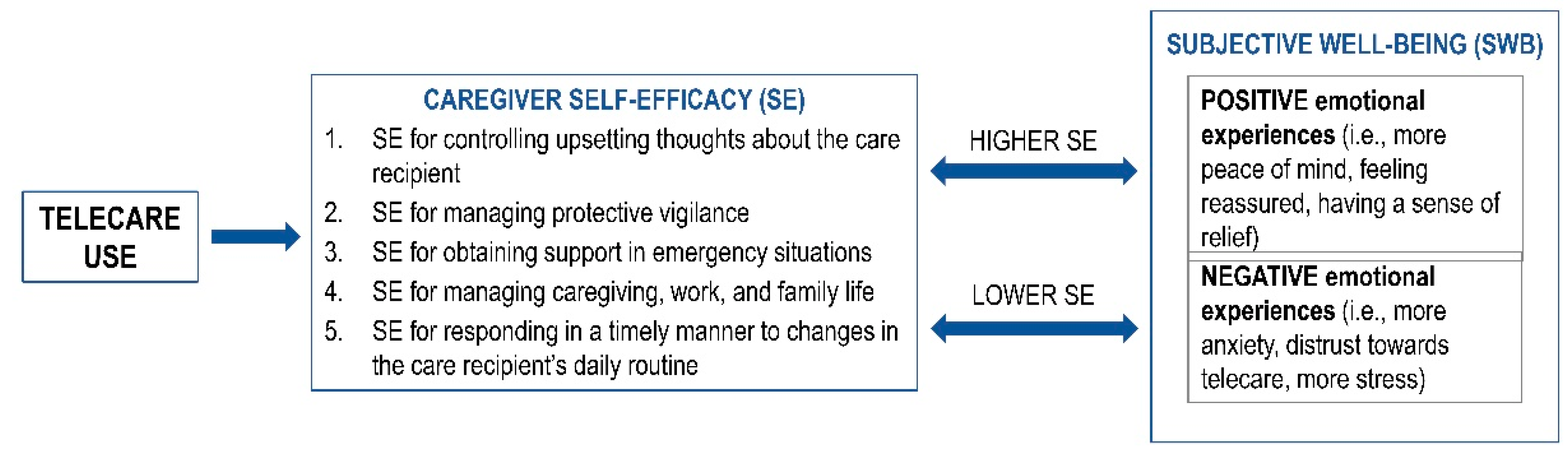
3.3. Caregiver Self-Efficacy and Subjective Well-Being
3.3.1. SE for Controlling Upsetting Thoughts about the Care Recipient
“Sure, yeah, those safety concerns are a strong pressure. I’ve woken up many times thinking, ‘what if,’ but you’re not going to call the person in the middle of the night, are you? So I’ve thought, who knows if she’s okay or not, especially if she was, let’s say, a little sick the day before. And that was hard for me. Now at least I know if, if something was wrong, she could notify me.”(IC14, F, 57)
“Yes, indeed, that was a concern for me. When I called her and she did not pick up the phone. In such cases, she might have fallen or who knows what worse. Mostly I got the information about her from her neighbour, but much later than I should have. Now it’s really more convenient. If she doesn’t answer, I just check the app to see what room she’s in. I know if something was wrong, she could press the button and I would be notified. That gives me peace of mind. In that sense, I knew she was under control, so to speak.”(IC4, F, 45)
“My mother doesn’t want to burden me, so she keeps quiet about some details, she doesn’t even say it, the neighbours do. Maybe that’s why I have an even bigger fantasy, ‘did something happen and she didn’t tell, maybe she just doesn’t want to tell me.’ So you have an extra check, an extra means of having some extra information that allows you to help her, but also to help yourself, so you feel like you’ve done more than just the minimum of the minimum.”(IC21, M, 45)
“As long as the alarm is on, I have that in mind. I’m not going to call her for something unimportant, at seven in the morning.”(IC10, M, 66)
“These false alarms were a problem for me at first, but later it was ok. But even if you put those notifications aside a little bit, you still think, ‘What if something really is wrong?’”(IC22, F, 48)
3.3.2. SE for Managing Protective Vigilance
“So, you set the device and if she forgets she left something on the stove, then the alarm goes off, so the fear of her burning something is no longer there.”(IC15, F, 62)
“the sense of calm that you say to yourself, look, I see, I call, I know where she is. So there’s definitely a sense of calmness there, which is also why I would like to use it in the future.”(IC1, F, 47)
“We still have to check on him because, look, if you check on him at six in the morning before you go to work, and in between that woman comes, and it’s five in the afternoon when work is over, and you still have to check on him. But in between, you didn’t worry about it. At work. When you’re at work, you don’t think about him as much. Actually, I don’t think about him at all anymore.”(IC12, F, 54)
“Now we have this device, which replaces the neighbor as much as possible. Now you look at the phone and you can continue to enjoy the holiday.”(IC15, F, 62)
“In the past, if she fell, you kind of didn’t know she could call someone if she didn’t have a phone nearby. But now she wears an alarm watch on her arm all the time. I’ve been looking for something like this for a while.”(IC15, F, 62)
“I’ll tell you, this solution almost brought me to the brink of life once when it didn’t work properly. When there was a false alarm.”(IC3, M, 56)
“If something really happened to her, and I didn’t get a text message, I would blame myself, ‘Oh, why did we rely on this device.’”(IC2, F, 35)
“Since there’s still a chance my mother might go somewhere, you can’t solve this with the sensors. Even if I assumed she wasn’t going anywhere right now, I couldn’t really know that she wasn’t going somewhere. So in that respect, it didn’t reassure me.”(IC8, F, 54)
3.3.3. SE for Obtaining Support in Emergency Situations
“You’re not on your own anymore and you don’t have to constantly monitor her, now there’s an app like this to help you do that.”(IC13, F, 54)
“Now you have someone controlling the situation. A system in the background that works for you. Otherwise, I’d have to take handle it myself.”(IC10, M, 66)
“Call center is what makes you feel, or let’s say it gives you some time to yourself. You have the feeling that there is someone on duty there and not you.”(IC5, M, 55).
