Surgical Treatment of Femoral Neck Fractures: A Brief Review


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
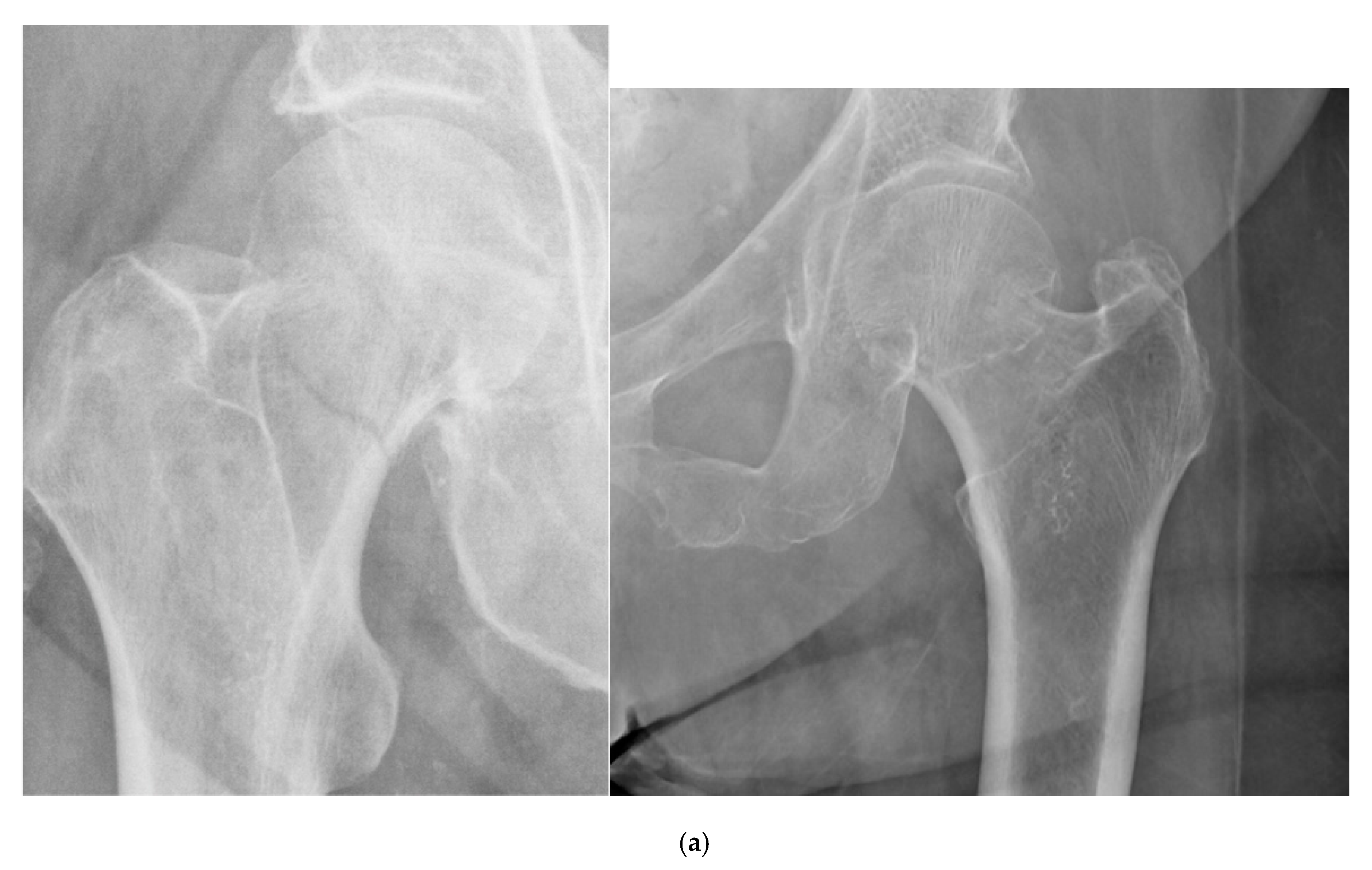
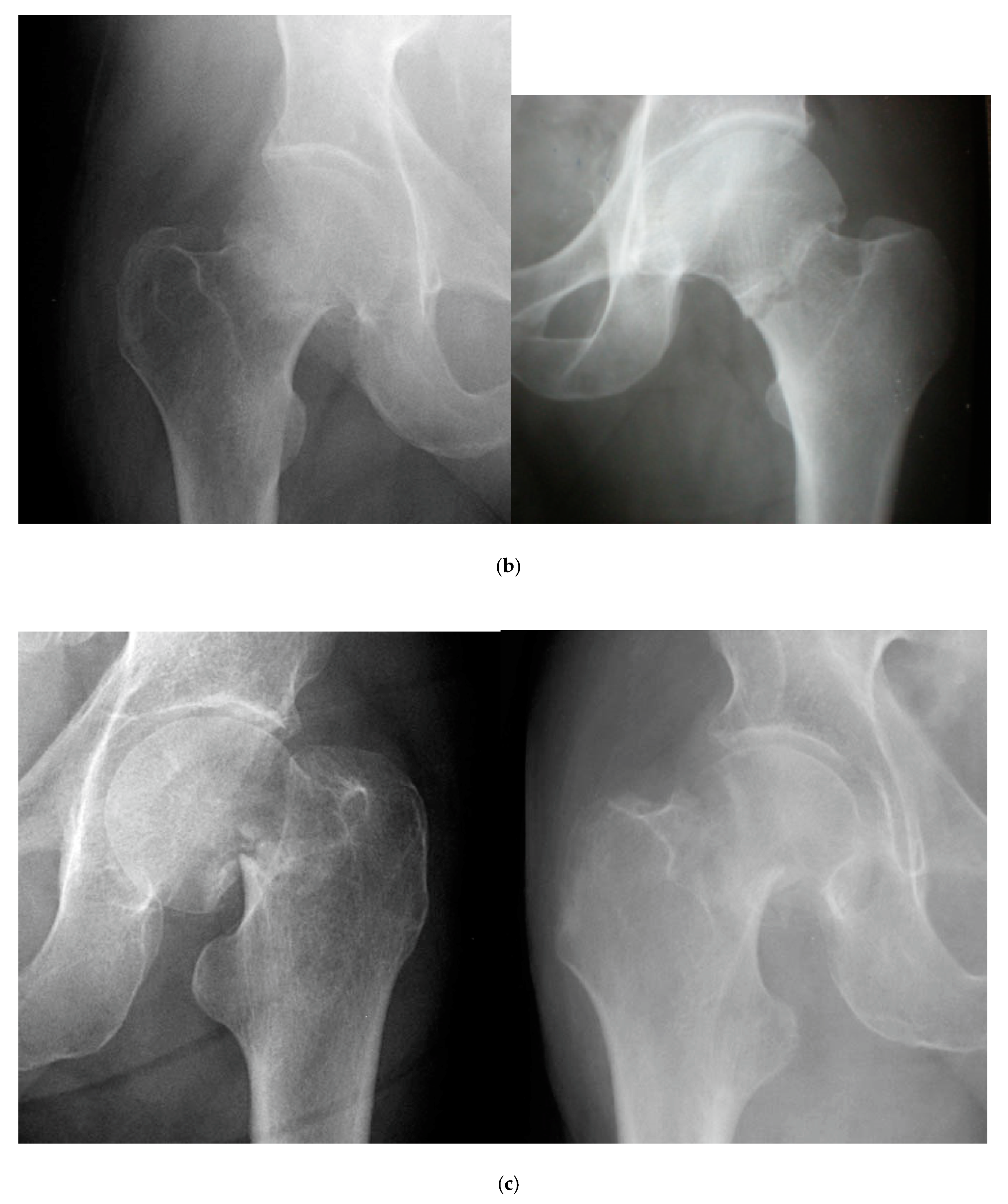
2.1. Classification of Femoral Neck Fractures
- Stage I: incomplete fracture; nondisplaced, valgus impacted
- Stage II: complete fracture; nondisplaced
- Stage III: complete fracture; partially displaced
- Stage IV: complete fracture; fully displaced
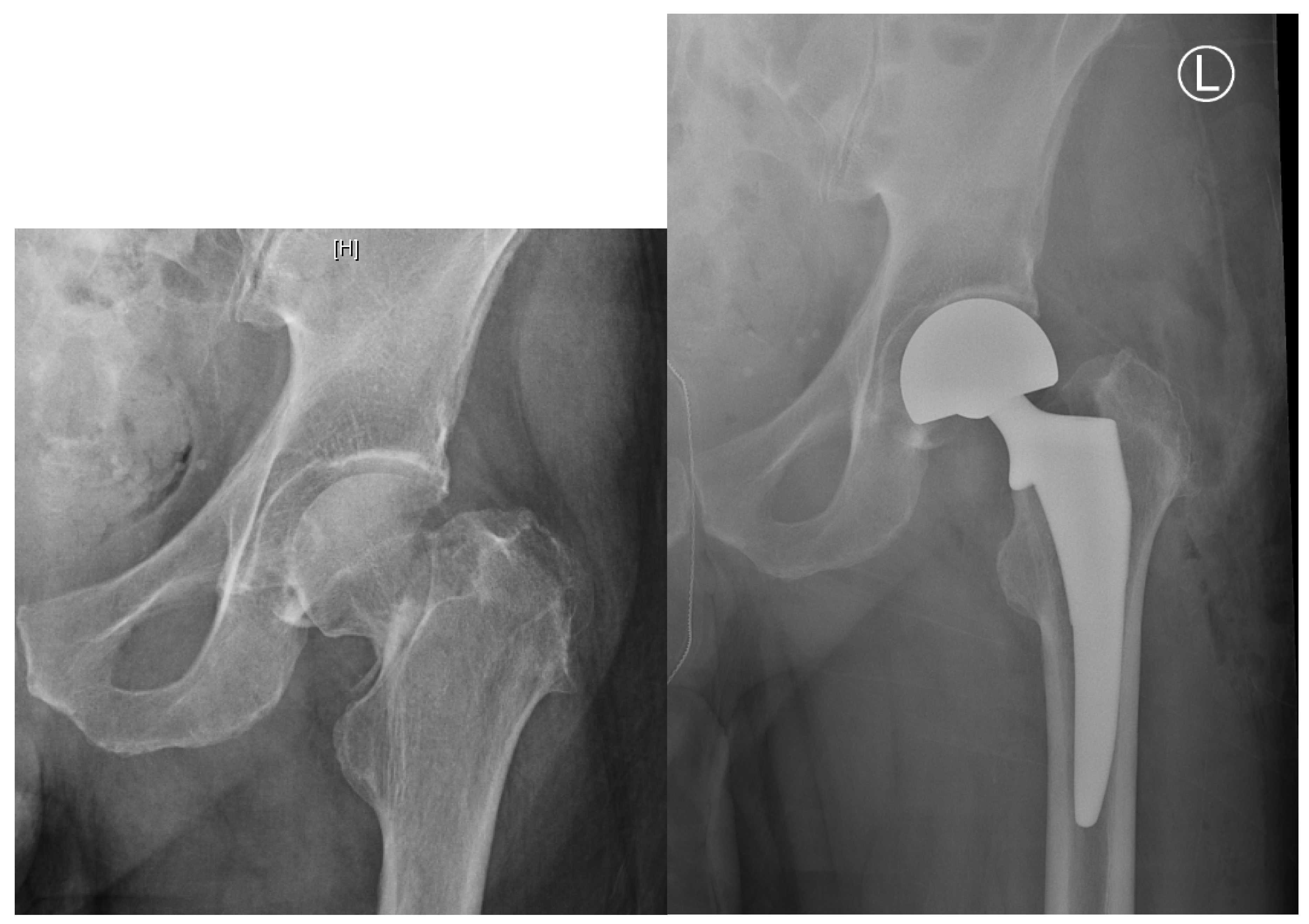
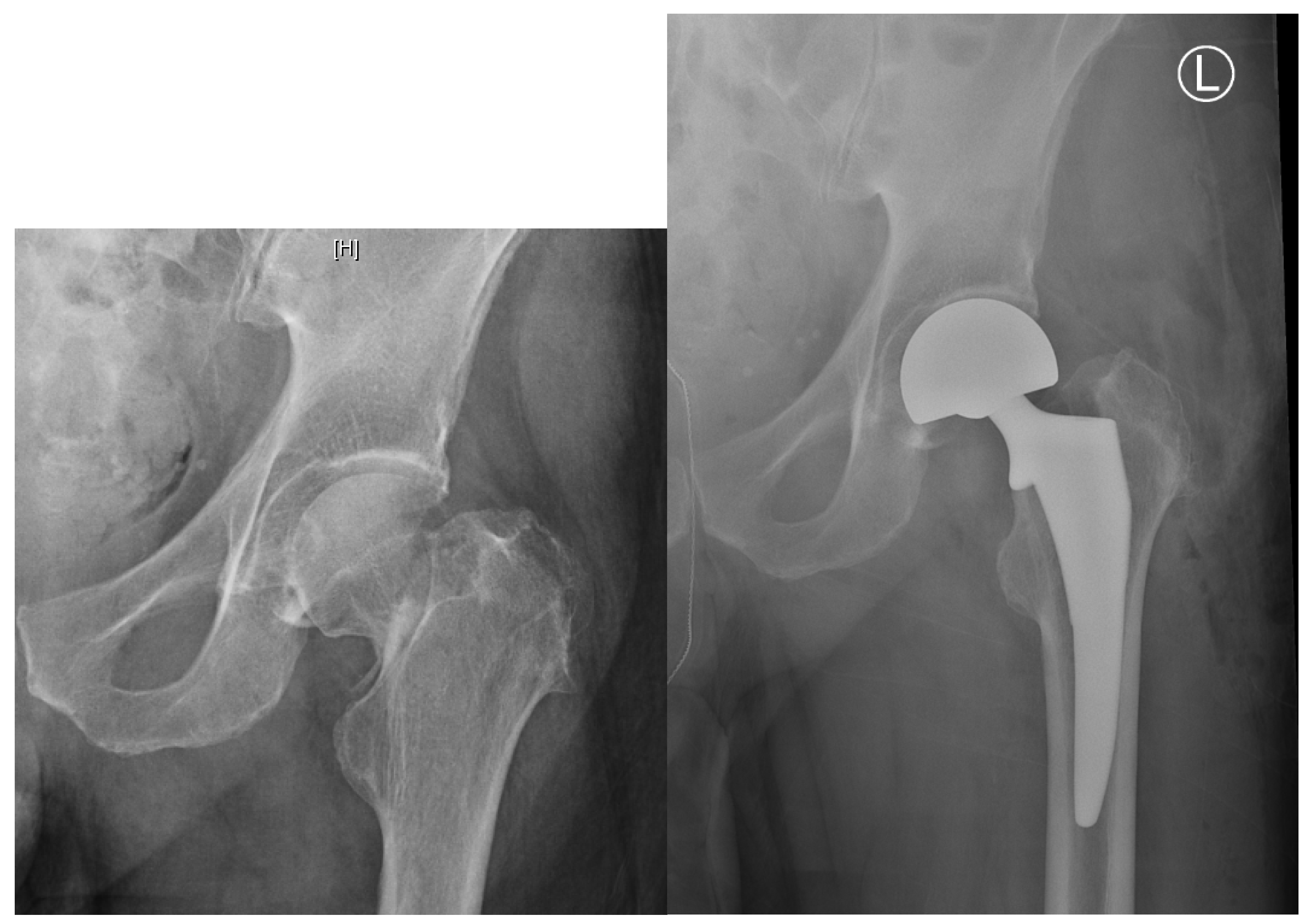
2.2. Nondisplaced Femoral Neck Fractures: Internal Fixation vs. Arthroplasty
2.3. Displaced Femoral Neck Fractures: Internal Fixation vs. Arthroplasty
2.4. Displaced Femoral Neck Fractures: Hemiarthroplasty vs. Total Hip Arthroplasty
2.5. Bone Cement Implantation Syndrome: Risks and Benefits of a Cemented vs. Uncemented Hemiarthroplasty
3. Discussion/Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ahn, J.; Man, L.X.; Park, S.; Sodl, J.F.; Esterhai, J.L. Systematic review of cemented and uncemented hemiarthroplasty outcomes for femoral neck fractures. Clin. Orthop. Relat. Res. 2008, 466, 2513–2518. [Google Scholar] [CrossRef] [Green Version]
- Brauer, C.A.; Coca-Perraillon, M.; Cutler, D.M.; Rosen, A.B. Incidence and mortality of hip fractures in the United States. JAMA 2009, 302, 1573–1579. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Bhattacharyya, T. Outcomes of hemiarthroplasty and total hip arthroplasty for femoral neck fracture: A Medicare cohort study. J. Orthop. Trauma 2017, 31, 260–263. [Google Scholar] [CrossRef] [Green Version]
- Kannus, P.; Niemi, S.; Parkkari, J.; Palvanen, M.; Vuori, I.; Jarvinen, M. Nationwide decline in incidence of hip fracture. J. Bone Miner. Res. 2006, 21, 1836–1838. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Coupland, C. Derivation and validation of updated QFracture algorithm to predict risk of osteoporotic fracture in primary care in the United Kingdom: Prospective open cohort study. BMJ 2012, 344, e3427. [Google Scholar] [CrossRef] [Green Version]
- Sambrook, P.; Cooper, C. Osteoporosis. Lancet 2006, 367, 2010–2018. [Google Scholar] [CrossRef]
- Ju, D.G.; Rajaee, S.S.; Mirocha, J.; Lin, C.A.; Moon, C.N. Nationwide analysis of femoral neck fractures in elderly patients: A receding tide. J. Bone Jt. Surg. Am. 2017, 99, 1932–1940. [Google Scholar] [CrossRef] [PubMed]
