Dysphagia Onset in Older Adults during Unrelated Hospital Admission: Quantitative Videofluoroscopic Measures

Abstract
:1. Introduction
2. Materials and Methods
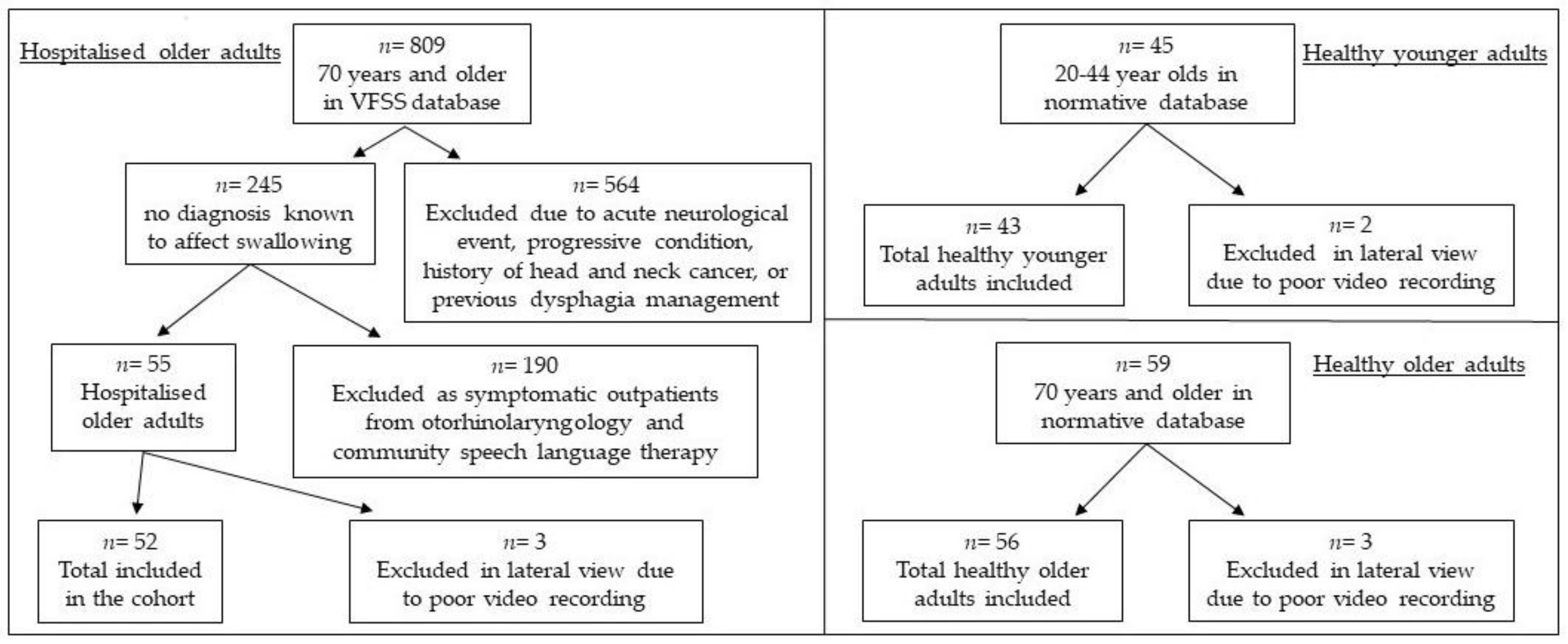
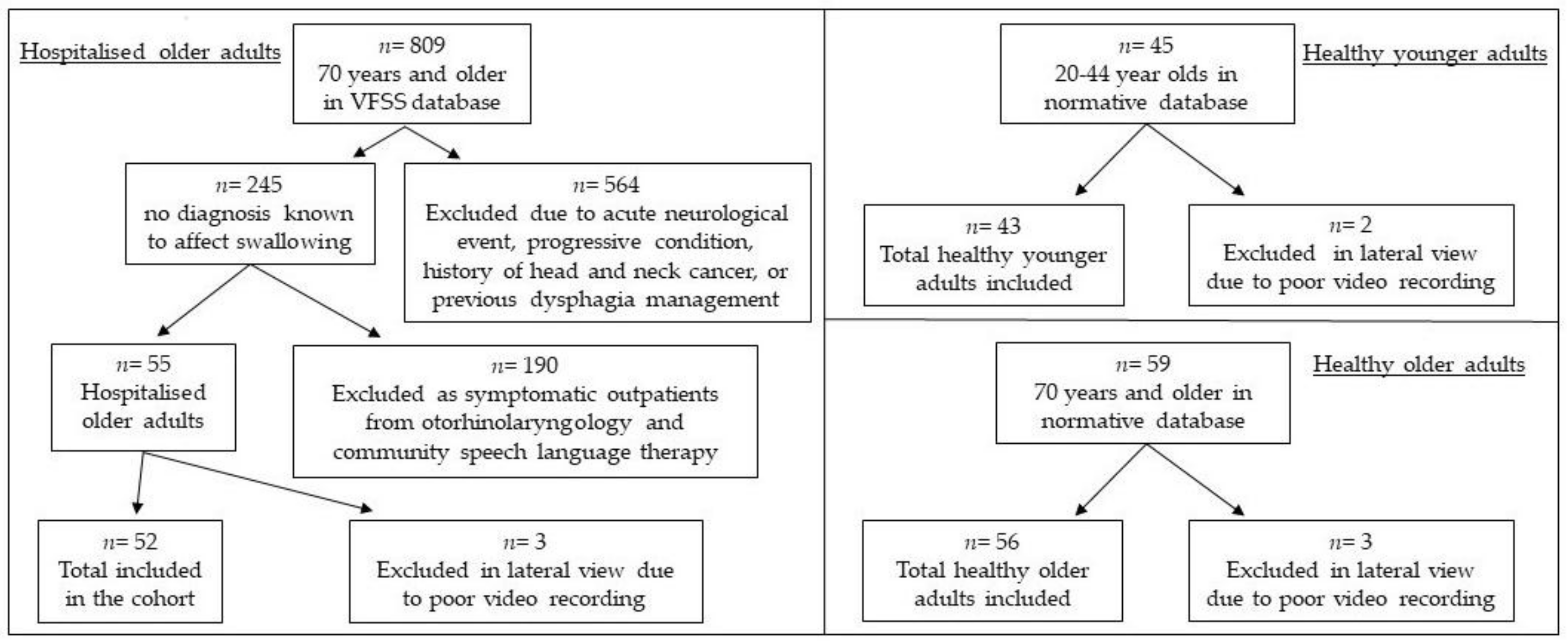
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Analysis
3. Results
3.1. Quantitative Swallowing Measures
3.2. Subjective Ratings
3.2.1. Penetration-Aspiration Scale
3.2.2. Number of Swallows Per 20 mL Bolus
3.3. Length of Stay
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Von Faber, M.; Bootsma–van der Wiel, A.; van Exel, E.; Gussekloo, J.; Lagaay, A.M.; van Dongen, E.; Westendorp, R.G. Successful aging in the oldest old: Who can be characterized as successfully aged? Arch. Intern. Med. 2001, 161, 2694–2700. [Google Scholar] [CrossRef] [PubMed]
- Roy, N.; Stemple, J.; Merrill, R.M.; Thomas, L. Dysphagia in the elderly: Preliminary evidence of prevalence, risk factors, and socioemotional effects. Ann. Otol. Rhinol. Laryngol. 2007, 116, 858–865. [Google Scholar] [CrossRef] [PubMed]
- Eglseer, D.; Halfens, R.J.G.; Schols, J.; Lohrmann, C. Dysphagia in hospitalized older patients: Associated factors and nutritional interventions. J. Nutr. Health Aging 2018, 22, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Kaplan, D. Aspiration pneumonia and dysphagia in the elderly. Chest 2003, 124, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Liesirova, K.; Broeg-Morvay, A.; Meisterernst, J.; Schlager, M.; Mono, M.-L.; Kägi, G.; El-Koussy, M.; Jung, S.; Sarikaya, H. Dysphagia in acute stroke: Incidence, burden and impact on clinical outcome. PLoS ONE 2016, 11, e0148424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howle, A.A.; Baguley, I.J.; Brown, L. Management of dysphagia following traumatic brain injury. Curr. Phys. Med. Rehabil. Rep. 2014, 2, 219–230. [Google Scholar] [CrossRef]
- Kalf, J.G.; De Swart, B.J.M.; Bloem, B.R.; Munneke, M. Prevalence of oropharyngeal dysphagia in Parkinson’s disease: A meta-analysis. Park. Relat. Disord. 2012, 18, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Langmore, S.E.; Olney, R.K.; Lomen-Hoerth, C.; Miller, B.L. Dysphagia in patients with frontotemporal lobar dementia. Arch. Neurol. 2007, 64, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Robbins, J. Swallowing in ALS and motor neuron disorders. Neurol. Clin. 1987, 5, 213–229. [Google Scholar] [CrossRef]
- Lazarus, C.L.; Logemann, J.A.; Pauloski, B.R.; Colangelo, L.A.; Kahrilas, P.J.; Mittal, B.B.; Pierce, M. Swallowing disorders in head and neck cancer patients treated with radiotherapy and adjuvant chemotherapy. Laryngoscope 1996, 106, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Leonard, R.J.; Kendall, K.A.; McKenzie, S.; Gonçalves, M.I.; Walker, A. Structural displacements in normal swallowing: A videofluoroscopic study. Dysphagia 2000, 15, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Peyron, M.-A.; Woda, A.; Bourdiol, P.; Hennequin, M. Age-related changes in mastication. J. Oral. Rehabil. 2017, 44, 299–312. [Google Scholar] [CrossRef] [PubMed]