“I wouldn’t help myself much with it [referring to a call center] if my mother was alone when she fell. I can assume that she would be able to say something in such a situation, but maybe she wouldn’t be.”(IC8, F, 54).
“With her illness, everything that happens is serious, and all that is needed is an ambulance and people who are trained to deal with such situations. So in her case, the call center wouldn’t be able to respond that quickly and resolve the situation.”(IC6, M, 55)
“Yes, that’s what worries me, because last time the alarm went off by itself, I really don’t know why, my mother doesn’t know why either. I don’t know what happened, but then they didn’t call her at all to check on her.”(IC14, F, 57)
3.3.4. SE for Managing Caregiving, Work, and Family Life
“I called her while I was at work. Before noon. Now I don’t. I check the app now and see she’s fine. I spend less time on the calls, to be perfectly honest. I can do a little more at work. Outside of work, I call her just like I used to because we’re used to hearing each other every day.”(IC11, F, 67)
“One simply makes other errands more carefree. And you make them easier. And then, of course, everything gets better. It’s a chain reaction.”(IC16, M, 48)
“I don’t know what it would be like if I didn’t have this app, I’d probably have to drive to another town several times. It’s pretty stressful for me to drive up and down every day.”(IC22, F, 48)
“Now I rarely go to see her just to see her. I go to do something useful, or to keep her company, so she won’t be bored. Not just to check on her. She’s happy with me and even compliments me, which hasn’t happened before.”(IC10, M, 66)
“On some occasions you had to rush from a social event immediately, but now you are calm, relaxed, you take your time. For you know that all is well.”(IC 15, F, 62).
“I have basically lost some peace of mind. I have a bigger problem now because this device has awakened all these things in me, and now I feel some moral responsibility, and before I was not aware of the whole situation. Sometimes I felt bad, but I said to myself, ‘Okay, I’m going to compensate by calling her and giving her more that way.’ Sometimes I was reminded, ‘We should meet with her.’”(IC2, F, 35)
3.3.5. SE for Responding in a Timely Manner to Changes in the Care Recipient’s Daily Routine
“The benefit for me was that I started thinking about all these things. Now we’re much more aware that we need to sit down one day and talk about how we’re going to handle things in the future. It’s better to talk about these things earlier and get the opinion of the loved one you care for when you know she still has sound judgment.”(IC2, F, 35)
“The information about her movement in the apartment also allowed us to communicate with my mother about using the toilet, which is very important for her health. She shouldn’t be accumulating water in her bladder and maybe she wasn’t taking the pill to eliminate water. Now we can see exactly how often she used the toilet. So I would say that the solution has worked for us.”(IC6, M, 55)
“I basically knew her daily routine. Her daily movements conformed to a pattern with which I became familiar. If something happened, like she went somewhere at the usual time or didn’t get up or something, I knew something wasn’t as it should be and something might have happened to her.”(IC5, M, 55)
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eurocarers. Enabling Carers to Care. An EU Strategy to Support and Empower Informal Carers; Eurocarers; European Association Working for Carers Eurocarers: Brussels, Belgium, 2018; p. 16. Available online: https://eurocarers.org/eu-strategy-to-support-and-empower-informal-carers-across-europe/ (accessed on 25 April 2021).
- Hlebec, V.; Rakar, T.; Dolničar, V.; Petrovčič, A.; Filipovič Hrast, M. Intergenerational Solidarity in Slovenia: Key Issues. In Families and Family Values in Society and Culture (Perspectives on Human Development); Albert, I., Ed.; Information Age: Charlotte, NC, USA, 2021; pp. 359–380. [Google Scholar]
- International Labour Organization. Care Work and Care Jobs for the Future of Decent Work; International Labour Organization: Geneva, Switzerland, 2018; p. 256. [Google Scholar]
- Spasova, S.; Baeten, R.; Coster, S.; Ghailani, D.; Peña-Casas, R.; Vanhercke, C. Challenges in Long-Term Care in Europe—A Study of National Policies; European Commission, Directorate-General for Employment, Social Affairs and Inclusion: Brussels, Belgium, 2018; Available online: https://ec.europa.eu/social/BlobServlet?docId=20225&langId=en (accessed on 25 January 2020).
- Zigante, V. The Role of New Technologies in Modernising Long-Term Care Systems—A Scoping Review; Social Situation Monitor; Publications Office of the European Union: Luxembourg, 2021; ISBN 978-92-76-28928-9. Available online: https://ec.europa.eu/social/BlobServlet?docId=23362&langId=mt (accessed on 8 May 2022).