- MacKinley, K.; Falls, T.; Lau, E.; Day, J.; Kurtz, S.; Ong, K.; Malkani, A. Decreasing incidence of femoral neck fractures in the Medicare population. Orthopaedics 2014, 37, 917–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, J.A.; Rudd, R.A. The impact of decreasing US hip fracture rates on future hip fracture estimates. Osteoporos. Int. 2013, 24, 2725–2728. [Google Scholar] [CrossRef] [PubMed]
- Frandsen, P.A.; Andersen, E.; Madsen, F.; Skjodt, T. Garden’s classification of femoral neck fractures. An assessment of inter-observer variation. J. Bone Jt. Surg. Br. 1988, 70, 588–590. [Google Scholar] [CrossRef]
- Van Embden, D.; Rhemrev, S.J.; Genelin, F.; Meylaerts, S.A.; Roukema, G.R. The reliability of a simplified Garden classification for intracapsular hip fractures. Orthop. Traumatol. Surg. Res. 2012, 98, 405–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.C.; Yu, S.W.; Tseng, I.C.; Su, J.Y.; Tu, Y.K.; Chen, W.J. Treatment of undisplaced femoral neck fractures in the elderly. J. Trauma 2005, 58, 1035–1039; discussion 1039. [Google Scholar] [CrossRef] [PubMed]
- Conn, K.S.; Parker, M.J. Undisplaced intracapsular hip fractures: Results of internal fixation in 375 patients. Clin. Orthop. Relat. Res. 2004, 421, 249–254. [Google Scholar] [CrossRef]
- Gjertsen, J.E.; Fevang, J.M.; Matre, K.; Vinje, T.; Engesaeter, L.B. Clinical outcome after undisplaced femoral neck fractures. Acta Orthop. 2011, 82, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.J.; White, A.; Boyle, A. Fixation versus hemiarthroplasty for undisplaced intracapsular hip fractures. Injury 2008, 39, 791–795. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.J.; Stockton, G. Internal fixation implants for intracapsular proximal femoral fractures in adults. Cochrane Database Syst. Rev. 2001, 4, CD001467. [Google Scholar]
- Fixation using Alternative Implants for the Treatment of Hip fractures (FAITH) Investigators. Fracture fixation in the operative management of hip fractures (FAITH): An international, multicenter, randomized controlled trial. Lancet 2017, 389, 1419–1427. [Google Scholar]
- Cronin, P.K.; Freccero, D.M.; Kain, M.S.; Marcantonio, A.J.; Horwitz, D.S.; Tornetta, P., 3rd. Garden 1 and 2 femoral neck fractures collapse more than expected after closed reduction and percutaneous pinning. J. Orthop. Trauma 2019, 33, 116–119. [Google Scholar] [CrossRef]