- Namasivayam-MacDonald, A.M.; Barbon, C.E.A.; Steele, C.M. A review of swallow timing in the elderly. Physiol. Behav. 2018, 184, 12–26. [Google Scholar] [CrossRef] [PubMed]
- Leonard, R.; Kendall, K. Dysphagia Assessment and Treatment Planning: A Team Approach, 4th ed.; Plural Publishing: San Diego, CA, USA, 2018. [Google Scholar]
- Bales, C.W.; Ritchie, C.S. Sarcopenia, weight loss, and nutritional frailty in the elderly. Annu. Rev. Nutr. 2002, 22, 309–323. [Google Scholar] [CrossRef] [PubMed]
- Leder, S.B.; Suiter, D.M.; Agogo, G.O.; Cooney, L.M. An epidemiologic study on ageing and dysphagia in the acute care geriatric-hospitalized population: A replication and continuation study. Dysphagia 2016, 31, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Belafsky, P.C.; Mouadeb, D.A.; Rees, C.J.; Pryor, J.C.; Postma, G.N.; Allen, J.; Leonard, R.J. Validity and reliability of the Eating Assessment Tool (EAT-10). Ann. Otol. Rhinol. Laryngol. 2008, 117, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, H.; Yoshimura, Y.; Ishizaki, N.; Ueno, T. Dysphagia is associated with functional decline during acute-care hospitalization of older patients. Geriatr. Gerontol. Int. 2017, 17, 1610–1616. [Google Scholar] [PubMed]
- English, K.L.; Paddon-Jones, D. Protecting muscle mass and function in older adults during bed rest. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 34–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalisch, B.J.; Lee, S.; Dabney, B.W. Outcomes of inpatient mobilization: A literature review. J. Clin. Nurs. 2014, 23, 1486–1501. [Google Scholar] [CrossRef] [PubMed]
- Young, H.M. Challenges and solutions for care of frail older adults. Online J. Issues Nurs. 2003, 8, 5. [Google Scholar] [PubMed]
- Sanchez-Garcia, S.; García-Peña, C.; Salvà, A.; Sánchez-Arenas, R.; Granados-Garcia, V.; Cuadros-Moreno, J.; Velázquez-Olmedo, L.B.; Cárdenas-Bahena, Á. Frailty in community-dwelling older adults: Association with adverse outcomes. Clin. Interv. Aging 2017, 12, 1003–1011. [Google Scholar] [CrossRef] [PubMed]