- Bauer, J.M.; Sousa-Poza, A. Impacts of Informal Caregiving on Caregiver Employment, Health, and Family. J. Popul. Ageing 2015, 8, 113–145. [Google Scholar] [CrossRef]
- Social Protection Committee (SPC); European Commission (DG EMPL). Long-Term Care Report 2021. Trends, Challenges and Opportunities in an Ageing Society—Volume I; Publications Office of the European Union: Luxembourg, 2021; Available online: https://www.socialserviceworkforce.org/system/files/resource/files/longtermcare.pdf (accessed on 15 January 2022).
- Social Protection Committee (SPC); European Commission (DG EMPL). Long-Term Care Report 2021 Trends, Challenges and Opportunities in an Ageing Society—Volume II, Country Porofiles; Publications Office of the European Union: Luxembourg, 2021; Available online: https://op.europa.eu/en/publication-detail/-/publication/b39728e3-cd83-11eb-ac72-01aa75ed71a1 (accessed on 15 January 2022).
- Willert, B.; Minnotte, K.L. Informal Caregiving and Strains: Exploring the Impacts of Gender, Race, and Income. Appl. Res. Qual. Life 2021, 16, 943–964. [Google Scholar] [CrossRef]
- da Rocha, C.G.; Perrenoud, B.; Ramelet, A.-S. Perceptions of Burden and Preparedness for Caregiving among the Family Caregivers of Hospitalised Older Adults: A Cross-Sectional Study. Geriatrics 2022, 7, 19. [Google Scholar] [CrossRef] [PubMed]
- Bednaš, M.; Kajzer, A. (Eds.) Active Ageing Strategy; Institute of Macroeconomic Analysis and Development of the Republic of Slovenia; Ministry of Labour, Family, Social Affairs and Equal Opportunities: Ljubljana, Slovenia, 2018. Available online: https://www.gov.si/assets/ministrstva/MDDSZ/Direktorat-za-starejse-in-deinstitucionalizacijo/strategije/Active-Ageing-Strategy-2017.pdf (accessed on 12 March 2020).
- Eurocarers. Eurocarers’ Position Paper: Information & Communication Technology (ICT) for Informal Carers; Eurocarers: Brussels, Belgium, 2021; Available online: https://eurocarers.org/download/37473/ (accessed on 5 February 2022).
- European Ageing Network. Long-Term Care 2030; European Ageing Network: Tábor, Czech Republic, 2019; Available online: https://www.ean.care/en/articles/long-term-care-2030 (accessed on 20 February 2022).
- Doughty, K.; Monk, A.; Bayliss, C.; Brown, S.; Dewsbury, L.; Dunk, B.; Gallagher, V.; Grafham, K.; Jones, M.; Lowe, C.; et al. Telecare, Telehealth and Assistive Technologies: Do We Know What We’re Talking About? Hous. Care Support 2008, 11, 36–41. [Google Scholar] [CrossRef]
- Karlsen, C.; Moe, C.E.; Haraldstad, K.; Thygesen, E. Caring by Telecare? A Hermeneutic Study of Experiences among Older Adults and Their Family Caregivers. J. Clin. Nurs. 2019, 28, 1300–1313. [Google Scholar] [CrossRef] [PubMed]
- Robertson, T.; Durick, J.; Brereton, M.; Vetere, F.; Howard, S.; Nansen, B. Knowing Our Users: Scoping Interviews in Design Research with Ageing Participants. In Proceedings of the 24th Australian Computer-Human Interaction Conference, Melbourne, Australia, 26–30 November 2012; Association for Computing Machinery: New York, NY, USA; pp. 517–520. [Google Scholar]
- Smole-Orehek, K.; Hvalič-Touzery, S.; Petrovčič, A.; Dolnicar, V.; Debevc, M.; Kozuh, I. Psychological Outcomes of ECare Technologies Use for Informal Carers: A Scoping Study. Gerontechnology 2019, 18, 15–28. [Google Scholar] [CrossRef]
- Sriram, V.; Jenkinson, C.; Peters, M. Informal Carers’ Experience of Assistive Technology Use in Dementia Care at Home: A Systematic Review. BMC Geriatr. 2019, 19, 160. [Google Scholar] [CrossRef]
- Lindeman, D.A.; Kim, K.K.; Gladstone, C.; Apesoa-Varano, E.C. Technology and Caregiving: Emerging Interventions and Directions for Research. Gerontologist 2020, 60, S41–S49. [Google Scholar] [CrossRef]
- Ryff, C.D. Happiness Is Everything, or Is It? Explorations on the Meaning of Psychological Well-Being. J. Personal. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Taneva, S. What Is Psychological Well-Being and How It Changes throughout the Employment Cycle? In Trabalho, Saúde e Sustentabilidade: Construindo a Cidadania = Work, Health and Sustainability: Building Citizenship; Monteiro, I., Iguti, A.M., Eds.; UnicampBFCM: Campinas, Brazil, 2016; pp. 83–90. ISBN 978-85-68467-03-9. [Google Scholar]
- Diener, E. Subjective Well-Being; Social Science Research Network: Rochester, NY, USA, 1984. [Google Scholar]
- Tov, W. Well-Being Concepts and Components. In Handbook of Well-Being; Diener, E., Oishi, S., Tay, L., Eds.; DEF Publishers: Salt Lake City, UT, USA, 2018. [Google Scholar]
- Zheng, L.; Li, G.; Gao, D.; Wang, S.; Meng, X.; Wang, C.; Yuan, H.; Chen, L. Cognitive Frailty as a Predictor of Dementia among Older Adults: A Systematic Review and Meta-Analysis. Arch. Gerontol. Geriatr. 2020, 87, 103997. [Google Scholar] [CrossRef]
