Effects of Walking on Coronary Heart Disease in Elderly Men with Diabetes

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Thompson, P.D.; Buchner, D.; Pina, I.L.; Balady, G.J.; Williams, M.A.; Marcus, B.H.; Berra, K.; Blair, S.N.; Costa, F.; Franklin, B.; et al. American Heart Association Council on Clinical Cardiology Subcommittee on Exercise, Rehabilitation and Prevention; American Heart Association Council on Nutrition, Physical Activity and Metabolism Subcommittee on Physical Activity. Circulation 2003, 107, e9053–e9054. [Google Scholar] [CrossRef] [PubMed]
- Press, V.; Freestone, I.; George, C.F. Physical activity: The evidence of benefit in the prevention of coronary heart disease. QJM 2003, 96, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B.; Sorlie, P. Some health benefits of physical activity. Arch. Intern. Med. 1979, 139, 857–861. [Google Scholar] [CrossRef] [PubMed]
- Hakim, A.A.; Curb, J.D.; Petrovitch, H.; Rodriguez, B.L.; Yano, K.; Ross, G.W.; White, L.R.; Abbott, R.D. Effects of walking on Coronary Heart disease in elderly men: The Honolulu Heart Program. Circulation 1999, 100, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A. Effects of daily exercise on blood pressure, plasma glucose and obesity measures in 55–64-year-old obese Asia Indian men: The Calcutta longitudinal study. Am. J. Hum. Biol. 2006, 18, 718–721. [Google Scholar] [CrossRef] [PubMed]
- Chimen, M.; Kennedy, A.; Nirantharakumar, K.; Pang, T.T.; Andrews, R.; Narendran, P. What are the health benefits of physical activity in type 1 diabetes mellitus? A literature review. Diabetologia 2012, 55, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B. Exercise and type 2 diabetes: American college of sports medicine and the American diabetes association: Joint position statement. Med. Sci. Sport Exerc. 2010, 42, 2282–2303. [Google Scholar]
- Najafipour, F.; Mobasseri, M.; Yavari, A.; Nadrian, H.; Aliasgarzadeh, A.; Mashinchi Abbasi, N.; Niafar, M.; Houshyar Gharamaleki, J.; Sadra, V. Effect of regular exercise training on changes in HbA1c, BMI and VO(2)max among patients with type 2 diabetes mellitus: An 8-year trial. BMJ Open Diabetes Res. Care 2017, 5, e000414. [Google Scholar] [CrossRef]
- Paffenbarger, R.S.; Hyde, R.T.; Wing, A.L.; Lee, I.; Jung, D.L.; Kampert, J.B. The association of changes in physical-activity level and other lifestyle characteristics with mortality among men. N. Engl. J. Med. 1993, 328, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Gregg, E.W.; Gerzoff, R.B.; Caspersen, C.J.; Williamson, D.F.; Narayan, K.M. Relationship of walking to mortality among US adults with diabetes. Arch. Intern. Med. 2003, 163, 1440–1447. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, B.L.; Abbott, R.D.; Fujimoto, W.; Waitzfelder, B.; Chen, R.; Masaki, K.; Schatz, I.; Petrovitch, H.; Ross, W.; Yano, K.; et al. The American Diabetes Association and World Health Organization classifications for diabetes: Their impact on diabetes prevalence and total and cardiovascular disease mortality in elderly Japanese-American men. Diabetes Care 2002, 25, 951–955. [Google Scholar] [CrossRef]
