Falls in Geriatric Populations and Hydrotherapy as an Intervention: A Brief Review



Abstract
1. Introduction
2. Postural Control in the Aging Population
3. Dual-Task Paradigm Leading to Falls
4. Balance Training for Fall Prevention
5. Hydrotherapy as an Intervention for Fall Prevention
6. Clinical Applications
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Important Facts about Fall. 2017. Available online: https://www.cdc.gov/homeandrecreationalsafety/falls/adultfalls.html (accessed on 8 October 2017).
- Agmon, M.; Belza, B.; Nguyen, H.Q.; Logsdon, R.G.; Kelly, V.E. A systematic review of interventions conducted in clinical or community settings to improve dual-task postural control in older adults. Clin. Interv. Aging 2014, 9, 477–492. [Google Scholar] [CrossRef] [PubMed]
- Sample, R.B.; Jackson, K.; Kinney, A.L.; Diestelkamp, W.S.; Reinert, S.S.; Bigelow, K.E. Manual and cognitive dual tasks contribute to fall-risk differentiation in posturography measures. J. Appl. Biomech. 2016, 32, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B.; Shupert, C.L.; Mirka, A. Components of postural dyscontrol in the elderly: A review. Neurobiol. Aging 1989, 10, 727–738. [Google Scholar] [CrossRef]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Dionyssiotis, Y. Analyzing the problem of falls among older people. Int. J. Gen. Med. 2012, 5, 805–813. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Lesinski, M.; Hortobágyi, T.; Muehlbauer, T.; Gollhofer, A.; Granacher, U. Effects of balance training on balance performance in healthy older adults: A systematic review and meta-analysis. Sports Med. 2015, 45, 1721–1738. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, 37–41. [Google Scholar] [CrossRef] [PubMed]
- McCollum, G.; Leen, T.K. Form and exploration of mechanical stability limits in erect stance. J. Motor. Behav. 1989, 21, 225–244. [Google Scholar] [CrossRef]
- Runge, C.F.; Shupert, C.L.; Horak, F.B.; Zajac, F.E. Ankle and hip postural strategies defined by joint torques. Gait Posture 1999, 10, 161–170. [Google Scholar] [CrossRef]
- Goble, D.J.; Coxon, J.P.; Wenderoth, N.; Van Impe, A.; Swinnen, S.P. Review: Proprioceptive sensibility in the elderly: Degeneration, functional consequences and plastic-adaptive processes. Neurosci. Biobehav. Rev. 2009, 33, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Silsupadol, P.; Ka-Chun, S.; Shumway-Cook, A.; Woollacott, M.H. Training of balance under single- and dual-task conditions in older adults with balance impairment. Phys. Ther. 2006, 86, 269–281. [Google Scholar] [PubMed]
