Economic Potential for Distributed Manufacturing of Adaptive Aids for Arthritis Patients in the U.S.



Abstract

1. Introduction
2. Materials and Methods
2.1. Materials
2.2. 3-D Printers
2.3. Adaptive Aid Selection
- They had freely available STL posted on an open-source 3-D printing design website MyMiniFactory (www.myminifactory.com). MyMiniFactory was used because all of the designs have already been pre-screened to be 3-D printable by MyMiniFactory staff.
- They contained the source code (e.g., CAD design file from an open source and thus accessible CAD software package). This allows for relatively straight-forward customization of the device for specific people needing the aid.
- They were licensed with an open-source compatible license or designer requests as defined by the Open Source Hardware Association [54].
- They were able to be printed on a consumer grade 3-D printer (e.g., no high-cost precision metal 3-D printing or large scale printing).
- They were able to be printed and used if manufactured from PLA (e.g., no specialty materials or applications that involved severe chemical compatibility).
- They possessed a functionally equivalent commercialized proprietary product or a clear application for arthritis patients.
2.4. Arthritis Patient Economics
3. Results
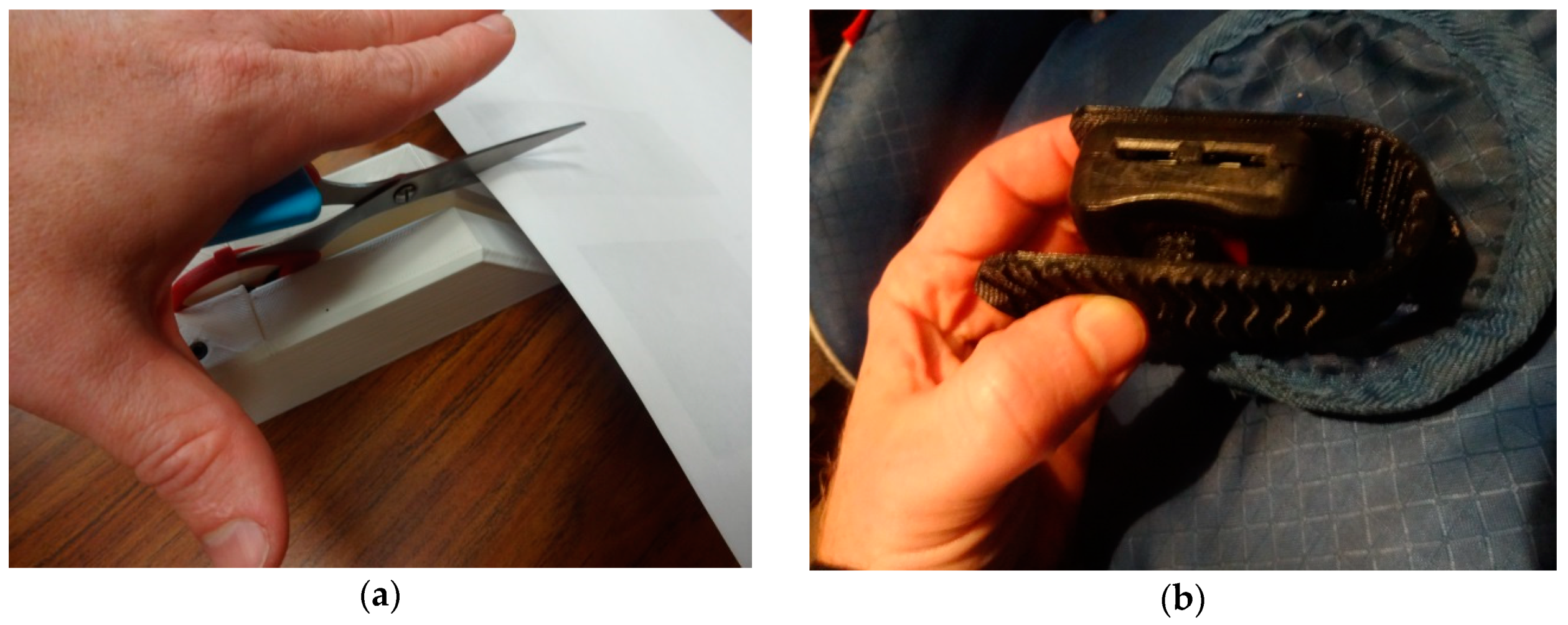
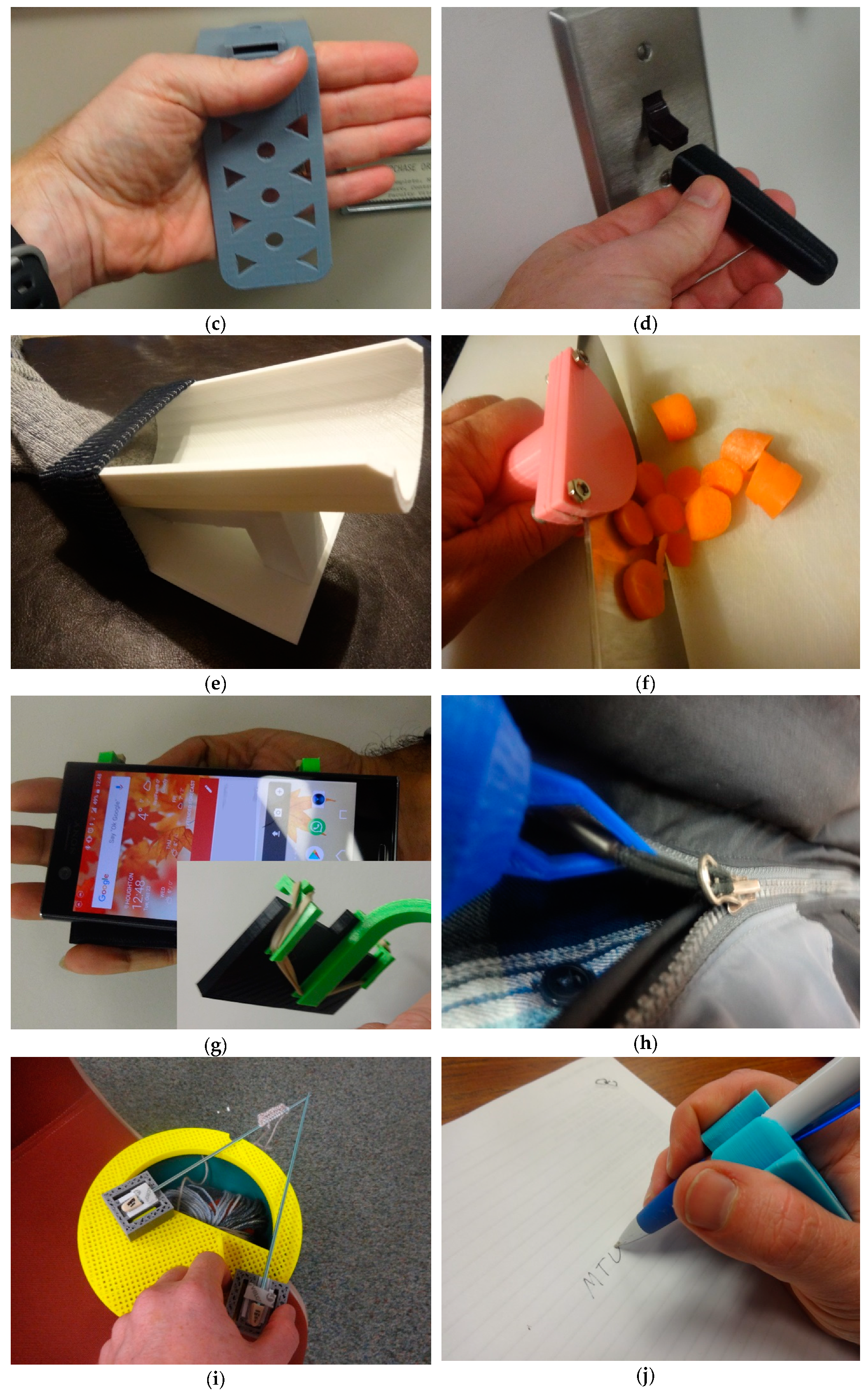