- Chudzicka-Czupała, A.; Zalewska-Łunkiewicz, K. Subjective Well-Being, General Self-Efficacy and Coping with Stress in Former Psychiatric Patients Preparing for the Peer Support Role: An Exploratory Study. Health Qual. Life Outcomes 2020, 18, 98. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Butler, J. Self-Efficacy. In Encyclopedia of Behavioral Medicine; Springer: New York, NY, 2013; pp. 1737–1738. [Google Scholar]
- Ajzen, I. The Theory of Planned Behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Crellin, N.E.; Orrell, M.; McDermott, O.; Charlesworth, G. Self-Efficacy and Health-Related Quality of Life in Family Carers of People with Dementia: A Systematic Review. Aging Ment. Health 2014, 18, 954–969. [Google Scholar] [CrossRef]
- Steffen, A.M.; McKibbin, C.; Zeiss, A.M.; Gallagher-Thompson, D.; Bandura, A. The Revised Scale for Caregiving Self-EfficacyReliability and Validity Studies. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, P74–P86. [Google Scholar] [CrossRef] [PubMed]
- Hampton, M. Self-Efficacy of Caregiving and Caregiver Stress in Adult Informal Caregivers of Individuals at End of Life. Ph.D. Thesis, The University of Texas at Arlington, Arlington, TX, USA, 2014. [Google Scholar]
- Keefe, F.J.; Ahles, T.A.; Porter, L.S.; Sutton, L.M.; McBride, C.M.; Pope, M.S.; McKinstry, E.T.; Furstenberg, C.P.; Dalton, J.; Baucom, D.H. The Self-Efficacy of Family Caregivers for Helping Cancer Patients Manage Pain at End-of-Life. Pain 2003, 103, 157–162. [Google Scholar] [CrossRef]
- Hampton, M.; Newcomb, P. Self-Efficacy and Stress Among Informal Caregivers of Individuals at End of Life. J. Hosp. Palliat. Nurs. 2018, 20, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Merluzzi, T.V.; Philip, E.J.; Vachon, D.O.; Heitzmann, C.A. Assessment of Self-Efficacy for Caregiving: The Critical Role of Self-Care in Caregiver Stress and Burden. Palliat. Support. Care 2011, 9, 15–24. [Google Scholar] [CrossRef]
- Andersson, S.; Erlingsson, C.; Magnusson, L.; Hanson, E. Information and Communication Technology-Mediated Support for Working Carers of Older Family Members: An Integrative Literature Review. Int. J. Care Caring 2017, 1, 247–273. [Google Scholar] [CrossRef]
- Carretero, S.; Stewart, J.; Centeno, C. Information and Communication Technologies for Informal Carers and Paid Assistants: Benefits from Micro-, Meso-, and Macro-Levels. Eur. J. Ageing 2015, 12, 163–173. [Google Scholar] [CrossRef]
- Davies, A.; Rixon, L.; Newman, S. Systematic Review of the Effects of Telecare Provided for a Person with Social Care Needs on Outcomes for Their Informal Carers. Health Soc. Care Community 2013, 21, 582–597. [Google Scholar] [CrossRef]
- Jarrold, K.; Yeandle, S. A Weight off My Mind: Exploring the Impact and Potential Benefits of Telecare for Unpaid Carers in Scotland; Carers Scotland, Scottish Joint Improvement Team: Glasgow, UK, 2009; p. 43. [Google Scholar]
- TMT Editorial Team. Caregivers & Technology: What They Want and Need A Guide for Innovators—Research from A Nationally Representative Sample of America’s 40 Million Family Caregivers. Telehealth Med. Today 2017, 2, 4–27. [Google Scholar] [CrossRef]
- Cook, E.J.; Randhawa, G.; Guppy, A.; Sharp, C.; Barton, G.; Bateman, A.; Crawford-White, J. Exploring Factors That Impact the Decision to Use Assistive Telecare: Perspectives of Family Care-Givers of Older People in the United Kingdom. Ageing Soc. 2018, 38, 1912–1932. [Google Scholar] [CrossRef]
- Karlsen, C.; Ludvigsen, M.S.; Moe, C.E.; Haraldstad, K.; Thygesen, E. Experiences of the Home-Dwelling Elderly in the Use of Telecare in Home Care Services: A Qualitative Systematic Review. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 1249–1255. [Google Scholar] [CrossRef]
- Rabinowitz, Y.G.; Mausbach, B.T.; Gallagher-Thompson, D. Self-Efficacy as a Moderator of the Relationship between Care Recipient Memory and Behavioral Problems and Caregiver Depression in Female Dementia Caregivers. Alzheimer Dis. Assoc. Disord. 2009, 23, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Hattink, B.J.J.; Meiland, F.J.M.; Overmars-Marx, T.; de Boer, M.; Ebben, P.W.G.; van Blanken, M.; Verhaeghe, S.; Stalpers-Croeze, I.; Jedlitschka, A.; Flick, S.E.; et al. The Electronic, Personalizable Rosetta System for Dementia Care: Exploring the User-Friendliness, Usefulness and Impact. Disabil. Rehabil. Assist. Technol. 2016, 11, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Hvalič Touzery, S.; Lebar, L.; Petrovčič, A.; Smole-Orehek, K.; Dolničar, V. Psychological Outcomes of Telecare Use for Working Family Carers of Older People. In Proceedings of the Smart Living Forum 2019, Villach, Austria, 14 November 2019; BoD: Norderstedt, Germany, 2020; pp. 26–33. [Google Scholar]