- Slobogean, G.P.; Stockton, D.J.; Zeng, B.F.; Wang, D.; Ma, B.; Pollak, A.N. Femoral neck shortening in adult patients under the age of 55 years is associated with worse functional outcomes: Analysis of the prospective multi-center study of hip fracture outcomes in China (SHOC). Injury 2017, 48, 1837–1842. [Google Scholar] [CrossRef]
- Zlowodzki, M.; Ayeni, O.; Petrisor, B.A.; Bhandari, M. Femoral neck shortening after fracture fixation with multiple cancer cancellous screws: Incidence and effect on function. J. Trauma 2008, 64, 163–169. [Google Scholar] [CrossRef]
- Parker, M.J.; Raghavan, R.; Gurusamy, K. Incidence of fracture-healing complications after femoral neck fractures. Clin. Orthop. Relat. Res. 2007, 458, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Dolatowski, F.C.; Frihagen, F.; Bartels, S.; Opland, V.; Saltyte Benth, J.; Talsnes, O.; Hoelsbrekken, S.E.; Utvag, S.E. Screw fixation versus hemiarthroplasty for nondisplaced femoral neck fractures in elderly patients: A multicenter randomized controlled trial. J. Bone Jt. Surg. Am. 2019, 101, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.J.; Gurusamy, K. Internal fixation versus arthroplasty for intracapsular proximal femoral fractures in adults. Cochrane Database Syst. Rev. 2006, 4, CD001708. [Google Scholar] [CrossRef] [PubMed]
- Chammout, G.K.; Mukka, S.S.; Carlsson, T.; Neander, G.F.; Stark, A.W.; Skoldenberg, O.G. Total hip replacement versus open reduction and internal fixation of displaced femoral neck fractures: A randomized long-term follow-up study. J. Bone Jt. Surg. Am. 2012, 94, 1921–1928. [Google Scholar] [CrossRef]
- Johansson, T. Internal fixation compared with total hip replacement for displaced femoral neck fractures: A minimum fifteen-year follow-up study of a previously reported randomized trial. J. Bone Jt. Surg. Am. 2014, 96, e46. [Google Scholar] [CrossRef] [PubMed]
- Keating, J.F.; Grant, A.; Masson, M.; Scott, N.W.; Forbes, J.F. Randomized comparison of reduction and fixation, bipolar hemiarthroplasty, and total hip arthroplasty. Treatment of displaced intracapsular hip fractures in healthy older patients. J. Bone Jt. Surg. Am. 2006, 88, 249–260. [Google Scholar] [CrossRef]
- Leonardsson, O.; Sernbo, I.; Carlsson, A.; Akesson, K.; Rogmark, C. Long-term follow-up of replacement compared with internal fixation for displaced femoral neck fractures: Results at ten years in a randomised study of 450 patients. J. Bone Jt. Surg. Br. 2010, 92, 406–412. [Google Scholar] [CrossRef] [Green Version]