- Bergamin, M.; Gobbo, S.; Zanotto, T.; Sieverdes, J.C.; Alberton, C.L.; Zaccaria, M.; Ermolao, A. Influence of age on postural sway during different dual-task conditions. Front. Aging Neurosci. 2014, 6, 271. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Cho, S.-R.; Yoo, G.E. The applicability of rhythm-motor tasks to a new dual task paradigm for older adults. Front. Neurol. 2017, 8, 671. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the Probability for Falls in Community-Dwelling Older Adults Using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar] [PubMed]
- Alfieri, F.; Riberto, M.; Abril-Carreres, A.; Boldó-Alcaine, M.; Rusca-Castellet, E.; Garreta-Figuera, R.; Battistella, L. Effectiveness of an exercise program on postural control in frail older adults. Clin. Interv. Aging 2012, 7, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Whitney, J.C.; Lord, S.R.; Herbert, R.D.; Cumming, R.G.; Close, J.T. Effective exercise for the prevention of falls: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2008, 56, 2234–2243. [Google Scholar] [CrossRef] [PubMed]
- Hrysomallis, C. Balance ability and athletic performance. Sports Med. 2011, 41, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Noh, D.K.; Lim, J.; Shin, H.; Paik, N. The effect of aquatic therapy on postural balance and muscle strength in stroke survivors—A randomized controlled pilot trial. Clin. Rehabil. 2008, 22, 966–976. [Google Scholar] [PubMed]
- Teasdale, N.; Simoneau, M. Attentional demands for postural control: The effects of aging and sensory reintegration. Gait Posture 2001, 14, 203–210. [Google Scholar] [CrossRef]
- Alikhajeh, Y.; Hosseini, S.A.; Moghaddam, A. Effects of hydrotherapy in static and dynamic balance among elderly men. Procedia Soc. Behav. Sci. 2012, 46, 2220–2224. [Google Scholar] [CrossRef]
- Resende, S.M.; Rassi, C.M.; Viana, F.P. Effects of hydrotherapy in balance and prevention of falls among elderly women. Braz. J. Phys. Ther. 2008, 12, 57. [Google Scholar] [CrossRef]