- Lobo, M.A.; Kagan, S.H.; Corrigan, J.D. Research Design Options for Intervention Studies. Pediatr. Phys. Ther. 2017, 29, S57–S63. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V.; Weate, P. Using Thematic Analysis in Sport and Exercise Research. In Routledge Handbook of Qualitative Research in Sport and Exercise; Routledge: London, UK, 2016. [Google Scholar] [CrossRef]
- Fereday, J.; Muir-Cochrane, E. Demonstrating Rigor Using Thematic Analysis: A Hybrid Approach of Inductive and Deductive Coding and Theme Development. Int. J. Qual. Methods 2006, 5, 80–92. [Google Scholar] [CrossRef]
- Saldaña, J. The Coding Manual for Qualitative Researchers, 2nd ed.; Sage: London, UK, 2013; ISBN 978-1-4462-7142-1. [Google Scholar]
- Boyatzis, R.E. Transforming Qualitative Information: Thematic Analysis and Code Development; Sage Publications: Thousand Oaks, CA, USA, 1998; ISBN 978-0-7619-0960-6. [Google Scholar]
- Braun, V.; Clarke, V. Successful Qualitative Research: A Practical Guide for Beginners; Sage: London, UK, 2013; ISBN 978-1-84787-581-5. [Google Scholar]
- Elliott, V. Thinking about the Coding Process in Qualitative Data Analysis. Qual. Rep. 2018, 23, 2850–2861. [Google Scholar] [CrossRef]
- Eurofamcare Consortium. The Questionnaire: The Common Assessment Tool [CAT] for the Family Caregiver Interview. 2004. Available online: https://www.uke.de/extern/eurofamcare/documents/deliverables/cat_uk.pdf (accessed on 10 September 2019).
- Lewis, V.; Bauer, M.; Winbolt, M.; Chenco, C.; Hanley, F. A Study of the Effectiveness of MP3 Players to Support Family Carers of People Living with Dementia at Home. Int. Psychogeriatr. 2015, 27, 471–479. [Google Scholar] [CrossRef]
- Butcher, H.K.; Holkup, P.A.; Park, M.; Maas, M. Thematic Analysis of the Experience of Making a Decision to Place a Family Member with Alzheimer’s Disease in a Special Care Unit. Res. Nurs. Health 2001, 24, 470–480. [Google Scholar] [CrossRef]
- Mooney, J.; Graham, K.; Watts, R.A. Impact of Caring for Someone with a Rare Rheumatic Condition, Views from Patients and Informal Carers-the Need for Cat-like Vigilance. Rheumatol. Adv. Pract. 2019, 3, rkz003. [Google Scholar] [CrossRef] [PubMed]
- Zigante, V. Informal Care in Europe: Exploring Formalisation, Availability and Quality; Publications Office: Brussels, Belgium, 2018; ISBN 978-92-79-86583-1. [Google Scholar]
- Heath, A.; Carey, L.B.; Chong, S. Helping Carers Care: An Exploratory Study of Factors Impacting Informal Family Carers and Their Use of Aged Care Services. J. Relig. Health 2018, 57, 1146–1167. [Google Scholar] [CrossRef] [PubMed]
- Leslie, M.; Gray, R.P.; Eales, J.; Fast, J.; Magnaye, A.; Khayatzadeh-Mahani, A. The Care Capacity Goals of Family Carers and the Role of Technology in Achieving Them. BMC Geriatr. 2020, 20, 52. [Google Scholar] [CrossRef]
- Huber, L.L.; Shankar, K.; Caine, K.; Connelly, K.; Camp, L.J.; Walker, B.A.; Borrero, L. How In-Home Technologies Mediate Caregiving Relationships in Later Life. Int. J. Hum.–Comput. Interact. 2013, 29, 441–455. [Google Scholar] [CrossRef]
- Torp, S.; Bing-Jonsson, P.C.; Hanson, E. Experiences with Using Information and Communication Technology to Build a Multi-Municipal Support Network for Informal Carers. Inform. Health Soc. Care 2013, 38, 265–279. [Google Scholar] [CrossRef] [PubMed]
- Keck, W.; Saraceno, C. Balancing Elderly Care and Employment in Germany; Wissenschaftszentrum Berlin für Sozialforschung (WZB): Berlin, Germany, 2009. [Google Scholar]
- Plaisier, I.; van Groenou, M.I.B.; Keuzenkamp, S. Combining Work and Informal Care: The Importance of Caring Organisations. Hum. Resour. Manag. J. 2015, 25, 267–280. [Google Scholar] [CrossRef]
- European Commission. Adequate Social Protection for Long-Term Care Needs in an Ageing Society. Report Jointly Prepared by the Social Protection Committee and the European Commission; Publications Office of the European Union: Luxembourg, 2014; Available online: https://op.europa.eu/en/publication-detail/-/publication/71532344-ddf1-4d34-a7aa-f65c701a22a2/language-en (accessed on 7 June 2019).
- World Health Organisation Regional Office for Europe. Health 2020—A European Policy Framework Supporting Action across Government and Society for Health and Well-Being; World Health Organisation Regional Office for Europe: Copenhagen, Denmark, 2013; Available online: https://apps.who.int/iris/handle/10665/131300 (accessed on 7 June 2022).