- Rogmark, C.; Carlsson, A.; Johnell, O.; Sernbo, I. A prospective randomised trial of internal fixation versus arthroplasty for displaced fractures of the neck of the femur. Functional outcome for 450 patients at two years. J. Bone Jt. Surg. Br. 2002, 84, 183–188. [Google Scholar] [CrossRef]
- McKinley, J.C.; Robinson, C.M. Treatment of displaced intracapsular hip fractures with total hip arthroplasty: Comparison of primary arthroplasty with early salvage arthroplasty after failed internal fixation. J. Bone Jt. Surg. Am. 2002, 84, 2010–2015. [Google Scholar] [CrossRef]
- Baker, R.P.; Squires, B.; Gargan, M.F.; Bannister, G.C. Total hip arthroplasty and hemiarthroplasty in mobile, independent patients with a displaced intracapsular fracture of the femoral neck. A randomized, controlled trial. J. Bone Jt. Surg. Am. 2006, 88, 2583–2589. [Google Scholar] [CrossRef]
- Chammout, G.; Kelly-Pettersson, P.; Hedbeck, C.J.; Stark, A.; Mukka, S.; Skoldenberg, O. HOPE-trial: Hemiarthroplasty compared with total hip arthroplasty for displaced femoral neck fractures in octogenarians. JBJS Open Access 2019, 4, e0059. [Google Scholar] [CrossRef] [PubMed]
- HEALTH Investigators; Bhandari, M.; Einhorn, T.A.; Guyatt, G.; Schemitsch, E.H.; Zura, R.D.; Sprague, S.; Frihagen, F.; Guerra-Farfan, E.; Kleinlugtenbelt, Y.V.; et al. Total hip arthroplasty or hemiarthroplasty for hip fracture. N. Engl. J. Med. 2019, 381, 2199–2208. [Google Scholar] [CrossRef] [Green Version]
- Hedbeck, C.J.; Enocson, A.; Lapidus, G.; Blomfeldt, R.; Tornkvist, H.; Ponzer, S.; Tidermark, J. Comparison of bipolar hemiarthroplasty with total hip arthroplasty for displaced femoral neck fractures: A concise four-year follow-up of a randomized trial. J. Bone Jt. Surg. Am. 2011, 93, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Leonardsson, O.; Rolfson, O.; Hommel, A.; Garellick, G.; Akesson, K.; Rogmark, C. Patient-reported outcome after displaced femoral neck fracture: A national survey of 4467 patients. J. Bone Jt. Surg. Am. 2013, 95, 1693–1699. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D.P.; Waever, D.; Thorninger, R.; Donnelly, W.J. Hemiarthroplasty vs total hip arthroplasty for the management of displaced neck of femur fractures: A systematic review and meta-analysis. J. Arthroplast. 2019, 34, 1837–1843. [Google Scholar] [CrossRef]