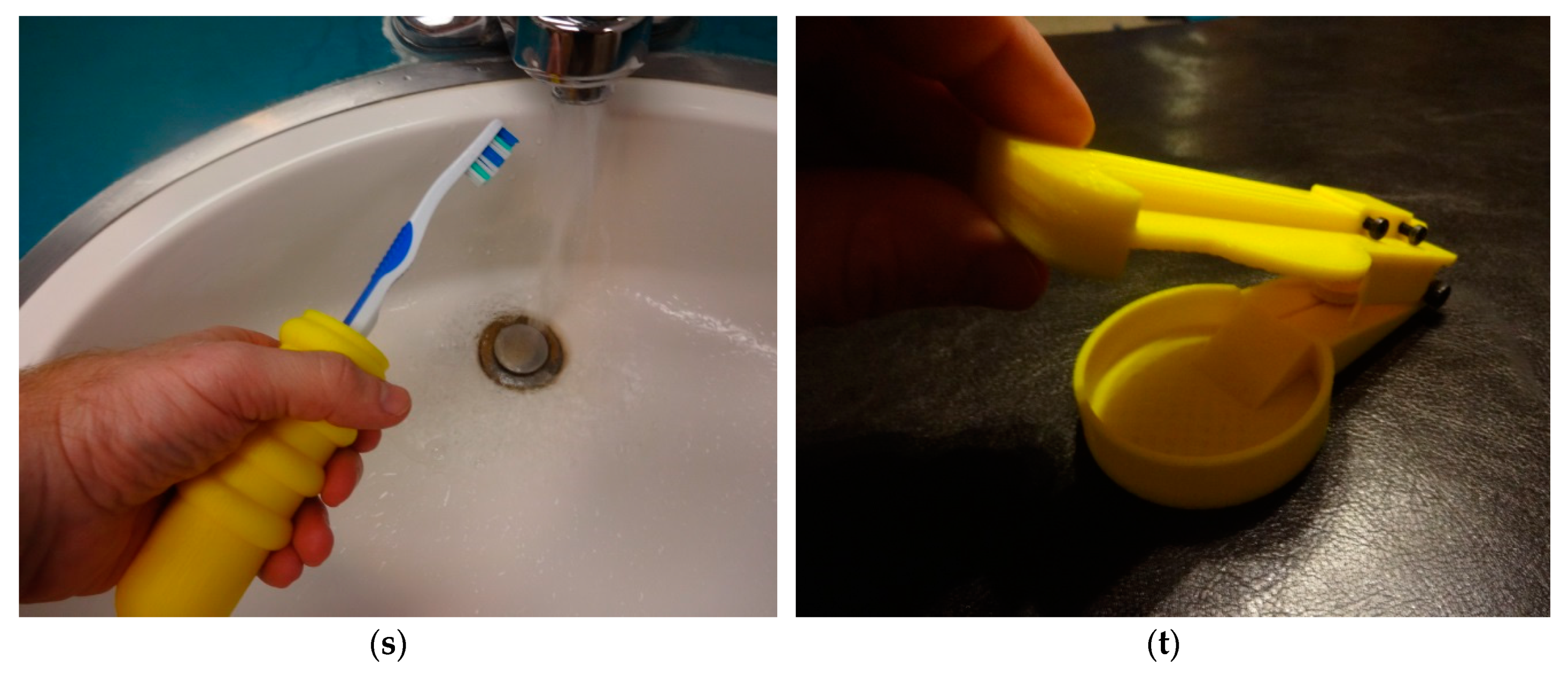
3-D Printable Adaptive Aids
4. Discussion
4.1. Distributed Manufacturing Economics
4.2. Limitations and Future Work
4.3. Applications for Both Old and Young People With Arthritis
4.4. Deployment of 3-D Printers as Manufacturing Tools in Context
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention (CDC). Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation—United States, 2010–2012. MMWR Morb. Mortal. Wkly. Rep. 2013, 62, 869–873. [Google Scholar]
- Barbour, K.E. Prevalence of Doctor-Diagnosed Arthritis at State and County Levels—United States, 2014. MMWR Morb. Mortal. Wkly. Rep. 2016, 65. [Google Scholar] [CrossRef]
- Barbour, K.E. Vital Signs: Prevalence of Doctor-Diagnosed Arthritis and Arthritis-Attributable Activity Limitation—United States, 2013–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66. [Google Scholar] [CrossRef]
- Arthritis-Related Statistics | Data and Statistics | Arthritis | CDC. Available online: https://www.cdc.gov/arthritis/data_statistics/arthritis-related-stats.htm (accessed on 24 October 2018).
- Hootman, J.M.; Helmick, C.G.; Barbour, K.E.; Theis, K.A.; Boring, M.A. Updated Projected Prevalence of Self-Reported Doctor-Diagnosed Arthritis and Arthritis-Attributable Activity Limitation among US Adults, 2015–2040. Arthritis Rheumatol. 2016, 68, 1582–1587. [Google Scholar] [CrossRef]