- World Health Organization Regional Office for Europe. Strategy and Action Plan for Healthy Ageing in Europe, 2012–2020; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2012; Available online: https://www.euro.who.int/__data/assets/pdf_file/0008/175544/RC62wd10Rev1-Eng.pdf (accessed on 7 June 2022).
- Carers UK; EFC—Employers for Carers. Supporting Working Carers: The Benefits to Families, Business and the Economy; Carers UK: London, UK, 2013. Available online: https://www.gov.uk/government/publications/supporting-working-carers-the-benefits-to-families-business-and-the-economy (accessed on 3 May 2022).
- Powell, C.; Blighe, A.; Froggatt, K.; McCormack, B.; Woodward-Carlton, B.; Young, J.; Robinson, L.; Downs, M. Family Involvement in Timely Detection of Changes in Health of Nursing Homes Residents: A Qualitative Exploratory Study. J. Clin. Nurs. 2018, 27, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, K.L.; Stewart, B.J.; Archbold, P.G. Conceptualization and Measurement of Doing Family Caregiving Well. Image J. Nurs. Sch. 1998, 30, 63–69. [Google Scholar] [CrossRef]
- Lucero, R.J.; Fehlberg, E.A.; Patel, A.G.M.; Bjarnardottir, R.I.; Williams, R.; Lee, K.; Ansell, M.; Bakken, S.; Luchsinger, J.A.; Mittelman, M. The Effects of Information and Communication Technologies on Informal Caregivers of Persons Living with Dementia: A Systematic Review. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2019, 5, 1–12. [Google Scholar] [CrossRef]
- Schwarzer, R.; Jerusalem, M. Generalized Self-Efficacy Scale. In Measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs; Weinman, J., Wright, S., Johnston, M., Eds.; NFER-NELSON: Windsor, UK, 1995; pp. 35–37. [Google Scholar]
- Zeiss, A.; Gallagher-Thompson, D.; Lovett, S.; Rose, J.; McKibbin, C. Self-Efficacy as a Mediator of Caregiver Coping: Development and Testing of an Assessment Model. J. Clin. Geropsychol. 1999, 5, 221. [Google Scholar] [CrossRef]
- McDonald, T.; Siegall, M. The Effects of Technological Self-Efficacy and Job Focus on Job Performance, Attitudes, and Withdrawal Behaviors. J. Psychol. 1992, 126, 465–475. [Google Scholar] [CrossRef]
- Lobo, E.H.; Abdelrazek, M.; Kensing, F.; Rasmussen, L.J.; Livingston, P.M.; Grundy, J.; Islam, S.M.S.; Frølich, A. Technology-Based Support for Stroke Caregiving: A Rapid Review of Evidence. J. Nurs. Manag. 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Hvalič Touzery, S.; Dolničar, V. Attitudes towards Smart Technologies among Older People and Their Informal Carers in Slovenia. In Proceedings of the Zdravje Starostnikov, Health of the Elderly-Proceedings; Petelin, A., Ed.; University of Primorska Press: Koper, Slovenija, 2021; pp. 71–80. [Google Scholar]
- Hvalič Touzery, S.; Dolničar, V. The Impact of the Care Situation on the Willingness to Use Telecare among Informal Carers of Older People in Slovenia. In Programme and Book of Abstracts, Proceedings of the CoE AgeCare Mid-Term Congress ‘Longer Lives, Better Care?’ Tampere, Finland,16 June 2022; CoE AgeCare, Tampere University: Tampere, Finland; p. 16.
- Sihto, T. Distances and Proximities of Care: Analysing Emotio-Spatial Distances in Informal Caring. Emot. Space Soc. 2018, 29, 62–68. [Google Scholar] [CrossRef]
- Benefield, L.E.; Beck, C. Reducing the Distance in Distance-Caregiving by Technology Innovation. Clin. Interv. Aging 2007, 2, 267–272. [Google Scholar] [PubMed]
- Magnusson, L.; Sandman, L.; Rosén, K.G.; Hanson, E. Extended Safety and Support Systems for People with Dementia Living at Home. J. Assist. Technol. 2014, 8, 188–206. [Google Scholar] [CrossRef]
- Mahoney, D. An Evidence-Based Adoption of Technology Model for Remote Monitoring of Elders’ Daily Activities. Ageing Int. 2011, 36, 66–81. [Google Scholar] [CrossRef]
- Mahoney, D.M.F.; Mutschler, P.H.; Tarlow, B.; Liss, E. Real World Implementation Lessons and Outcomes from the Worker Interactive Networking (WIN) Project: Workplace-Based Online Caregiver Support and Remote Monitoring of Elders at Home. Telemed. e-Health 2008, 14, 224–234. [Google Scholar] [CrossRef]
- Dolničar, V.; Petrovčič, A.; Šetinc, M.; Košir, I.; Kavčič, M. Understanding Acceptance Factors for Using E-Care Systems and Devices: Insights from a Mixed-Method Intervention Study in Slovenia. In Human Aspects of IT for the Aged Population: Applications, Services and Contexts: Third International Conference, ITAP 2017, Held as Part of HCI International 2017, Vancouver, BC, Canada, 9–14 July 2017, Proceedings, Part 2, (Lecture Notes in Computer Science (LNCS), 10298); Zhou, J., Salvendy, G., Eds.; Springer: Cham, Switzerland, 2017; pp. 362–377. [Google Scholar]