- Macaulay, W.; Nellans, K.W.; Garvin, K.L.; Iorio, R.; Healy, W.L.; Rosenwasser, M.P.; DFACTO Consortium. Prospective randomized clinical trial comparing hemiarthroplasty to total hip arthroplasty in the treatment of displaced femoral neck fractures: Winner of the Dorr Award. J. Arthroplast. 2008, 23, 2–8. [Google Scholar] [CrossRef]
- Tol, M.C.; van den Bekerom, M.P.; Sierevelt, I.N.; Hilverdink, E.F.; Raaymakers, E.L.; Goslings, J.C. Hemiarthroplasty or total hip arthroplasty for the treatment of a displaced intracapsular fracture in active elderly patients. 12-year follow-up of randomized trial. Bone Jt. J. 2017, 99, 250–254. [Google Scholar] [CrossRef]
- Stronach, B.M.; Bergin, P.F.; Perez, J.L.; Watson, S.; Jones, L.C.; McGwin, G.; Ponce, B.A. The rising use of total hip arthroplasty for femoral neck fractures in the United States. HIP Int. 2019, 30, 107–113. [Google Scholar] [CrossRef]
- van den Bekerom, M.P.; Hilverdink, E.F.; Sierevelt, I.N.; Reuling, E.M.; Schnater, J.M.; Bonke, H.; Goslings, J.C.; van Dijk, C.N.; Raaymakers, E.L. A comparison of hemiarthroplasty with total hip replacement for displaced intracapsular fracture of the femoral neck: A randomised controlled multicentre trial in patients aged 70 years and over. J. Bone Jt. Surg. Br. 2010, 92, 1422–1428. [Google Scholar] [CrossRef] [Green Version]
- Burgers, P.T.; van Geene, A.R.; van den Bekerom, M.P.; van Lieshout, E.M.; Blom, B.; Aleem, I.S.; Bhandari, M.; Poolman, R.W. Total hip arthroplasty versus hemiarthroplasty for displaced femoral neck fractures in the healthy elderly: A meta-analysis and systematic review of randomized trials. Int. Orthop. 2012, 36, 1549–1560. [Google Scholar] [CrossRef] [Green Version]
- Jobory, A.; Karrholm, J.; Overgaard, S.; Becic Pedersen, A.; Hallan, G.; Gjertsen, J.E.; Makela, K.; Rogmark, C. Reduced revision risk for dual-mobility cup in total hip replacement due to hip fracture: A matched-pair analysis of 9040 cases from the Nordic Arthroplasty Register Association (NARA). J. Bone Jt. Surg. Am. 2019, 101, 1278–1285. [Google Scholar] [CrossRef] [PubMed]
