
Biomarker Signatures of Two Phenotypical Prefrailty Types in the Irish Longitudinal Study on Ageing




Abstract
:1. Introduction
2. Materials and Methods
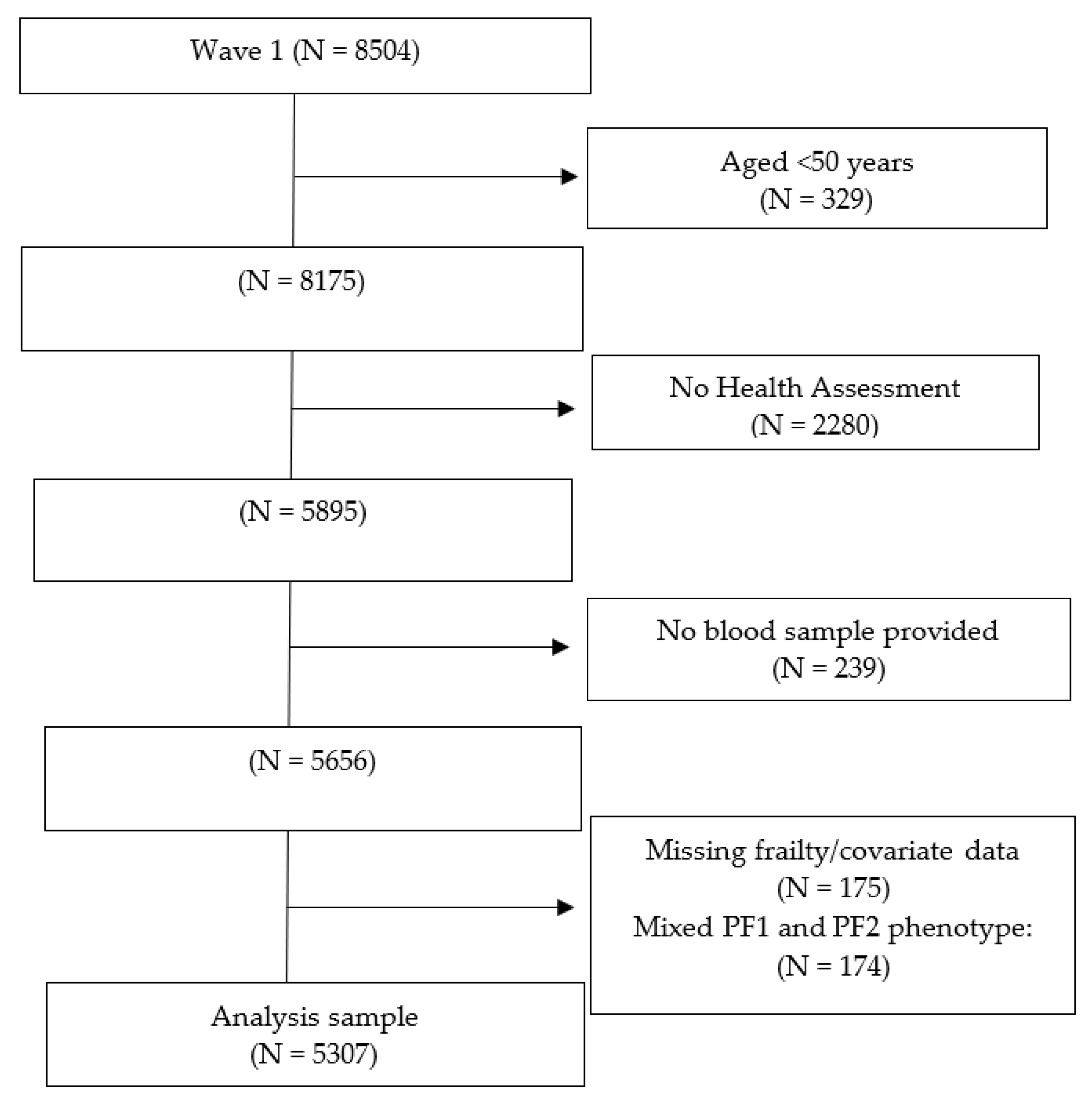
2.1. Study Sample
2.2. Frailty Operationalisation
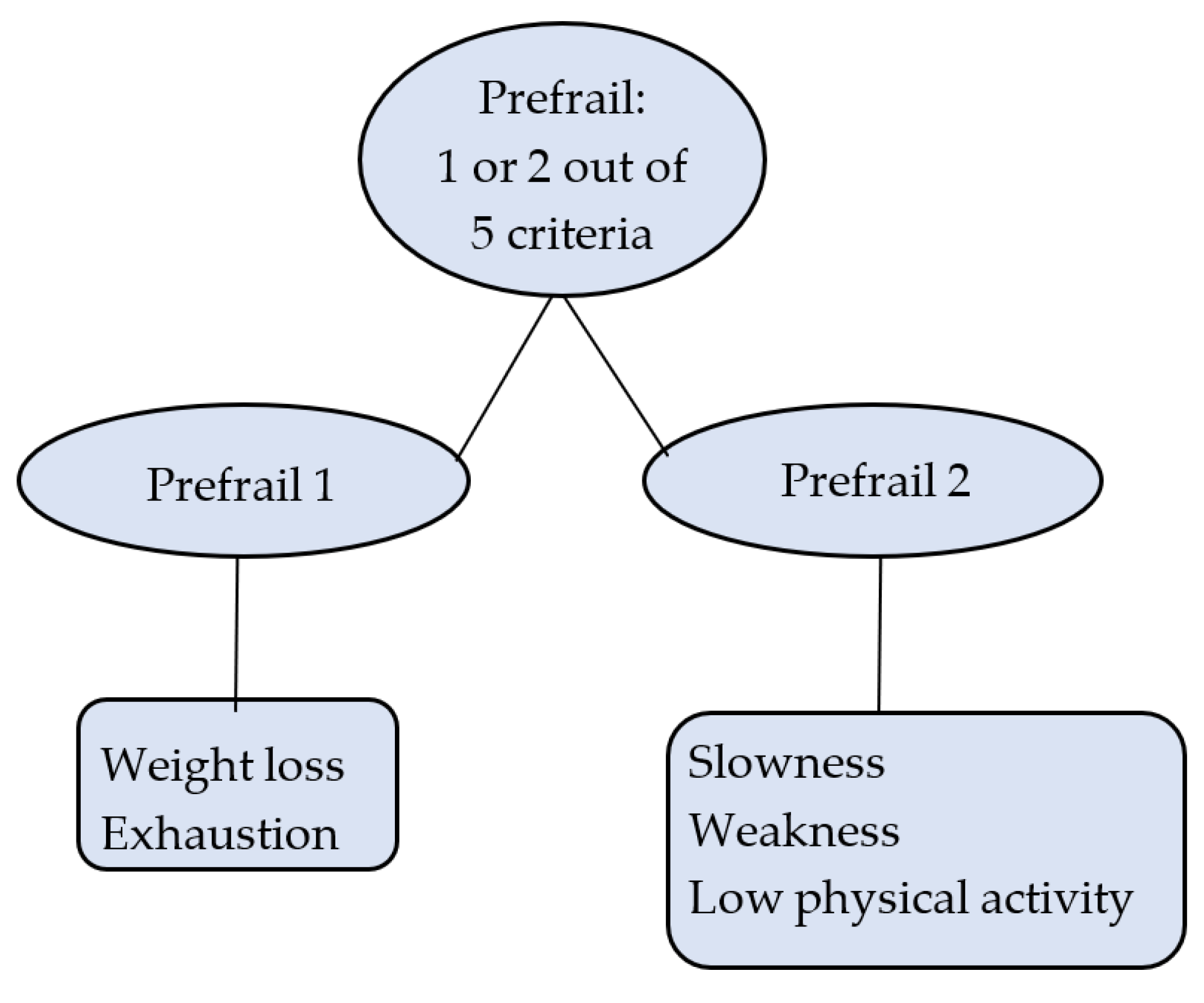
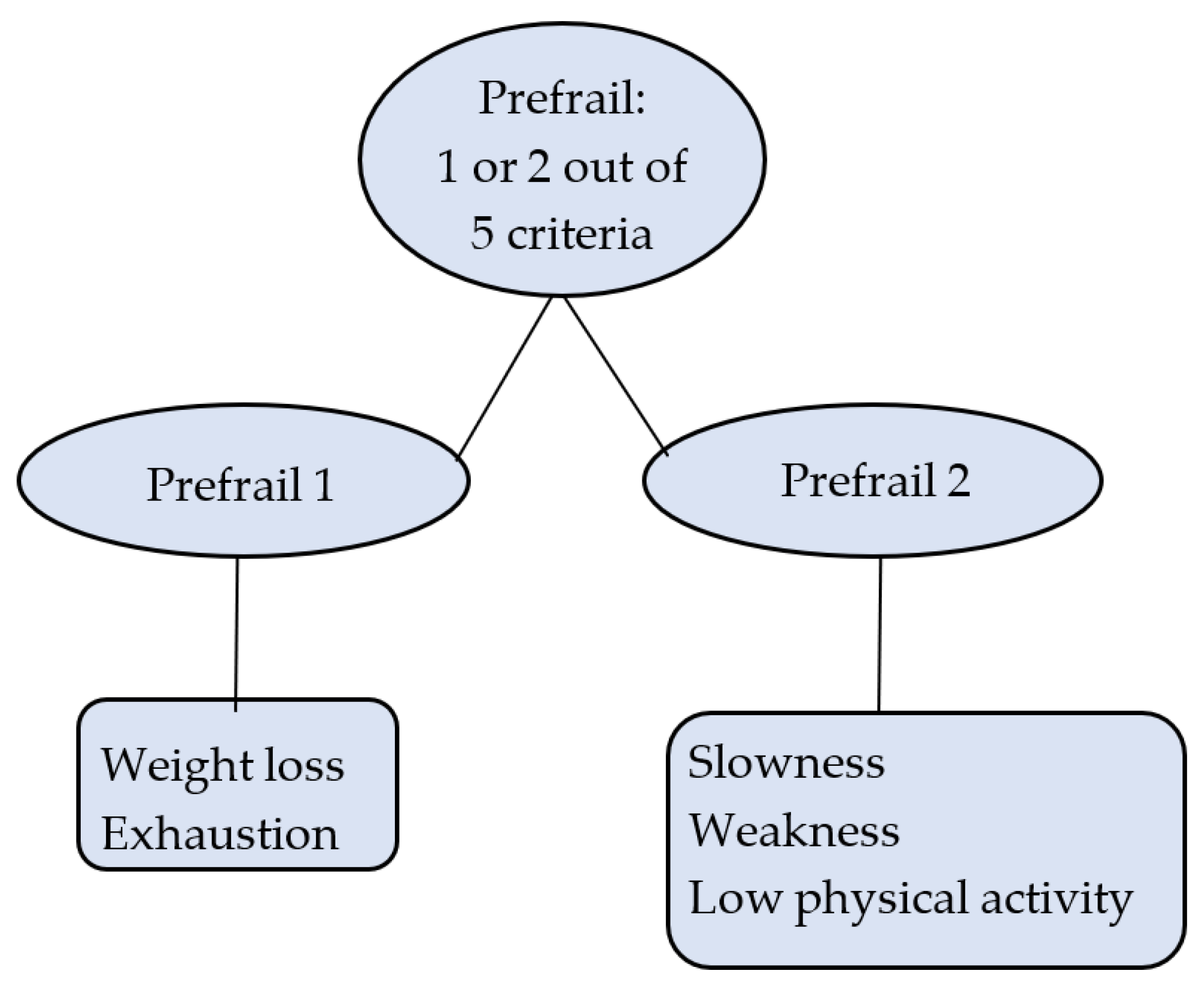
2.3. Prefrailty Operationalisation
2.4. Biomarkers and Other Measures
2.5. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walston, J.; Buta, B.; Xue, Q.-L. Frailty screening and interventions: Considerations for clinical practice. Clin. Geriatr. Med. 2018, 34, 25–38. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef] [Green Version]
- Sarkisian, C.A.; Gruenewald, T.L.; Boscardin, W.J.; Seeman, T.E. Preliminary evidence for subdimensions of geriatric frailty: The MacArthur study of successful aging. J. Am. Geriatr. Soc. 2008, 56, 2292–2297. [Google Scholar] [CrossRef]
- Sezgin, D.; Liew, A.; O’Donovan, M.R.; O’Caoimh, R. Pre-frailty as a multi-dimensional construct: A systematic review of definitions in the scientific literature. Geriatr. Nurs. 2020, 41, 139–146. [Google Scholar] [CrossRef]
- Romero-Ortuno, R.; Scarlett, S.; O’Halloran, A.M.; Kenny, R.A. Is phenotypical prefrailty all the same? A longitudinal investigation of two prefrailty subtypes in TILDA. Age Ageing 2019, 49, 39–45. [Google Scholar] [CrossRef]
- Luan, Y.Y.; Yao, Y.M. The Clinical Significance and Potential Role of C-Reactive Protein in Chronic Inflammatory and Neurodegenerative Diseases. Front. Immunol. 2018, 9, 1302. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.L.; Chang, I.C.; Liou, H.H.; Wang, C.H.; Lai, Y.H.; Kuo, C.H.; Hsu, B.G. Serum indices based on creatinine and cystatin C predict mortality in patients with non-dialysis chronic kidney disease. Sci. Rep. 2021, 11, 16863. [Google Scholar] [CrossRef]