- Yelin, E.; Murphy, L.; Cisternas, M.G.; Foreman, A.J.; Pasta, D.J.; Helmick, C.G. Medical care expenditures and earnings losses among persons with arthritis and other rheumatic conditions in 2003, and comparisons with 1997. Arthritis Rheum. 2007, 56, 1397–1407. [Google Scholar] [CrossRef]
- Average (Median) Household Income 1990–2016. Available online: https://www.statista.com/statistics/200838/median-household-income-in-the-united-states/ (accessed on 24 October 2018).
- Right Hand Scoop Spoon. Available online: https://www.arthritissupplies.com/right-hand-scoop-spoon.html (accessed on 24 October 2018).
- Amazon.com: Winco 18/0 Stainless Steel Dinner Spoons, Set of 12, Windsor Pattern: Kitchen & Dining. Available online: https://www.amazon.com/Winco-Stainless-Dinner-Windsor-pattern/dp/B002XG5504/ref=sr_1_3?ie=UTF8&qid=1540388097&sr=8-3&keywords=spoon (accessed on 24 October 2018).
- Trump Tariff, China Trade War: Consumer Goods, Americans Will Be Hit—Business Insider. Available online: https://www.businessinsider.com/trump-tariff-china-trade-war-consumer-goods-2018-9 (accessed on 24 October 2018).
- Trump Pulls US out of UN Postal Scheme on China Price Concerns. Available online: http://www.theguardian.com/us-news/2018/oct/17/trump-universal-postal-union-withdraw-foreign-postal-rates (accessed on 24 October 2018).