- Chong, E.; Ho, E.; Baldevarona-Llego, J.; Chan, M.; Wu, L.; Tay, L.; Ding, Y.Y.; Lim, W.S. Frailty in hospitalized older adults: Comparing different frailty measures in predicting short-and long-term patient outcomes. J. Am. Med. Dir. Assoc. 2018, 19, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Levers, M.; Estabrooks, C.A.; Ross Kerr, J.C. Factors contributing to frailty: Literature review. J. Adv. Nurs. 2006, 56, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Incalzi, R.A.; Capparella, O.; Gemma, A.; Landi, F.; Bruno, E.; Di Meo, F.; Carbonin, P. The interaction between age and comorbidity contributes to predicting the mortality of geriatric patients in the acute-care hospital. J. Intern Med. 1997, 242, 291–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crary, M.A.; Mann, G.D.C.; Groher, M.E. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch. Phys. Med. Rehabil. 2005, 86, 1516–1520. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, R.C.; Rose, S.S.; Roe, J.W.G.; Khan, A.S.; Pepper, C.; Nutting, C.M.; Clarke, P.M.; Kerawala, C.J.; Rhys-Evans, P.H.; Harrington, K.J. Validation of the Sydney Swallow Questionnaire (SSQ) in a cohort of head and neck cancer patients. Oral. Oncol. 2010, 46, e10–14. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, M.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M. Validation of the Mini Nutritional Assessment Short-Form (MNA®-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Rosenbek, J.C.; Robbins, J.A.; Roecker, E.B.; Coyle, J.L.; Wood, J.L. A penetration-aspiration scale. Dysphagia 1996, 11, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Leonard, R. Two methods for quantifying pharyngeal residue on fluoroscopic swallow studies: Reliability assessment. Ann. Otolaryngol. Rhinol. 2017, 4, 1168. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics; Sage Publications: London, UK, 2018. [Google Scholar]
- Hinds, N.P; Wiles, C.M. Assessment of swallowing and referral to speech and language therapists in acute stroke. QJM Mon J. Assoc Physicians 1998, 91, 829–835. [Google Scholar] [CrossRef] [Green Version]
- Laan, D.V.; Pandian, T.K; Jenkins, D.H.; Kim, B.D.; Morris, D.S. Swallowing dysfunction in elderly trauma patients. J. Crit. Care 2017, 42, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Hvid, L.G.; Suetta, C.; Nielsen, J.H.; Jensen, M.M.; Frandsen, U.; Ørtenblad, N.; Kjaer, M.; Aagaard, P. Aging impairs the recovery in mechanical muscle function following 4 days of disuse. Exp. Gerontol. 2014, 52, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kortebein, P.; Symons, T.B.; Ferrando, A.; Paddon-Jones, D.; Ronsen, O.; Protas, E.; Conger, S.; Lombeida, J.; Wolfe, R.; Evans, W.J. Functional impact of 10 days of bed rest in healthy older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 1076–1081. [Google Scholar] [CrossRef]
- Maeda, K.; Koga, T.; Akagi, J. Tentative nil per os leads to poor outcomes in older adults with aspiration pneumonia. Clin. Nutr. 2016, 35, 1147–1152. [Google Scholar] [CrossRef] [PubMed]
