

Development of an Adult Daycare Center Service Model for the Elderly Through Community Participation: An Action Research Approach


 and
and 
Abstract
1. Introduction
2. Methods
2.1. Population and Sample
- (1)
- Cluster Sampling: the subdistrict was divided into 20 villages to capture geographic and demographic diversity.
- (2)
- Simple Random Sampling: within each village, elderly individuals were randomly selected using a computerized randomization process to minimize selection bias.
2.1.1. Inclusion Criteria
- -
- Elderly individuals aged 60 years and above residing in Ban Kho Subdistrict, Phon Sawan District, Nakhon Phanom Province.
- -
- Permanent residents of the community.
- -
- Individuals with chronic illnesses who are ambulatory and able to participate in activities (e.g., diabetes, hypertension) as identified in the community health survey.
- -
- Socially active elderly individuals.
- -
- Participants who provided informed consent.
- -
- Key community informants, such as elderly club leaders, subdistrict health promotion hospital staff, and village health volunteers.
2.1.2. Exclusion Criteria
- -
- Bedridden or homebound elderly individuals unable to participate in community activities.
- -
- Individuals with severe cognitive impairments (e.g., advanced dementia) that limit engagement in study activities.
- -
- Temporary residents or individuals living outside the study area.
- -
- Participants who declined to give consent or withdrew from the study.
- -
- Individuals facing logistical barriers, such as lack of transportation or caregiver support.
2.1.3. Functional Status Assessment
2.2. Implementation Phases and Quality Control
2.2.1. Phase 1: Planning and Community Engagement
2.2.2. Phase 2: Service Implementation
2.2.3. Phase 3: Monitoring and Evaluation
2.3. Research Tools
2.4. Data Collection and Reliability Concern
- (1)
- Preparation and Validation: The semi-structured interview tool was developed and reviewed by three experts. Feedback was incorporated to ensure content accuracy and appropriateness.
- (2)
- Pilot Testing: pilot interviews were conducted with individuals resembling the study participants to refine the tool and ensure its effectiveness.
- (3)
- Training: The research team received extensive training in qualitative research methodologies and had substantial experience in conducting qualitative studies. This training ensured that the data collected would be reliable and valid.
- (1)
- Credibility: ensuring the data accurately reflected participants’ experiences by involving those with direct experience of the phenomena under investigation.
- (2)
- Transferability: providing rich, detailed descriptions of the findings to enable other researchers to determine the applicability of the results to similar contexts.
- (3)
- Dependability: meticulously documenting the research process to ensure consistent procedures and agreement among the research team.
- (4)
- Conformability: using activity logs and reflective notes to allow verification by other researchers and employing triangulation techniques, which involved cross-checking information from multiple sources and methods, with data reviewed by two independent experts.
2.5. Data Analysis
2.5.1. Data Description
2.5.2. Comparative Analysis
2.5.3. Instrument Reliability
2.6. Project Implementation Financial Considerations
2.6.1. Establishment of the Daycare Center
- (1)
- Planning and Community Engagement: Initial consultations were conducted with stakeholders, including village health volunteers, local administrative officers, elderly club representatives, and healthcare workers. These discussions helped identify the needs of the elderly population and secure community support.
- (2)
- Infrastructure Setup: The project leveraged existing community facilities to minimize construction costs. A multipurpose community building was renovated to accommodate elderly-friendly services, including designated areas for social interaction, recreational activities, and basic healthcare services.
- (3)
- Service Design and Implementation: The daycare center was designed to operate on weekdays, providing health screenings, social engagement programs, cognitive stimulation activities, and nutritional support for elderly participants.
2.6.2. Financial Considerations and Sustainability
- Government Contributions:
- 2.
- Community Fundraising and Private Donations:
- 3.
