
Intra- and Intermuscular Coherence and Body Acceleration Control in Older Adults during Bipedal Stance


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurement
2.3. Data Processing
2.4. Coherence Analysis
2.5. Cross-Correlation Function Analysis for COP
2.6. Correlation Analysis for the Coherence Value and COMacc
2.7. Statistical Analysis
3. Results
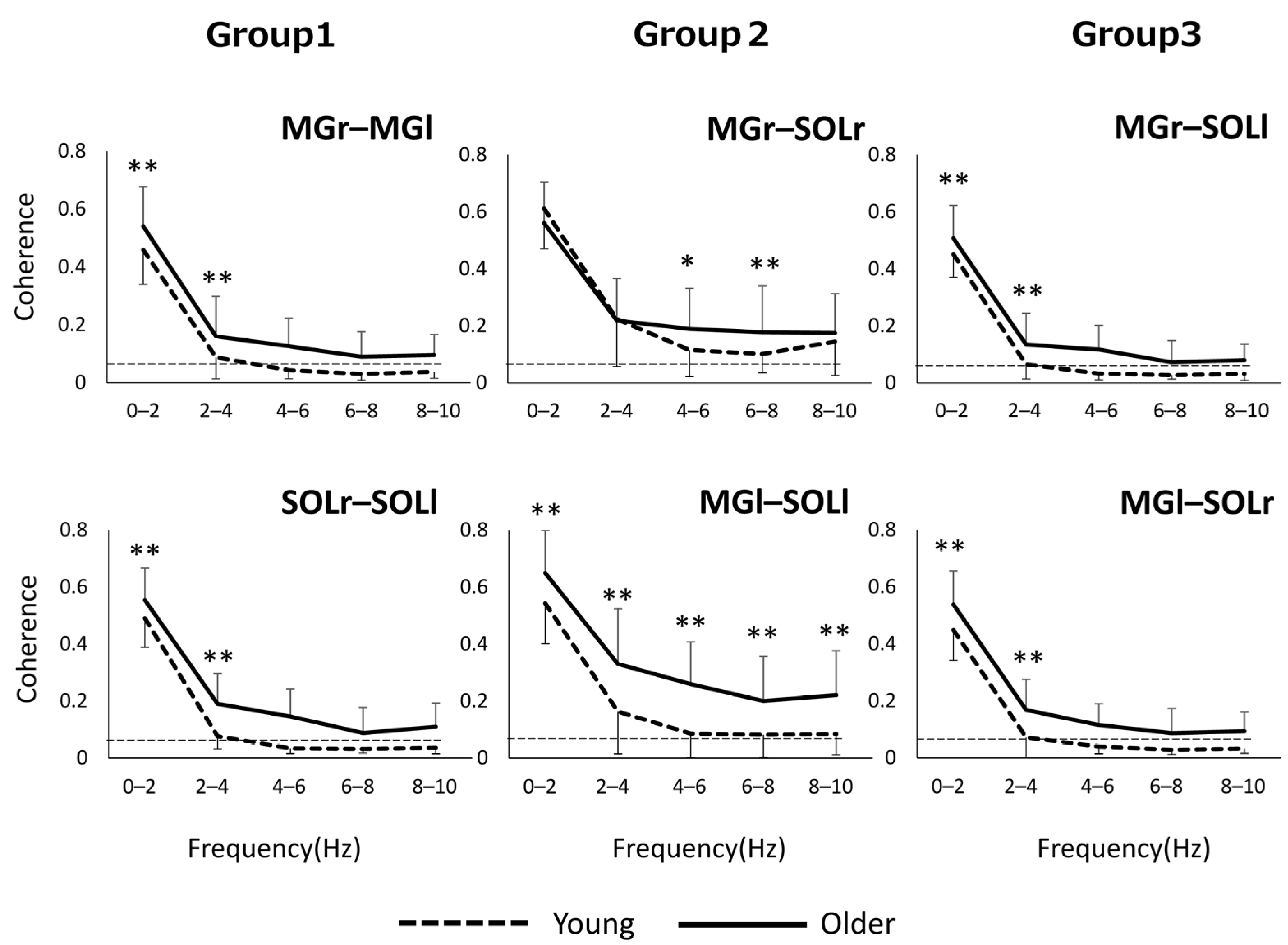
3.1. Coherence Analysis
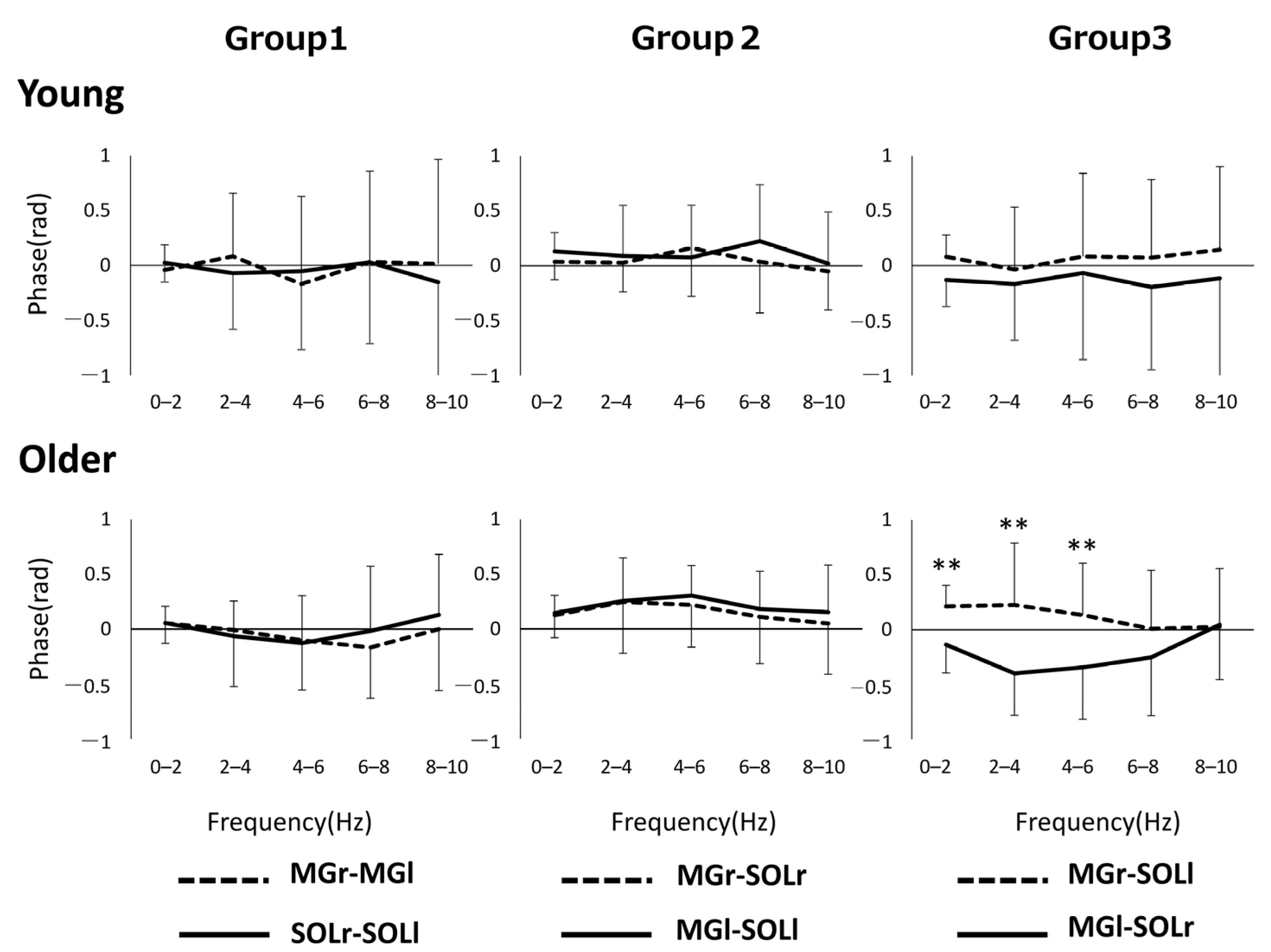
3.2. Phase Analysis
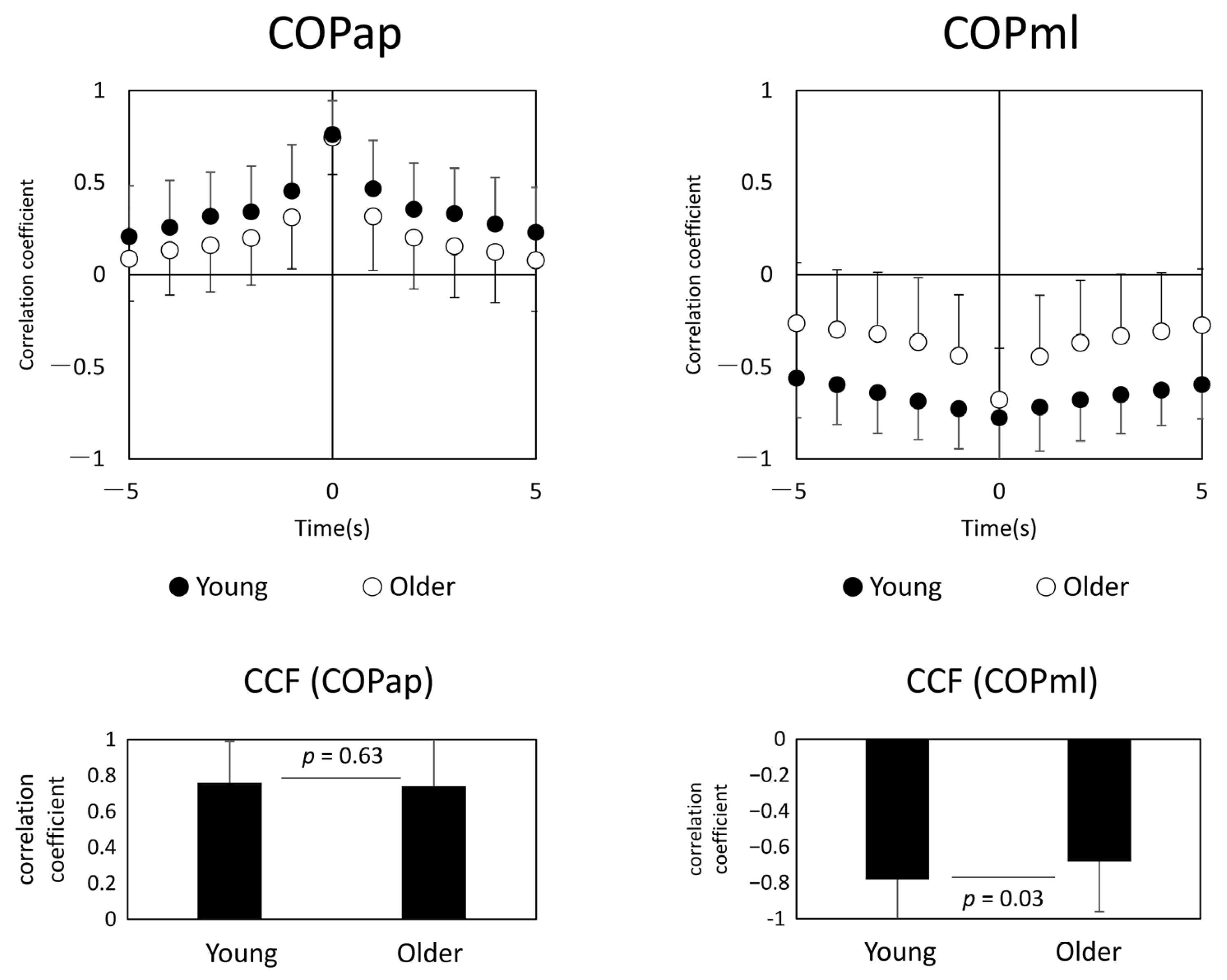
3.3. Synchronization of COP Motion between Both Feet
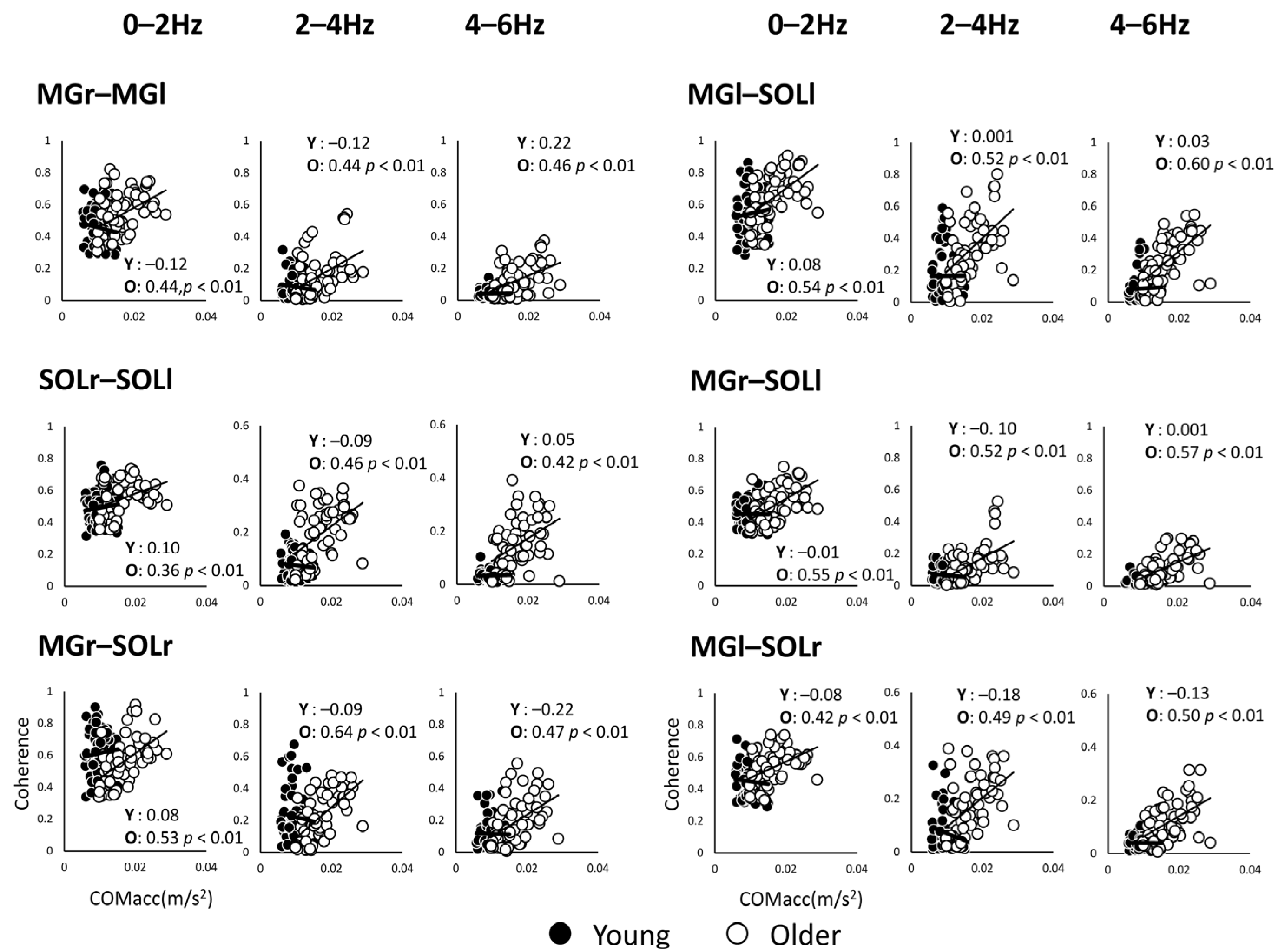
3.4. Correlation Analysis for the Coherence Value and COMacc
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paillard, T.; Noé, F. Techniques and Methods for Testing the Postural Function in Healthy and Pathological Subjects. BioMed Res. Int. 2015, 2015, 891390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duarte, M.; Freitas, S.M.S.F. Revision of posturography based on force plate for balance evaluation. Rev. Bras. Fisioter. 2010, 14, 183–192. [Google Scholar] [CrossRef] [Green Version]
- Tanabe, H.; Fujii, K.; Kouzaki, M. Intermittent muscle activity in the feedback loop of postural control system during natural quiet standing. Sci. Rep. 2017, 7, 10631. [Google Scholar] [CrossRef] [Green Version]