- Popman, A.; Richter, M.; Allen, J.; Wham, C. High nutrition risk is associated with higher risk of dysphagia in advanced age adults newly admitted to hospital. Nutr. Diet. 2018, 75, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Leonard, R.; Belafsky, P.C.; Rees, C.J. Relationship between fluoroscopic and manometric measures of pharyngeal constriction: The pharyngeal constriction ratio. Ann. Otol. Rhinol. Laryngol. 2006, 115, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Stokely, S.L.; Peladeau-Pigeon, M.; Leigh, C.; Molfenter, S.M.; Steele, C.M. The relationship between pharyngeal constriction and post-swallow residue. Dysphagia 2015, 30, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Molfenter, S.M.; Amin, M.R.; Branski, R.C.; Brumm, J.D.; Hagiwara, M.; Roof, S.A.; Lazarus, C.L. Age-Related Changes in Pharyngeal Lumen Size: A Retrospective MRI Analysis. Dysphagia 2015, 30, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Molfenter, S.M.; Lenell, C.; Lazarus, C.L. Volumetric Changes to the Pharynx in Healthy Aging: Consequence for Pharyngeal Swallow Mechanics and Function. Dysphagia 2018, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Miles, A.; Clark, S.; Jardine, M.; Allen, J. Esophageal Swallowing Timing Measures in Healthy Adults during Videofluoroscopy. Ann. Otol. Rhinol. Laryngol. 2016, 125, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Kendall, K.A.; Leonard, R.J.; McKenzie, S. Common medical conditions in the elderly: Impact on pharyngeal bolus transit. Dysphagia 2004, 19, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Roos, M.R.; Rice, C.L.; Vandervoort, A.A. Age-related changes in motor unit function. Muscle Nerve 1997, 20, 679–690. [Google Scholar] [CrossRef]
- Im, I.; Kim, Y.; Oommen, E.; Kim, H.; Ko, M.H. The effects of bolus consistency in pharyngeal transit duration during normal swallowing. Ann. Rehabil. Med. 2012, 36, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Leonard, R. Swallowing in the Elderly: Evidence From Fluoroscopy. Perspect Swallowing Disord. 2010, 19, 103–114. [Google Scholar] [CrossRef]
- Covinsky, K.E.; Palmer, R.M.; Fortinsky, R.H.; Counsell, S.R.; Stewart, A.L.; Kresevic, D.; Burant, C.J.; Landefeld, C.S. Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: Increased vulnerability with age. J. Am. Geriatr. Soc. 2003, 51, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Hogan, D.B; Maxwell, C.J; Afilalo, J.; Arora, R.C; Bagshaw, S.M; Basran, J.; Bergman, H.; Bronskill, S.E.; Dixon, E.; Hemmelgarn, B.; et al. A scoping review of frailty and acute care in middle-aged and older individuals with recommendations for future research. Can. Geriatr. J. 2017, 20, 22–37. [Google Scholar] [CrossRef] [PubMed]