- Jaschinski, C.; Ben Allouch, S. Listening to the Ones Who Care: Exploring the Perceptions of Informal Caregivers towards Ambient Assisted Living Applications. J. Ambient. Intell. Humaniz. Comput. 2019, 10, 761–778. [Google Scholar] [CrossRef]
- Roberts, C.; Mort, M. Reshaping What Counts as Care: Older People, Work and New Technologies. Alter 2009, 3, 138–158. [Google Scholar] [CrossRef]
- Pritchard, G.W.; Brittain, K. Alarm Pendants and the Technological Shaping of Older People’s Care: Between (Intentional) Help and (Irrational) Nuisance. Technol. Forecast. Soc. Change 2015, 93, 124–132. [Google Scholar] [CrossRef]
- van Hoof, J.; Kort, H.S.M.; Rutten, P.G.S.; Duijnstee, M.S.H. Ageing-in-Place with the Use of Ambient Intelligence Technology: Perspectives of Older Users. Int. J. Med. Inform. 2011, 80, 310–331. [Google Scholar] [CrossRef] [PubMed]
- Bentley, C.L.; Powell, L.A.; Orrell, A.; Mountain, G.A. Addressing Design and Suitability Barriers to Telecare Use: Has Anything Changed? Technol. Disabil. 2014, 26, 221–235. [Google Scholar] [CrossRef]
- Czaja, S.J. Long-Term Care Services and Support Systems for Older Adults: The Role of Technology. Am. Psychol. 2016, 71, 294–301. [Google Scholar] [CrossRef]
- Hawley-Hague, H.; Boulton, E.; Hall, A.; Pfeiffer, K.; Todd, C. Older Adults’ Perceptions of Technologies Aimed at Falls Prevention, Detection or Monitoring: A Systematic Review. Int. J. Med. Inform. 2014, 83, 416. [Google Scholar] [CrossRef] [PubMed]
- Johannessen, T.B.; Storm, M.; Holm, A.L. Safety for Older Adults Using Telecare: Perceptions of Homecare Professionals. Nurs. Open 2019, 6, 1254–1261. [Google Scholar] [CrossRef]
- Thordardottir, B.; Malmgren Fänge, A.; Lethin, C.; Rodriguez Gatta, D.; Chiatti, C. Acceptance and Use of Innovative Assistive Technologies among People with Cognitive Impairment and Their Caregivers: A Systematic Review. BioMed Res. Int. 2019, 2019, 9196729. [Google Scholar] [CrossRef] [PubMed]
- Dinsmore, J. Avoiding the “Iceberg Effect”: Incorporating a Behaviourial Change Approach to Technology Design in Chronic Illness. In Aging and the Digital Life Course; Prendergast, D., Garattini, C., Eds.; Berghahn Books: New York, NY, USA; Oxford, UK, 2015; pp. 125–148. ISBN 978-1-78238-691-9. [Google Scholar]
- Arntzen, C.; Holthe, T.; Jentoft, R. Tracing the Successful Incorporation of Assistive Technology into Everyday Life for Younger People with Dementia and Family Carers. Dement. Int. J. Soc. Res. Pract. 2016, 15, 646–662. [Google Scholar] [CrossRef]
- Berridge, C. Breathing Room in Monitored Space: The Impact of Passive Monitoring Technology on Privacy in Independent Living. Gerontologist 2016, 56, 807–816. [Google Scholar] [CrossRef]
- Gibson, G.; Dickinson, C.; Brittain, K.; Robinson, L. The Everyday Use of Assistive Technology by People with Dementia and Their Family Carers: A Qualitative Study. BMC Geriatr. 2015, 15, 89. [Google Scholar] [CrossRef]
- Merkel, S.; Kucharski, A. Participatory Design in Gerontechnology: A Systematic Literature Review. Gerontologist 2019, 59, e16–e25. [Google Scholar] [CrossRef]


{kind=link}
| IC 1 | Age (Years) | Sex | Family Relation | Frequency of Visits | Weekly Hours of Care per Week | Years of Care | Spatial Distance from OP | Subjective Burden of Care | OP’s 2 Dependency 4 | OP’s Overall Health Condition |
|---|---|---|---|---|---|---|---|---|---|---|
| IC1 | 47 | Female | Daughter | At least once a week | 5 | 5 | Within 10 min. drive | Little or no burden | Moderate | Good |
| IC2 | 35 | Female | Daughter-in-law | At least once a month | 5 | 3 | Within walking distance | Little or no burden | Moderate | Fair |
| IC3 | 56 | Male | Son | At least once a week | 3 3 | 2 | Within 30 min. drive | Little or no burden | Slight | Fair |
| IC4 | 45 | Female | Daughter | (Almost) Every day | 4 | 8 | Within 30 min. drive | Moderate burden | Moderate | Poor |
| IC5 | 55 | Male | Son | (Almost) Every day | 5 | 10 | Within 30 min. drive | Moderate burden | Moderate | Good |
| IC6 | 55 | Male | Son | (Almost) Every day | 8 | 25 | Within 10 min. drive | Severe burden | Severe | Fair |
| IC7 | 50 | Female | Daughter | (Almost) Every day | 5 | 2 | Within 30 min. drive | Moderate burden | Moderate | Fair |
| IC8 | 54 | Female | Daughter | (Almost) Every day | 60 | <1 | Within 30 min. drive | Moderate burden | Severe | Fair |
| IC9 | 51 | Male | Son | (Almost) Every day | 14 | 7 | Within walking distance | Moderate burden | Moderate | Fair |