- Lai, H.C.; Seal, R.P.; Johnson, J.E. Making sense out of spinal cord somatosensory development. Development 2016, 143, 3434–3448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boonstra, T.W.; Danna-Dos-Santos, A.; Xie, H.-B.; Roerdink, M.; Stins, J.; Breakspear, M. Muscle networks: Connectivity analysis of EMG activity during postural control. Sci. Rep. 2015, 5, 17830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danna-Dos-Santos, A.; Boonstra, T.W.; Degani, A.M.; Cardoso, V.S.; Magalhaes, A.T.; Mochizuki, L.; Leonard, C.T. Multi-muscle control during bipedal stance: An EMG–EMG analysis approach. Exp. Brain Res. 2014, 232, 75–87. [Google Scholar] [CrossRef]
- Zehr, E.; Barss, T.; Dragert, K.; Frigon, A.; Vasudevan, E.; Haridas, C.; Hundza, S.; Kaupp, C.; Klarner, T.; Klimstra, M.; et al. Neuromechanical interactions between the limbs during human locomotion: An evolutionary perspective with translation to rehabilitation. Exp. Brain Res. 2016, 234, 3059–3081. [Google Scholar] [CrossRef] [Green Version]
- Akay, T.; Tourtellotte, W.G.; Arber, S.; Jessell, T.M. Degradation of mouse locomotor pattern in the absence of proprioceptive sensory feedback. Proc. Natl. Acad. Sci. USA 2014, 111, 16877–16882. [Google Scholar] [CrossRef] [Green Version]
- Héroux, M.E.; Dakin, C.J.; Luu, B.L.; Inglis, J.T.; Blouin, J.-S. Absence of lateral gastrocnemius activity and differential motor unit behavior in soleus and medial gastrocnemius during standing balance. J. Appl. Physiol. 2014, 116, 140–148. [Google Scholar] [CrossRef] [Green Version]