- Academic and Institutional Partnerships:
2.7. Ethical Considerations
3. Results
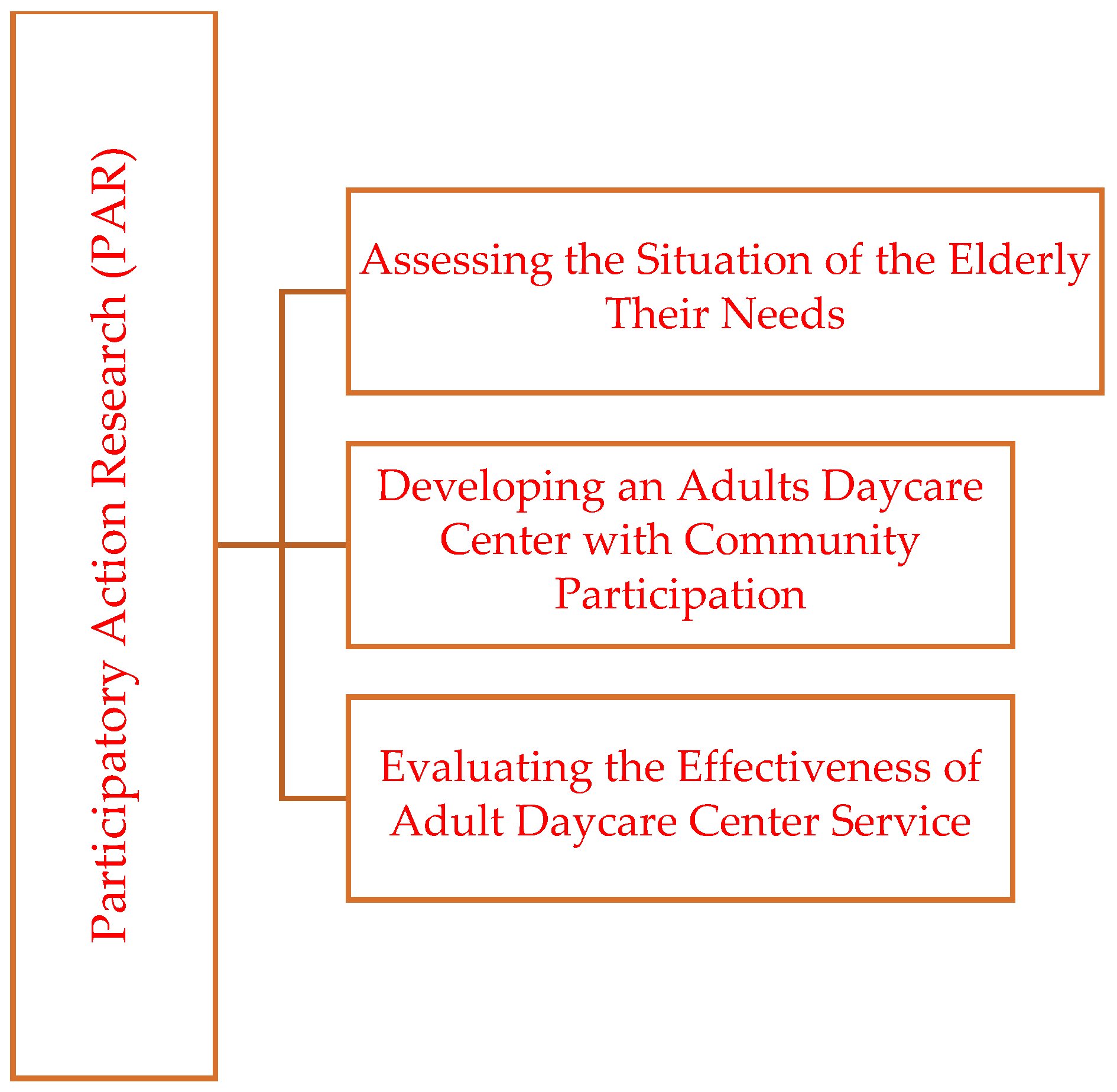
3.1. Phase 1: Investigated the Current Situation and Specific Needs of the Elderly
3.1.1. The Socioeconomic Information and the Specific Needs of the Elderly
3.1.2. The Participants Approaching
- Health: Chronic illnesses, access to healthcare services, and preventive care strategies were identified as primary concerns. Understanding the health needs of the elderly ensures that interventions are tailored to manage chronic diseases and promote active, healthy lifestyles.