| IC10 | 66 | Male | Son | At least once a week | 4 | <1 | Within 30 min. drive | Moderate burden | Moderate | Poor |
| IC11 | 67 | Female | Daughter | (Almost) Every day | 10 | 1 | Within 30 min. drive | Little or no burden | Slight | Very good |
| IC12 | 54 | Female | Daughter | (Almost) Every day | 14 | 8 | Within 10 min. drive | Moderate burden | Severe | Poor |
| IC13 | 54 | Female | Daughter-in-law | At least once a week | 5 | 1 | Within 10 min. drive | Little or no burden | Slight | Fair |
| IC14 | 57 | Female | Daughter | (Almost) Every day | 10 | 9 | Within 30 min. drive | Moderate burden | Severe | Poor |
| IC15 | 62 | Female | Daughter | At least once a week | 5 | 5 | Within 30 min. drive | Moderate burden | Slight | Fair |
| IC16 | 48 | Male | Son | At least once a week | 4 | <1 | Within 1 h drive | Moderate burden | Slight | Fair |
| IC17 | 55 | Male | Son | (Almost) Every day | 4 | 2 | Within 10 min. drive | Little or no burden | Moderate | Poor |
| IC18 | 61 | Male | Son | At least once a month | 5 | 5 | Within 30 min. drive | Little or no burden | Slight | Very good |
| IC19 | 61 | Female | Daughter | (Almost) Every day | 4 | 10 | Within 10 min. drive | Little or no burden | Slight | Fair |
| IC20 | 62 | Female | Daughter | (Almost) Every day | 12 | 2 | Within 30 min. drive | Moderate burden | Severe | Poor |
| IC21 | 45 | Male | Son | At least once a week | 5 | 4 | Within 30 min. drive | Moderate burden | Slight | Good |
| IC22 | 48 | Female | Daughter | At least once a week | 4 | <1 | Within 30 min. drive | Little or no burden | Slight | Good |
| IC 1 | Telecare Service 2 | Emergency Event | Telecare Use after the Intervention |
|---|---|---|---|
| IC1 | TC1 | No | Yes |
| IC2 | TC1 | No | No |
| IC3 | TC1 | No | Yes |
| IC4 | TC1 | No | Yes |
| IC5 | TC2 | No | No |
| IC6 | TC1 | No | Yes |
| IC7 | TC1 | No | No information |
| IC8 | TC1 | No | No |
| IC9 | TC1 | Yes (care recipient fall) | Yes |
| IC10 | TC1 | No | Yes |
| IC11 | TC1 | No | Yes |
| IC12 | TC2 | Yes (smoke alarm during cooking) | Yes |
| IC13 | TC2 | Yes (care recipient fall) | Yes |
| IC14 | TC2 | No | Yes |
| IC15 | TC2 | No | Yes |
| IC16 | TC2 | No | Yes |
| IC17 | TC2 | Yes (care recipient fall) | Yes |
| IC18 | TC2 | No | No information |
| IC19 | TC1 | No | Yes |
| IC20 | TC1 | Yes (care recipient fall) | Yes |
| IC21 | TC1 | No | Yes |
| IC22 | TC1 | No | No |
| Task-Specific Dimensions of IC SE | Explanation |
|---|---|
| SE for controlling upsetting thoughts about the care recipient | ICs’ sense of control over negative thoughts (e.g., fear for the safety of their care recipient) regarding the care recipient’s situation. |
| SE for managing protective vigilance | ICs’ personal sense of control over the unexpected and potentially harmful events for the care recipient (e.g., knowing that they will be notified immediately if something happens). |
| SE for obtaining support in emergency situations | ICs’ personal belief that they are not alone in the caregiving situation, especially in emergencies. |
| SE for managing caregiving, work, and family life | ICs’ personal belief in their own ability to balance caregiving, work and family life. |
| SE for responding in a timely manner to changes in the care recipient’s daily routine | ICs’ personal belief in their own ability to detect changes in the care recipient’s daily routine in a timely manner. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hvalič-Touzery, S.; Smole-Orehek, K.; Dolničar, V. Informal Caregivers’ Perceptions of Self-Efficacy and Subjective Well-Being When Using Telecare in the Home Environment: A Qualitative Study. Geriatrics 2022, 7, 86. https://doi.org/10.3390/geriatrics7050086
Hvalič-Touzery S, Smole-Orehek K, Dolničar V. Informal Caregivers’ Perceptions of Self-Efficacy and Subjective Well-Being When Using Telecare in the Home Environment: A Qualitative Study. Geriatrics. 2022; 7(5):86. https://doi.org/10.3390/geriatrics7050086
Chicago/Turabian StyleHvalič-Touzery, Simona, Kaja Smole-Orehek, and Vesna Dolničar. 2022. "Informal Caregivers’ Perceptions of Self-Efficacy and Subjective Well-Being When Using Telecare in the Home Environment: A Qualitative Study" Geriatrics 7, no. 5: 86. https://doi.org/10.3390/geriatrics7050086
APA StyleHvalič-Touzery, S., Smole-Orehek, K., & Dolničar, V. (2022). Informal Caregivers’ Perceptions of Self-Efficacy and Subjective Well-Being When Using Telecare in the Home Environment: A Qualitative Study. Geriatrics, 7(5), 86. https://doi.org/10.3390/geriatrics7050086