- Latash, M.L. Muscle coactivation: Definitions, mechanisms, and functions. J. Neurophysiol. 2018, 120, 88–104. [Google Scholar] [CrossRef]
- Masani, K.; Vette, A.H.; Kouzaki, M.; Kanehisa, H.; Fukunaga, T.; Popovic, M.R. Larger center of pressure minus center of gravity in the elderly induces larger body acceleration during quiet standing. Neurosci. Lett. 2007, 422, 202–206. [Google Scholar] [CrossRef]
- Yu, E.; Abe, M.; Masani, K.; Kawashima, N.; Eto, F.; Haga, N.; Nakazawa, K. Evaluation of Postural Control in Quiet Standing Using Center of Mass Acceleration: Comparison Among the Young, the Elderly, and People With Stroke. Arch. Phys. Med. Rehabil. 2008, 89, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Oba, N.; Sasagawa, S.; Yamamoto, A.; Nakazawa, K. Difference in Postural Control during Quiet Standing between Young Children and Adults: Assessment with Center of Mass Acceleration. PLoS ONE 2015, 10, e0140235. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, T.; Saito, K.; Ishida, K.; Tanabe, S.; Nojima, I. Coordination of plantar flexor muscles during bipedal and unipedal stances in young and elderly adults. Exp. Brain Res. 2018, 236, 1229–1239. [Google Scholar] [CrossRef]
- Minamisawa, T.; Chiba, N.; Inoue, K.; Nakanowatari, T.; Suzuki, E. Analysis of vertical microacceleration during standing shows age-related changes. Geriatrics 2020, 5, 105. [Google Scholar] [CrossRef] [PubMed]