- Orgera, K.; Damico, A. 2018 How Many Seniors Are Living in Poverty? National and State Estimates under the Official and Supplemental Poverty Measures in 2016; The Henry J. Kaiser Family Foundation: Oakland, CA, USA, 2018. [Google Scholar]
- Scan, B. How to Make (almost) Anything. The Economist. 2005. Available online: http://www.economist.com/node/4031304 (accessed on 11 October 2017).
- Gershenfeld, N. How to Make almost Anything: The Digital Fabrication Revolution. 2012. Available online: http://cba.mit.edu/docs/papers/12.09.FA.pdf (accessed on 28 October 2017).
- Markillie, P. A Third Industrial Revolution. The Economist. 2012. Available online: http://www.economist.com/node/21552901 (accessed on 11 October 2017).
- Gwamuri, J.; Wittbrodt, B.; Anzalone, N.; Pearce, J. Reversing the Trend of Large Scale and Centralization in Manufacturing: The Case of Distributed Manufacturing of Customizable 3-D-Printable Self-Adjustable Glasses. Chall. Sustain. 2014, 2, 30–40. [Google Scholar] [CrossRef]
- Wohler, T. Wohlers Report 2016: 3D Printing and Additive Manufacturing State of the Industry Annual Worldwide Progress Report; Wohlers Associates Inc.: Fort Collins, CO, USA, 2016. [Google Scholar]
- Anderson, P.; Sherman, C.A. A discussion of new business models for 3D printing. Int. J. Technol. Mark. 2007, 2, 280–294. [Google Scholar] [CrossRef]
- Laplume, A.; Petersen, B.; Pearce, J. Global value chains from a 3D printing perspective. J. Int. Bus. Stud. 2016, 47, 595–609. [Google Scholar] [CrossRef]
- Laplume, A.; Anzalone, G.; Pearce, J. Open-source, self-replicating 3-D printer factory for small-business manufacturing. Int. J. Adv. Manuf. Technol. 2015, 85, 633–642. [Google Scholar] [CrossRef]
- Ariel Bogle. Can UPS Help Make 3-D Printing Mainstream? Available online: http://www.slate.com/blogs/future_tense/2013/08/02/ups_plans_to_test_3_d_printing_services_in_u_s_stores.html (accessed on 22 March 2018).
- HOME DEPOT | DIY MEETS MIY (MAKE IT YOURSELF). Available online: https://www.makerbot.com/media-center/2014/07/14/home-depot-diy-meets-miy-make (accessed on 22 March 2018).
- Byard, D.J.; Woer, A.L.; Oakley, R.B.; Fiedler, M.J.; Snabes, S.L.; Pearce, J.M. Green Fab Lab Applications of Large-Area Waste Polymer-based Additive Manufacturing. Unpublished work. 2018. [Google Scholar]
- Michele Moorefield-Lang, H. Makers in the library: Case studies of 3D printers and maker spaces in library settings. Libr. Hi Tech 2014, 32, 583–593. [Google Scholar] [CrossRef]
- Moorefield-Lang, H. Change in the Making: Makerspaces and the Ever-Changing Landscape of Libraries. TechTrends 2015, 59, 107–112. [Google Scholar] [CrossRef]
- Pryor, S. Implementing a 3D Printing Service in an Academic Library. J. Libr. Adm. 2014, 54, 1–10. [Google Scholar] [CrossRef]
- Weber, S. The Success of Open Source; Harvard University Press: Cambridge, MA, USA, 2004; ISBN 978-0-674-01292-9. [Google Scholar]
- Gibb, A.; Abadie, S. Building Open Source Hardware: DIY Manufacturing for Hackers and Makers, 1st ed.; Addison-Wesley Professional: Boston, MA, USA, 2014; ISBN 978-0-321-90604-5. [Google Scholar]
- Oberloier, S.; Pearce, J.; Oberloier, S.; Pearce, J.M. General Design Procedure for Free and Open-Source Hardware for Scientific Equipment. Designs 2017, 2, 2. [Google Scholar] [CrossRef]
- Rundle, G. A Revolution in the Making; Simon and Schuster: New York, NY, USA, 2014; ISBN 978-1-922213-48-8. [Google Scholar]
- Sells, E.; Bailard, S.; Smith, Z.; Bowyer, A.; Olliver, V. RepRap: The Replicating Rapid Prototyper-Maximizing Customizability by Breeding the Means of Production 2010. In Proceedings of the World Conference on Mass Customization and Personalization, Cambridge, MA, USA, 7–10 October 2007; ISBN 978-981-4280-25-9. [Google Scholar]
- Jones, R.; Haufe, P.; Sells, E.; Iravani, P.; Olliver, V.; Palmer, C.; Bowyer, A. RepRap-the Replicating Rapid Prototyper. Robotica 2011, 29, 177–191. [Google Scholar] [CrossRef]
- Bowyer, A. 3D Printing and Humanity’s First Imperfect Replicator. 3D Print. Addit. Manuf. 2014, 1, 4–5. [Google Scholar] [CrossRef]