- Economic: issues such as financial insecurity, dependency on remittances, and insufficient income were analyzed to highlight the need for sustainable income-generating opportunities and financial support mechanisms.
- Social: Social isolation, familial relationships, and the need for community engagement were explored. Addressing these social dynamics can foster stronger intergenerational bonds and improve the overall social well-being of elderly individuals.
- Environmental: The accessibility and safety of physical environments, both in public spaces and at home, were examined. Enhancing infrastructure to support mobility and safety is crucial for ensuring the elderly’s independence and active participation in their communities.
3.1.3. Role of Community Leaders in Assisting the Elderly
3.1.4. Role of the Elderly in Community Engagement
3.1.5. Services Required in a Daycare Center for the Elderly
- (1)
- Facility Requirements: The physical environment of a daycare center should prioritize accessibility and safety to accommodate the mobility challenges often faced by the elderly. Key requirements include the following:
- 1.
- Accessible Restrooms: equipped with grab bars and non-slip surfaces to ensure safety and ease of use.
- 2.
- Open Spaces: designated areas for communal gatherings and group activities.
- 3.
- Outdoor Areas: spaces designed for light exercise, gardening, or simply enjoying nature.
- (2)
- Activity Requirements: Comprehensive programming is essential to address the physical, mental, and social needs of the elderly. Such activities should include the following:
- 4.
- Health Services: regular health screenings, exercise sessions, and wellness programs.
- 5.
- Vocational Training: opportunities for skill development, such as handicrafts or agricultural techniques that allow the elderly to remain productive and engaged.
- 6.
- Social Engagement: group activities, such as music therapy, storytelling sessions, or cultural events, to foster social connections and reduce isolation.
- (3)
- Environmental Accommodations: to create a supportive and inclusive environment, the health center should carry out the following:
- 7.
- Conduct home safety assessments for elderly participants to identify potential hazards and recommend modifications.
- 8.
- Integrate age-friendly design elements, such as ramps, handrails, and adjustable seating, to enhance mobility and comfort.
3.1.6. Living Conditions of the Elderly Participants
- (1)
- Quantitative Assessment
- Living Alone: approximately 7.1% (15 individuals) of elderly participants live alone without residing with any family members or caregivers.
- Living with Spouse Only: a significant proportion (30%, 64 individuals) resides solely with their spouse, without the presence of children or extended family members.
- Living with Children or Grandchildren: over a third of the participants (34.3%, 72 individuals) live in multigenerational households with their children or grandchildren, reflecting traditional Thai family structures.
- Living with Spouse and Children or Grandchildren: approximately 27.1% (57 individuals) reside with both spouse and children or grandchildren, indicating prevalent multi-generational living arrangements.
- Living with Spouse and Extended Family: a small proportion (0.5%, 1 individual) live with their spouse along with extended family members.
- Living with Children or Grandchildren and Extended Family: approximately 0.5% (1 individual) reside with their children or grandchildren and extended family members.
- (2)
- Qualitative Insights
- -
- Participants who live alone often reported concerns about safety, difficulties accessing healthcare, and feelings of loneliness. As one 72-year-old participant stated:
- -
- “I live alone because my children work in another province. They visit sometimes, but I feel lonely most days”.
- -
- Elderly participants living with their children or grandchildren frequently served in caregiving roles, actively contributing to their family’s daily routines. Another participant shared:
- -
- “Even though I’m old, I still help take care of my grandchildren while their parents work”.