- Mima, T.; Hallett, M. Electroencephalographic analysis of cortico-muscular coherence: Reference effect, volume conduction and generator mechanism. Clin. Neurophysiol. 1999, 110, 1892–1899. [Google Scholar] [CrossRef]
- Rosenberg, J.; Amjad, A.; Breeze, P.; Brillinger, D.; Halliday, D. The Fourier approach to the identification of functional coupling between neuronal spike trains. Prog. Biophys. Mol. Biol. 1989, 53, 1–31. [Google Scholar] [CrossRef]
- Degani, A.M.; Leonard, C.T.; Danna-Dos-Santos, A. The effects of aging on the distribution and strength of correlated neural inputs to postural muscles during unperturbed bipedal stance. Exp. Brain Res. 2020, 238, 1537–1553. [Google Scholar] [CrossRef]
- Gervasio, S.; Kersting, U.G.; Farina, D.; Mrachacz-Kersting, N. The effect of crossed reflex responses on dynamic stability during locomotion. J. Neurophysiol. 2015, 114, 1034–1040. [Google Scholar] [CrossRef] [Green Version]
- Baudry, S.; Duchateau, J. Age-related influence of vision and proprioception on Ia presynaptic inhibition in soleus muscle during upright stance. J. Physiol. 2012, 590, 5541–5554. [Google Scholar] [CrossRef]
- Henry, M.; Baudry, S. Age-related changes in leg proprioception: Implications for postural control. J. Neurophysiol. 2019, 122, 525–538. [Google Scholar] [CrossRef] [Green Version]
- Blaszczyk, J.W.; Prince, F.; Raiche, M.; Hébert, R. Effect of ageing and vision on limb load asymmetry during quiet stance. J. Biomech. 2000, 33, 1243–1248. [Google Scholar] [CrossRef]