- Wittbrodt, B.; Glover, A.; Laureto, J.; Anzalone, G.; Oppliger, D.; Irwin, J.; Pearce, J. Life-Cycle Economic Analysis of Distributed Manufacturing with Open-Source 3-D Printers. Mechatronics 2013, 23, 713–726. [Google Scholar] [CrossRef]
- Petersen, E.E.; Pearce, J. Emergence of Home Manufacturing in the Developed World: Return on Investment for Open-Source 3-D Printers. Technologies 2017, 5, 7. [Google Scholar] [CrossRef]
- Petersen, E.E.; Kidd, R.W.; Pearce, J.M. Impact of DIY Home Manufacturing with 3D Printing on the Toy and Game Market. Technologies 2017, 5, 45. [Google Scholar] [CrossRef]
- Woern, A.L.; Pearce, J.M. Distributed Manufacturing of Flexible Products: Technical Feasibility and Economic Viability. Technologies 2017, 5, 71. [Google Scholar] [CrossRef]
- Smith, P. Commons people: Additive manufacturing enabled collaborative commons production. In Proceedings of the 15th RDPM Conference, Loughborough, UK, 26–27 April 2015. [Google Scholar]
- Pearce, J.M. Return on investment for open source scientific hardware development. Sci. Public Policy 2016, 43, 192–195. [Google Scholar] [CrossRef]
- Wijnen, B.; Sanders, P.; Pearce, J.M. Improved model and experimental validation of deformation in fused filament fabrication of polylactic acid. Prog. Addit. Manuf. 2018. [Google Scholar] [CrossRef]
- Hoffman, T.; LulzBot TAZ 5 3D Printer. PCMAG. 2015. Available online: http://www.pcmag.com/article2/0,2817,2489833,00.asp (accessed on 6 February 2017).
- Chilson, L.; The Difference between ABS and PLA for 3D Printing. ProtoParadigm. 2013. Available online: http://www.protoparadigm.com/news-updates/the-difference-between-abs-and-pla-for-3d-printing/ (accessed on 6 February 2017).
- Stephens, B.; Azimi, P.; El Orch, Z.; Ramos, T. Ultrafine Particle Emissions from Desktop 3D Printers. Atmos. Environ. 2013, 79, 334–339. [Google Scholar] [CrossRef]
- Tokiwa, Y.; Calabia, B.; Ugwu, C.; Aiba, S. Biodegradability of Plastics. Int. J. Mol. Sci. 2009, 10, 3722–3742. [Google Scholar] [CrossRef]
- Woern, A.L.; McCaslin, J.R.; Pringle, A.M.; Pearce, J.M. RepRapable Recyclebot: Open source 3-D printable extruder for converting plastic to 3-D printing filament. HardwareX 2018, 4, e00026. [Google Scholar] [CrossRef]
- Anderson, I. Mechanical Properties of Specimens 3D Printed with Virgin and Recycled Polylactic Acid. 3D Print. Addit. Manuf. 2017, 4, 110–115. [Google Scholar] [CrossRef]
- Cruz Sanchez, F.A.C.; Boudaoud, H.; Hoppe, S.; Camargo, M. Polymer recycling in an open-source additive manufacturing context: Mechanical issues. Addit. Manuf. 2017, 17, 87–105. [Google Scholar] [CrossRef]
- Pearce, J.M.; Wijnen, B.; Anzalone, G.C. Multi-material additive and subtractive prosumer digital fabrication with a free and open-source convertible delta RepRap 3-D printer. Rapid Prototyp. J. 2015, 21, 506–519. [Google Scholar] [CrossRef]
- All Things Athena, II. Contribute to Phidiasllc/AthenaII Development by Creating an Account on GitHub, phidiasllc. 2018. Available online: https://github.com/phidiasllc/athenaII (accessed on 4 December 2018).
- GNU Affero General Public License. gnu.org. Available online: https://www.gnu.org/licenses/agpl-3.0.en.html (accessed on 24 October 2018).
- Ultimaker Cura: Advanced 3D Printing Software, Made Accessible | Ultimaker. Available online: https://ultimaker.com/en/products/ultimaker-cura-software (accessed on 24 October 2018).
- Tymrak, B.M.; Kreiger, M.; Pearce, J.M. Mechanical properties of components fabricated with open-source 3-D printers under realistic environmental conditions. Mater. Des. 2014, 58, 242–246. [Google Scholar] [CrossRef]
- Wijnen, B.; Anzalone, G.C.; Haselhuhn, A.S.; Sanders, P.G.; Pearce, J.M. Free and Open-source Control Software for 3-D Motion and Processing. J. Open Res. Softw. 2016, 4, e2. [Google Scholar] [CrossRef]
- Open Source Hardware (OSHW) Definition 1.0. Definition (English). Available online: https://www.oshwa.org/definition/ (accessed on 24 October 2018).
- Amazon.com: 1.75 mm Black PLA 3D Printer Filament—1 kg Spool (2.2 lbs)—Dimensional Accuracy +/− 0.03 mm: Industrial & Scientific. Available online: https://www.amazon.com/1-75mm-Black-PLA-Printer-Filament/dp/B01BZ5ND8O (accessed on 25 October 2018).