- Zhu, Z.; Cui, L.; Yin, M.; Yu, Y.; Zhou, X.; Wang, H.; Yan, H. Hydrotherapy vs. conventional land-based exercise for improving walking and balance after stroke: A randomized controlled trial. Clin. Rehabil. 2015, 30, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Volpe, D.; Giantin, M.G.; Maestri, R.; Frazzitta, G. Comparing the effects of hydrotherapy and land-based therapy on balance in patients with Parkinson’s disease: A randomized controlled pilot study. Clin. Rehabil. 2014, 28, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Devereux, K.; Robertson, D.; Kathryn Briffa, N. Effects of a water-based program on women 65 years and over: A randomised controlled trial. Aust. J. Physiother. 2005, 51, 102–108. [Google Scholar] [CrossRef]
- Hale, L.A.; Waters, D.; Herbison, P. A randomized controlled trial to investigate the effects of water-based exercise to improve falls risk and physical function in older adults with lower-extremity osteoarthritis. Arch. Phys. Med. Rehabil. 2012, 93, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Oddsson, L.I.; Boissy, P.; Melzer, I. How to improve gait and balance function in elderly individuals—Compliance with principles of training. Eur. Rev. Aging Phys. Act. 2007, 4, 15–23. [Google Scholar] [CrossRef]
- Melzer, I.; Elbar, O.; Tsedek, I.; Oddsson, L.I.E. A water-based training program that include perturbation exercises to improve stepping responses in older adults: Study protocol for a randomized controlled cross-over trial. BMC Geriatr. 2008, 8, 19. [Google Scholar] [CrossRef] [PubMed]
- Gobbo, S.; Bergamin, M.; Sieverdes, J.C.; Ermolao, A.; Zaccaria, M. Effects of exercise on dual-task ability and balance in older adults: A systematic review. Arch. Gerontol. Geriatr. 2014, 58, 177–187. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Level | Hydrotherapy Exercises |
|---|---|
| Level 1 & 2: Sit to stand exercises with external support (Level 1 exercises are performed with external support while Level 2 exercises are performed without external support) | Standing next to pool wall, wide base with feet, one hand support on pool wall. Repeat with shoulder-width stance and support. |
| Wide-base foot stance with hand support on wall, shift body weight in different directions as much as possible. | |
| Standing with pool wall hand support, and twisting trunk right and left as much as possible. | |
| Standing with support hand on the wall, wide-base foot stance, lift one foot from the pool base at a time. Repeat while in narrow stance. | |
| Standing with support, wide-base foot stance, and introduce leaning forward into the water. | |
| Shifting the base of support or closing eyes will increase the intensity of the exercises. | |
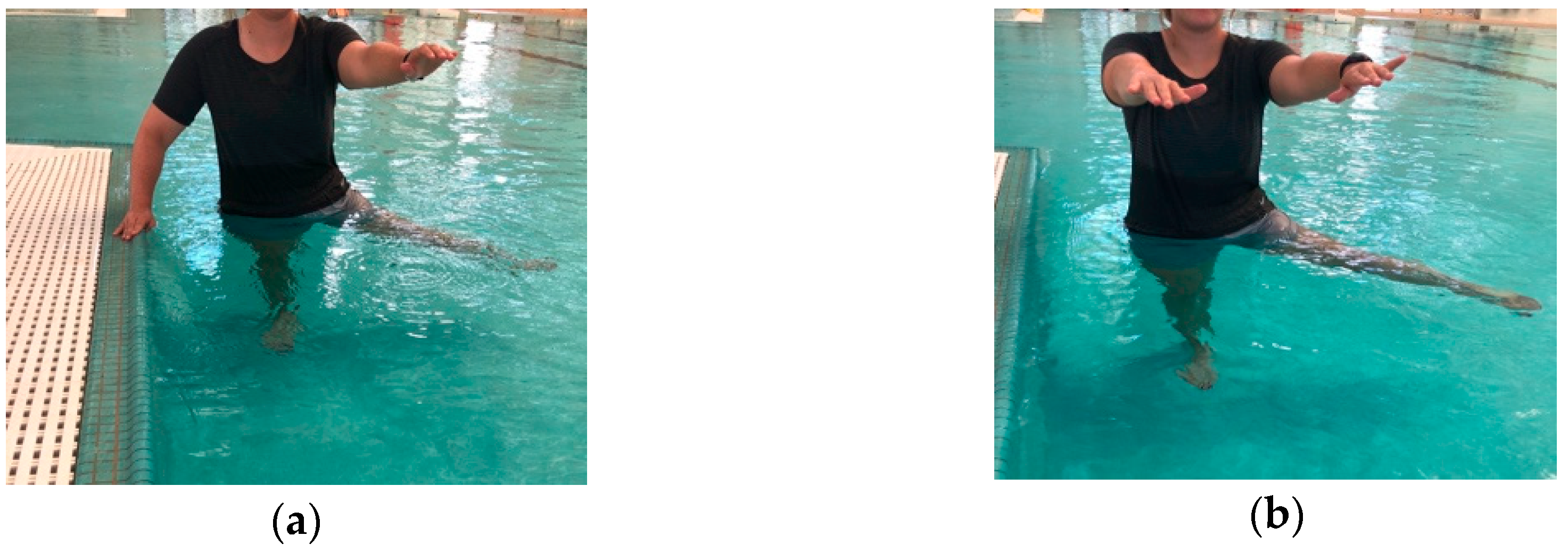
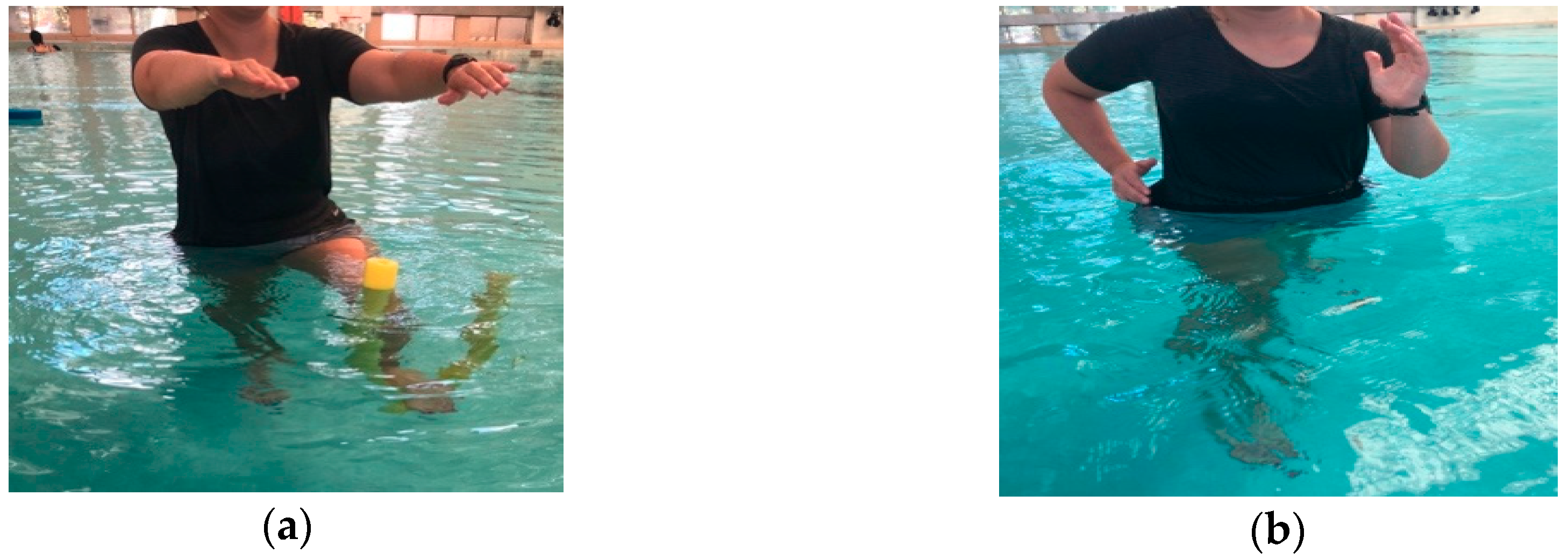