- Rodriguez, B.L.; Curb, J.D.; Burchfiel, C.M.; Huang, B.; Sharp, D.S.; Lu, G.Y.; Fujimoto, W.; Yano, K. Impaired glucose tolerance, diabetes and cardiovascular disease risk factor profiles in the elderly: The Honolulu Heart Program. Diabetes Care 1996, 19, 587–590. [Google Scholar] [CrossRef] [PubMed]
- Yano, K.; Reed, D.M.; McGee, D.L. Ten-year incidence of coronary heart disease in the Honolulu Heart Program: Relationship to biologic and lifestyle characteristics. Am. J. Epidemiol. 1984, 119, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Hakim, A.A.; Petrovitch, H.; Burchfiel, C.M.; Ross, G.W.; Rodriguez, B.L.; White, L.R.; Yano, K.; Curb, J.D.; Abbott, R.D. Effects of walking on mortality among nonsmoking retired men. N. Engl. J. Med. 1998, 338, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, B.L.; Lau, N.; Burchfiel, C.M.; Abbott, R.D.; Sharp, D.S.; Yano, K.; Curb, J.D. Glucose intolerance and 23-year risk of coronary heart disease and total mortality. Diabetes Care 1999, 22, 1262–1265. [Google Scholar] [CrossRef] [PubMed]
- Abbott, R.D.; White, L.R.; Ross, G.W.; Masaki, K.H.; Curb, J.D.; Petrovitch, H. Walking and dementia in physically capable elderly men. JAMA 2004, 292, 1447–1453. [Google Scholar] [CrossRef]
- Lane, P.W.; Nelder, J.A. Analysis of covariance and standardization as instances of prediction. Biometrics 1982, 38, 613–621. [Google Scholar] [CrossRef]
- Burchfiel, C.M.; Abbott, R.D.; Sharp, D.S.; Curb, J.D.; Rodriguez, B.L.; Yano, K. Distribution and correlates of lipids and lipoproteins in elderly Japanese-American men: The Honolulu Heart Program. Arterioscler. Thromb. Vasc. Biol. 1996, 16, 1356–1364. [Google Scholar] [CrossRef] [PubMed]
- Burchfiel, C.M.; Curb, J.D.; Sharp, D.S.; Rodriguez, B.L.; Arakaki, R.; Chyou, P.H.; Yano, K. Distribution and correlates of insulin in elderly men. The Honolulu Heart Program. Arterioscler. Thromb. Vasc. Biol. 1995, 15, 2213–2221. [Google Scholar] [CrossRef]
- Rhoads, G.G.; Kagan, A.; Yano, K. Usefulness of community surveillance for the ascertainment of coronary heart disease and stroke. Int. J. Epidemiol. 1975, 4, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Puthoff, M.L.; Janz, K.F.; Nielson, D. The relationship between lower extremity strength and power to everyday walking behaviors in older adults with functional limitations. J. Geriatr. Phys. Ther. 2008, 31, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.C.; Pate, R.R.; Lavie, C.J.; Sui, X.; Church, T.S.; Blair, S.N. Leisure-time running reduces all-cause and cardiovascular mortality risk. J. Am. Coll. Cardiol. 