- Electric Power Monthly, Energy Information Administration, Electricity Data. Available online: https://www.eia.gov/electricity/monthly/epm_table_grapher.php?t=epmt_5_6_a (accessed on 25 October 2018).
- 3D Printable Scissor Arthritis Aid by Aubrey. Available online: https://www.myminifactory.com/object/3d-print-scissor-arthritis-aid-77550 (accessed on 25 October 2018).
- 3D Printable Car Seat Arthritis Aid by Matthew Olson. Available online: https://www.myminifactory.com/object/3d-print-car-seat-arthritis-aid-77397 (accessed on 25 October 2018).
- 3D Printable Arthritis Handle with Can Opener by Andrew Wunderlin. Available online: https://www.myminifactory.com/object/3d-print-arthritishandlewithcanopener-77533 (accessed on 25 October 2018).
- 3D Printable Light Switch Extension Lever by Devon Smith. Available online: https://www.myminifactory.com/object/3d-print-77490 (accessed on 25 October 2018).
- 3D Printable Sock Assistant by Emily Weidensee. Available online: https://www.myminifactory.com/object/3d-print-sock-assist-77472 (accessed on 25 October 2018).
- 3D Printable Knife Guide Arthritis Aid by Christopher Thormodson. Available online: https://www.myminifactory.com/object/3d-print-knife-guide-arthritis-aid-77506 (accessed on 25 October 2018).
- 3D Printable Adaptive Aid Phone Holder by Wesley. Available online: https://www.myminifactory.com/object/3d-print-adaptive-aid-phone-holder-77771 (accessed on 25 October 2018).
- 3D Printable Zipper Pull Arthritic Aide by Ben Joseph. Available online: https://www.myminifactory.com/object/3d-print-zipper-pull-arthritic-aide-77532 (accessed on 25 October 2018).
- 3D Printable Arthritis Knitting Aid by Cassandra Gietek. Available online: https://www.myminifactory.com/object/3d-print-arthritis-knitting-aid-77534 (accessed on 25 October 2018).
- 3D Printable Arthritis Pen Holder by Brian Roman. Available online: https://www.myminifactory.com/object/3d-print-arthritis-pen-holder-77541 (accessed on 25 October 2018).
- 3D Printable Nail Clipper Holder by Jacob Jarvis. Available online: https://www.myminifactory.com/object/3d-print-nail-clipper-holder-77548 (accessed on 25 October 2018).
- 3D Printable Cane Holder for Arthritis Patients by Shaunak Prasad Mhatre. Available online: https://www.myminifactory.com/object/3d-print-77539 (accessed on 25 October 2018).
- 3D Printable Key Turner Aid by Adam Mitchell. Available online: https://www.myminifactory.com/object/3d-print-77416 (accessed on 25 October 2018).
- 3D Printable Arthritis Typing Aid by Alec Stilwell. Available online: https://www.myminifactory.com/object/3d-print-arthritis-typing-aid-77579 (accessed on 25 October 2018).
- 3D Printable Pop Can Opener by Logan Brunette. Available online: https://www.myminifactory.com/object/3d-print-pop-can-opener-77588 (accessed on 25 October 2018).
- 3D Printable Arthritis Assist Dog Leash Snap by Michael James. Available online: https://www.myminifactory.com/object/3d-print-arthritus-assist-dog-leash-snap-77596 (accessed on 25 October 2018).
- 3D Printable Gas Cap Wrench by Cal McCarty. Available online: https://www.myminifactory.com/object/3d-print-77777 (accessed on 25 October 2018).
- 3D Printable Handle Aid by Quinn Kaspriak. Available online: https://www.myminifactory.com/object/3d-print-handle-adapter-arthritis-aid-77606 (accessed on 25 October 2018).
- 3D Printable Arthritis Toothbrush Grip by Weston Butler. Available online: https://www.myminifactory.com/object/3d-print-arthritis-toothbrush-grip-77601 (accessed on 25 October 2018).
- 3D Printable Pill Splitter by Alieksei Petsiuk. Available online: https://www.myminifactory.com/object/3d-print-77608 (accessed on 25 October 2018).