| Level 3: Standing exercises including bi-lateral stance with external support | Standing in unilateral stance while the opposite leg flexes and extends the knee with “noodle” under the foot. |
| Same as above, while throwing or catching a ball. | |
| Standing with wide/narrow foot base, holding a “noodle” with both hands and trying to drive it into the water while staying upright. | |
| Sitting on a “noodle” and staying upright with chest out of the water. | |
| Standing with both feet on the “noodle” and staying upright, with or without a cognitive task. | |
| Standing with both feet on a “noodle”, holding a “noodle” with both hands and trying to drive it into the water while staying upright. | |
| Cutting in different directions (e.g., anteriorly/posteriorly and medial/lateral), at differing speeds and in deeper water. | |
| Level 4: Standing exercises including uni-lateral stance, walking with no external support | Cutting directions as quickly as the subject can withstand. |
| Walking on a “noodle” with and without differing cognitive tasks. | |
| Adding neck movements to challenge the vestibular system. | |
| Similar to levels 3 and 4 but with added water turbulence and in different water depths. | |
| Level 5: Pushing exercises, reaction responses | Standing, wide base stance, while instructor pushes the participant in different directions, with and without knowledge. |
| Similar to level 4 but while standing on noodle, shifting base of support, while opening/closing eyes, adding cognitive tasks. | |
| Walking and being pushed by instructor/classmates with and without additional cognitive tasks. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turner, A.J.; Chander, H.; Knight, A.C. Falls in Geriatric Populations and Hydrotherapy as an Intervention: A Brief Review. Geriatrics 2018, 3, 71. https://doi.org/10.3390/geriatrics3040071
Turner AJ, Chander H, Knight AC. Falls in Geriatric Populations and Hydrotherapy as an Intervention: A Brief Review. Geriatrics. 2018; 3(4):71. https://doi.org/10.3390/geriatrics3040071
Chicago/Turabian StyleTurner, Alana J., Harish Chander, and Adam C. Knight. 2018. "Falls in Geriatric Populations and Hydrotherapy as an Intervention: A Brief Review" Geriatrics 3, no. 4: 71. https://doi.org/10.3390/geriatrics3040071
APA StyleTurner, A. J., Chander, H., & Knight, A. C. (2018). Falls in Geriatric Populations and Hydrotherapy as an Intervention: A Brief Review. Geriatrics, 3(4), 71. https://doi.org/10.3390/geriatrics3040071