- Vielpeau, C.; Lebel, B.; Ardouin, L.; Burdin, G.; Lautridou, C. The dual mobility socket concept: Experience with 668 cases. Int. Orthop. 2011, 35, 225–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamadouche, M.; Biau, D.J.; Huten, D.; Musset, T.; Gaucher, F. The use of a cemented dual mobility socket to treat recurrent dislocation. Clin. Orthop. Relat. Res. 2010, 468, 3248–3254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.T.; Kozick, Z.; Sherman, M.; Restrepo, C.; Smith, E.B.; Courtney, P.M. Dual mobility bearing articulations result in lower rates of dislocation after revision total hip arthroplasty. J. Am. Acad. Orthop. Surg. 2019. (Published electronically). [Google Scholar] [CrossRef] [Green Version]
- Darrith, B.; Courtney, P.M.; Della Valle, C.J. Outcomes of dual mobility components in total hip arthroplasty: A systematic review of the literature. Bone Jt. J. 2018, 100, 11–19. [Google Scholar] [CrossRef]
- Reina, N.; Pareek, A.; Krych, A.J.; Pagnano, M.W.; Berry, D.J.; Abdel, M.P. Dual-mobility constructs in primary and revision total hip arthroplasty: A systematic review of comparative studies. J. Arthroplast. 2019, 34, 594–603. [Google Scholar] [CrossRef]
- Bensen, A.S.; Jakobsen, T.; Krarup, N. Dual mobility cup reduces dislocation and re-operation when used to treat displaced femoral neck fractures. Int. Orthop. 2014, 38, 1241–1245. [Google Scholar] [CrossRef] [Green Version]
- Iorio, R.; Iannotti, F.; Mazza, D.; Speranza, A.; Massafra, C.; Guzzini, M.; D’Arrigo, C.; Ferretti, A. Is dual cup mobility better than hemiarthroplasty in patients with dementia and femoral neck fracture? A randomized controlled trial. SICOT J. 2019, 5. (Published Electronically). [Google Scholar] [CrossRef]
- Ukaj, S.; Zhuri, O.; Ukaj, F.; Podvorica, V.; Grezda, K.; Caton, J.; Prudhon, J.L.; Krasnigi, S. Dual mobility acetabular cup versus hemiarthroplasty in treatment of displaced femoral neck fractures in elderly patients: Comparative study and results at minimum 3-year follow up. Geriatr. Orthop. Surg. Rehabil. 2019, 10, 2151459319848610, (Published Electronically). [Google Scholar] [CrossRef]
- Kim, Y.T.; Yoo, J.H.; Kim, M.K.; Kim, S.; Hwang, J. Dual mobility hip arthroplasty provides better outcomes compared to hemiarthroplasty for displaced femoral neck fractures: A retrospective comparative clinical study. Int. Orthop. 2018, 42, 1241–1246. [Google Scholar] [CrossRef]
- Nonne, D.; Sanna, F.; Bardelli, A.; Milano, P.; Rivera, F. Use of a dual mobility cup to prevent hip early arthroplasty dislocation in patients at high falls risk. Injury 2019, 50 (Suppl. 4), S26–S29. [Google Scholar] [CrossRef] [PubMed]