2014, 64, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Grøntved, A.; Koivula, R.W.; Johansson, I.; Wennberg, P.; Østergaard, L.; Hallmans, G.; Renström, F.; Franks, P.W. Bicycling to Work and Primordial Prevention of Cardiovascular Risk: A Cohort Study Among Swedish Men and Women. J. Am. Heart Assoc. 2016, 5, e004413. [Google Scholar] [CrossRef] [PubMed]
- Nualnim, N.; Parkhurst, K.; Dhindsa, M.; Tarumi, T.; Vavrek, J.; Tanaka, H. Effects of swimming training on blood pressure and vascular function in adults >50 years of age. Am. J. Cardiol. 2012, 109, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Nualnim, N.; Barnes, J.N.; Tarumi, T.; Renzi, C.P.; Tanaka, H. Comparison of central artery elasticity in swimmers, runners and the sedentary. Am. J. Cardiol. 2011, 107, 783–787. [Google Scholar] [CrossRef]
- Rodriguez, B.L.; D’Agostino, R.; Abbott, R.D.; Kagan, A.; Burchfiel, C.M.; Yano, K.; Ross, G.W.; Silbershatz, H.; Higgins, M.W.; Popper, J.; et al. Risk of hospitalized stroke in men enrolled in the Honolulu Heart Program and the Framingham Study: A comparison of incidence and risk factor effects. Stroke 2002, 33, 230–237. [Google Scholar] [CrossRef]
- Yano, K.; Reed, D.; Kagan, A. Coronary heart disease and stroke among Japanese-American men in Hawaii: The Honolulu Heart Program. Hawaii Med. J. 1985, 44, 297–300. [Google Scholar] [PubMed]
- Weuve, J.; Kang, J.H.; Manson, J.E.; Breteler, M.M.B.; Ware, J.H.; Grodstein, F. Physical activity, including walking and cognitive function in older women. JAMA 2004, 292, 1454–1461. [Google Scholar] [CrossRef] [PubMed]
- Petrovitch, H.; Ross, G.W.; Abbott, R.D.; Sanderson, W.T.; Sharp, D.S.; Tanner, C.M.; Masaki, K.H.; Blanchette, P.L.; Popper, J.S.; Foley, D.; et al. Plantation work and risk of Parkinson disease in a population-based longitudinal study. Arch. Neurol. 2002, 59, 1787–1792. [Google Scholar] [CrossRef] [PubMed]
- Ascherio, A.; Chen, H.; Weisskopf, M.G.; O’Reilly, E.; McCullough, M.L.; Calle, E.E.; Schwarzschild, M.A.; Thun, M.J. Pesticide exposure and risk for Parkinson’s disease. Ann. Neurol. 2006, 60, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.C.; Wingard, D.L.; Smith, B.; Kritz-Silverstein, D.; Barrett-Connor, E. Walking decreased risk of cardiovascular disease mortality in older adults with diabetes. J. Clin. Epidemiol. 2007, 60, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Stampfer, M.J.; Solomon, C.; Liu, S.; Colditz, G.A.; Speizer, F.E.; Willett, W.C.; Manson, J.E. Physical activity and risk for cardiovascular events in diabetic women. Ann. Intern. Med. 2001, 134, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Lakka, T.A.; Laaksonen, D.E. Physical activity in prevention and treatment of the metabolic syndrome. Appl. Physiol. Nutr. Metab. 2007, 32, 76–88. [Google Scholar] [CrossRef]