- Upadhyay, R.K. Emerging risk biomarkers in cardiovascular diseases and disorders. J. Lipids 2015, 2015, 971453. [Google Scholar] [CrossRef]
- Moghissi, E. Management of type 2 diabetes mellitus in older patients: Current and emerging treatment options. Diabetes Ther. 2013, 4, 239–256. [Google Scholar] [CrossRef]
- Wu, J.; Cho, E.; Willett, W.C.; Sastry, S.M.; Schaumberg, D.A. Intakes of Lutein, Zeaxanthin, and other Carotenoids and Age-Related Macular Degeneration during 2 Decades of Prospective Follow-Up. JAMA Ophthalmol. 2015, 133, 1415–1424. [Google Scholar] [CrossRef]
- Feeney, J.; O’Leary, N.; Moran, R.; O’Halloran, A.M.; Nolan, J.M.; Beatty, S.; Young, I.S.; Kenny, R.A. Plasma Lutein and Zeaxanthin Are Associated with Better Cognitive Function Across Multiple Domains in a Large Population-Based Sample of Older Adults: Findings from The Irish Longitudinal Study on Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1431–1436. [Google Scholar] [CrossRef] [Green Version]
- Kearney, P.M.; Cronin, H.; O’Regan, C.; Kamiya, Y.; Savva, G.M.; Whelan, B.; Kenny, R.A. Cohort profile: The Irish Longitudinal Study on Ageing. Int. J. Epidemiol. 2011, 40, 877–884. [Google Scholar] [CrossRef]
- Chung, R.W.S.; Leanderson, P.; Lundberg, A.K.; Jonasson, L. Lutein exerts anti-inflammatory effects in patients with coronary artery disease. Atherosclerosis 2017, 262, 87–93. [Google Scholar] [CrossRef] [Green Version]