- Azegami, S.; Gurusamy, K.S.; Parker, M.J. Cemented versus uncemented hemiarthroplasty for hip fractures: A systematic review of randomised controlled trials. HIP Int. 2011, 21, 509–517. [Google Scholar] [CrossRef]
- Barenius, B.; Inngul, C.; Alagic, Z.; Enocson, A. A randomized controlled trial of cemented versus cementless arthroplasty in patients with a displaced femoral neck fracture: A four-year follow-up. Bone Jt. J. 2018, 100, 1087–1093. [Google Scholar] [CrossRef] [PubMed]
- Emery, R.J.; Broughton, N.S.; Desai, K.; Bulstrode, C.J.; Thomas, T.L. Bipolar hemiarthroplasty for subcapital fracture of the femoral neck. A prospective randomised trial of cemented Thompson and uncemented Moore stems. J. Bone Jt. Surg. Br. 1991, 73, 322–324. [Google Scholar] [CrossRef]
- Inngul, C.; Blomfeldt, R.; Ponzer, S.; Enocson, A. Cemented versus uncemented arthroplasty in patients with a displaced fracture of the femoral neck: A randomised controlled trial. Bone Jt. J. 2015, 97, 1475–1480. [Google Scholar] [CrossRef] [Green Version]
- Langslet, E.; Frihagen, F.; Opland, V.; Madsen, J.E.; Nordsletten, L.; Figved, W. Cemented versus uncemented hemiarthroplasty for displaced femoral neck fractures: 5-year followup of a randomized trial. Clin. Orthop. Relat. Res. 2014, 472, 1291–1299. [Google Scholar] [CrossRef] [Green Version]
- Moerman, S.; Mathijssen, N.M.C.; Niesten, D.D.; Riedijk, R.; Rijnberg, W.J.; Koeter, S.; Kremers van de Hei, K.; Tuinebreijer, W.E.; Molenaar, T.L.; Nelissen, R.G.H.H.; et al. More complications in uncemented compared to cemented hemiarthroplasty for displaced femoral neck fractures: A randomized controlled trial of 201 patients, with one year follow-up. BMC Musculoskelet. Disord. 2017, 18, 169. [Google Scholar]
- Parker, M.J.; Gurusamy, K.S.; Azegami, S. Arthroplasties (with and without bone cement) for proximal femoral fractures in adults. Cochrane Database Syst. Rev. 2010, 6, CD001706. [Google Scholar] [CrossRef]
- Evaniew, N.; Madden, K.; Bhandari, M. Cochrane in CORR(R): Comment on: Arthroplasties (with and without bone cement) for proximal femoral fractures in adults. Clin. Orthop. Relat. Res. 2014, 472, 1367–1372. [Google Scholar] [CrossRef] [Green Version]
- Boymans, T.A.; Heyligers, I.C.; Grimm, B. Discrepancy and contradiction regarding fixation of hip stems with or without cement: Survey among 765 hip arthroplasty specialists. HIP Int. 2018, 28, 514–521. [Google Scholar] [CrossRef]