- Thelen, D.G.; Wojcik, L.A.; Schultz, A.B.; Ashton-Miller, J.A.; Alexander, N.B. Age Differences in Using a Rapid Step To Regain Balance During a Forward Fall. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 1997, 52, M8–M13. [Google Scholar] [CrossRef]
- Vieira, T.M.; Minetto, M.A.; Hodson-Tole, E.; Botter, A. How much does the human medial gastrocnemius muscle contribute to ankle torques outside the sagittal plane? Hum. Mov. Sci. 2013, 32, 753–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melzer, I.; Kurz, I.; Oddsson, L.I. A retrospective analysis of balance control parameters in elderly fallers and non-fallers. Clin. Biomech. 2010, 25, 984–988. [Google Scholar] [CrossRef] [PubMed]
- Piirtola, M.; Era, P. Force Platform Measurements as Predictors of Falls among Older People—A Review. Gerontology 2006, 52, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Stel, V.S.; Smit, J.H.; Pluijm, S.M.; Lips, P. Balance and mobility performance as treatable risk factors for recurrent falling in older persons. J. Clin. Epidemiol. 2003, 56, 659–668. [Google Scholar] [CrossRef]
- Winter, D.A.; Prince, F.; Frank, J.S.; Powell, C.; Zabjek, K.F. Unified theory regarding A/P and M/L balance in quiet stance. J. Neurophysiol. 1996, 75, 2334–2343. [Google Scholar] [CrossRef]