- van Herpen-Broekmans, W.M.; Klopping-ketelaars, I.; Michiel, B.; Cornelis, K.; Hans, P.; Hendriks, F.J.; Tijburg, L.; van Poppel, G.; Kaardinal, A. Serum carotenoids and vitamins in relation to markers of endothelial function and inflammation. Eur. J. Epidemiol. 2004, 19, 915–921. [Google Scholar] [CrossRef]
- Moran, R.; Nolan, J.M.; Stack, J.; O’Halloran, A.M.; Feeney, J.; Akuffo, K.O.; Kenny, R.A.; Beatty, S. Non-Dietary Correlates and Determinants of Plasma Lutein and Zeaxanthin Concentrations in the Irish Population. J. Nutr. Health Aging 2017, 21, 254–261. [Google Scholar] [CrossRef]
- Canney, M.; O’Connell, M.D.L.; Sexton, D.J.; O’Leary, N.; Kenny, R.A.; Little, M.A.; O’Seaghdha, C.M. Graded Association Between Kidney Function and Impaired Orthostatic Blood Pressure Stabilization in Older Adults. J. Am. Heart Assoc. 2017, 6, e005661. [Google Scholar] [CrossRef]
- Rao, M.; Jaber, B.L.; Balakrishnan, V.S. Chronic kidney disease and acquired mitochondrial myopathy. Curr. Opin. Nephrol. Hypertens. 2018, 27, 113–120. [Google Scholar] [CrossRef]
- Ferrara, A.; Barrett-Connor, E.; Shan, J. Total, LDL, and HDL cholesterol decrease with age in older men and women. The Rancho Bernardo Study 1984–1994. Circulation 1997, 96, 37–43. [Google Scholar] [CrossRef]
- Cabrera, M.A.S.; de Andrade, S.M.; Dip, R.M. Lipids and All-Cause Mortality among Older Adults: A 12-Year Follow-Up Study. Sci. World J. 2012, 2012, 930139. [Google Scholar] [CrossRef] [Green Version]
- Klancic, T.; Woodward, L.; Hofmann, S.M.; Fisher, E.A. High density lipoprotein and metabolic disease: Potential benefits of restoring its functional properties. Mol. Metab. 2016, 5, 321–327. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Fried Criteria | Cut-Offs | Scoring |
|---|---|---|