- Chechik, O.; Khashan, M.; Lador, R.; Salai, M.; Amar, E. Surgical approach and prosthesis fixation in hip arthroplasty world wide. Arch. Orthop. Trauma Surg. 2013, 133, 1595–1600. [Google Scholar] [CrossRef] [PubMed]
- Huo, M.H.; Dumont, G.D.; Knight, J.R.; Mont, M.A. What’s new in total hip arthroplasty. J. Bone Jt. Surg. Am. 2011, 83, 1944–1950. [Google Scholar] [CrossRef] [PubMed]
- Troelsen, A.; Malchau, E.; Sillesen, N.; Malchau, H. A review of current fixation use and registry outcomes in total hip arthroplasty: The uncemented paradox. Clin. Orthop. Relat. Res. 2013, 471, 2052–2059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, L.C.; Hungerford, D.S. Cement disease. Clin. Orthop. Relat. Res. 1987, 192–206. [Google Scholar] [CrossRef]
- Donaldson, A.J.; Thomson, H.E.; Harper, N.J.; Kenny, N.W. Bone cement implantation syndrome. Br. J. Anaesth. 2009, 102, 12–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parvizi, J.; Holiday, A.D.; Ereth, M.H.; Lewallen, D.G. The Frank Stinchfield Award. Sudden death during primary hip arthroplasty. Clin. Orthop. Relat. Res. 1999, 369, 39–48. [Google Scholar] [CrossRef]
- Ekman, E.; Laaksonen, I.; Isotalo, K.; Liukas, A.; Vahlberg, T.; Makela, K. Cementing does not increase the immediate postoperative risk of death after total hip arthroplasty or hSemiarthroplasty: A hospital-based study of 10,677 patients. Acta Orthop. 2019, 90, 270–274. [Google Scholar] [CrossRef] [Green Version]
- Hines, C.B. Understanding bone cement implantation syndrome. AANA J. 2018, 86, 433–441. [Google Scholar]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lutnick, E.; Kang, J.; Freccero, D.M. Surgical Treatment of Femoral Neck Fractures: A Brief Review. Geriatrics 2020, 5, 22. https://doi.org/10.3390/geriatrics5020022
Lutnick E, Kang J, Freccero DM. Surgical Treatment of Femoral Neck Fractures: A Brief Review. Geriatrics. 2020; 5(2):22. https://doi.org/10.3390/geriatrics5020022
Chicago/Turabian StyleLutnick, Ellen, Jeansol Kang, and David M. Freccero. 2020. "Surgical Treatment of Femoral Neck Fractures: A Brief Review" Geriatrics 5, no. 2: 22. https://doi.org/10.3390/geriatrics5020022
APA StyleLutnick, E., Kang, J., & Freccero, D. M. (2020). Surgical Treatment of Femoral Neck Fractures: A Brief Review. Geriatrics, 5(2), 22. https://doi.org/10.3390/geriatrics5020022