- Zhang, C.; Anzalone, N.C.; Faria, R.P.; Pearce, J.M. Open-source 3D-printable optics equipment. PLoS ONE 2013, 8, e59840. [Google Scholar] [CrossRef]
- Pearce, J. Building Research Equipment with Free, Open-Source Hardware. Science 2012, 337, 1303–1304. [Google Scholar] [CrossRef]
- Pearce, J. Open-Source Lab: How to Build Your Own Hardware and Reduce Research Costs, 1st ed.; Elsevier: Waltham, MA, USA, 2014; ISBN 978-0-12-410486-0. [Google Scholar]
- Baden, T.; Chagas, A.; Marzullo, T.; Prieto-Godino, L.; Euler, T. Open Labware: 3-D Printing Your Own Lab Equipment. PLoS Biol. 2015, 13, e1002086. [Google Scholar] [CrossRef]
- Coakley, M.; Hurt, D.E. 3D Printing in the Laboratory: Maximize Time and Funds with Customized and Open-Source Labware. J. Lab. Autom. 2016, 21, 489–495. [Google Scholar] [CrossRef]
- Pearce, J. Quantifying the Value of Open Source Hardware Development. Mod. Econ. 2015, 6, 1–11. [Google Scholar] [CrossRef]
- Nilsiam, Y.; Pearce, J.M.; Nilsiam, Y.; Pearce, J.M. Free and Open Source 3-D Model Customizer for Websites to Democratize Design with OpenSCAD. Designs 2017, 1, 5. [Google Scholar] [CrossRef]
- Alexander Hars, S.O. Working for Free? Motivations for Participating in Open-Source Projects. Int. J. Electron. Commer. 2002, 6, 25–39. [Google Scholar] [CrossRef]
- Stallman, R. Viewpoint: Why “Open Source” Misses the Point of Free Software. Commun. ACM 2009, 52, 31–33. [Google Scholar] [CrossRef]
- Samoladas, I.; Stamelos, I.; Angelis, L.; Oikonomou, A. Open Source Software Development Should Strive for Even Greater Code Maintainability. Commun. ACM 2004, 47, 83–87. [Google Scholar] [CrossRef]
- Batalden, P.; Splaine, M. What Will It Take to Lead the Continual Improvement and Innovation of Health Care in the Twenty-first Century? Qual. Manag. Healthc. 2002, 11, 45. [Google Scholar] [CrossRef]
- Hastings, S.; Choate, A.; Mahanna, E.; Floegel, T.; Allen, K.; Van Houtven, C.; Wang, V.; Hastings, S.N.; Choate, A.L.; Mahanna, E.P.; et al. Early Mobility in the Hospital: Lessons Learned from the STRIDE Program. Geriatrics 2018, 3, 61. [Google Scholar] [CrossRef]
- CNN, G.R. Caroline Wozniacki “Shocked” by Rheumatoid Arthritis Diagnosis. Available online: https://edition.cnn.com/2018/10/26/sport/caroline-wozniacki-rheumatoid-arthritis-tennis-wta-finals-spt-intl/index.html (accessed on 5 November 2018).
- Helmick, C.G.; Felson, D.T.; Lawrence, R.C.; Gabriel, S.; Hirsch, R.; Kwoh, C.K.; Liang, M.H.; Kremers, H.M.; Mayes, M.D.; Merkel, P.A.; et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part I. Arthritis Rheum. 2008, 58, 15–25. [Google Scholar] [CrossRef]
- Maetzel, A.; Li, L.C.; Pencharz, J.; Tomlinson, G.; Bombardier, C. The economic burden associated with osteoarthritis, rheumatoid arthritis, and hypertension: A comparative study. Ann. Rheum. Dis. 2004, 63, 395–401. [Google Scholar] [CrossRef]
- National Statistics | Data and Statistics | Arthritis | CDC. Available online: https://www.cdc.gov/arthritis/data_statistics/national-statistics.html (accessed on 9 November 2018).
- Murphy, L.B.; Cisternas, M.G.; Pasta, D.J.; Helmick, C.G.; Yelin, E.H. Medical Expenditures and Earnings Losses among US Adults with Arthritis in 2013. Arthritis Care Res. 2018, 70, 869–876. [Google Scholar] [CrossRef]
- 3D Printable Doorknob Extender by Reis Jones. Available online: https://www.myminifactory.com/object/3d-print-doorknob-extender-77597 (accessed on 9 November 2018).
- 3D Printable Easy Automotive Handle by Anthony. Available online: https://www.myminifactory.com/object/3d-print-easy-automotive-handle-77589 (accessed on 9 November 2018).
- Abell, J.E.; Hootman, J.M.; Helmick, C.G. Prevalence and impact of arthritis among nursing home residents. Ann. Rheum. Dis. 2004, 63, 591–594. [Google Scholar] [CrossRef]
- Torio, C.M.; Moore, B.J. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2013: Statistical Brief #204; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2006.