- Genthon, N.; Rougier, P. Analyse biomécanique de la contribution relative de chacun des appuis dans le contrôle de la station debout non-perturbée. ITBM-RBM 2003, 24, 238–247. [Google Scholar] [CrossRef]
- Dietz, V.; Horstmann, G.A.; Berger, W. Interlimb coordination of leg-muscle activation during perturbation of stance in humans. J. Neurophysiol. 1989, 62, 680–693. [Google Scholar] [CrossRef]
- Lee, P.J.; Rogers, E.L.; Granata, K.P. Active trunk stiffness increases with co-contraction. J. Electromyogr. Kinesiol. 2006, 16, 51–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minamisawa, T.; Chiba, N.; Suzuki, E. Intra- and Intermuscular Coherence and Body Acceleration Control in Older Adults during Bipedal Stance. Geriatrics 2021, 6, 114. https://doi.org/10.3390/geriatrics6040114
Minamisawa T, Chiba N, Suzuki E. Intra- and Intermuscular Coherence and Body Acceleration Control in Older Adults during Bipedal Stance. Geriatrics. 2021; 6(4):114. https://doi.org/10.3390/geriatrics6040114
Chicago/Turabian StyleMinamisawa, Tadayoshi, Noboru Chiba, and Eizaburo Suzuki. 2021. "Intra- and Intermuscular Coherence and Body Acceleration Control in Older Adults during Bipedal Stance" Geriatrics 6, no. 4: 114. https://doi.org/10.3390/geriatrics6040114
APA StyleMinamisawa, T., Chiba, N., & Suzuki, E. (2021). Intra- and Intermuscular Coherence and Body Acceleration Control in Older Adults during Bipedal Stance. Geriatrics, 6(4), 114. https://doi.org/10.3390/geriatrics6040114