- Stål, P.; Marklund, S.; Thornell, L.-E.; De Paul, R.; Eriksson, P.-O. Fibre composition of human intrinsic tongue muscles. Cells Tissues Organs 2003, 173, 147–161. [Google Scholar] [CrossRef] [PubMed]
- Brummel, N.E.; Balas, M.C.; Morandi, A.; Ferrante, L.E.; Gill, T.M.; Ely, E.W. Understanding and reducing disability in older adults following critical illness. Crit. Care Med. 2015, 43, 1265–1275. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, K. Optimizing reserve in hospitalized elderly. Crit. Care Nurs. Clin. N. Am. 2007, 19, 285–302. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Measure | Description |
|---|---|
| Timing (sec) | |
| Hdur | Duration of maximum hyoid displacement |
| PESop | Pharyngoesophageal segment (PES) opening duration |
| Airwaycl | Onset and completion of supraglottic closure |
| Airwaydur | Duration of airway closure |
| BP1AEcl | Time from airway closure to bolus entering PES |
| TPT | Onset of swallow (first movement past the posterior nasal spine) to clearance of the bolus tail through the PES: total pharyngeal transit time. |
| ETT | Entrance of the bolus through the PES to clearance through the lower esophageal sphincter (LES): esophageal transit time |
| Displacement (cm) | |
| PESmax | The maximum distension of the PES |
| Hmax | Change in hyoid position from rest to maximum anterior-posterior displacement |
| HLmax | Difference in distance between hyoid and larynx at rest and when maximally approximated during swallow |
| Area (cm2) | |
| PAhold | Area of pharynx at rest |
| Ratio (area:area) | |
| PCR | Pharyngeal constriction ratio: pharyngeal area of maximum constriction/ open pharyngeal area |
| BCR | Bolus clearance ratio: bolus residual/ area of bolus prior to PES opening |
| n | Healthy Younger Adults | Healthy Older Adults | Hospitalized Older Adults | p-Value | |
|---|---|---|---|---|---|
| 43 | 56 | 52 | |||
| Age (years) | M, SD Range | 30.84, 7.71 20–44 | 81.20, 8.18 70–99 | 84.73, 7.02 71–100 | <0.001 |
| Sex n (%) | Female Male | 24 (55.8%) 19 (44.2%) | 35 (62.5%) 21 (37.5%) | 18 (34.6%) 34 (65.4%) | 0.011 |
| Ethnicity n (%) | NZ Māori NZ European Other | 4 (9.3%) 24 (55.8%) 15 (34.9%) | 1 (1.8%) 49 (87.5%) 6 (10.7%) | 1 (1.9%) 42 (80.8%) 9 (17.3%) | 0.004 |
| Residence n (%) | Independent Rest home | 43 (100%) 0 | 45 (80.4%) 11 (19.6%) | 46 (88.5%) 6 (11.5%) | 0.009 |
| Mdn | IQR | Spread | |
|---|---|---|---|
| Comorbidities | 9 | 5 | 1–20 |
| Medications | 10 | 6 | 2–19 |
| Days admitted until VFSS | 15 | 25 | 2–75 |
| Length of stay (days) | 21 | 47 | 3–135 |
| n (%) | |||
| Reason for admission | Medical 33 (63.5%) Surgical 19 (36.5%) | ||
| ETT documented 1 | Yes 35 (67.3%) No 17 (32.7%) | ||
| Nutrition documented 2 | Yes 16 (32.7%) No 36 (67.3%) | ||