- Yeung, K.-T.; Lin, C.-H.; Teng, Y.-L.; Chen, F.-F.; Lou, S.-Z.; Chen, C.-L. Use of and Self-Perceived Need for Assistive Devices in Individuals with Disabilities in Taiwan. PLoS ONE 2016, 11, e0152707. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Adaptive Aid | Description | CAD | Source |
|---|---|---|---|
| Scissor aid | Enables the use of scissors using palm for cutting and fist for opening. | FreeCAD | [57] |
| Car seat aid | Car seat buckle depressor using a living hinge. | FreeCAD | [58] |
| Drawer aid | Drawer and cabinet opener with built in can opener. | FreeCAD | [59] |
| Light switch aid | Easier access for turning on and off light switches. | FreeCAD | [60] |
| Sock aid | An assistive aid for putting on socks that will not slip on carpet. | OpenSCAD | [61] |
| Knife guide aid | Used to cut up ingredients with large handle attached. | FreeCAD | [62] |
| Phone holder aid | Attaches to write for the easy accessibility of your phone. | FreeCAD | [63] |
| Zipper pull aid | Used to pull up zippers of necessary clothing items. | FreeCAD | [64] |
| Knitting aid | Large blocks for a better grip on the knitting needles. | OpenSCAD | [65] |
| Pen holder aid | Provides a larger area that encompasses the pen to hold in hand. | OpenSCAD | [66] |
| Nail clipper aid | Provides easy access to clip one’s nails by using the palm of your hand. | OpenSCAD | [67] |
| Cane holder aid | Allows the user to hang their cane for easy access. | FreeCAD | [68] |
| Key aid | Attaches to the users key for a larger surface area to grab on to. | FreeCAD | [69] |
| Typing aid | Round ball can be customized for palm size and allows user to type on keyboard easier. | OpenSCAD | [70] |
| Pop can aid | Assists in the opening of pop cans by use of a hook. | OpenSCAD | [71] |
| Dog leash aid | Uses a “lock and key” method to hold onto your dog’s leash. | OpenSCAD | [72] |
| Gas cap aid | Easy grip handle to be able to open gas cap on car. | OpenSCAD | [73] |
| Handle adapter aid | Ability to attach to any handle for easier use and grip. | FreeCAD | [74] |
| Toothbrush aid | Enables user to grab their toothbrush more easily. Can be customized for hand size. | OpenSCAD | [75] |
| Pill splitter aid | Users can use their palm to push down and split their medication. | FreeCAD | [76] |
| Adaptive Aid | Mass (g) | Distributed Manufacturing Cost (US$) | Purchase Cost (US$) | Savings (US$) | Savings (%) |
|---|---|---|---|---|---|
| Scissor aid | 116.19 | 2.62 | 31.95 | 29.33 | 91.8 |
| Car seat aid | 16.36 | 0.33 | 14.99 | 14.66 | 97.8 |
| Can opener aid | 27.50 | 0.55 | 9.99 | 9.44 | 94.5 |
| Light switch aid | 19.98 | 0.40 | 17.99 | 17.59 | 97.8 |
| Sock aid | 161.16 | 3.22 | 43.95 | 40.73 | 92.7 |
| Knife guide aid | 37.61 | 0.95 | 12.95 | 12.00 | 92.7 |
| Phone holder aid | 36.77 | 0.79 | 49.99 | 49.20 | 98.4 |
| Zipper pull aid | 22.62 | 0.45 | 19.75 | 19.30 | 97.7 |
| Knitting aid | 88.07 | 1.96 | 16.99 | 15.03 | 88.4 |
| Pen holder aid | 11.14 | 0.22 | 9.95 | 9.73 | 97.8 |
| Nail clipper aid | 50.75 | 1.01 | 10.95 | 9.94 | 90.8 |
| Cane holder aid | 25.00 | 0.50 | 14.95 | 14.45 | 96.7 |
| Key aid | 20.66 | 0.41 | 9.10 | 8.69 | 95.5 |
| Typing aid | 70.25 | 1.40 | 49.95 | 48.55 | 97.2 |
| Pop can aid | 20.03 | 0.45 | 5.99 | 5.54 | 92.5 |
| Dog leash aid | 14.92 | 0.30 | 19.99 | 19.69 | 98.5 |
| Gas cap aid | 102.42 | 2.05 | 14.95 | 12.90 | 86.3 |
| Handle adapter aid | 85.89 | 1.72 | 21.95 | 20.23 | 92.1 |
| Toothbrush aid | 69.55 | 1.40 | 18.79 | 17.39 | 92.5 |
| Pill splitter aid | 53.55 | 1.27 | 23.75 | 22.48 | 94.7 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallup, N.; Bow, J.K.; Pearce, J.M. Economic Potential for Distributed Manufacturing of Adaptive Aids for Arthritis Patients in the U.S. Geriatrics 2018, 3, 89. https://doi.org/10.3390/geriatrics3040089
Gallup N, Bow JK, Pearce JM. Economic Potential for Distributed Manufacturing of Adaptive Aids for Arthritis Patients in the U.S. Geriatrics. 2018; 3(4):89. https://doi.org/10.3390/geriatrics3040089
Chicago/Turabian StyleGallup, Nicole, Jennifer K. Bow, and Joshua M. Pearce. 2018. "Economic Potential for Distributed Manufacturing of Adaptive Aids for Arthritis Patients in the U.S." Geriatrics 3, no. 4: 89. https://doi.org/10.3390/geriatrics3040089
APA StyleGallup, N., Bow, J. K., & Pearce, J. M. (2018). Economic Potential for Distributed Manufacturing of Adaptive Aids for Arthritis Patients in the U.S. Geriatrics, 3(4), 89. https://doi.org/10.3390/geriatrics3040089