- -
- Experiences of elderly individuals in extended family households varied significantly, with some reporting robust familial support while others described feelings of neglect and insufficient attention within their larger family settings.
- (3)
- Implications for Elderly Care
- -
- Elderly individuals living alone require community-based support such as regular health checks and social engagement programs to mitigate isolation and improve safety.
- -
- Families caring for elderly members require additional resources and education to better manage caregiving responsibilities and reduce associated stress. Multi-generational family arrangements should be carefully evaluated to ensure adequate support for elderly individuals experiencing neglect or isolation despite living with extended family.
3.2. Phase 2: Development of a Daycare Center for the Elderly with Community Participation
- Location Determination: A community meeting decided to utilize the multipurpose building in Baan Kho Community, Village 15, Baan Kho Subdistrict, Phon Sawan District, Nakhon Phanom Province, as the daycare center’s location. This site was selected due to its accessibility and central location within the community.
- Establishment of a Working Group: A multidisciplinary working group was formed to oversee the center’s operations. This group included representatives from key community stakeholders: The president of the elderly club, representatives from the local health promotion hospital (RPH), officers from the Subdistrict Administrative Organization (SAO), the village headman, and community health volunteers.
- Target Group Identification: The working group identified elderly individuals in need of services at the daycare center. Selection criteria included health status, socioeconomic conditions, and potential benefits from participation.
- Service Design: The center’s services were scheduled to operate from Monday to Friday, with health rehabilitation services provided once a week. The comprehensive service packages included the following:
- (1)
- Health Services: regular health screenings, nutritional guidance, cooking demonstrations, shared meals, health rehabilitation sessions, brain exercises (e.g., making sandalwood flowers and traditional crafts), and access to traditional medicine.
- (2)
- Social Services: activities such as folk music, music therapy, organic gardening, family support for household vegetable gardens, legal advice, and haircut services.
- (3)
- Psychological Services: listening to Buddhist teachings, relationship-building activities with grandchildren, and participating in community religious events and festivals.
- (4)
- Economic Services: vocational training, market linkage for product sales, selling community-made products, and establishing a savings fund.
- (5)
- Environmental Services: conducting International Classification of Functioning, Disability, and Health (ICF) surveys for home modifications and designing adjustments to suit the elderly’s specific needs.
- Coordinating activities according to the schedule.
- Engaging key community leaders and volunteers to ensure seamless execution.
- Establishing communication channels to address immediate concerns during service delivery.
- Monitoring Operations: Researchers and stakeholders observed the execution of services to verify that activities were conducted as planned. This included ensuring adherence to schedules, availability of resources, and the effectiveness of service delivery.
- Behavioral Observation: The behavior and engagement levels of elderly participants were closely monitored. This helped identify patterns of participation, preferences, and any challenges faced by the elderly during activities.
- Data Analysis: Researchers analyzed qualitative and quantitative data collected during the implementation and observation phases. This analysis identified key issues, barriers, and areas requiring improvement.
- Group Meetings: regular meetings were held with activity organizers and stakeholders to discuss findings, share experiences, and collaboratively explore solutions to identified challenges.
- Plan Adjustment: Feedback from data analysis and group meetings was used to refine the operational plan. Adjustments were made to improve service delivery and participant satisfaction.
3.3. Phase 3: Evaluation of Daycare Services for the Elderly
- Evaluation Process through Lesson Summarization
- A workshop was conducted to summarize lessons learned from the operations of the daycare center. This activity involved key leaders who participated in the center’s service delivery, providing insights into its development and impact. The key lessons included:
- (1)
- Development Stages of the Baan Kho Elderly Daycare Center: the daycare center originated from the Baan Kho Elderly Club, which had previously collaborated with the Node Health Promotion Foundation due to its exemplary work in elderly care.
- ○
- January 2021: initial activities were held on temple grounds, which served as the first venue.