| Mortality since VFSS | <2 months 10 (19.2%) 2–6 months 8 (15.4%) 6–12 months 1 (1.9%) 2–3 years 4 (7.7%) Living 23 (44.2%) | ||
| Measure 1 | Healthy Younger Adults | Healthy Older Adults | Hospitalized Older Adults | p-Value | |||
|---|---|---|---|---|---|---|---|
| Mdn | IQR | Mdn | IQR | Mdn | IQR | ||
| Hdur | 0.30 | 0.19 | 0.27 | 0.15 | 0.33 | 0.17 | 0.291 |
| PESop 2 | 0.60 | 0.07 | 0.62 | 0.11 | 0.61 | 0.17 | 0.732 |
| Airwaycl | 0.20 | 0.30 | 0.27 | 0.30 | 0.30 | 0.53 | 0.028 |
| Airwaydur | 0.80 | 0.22 | 0.87 | 0.37 | 0.80 | 0.47 | 0.221 |
| BP1AEcl | −0.07 | 0.07 | −0.15 | 0.23 | −0.07 | 0.30 | <0.001 |
| TPT | 0.77 | 0.13 | 0.90 | 0.23 | 1.00 | 0.60 | <0.001 |
| ETT | 5.58 | 4.18 | 7.97 | 11.02 | 10.58 | 11.33 | <0.001 |
| PESmax 2 | 0.78 | 0.15 | 0.77 | 0.19 | 0.72 | 0.21 | 0.384 |
| Hmax | 1.81 | 0.47 | 1.86 | 0.75 | 1.53 | 0.51 | 0.023 |
| HLmax | 0.94 | 0.31 | 0.63 | 0.27 | 1.07 | 1.00 | <0.001 |
| Pahold2 | 11.28 | 3.07 | 11.45 | 2.51 | 14.35 | 3.12 | <0.001 |
| PCR | 0.01 | 0.00 | 0.02 | 0.02 | 0.06 | 0.06 | <0.001 |
| BCR | 0.00 | 0.00 | 0.00 | 0.00 | 0.054 | 0.07 | <0.001 |
| Healthy Younger Adults | Healthy Older Adults | Healthy Younger Adults | ||||||
|---|---|---|---|---|---|---|---|---|
| Hospitalized older adults | Measure 1 | p | r | P | r | Healthy older adults | p | r |
| Airwaycl | 0.026 * | 0.22 | 1 | 0.02 | 0.167 | 0.16 | ||
| BP1AEcl | 1 | 0.02 | 0.004 * | 0.26 | 0.011 * | 0.24 | ||
| TPT | <0.001 * | 0.45 | 0.120 | 0.17 | 0.001 * | 0.30 | ||
| ETT | <0.001 * | 0.38 | 0.158 | 0.17 | 0.013 * | 0.24 | ||
| Hmax | 0.198 | 0.15 | 0.023 * | 0.22 | 1 | 0.06 | ||
| HLmax | 0.410 | 0.12 | <0.001 * | 0.47 | <0.001 * | 0.32 | ||
| PAhold | <0.001 * | - | <0.001 * | - | 1 | - | ||
| PCR | <0.001 * | 0.48 | <0.001 * | 0.50 | 1 | 0.02 | ||
| BCR | <0.001 * | 0.61 | <0.001 * | 0.76 | 0.627 | 0.11 | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jardine, M.; Miles, A.; Allen, J. Dysphagia Onset in Older Adults during Unrelated Hospital Admission: Quantitative Videofluoroscopic Measures. Geriatrics 2018, 3, 66. https://doi.org/10.3390/geriatrics3040066
Jardine M, Miles A, Allen J. Dysphagia Onset in Older Adults during Unrelated Hospital Admission: Quantitative Videofluoroscopic Measures. Geriatrics. 2018; 3(4):66. https://doi.org/10.3390/geriatrics3040066
Chicago/Turabian StyleJardine, Marie, Anna Miles, and Jacqui Allen. 2018. "Dysphagia Onset in Older Adults during Unrelated Hospital Admission: Quantitative Videofluoroscopic Measures" Geriatrics 3, no. 4: 66. https://doi.org/10.3390/geriatrics3040066
APA StyleJardine, M., Miles, A., & Allen, J. (2018). Dysphagia Onset in Older Adults during Unrelated Hospital Admission: Quantitative Videofluoroscopic Measures. Geriatrics, 3(4), 66. https://doi.org/10.3390/geriatrics3040066