| Weight Loss | “In the past year, have you lost 10 pounds or more?” | Yes = 1 |
| Slowness | Male: Height ≤ 173 cm: gait speed < 109.7 cm/s Height > 173 cm: gait speed < 116.7 cm/s Female: Height ≤ 159 cm: gait speed < 100.7 cm/s Height > 159 cm: gait speed < 108.4 cm/s | Yes = 1 |
| Weakness | Male: BMI < 24: grip strength ≤ 20.5 kg BMI 24–26: grip strength < 21.5 kg BMI > 26: grip strength < 23 kg Female: BMI ≤ 23: grip strength < 11.5 kg BMI > 23: grip strength < 13 kg | Yes = 1 |
| Physical Activity | Male (low on IPAQ-SF per 20th percentile): IPAQ-SF score < 462 Female (low on IPAQ-SF per 20th percentile): IPAQ-SF score < 99 | Yes = 1 |
| Exhaustion | “I could not get going” or “Everything I did was an effort” | Yes = 1 |
| Total N = 5307 | Robust † N = 3663 | PF1 N = 469 | PF2 N = 1004 | Frail N = 171 | PF1 vs. PF2 (Absolute Difference) | |
|---|---|---|---|---|---|---|
| Age, median (IQR) years | 61.0 (14.0) | 60.0 (12.0) | 60.0 (12.0) | 68.0 (17.0) c | 73. (18.0) c | 8.0 c |
| Female sex % | 53.4 | 53.4 | 63.8 | 48.9 c | 52.2 b | 14.9 c |
| Education % | ||||||
| Primary | 25.1 | 21.3 | 25.8 | 34.8 | 46.8 | 9.0 |
| Secondary | 41.2 | 42.0 | 38.6 | 40.4 | 36.2 | 1.8 |
| Third level | 33.7 | 36.7 | 35.6 | 24.8 | 17.0 | 10.8 c |
| BMI, median (IQR) kg/m2 | 28.1 (6.00) | 27.9 (5.7) | 27.9 (6.7) | 28.9 (6.4) c | 28.3 (8.3) | 1.0 c |
| Statin use % | 30.2 | 27.0 | 32.6 | 38.3 | 43.3 | 5.7 a |
| CRP, median (IQR) mg/L | 1.67 (2.36) | 1.57 (2.09) | 1.66 (2.52) | 2.00 (3.02) c | 3.06 (6.36) c | 0.34 b |
| Lutein, median (IQR) µmol/L | 0.181 (0.123) | 0.186 (0.124) | 0.164 (0.123) c | 0.172 (0.125) c | 0.130 (0.85) b | 0.008 |
| Zeaxanthin, median (IQR) µmol/L | 0.045 (0.040) | 0.047 (0.041) | 0.040 (0.039) b | 0.040 (0.038) c | 0.031 (0.023) a | 0.00 |