- ○
- February 2021: activities were relocated to the SME Pavilion in the village, a space better suited to the nature of the center’s operations and the elderly’s needs.
- (2)
- Goals for Establishing the Daycare Center: the primary aim was to create a central hub where elderly individuals could gather and participate in a variety of activities tailored to their needs.
- ○
- Activities were designed to be voluntary, ensuring that participation was based on interest and willingness.
- ○
- Retired professionals were encouraged to volunteer, contributing their expertise to the center’s programs.
- ○
- The center sought collaboration with external organizations for knowledge sharing and resource donations, enhancing its operational capacity.
- (3)
- Community Expectations for the Daycare Center: the community envisioned the center as a venue that would accomplish the following:
- ○
- Provide activities tailored to the elderly’s physical, mental, and social needs.
- ○
- Promote cheerfulness and stress relief among the elderly.
- ○
- Serve as a daily activity center equipped with adequate facilities to support elderly engagement.
- (4)
- Development Path of the Elderly Daycare Center: the step-by-step progress and milestones of establishing the center were documented in detail, highlighting the systematic approach taken to create and enhance the center’s operations.
- II.
- Meeting the Needs of the ElderlyThe evaluation ensured that the daycare center’s services aligned with the specific requirements of the elderly. This included providing health, social, psychological, and vocational support while addressing environmental needs.
- III.
- Providing Community ValueThe center was assessed for its contribution to the community, particularly in fostering social cohesion, reducing caregiver burdens, and involving community members and organizations in elderly care.
- IV.
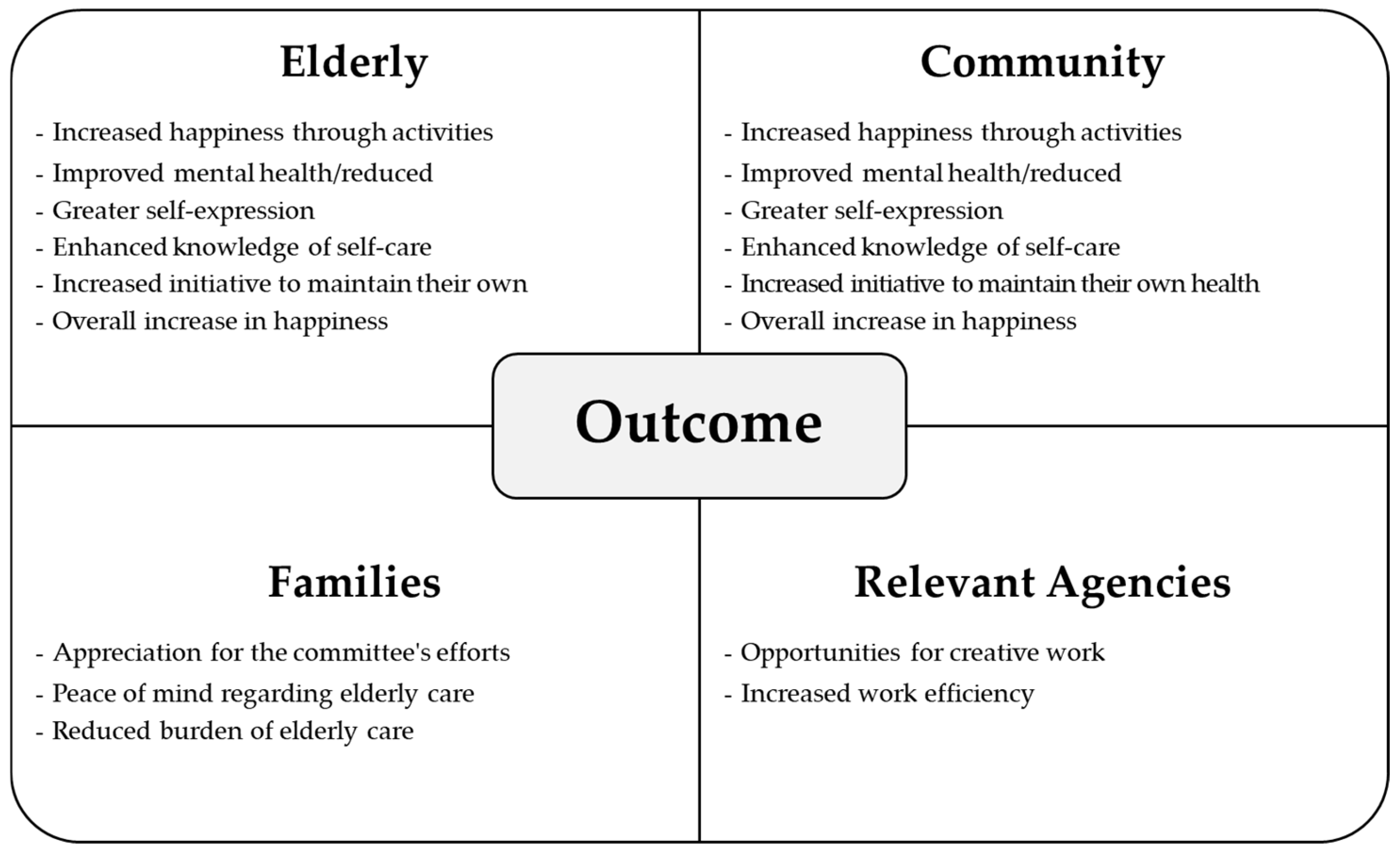
- Achieving Intended GoalsThe evaluation verified that the center achieved its goals, including creating a welcoming and functional hub for the elderly, promoting well-being, and establishing a sustainable model for elderly care.By evaluating these aspects, the research provided evidence of the center’s success in enhancing the quality of life for the elderly while meeting the community’s expectations. The findings demonstrated the effectiveness of community-driven initiatives in establishing sustainable and impactful care models (See Figure 4).