- Hilberg, T. Physical activity in the prevention of cardiovascular diseases. Epidemiol. Mech. Hamostaseol. 2008, 28, 9–15. [Google Scholar]
- Rodriguez, B.L.; Curb, J.D.; Burchfiel, C.M.; Abbott, R.D.; Petrovitch, H.; Masaki, K.; Chiu, D. Physical activity and 23-year incidence of coronary heart disease morbidity and mortality among middle-aged men. The Honolulu Heart Program. Circulation 1994, 89, 2540–2544. [Google Scholar] [CrossRef] [PubMed]
- Temple, B.; Janzen, B.L.; Chad, K.; Bell, G.; Reeder, B.; Martin, L. The health benefits of a physical activity program for older adults living in congregate housing. Can. J. Public Health 2008, 99, 36–40. [Google Scholar] [PubMed]
- Sardu, C.; Marfella, R.; Santulli, G. Impact of diabetes mellitus on the clinical response to cardiac resynchronization therapy in elderly people. J. Cardiovasc. Transl. Res. 2014, 7, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Cardona, S.; Pasquel, F.J.; Fayfman, M.; Peng, L.; Jacobs, S.; Vellanki, P.; Weaver, J.; Halkos, M.; Guyton, R.A.; Thourani, V.H.; et al. Hospitalization costs and clinical outcomes in CABG patients treated with intensive insulin therapy. J. Diabetes Complicat. 2017, 31, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Gregg, E.W.; Beckles, G.L.; Williamson, D.F.; Leveille, S.G.; Langlois, J.A.; Engelgau, M.M.; Narayan, K.M. Diabetes and physical disability among older U.S. adults. Diabetes Care 2000, 23, 1272–1277. [Google Scholar] [CrossRef]
- Kalyani, R.R.; Rodriguez, D.C.; Yeh, H.C.; Golden, S.H.; Thorpe, R.J., Jr. Diabetes, race and functional limitations in older U.S. men and women. Diabetes Res. Clin. Pract. 2015, 108, 390–397. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bardenheier, B.H.; Gregg, E.W.; Zhuo, X.; Cheng, Y.J.; Geiss, L.S. Association of functional decline with subsequent diabetes incidence in U.S. adults aged 51 years and older: The Health and Retirement Study 1998–2010. Diabetes Care 2014, 37, 1032–1038. [Google Scholar] [CrossRef][Green Version]
- McGuire, L.C.; Ford, E.S.; Ajani, U.A. The impact of cognitive functioning on mortality and the development of functional disability in older adults with diabetes: The second longitudinal study on aging. BMC Geriatr. 2006, 6, 8. [Google Scholar] [CrossRef]


{kind=link}
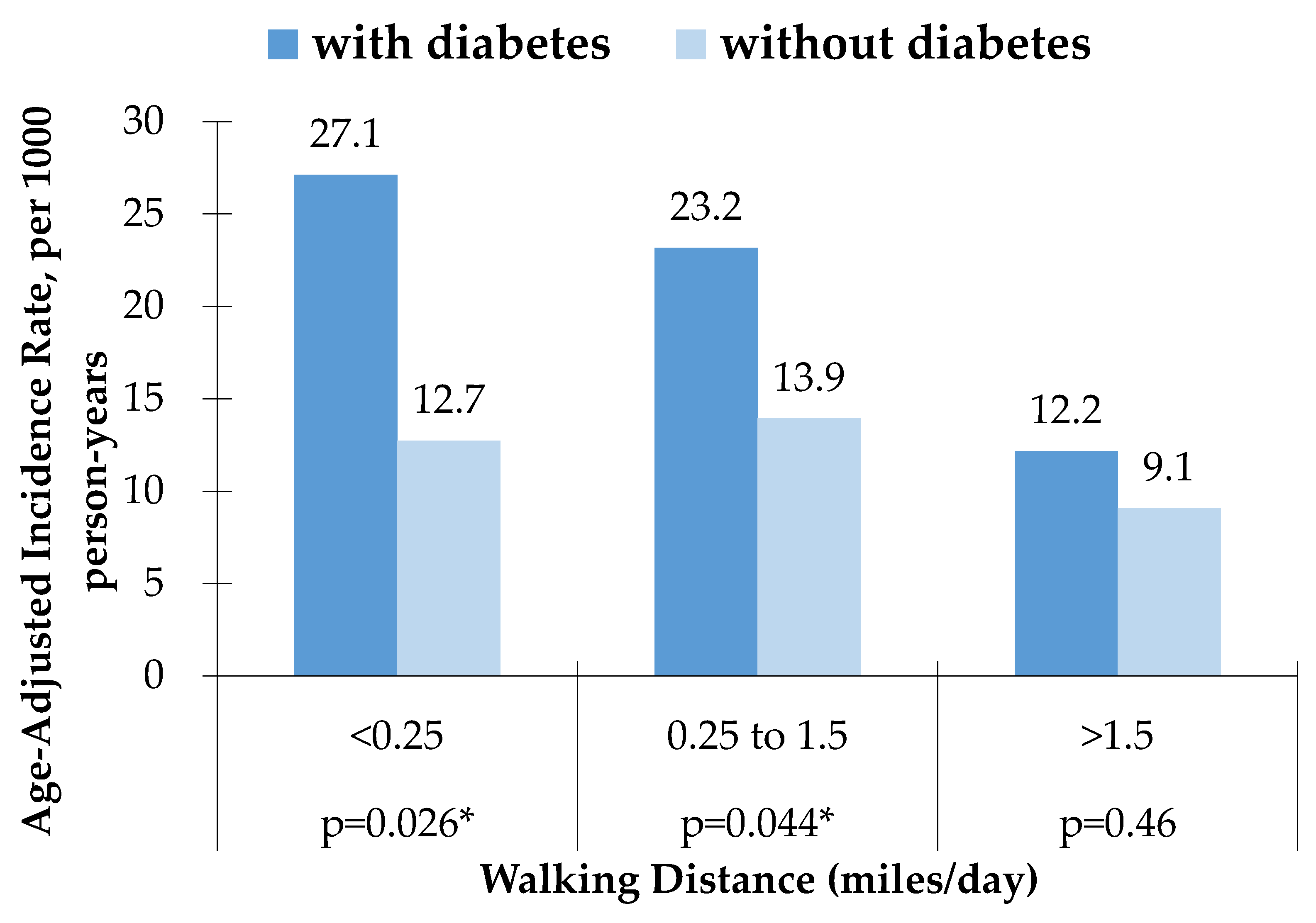
| Walking Distance, miles/day | Number of Subjects (%) | Number of Events (%) | Age-Adjusted Incidence Rate, per 1000 Person-Years (95% CI) | |||
|---|---|---|---|---|---|---|