| Creatinine, median (IQR) µmol/L | 77.0 (23.0) | 77.0 (22.0) | 74.0 (24.0) a | 80.0 (24.0) c | 84.0 (40.0) c | 6.0 c |
| Cystatin C, median (IQR) mg/L | 0.94 (0.21) | 0.93 (0.19) | 0.93 (0.20) | 1.02 (0.29) c | 1.16 (0.50) c | 0.09 c |
| HbA1c, median (IQR) mmol/L | 32.0 (5.0) | 32.0 (5.0) | 32.0 (5.0) | 33.0 (6.0) c | 34.0 (6.0) c | 1.0 c |
| Total Cholesterol, median (IQR) mmol/L | 5.1 (1.4) | 5.2 (1.5) | 5.2 (1.4) | 4.90 (1.4) c | 4.6 (1.6) c | 0.3 c |
| HDL, median (IQR) mmol/L | 1.48 (0.57) | 1.50 (0.57) | 1.47 (0.58) | 1.41 (0.55) c | 1.34 (0.46) c | 0.06 b |
| LDL, median (IQR) mmol/L | 2.90 (1.21) | 2.92 (1.26) | 2.90 (1.40) | 2.63 (1.32) c | 2.50 (1.30) c | 0.27 c |
| Triglycerides, median (IQR) mmol/L | 1.47 (1.11) | 1.45 (1.11) | 1.53 (1.09) | 1.53 (1.14) a | 1.49 (0.99) | 0.00 |
| Slowness, median (IQR) TUG time, s | 8.4 (2.2) | 8.2 (1.8) | 8.3 (1.9) a | 9.9 (4.1) c | 14.3 (6.4) c | 1.6 c |
| Weakness, median (IQR) grip strength, kg | 24.5 (14.0) | 26.5 (14.0) | 23.0 (11.5) c | 20.5 (15.5) c | 16.0 (11.0) c | 2.5 c |
| Physical activity, median (IQR) IPAQ-SF met minutes | 1935 (3573) | 2586 (3863) | 1986 (3366) c | 396 (1666) c | 0 (198) c | 1590 c |
| Weight loss % | 5.6 | 0.0 | 46.5 | 0.00 | 45.6 | 46.5 c |
| Exhaustion % | 7.3 | 0.0 | 61.2 | 0.00 | 58.5 | 61.2 c |
| PF1 vs. ROBUST | PF2 vs. Robust | PF2 vs. PF1 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | |
| CRP | 1.13 | 1.02–1.25 | 0.015 | 1.19 | 1.10–1.28 | <0.001 † | 1.04 | 0.93–1.17 | 0.471 |
| Lutein | 0.77 | 0.69–0.86 | <0.001 † | 0.89 | 0.81–0.96 | 0.005 | 1.13 | 0.99–1.28 | 0.065 |
| Zeaxanthin | 0.81 | 0.73–0.91 | <0.001 † | 0.89 | 0.82–0.97 | 0.010 | 1.07 | 0.94–1.22 | 0.298 |
| Creatine | 1.07 | 0.94–1.22 | 0.280 | 1.06 | 0.97–1.16 | 0.174 | 0.99 | 0.87–1.14 | 0.937 |
| Cystatin C | 1.23 | 1.08–1.39 | 0.001 † | 1.36 | 1.25–1.49 | <0.001 † | 1.10 | 0.96–1.27 | 0.176 |
| Hb1AC | 1.09 | 0.99–1.21 | 0.095 | 1.18 | 1.09–1.27 | <0.001 † | 1.07 | 0.95–1.19 | 0.272 |
| Cholesterol | 0.86 | 0.78–0.96 | 0.007 | 0.89 | 0.82–0.96 | 0.004 † | 1.03 | 0.92–1.17 | 0.581 |
| HDL | 0.86 | 0.77–0.96 | 0.006 | 0.87 | 0.80–0.94 | <0.001 † | 0.99 | 0.87–1.13 | 0.915 |
| LDL | 0.90 | 0.81–0.99 | 0.042 | 0.91 | 0.85–0.98 | 0.015 | 1.02 | 0.90–0.15 | 0.774 |
| Triglycerides | 1.08 | 0.98–1.19 | 0.104 | 1.12 | 1.03–1.20 | 0.005 | 1.06 | 0.94–1.19 | 0.371 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piankova, P.; Romero-Ortuno, R.; O’Halloran, A.M. Biomarker Signatures of Two Phenotypical Prefrailty Types in the Irish Longitudinal Study on Ageing. Geriatrics 2022, 7, 25. https://doi.org/10.3390/geriatrics7020025
Piankova P, Romero-Ortuno R, O’Halloran AM. Biomarker Signatures of Two Phenotypical Prefrailty Types in the Irish Longitudinal Study on Ageing. Geriatrics. 2022; 7(2):25. https://doi.org/10.3390/geriatrics7020025
Chicago/Turabian StylePiankova, Palina, Roman Romero-Ortuno, and Aisling M. O’Halloran. 2022. "Biomarker Signatures of Two Phenotypical Prefrailty Types in the Irish Longitudinal Study on Ageing" Geriatrics 7, no. 2: 25. https://doi.org/10.3390/geriatrics7020025
APA StylePiankova, P., Romero-Ortuno, R., & O’Halloran, A. M. (2022). Biomarker Signatures of Two Phenotypical Prefrailty Types in the Irish Longitudinal Study on Ageing. Geriatrics, 7(2), 25. https://doi.org/10.3390/geriatrics7020025