| With Diabetes | Without Diabetes | With Diabetes | Without Diabetes | With Diabetes | Without Diabetes | |
| <0.25 | 161 (30) | 633 (30) | 23 (38) | 44 (30) | 27.1 (24.6–29.6) * | 12.7 (11.6–13.9) * |
| 0.25 to 1.5 | 220 (41) | 831(39) | 27 (44) | 69 (46) | 23.2 (21.2–25.1) * | 13.9 (12.3–15.0) * |
| >1.5 | 157 (29) | 645 (31) | 11(18) | 36 (24) | 12.2 (4.7–19.6) | 9.1 (6.0–12.0) |
| Baseline (1991–1993) Risk Factor | Walking Distance, miles/day | |||||
|---|---|---|---|---|---|---|
| <0.25 miles/day | 0.25 to 1.5 miles/day | >1.5 miles/day | ||||
| With Diabetes | Without Diabetes | With Diabetes | Without Diabetes | With Diabetes | Without Diabetes | |
| Age | 77.4 (4.6) | 77.60 (4.3) ‡ | 77.2 (3.9) † | 77.6 (4.3) § | 76.2 (3.5) | 76.6 (3.9) |
| BMI | 24.0 (3.4) | 23.2 (3.3) | 23.8 (3.3) | 23.3 (3.0) | 24.1 (2.8) | 23.5 (2.9) |
| Fasting glucose, mg/dL | 144.9 (42.1) | 103.0 (9.1) | 145.5 (45.2) | 102.7 (8.4) | 146.9 (45.4) | 103.5 (8.6) |
| Total cholesterol, mg/dL | 190.4 (190.4) | 191.5 (34.2) | 190.6 (34.9) | 190.4 (31.8) | 193.5 (32.4) | 194.8 (31.4) |
| HDL cholesterol, mg/dL | 48.3 (11.0) | 53.3 (13.8) | 49.2 (14.9) | 52.1 (13.6) | 48.6 (12.4) | 52.6 (12.8) |
| SBP, mmHg | 153.0 (24.5) | 148.9 (23.2) † | 151.3 (22.7) | 149.4 (22.0) | 154.6 (23.7) | 150.9 (22.4) |
| Current smoker, % | 7.8 † | 11.3 ‡ | 5.90 | 7.30 | 2.50 | 5.40 |
| Alcohol intake, oz/month | 21.4 (45.2) | 20.3 (40.1) | 25.1 (57.6) | 20.3 (41.6) | 13.7 (26.0) | 17.1 (33.7) |
| Walking Distance, miles/day | Age-Adjusted Relative Risk (95% CI) | Risk Factor-Adjusted Relative Risk (95% Cl) * | ||
|---|---|---|---|---|
| With Diabetes | Without Diabetes | With Diabetes | Without Diabetes | |
| <0.25 † | 1 | 1 | 1 | 1 |
| 0.25 to 1.5 | 0.77 (0.45–1.32) | 1.07 (0.75–1.54) | 0.81 (0.47–1.41) | 1.16 (0.78–1.72) |
| >1.5 | 0.48 (0.24–0.98) ‡ | 0.70 (0.46–1.07) | 0.45 (0.22–0.93) ‡ | 0.74 (0.47–1.17) |
| test for trend § | p = 0.043 | p = 0.070 | p = 0.025 | p = 0.10 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimata, C.; Willcox, B.; Rodriguez, B.L. Effects of Walking on Coronary Heart Disease in Elderly Men with Diabetes. Geriatrics 2018, 3, 21. https://doi.org/10.3390/geriatrics3020021
Kimata C, Willcox B, Rodriguez BL. Effects of Walking on Coronary Heart Disease in Elderly Men with Diabetes. Geriatrics. 2018; 3(2):21. https://doi.org/10.3390/geriatrics3020021
Chicago/Turabian StyleKimata, Chieko, Bradley Willcox, and Beatriz L. Rodriguez. 2018. "Effects of Walking on Coronary Heart Disease in Elderly Men with Diabetes" Geriatrics 3, no. 2: 21. https://doi.org/10.3390/geriatrics3020021
APA StyleKimata, C., Willcox, B., & Rodriguez, B. L. (2018). Effects of Walking on Coronary Heart Disease in Elderly Men with Diabetes. Geriatrics, 3(2), 21. https://doi.org/10.3390/geriatrics3020021