- I.
- Lessons Learned from Developing the Daycare Center
- The development process revealed key mechanisms and support structures crucial to the center’s success:
- (1)
- Main Mechanisms: four primary components were instrumental in establishing and sustaining the daycare center:
- Elderly Club: acted as the core group for coordinating activities and promoting participation.
- Subdistrict Health Promotion Hospital (RPH): provided health services and expertise.
- Volunteer Teachers/Artisans: facilitated skill-building and vocational activities.
- Village Health Volunteers (VHVs): supported health-related initiatives and outreach efforts.
- (2)
- Supporting Mechanisms: A wide range of stakeholders contributed to the center’s development and operations, including the following:
- Academic institutions and hospitals for technical and financial support.
- Temples for spiritual and cultural activities.
- Village headmen and Subdistrict Administrative Organizations (SAOs) for administrative and logistical support.
- Non-formal education centers and foundations for additional resources and training.
- II.
- Outcomes of the Elderly Daycare Center
- The elderly daycare center in Baan Kho Community marks a key achievement in improving the quality of life for elderly individuals. Using a community-driven approach, the center integrates health, social, vocational, psychological, and environmental services to address diverse needs. It fosters active participation and utilizes local resources, benefiting not only the elderly but also families, the community, and related agencies. Systematic evaluations, including satisfaction surveys and comparative analyses, highlight its effectiveness in promoting well-being and generating innovations. These outcomes showcase the center’s value as a model for addressing aging challenges through community-based care.
- (1)
- Creation of New Knowledge and Innovations: The establishment of the center led to the development of innovative service packages tailored to the needs of the elderly. These included diverse daily activities that promoted physical, mental, and social well-being, such as health rehabilitation, traditional crafts, and cultural events.
- (2)
- Improvement in Well-being and Satisfaction: The effectiveness of the center was evaluated through a comparative analysis of data collected before and after elderly participation in its activities. Satisfaction surveys from 50 elderly respondents were analyzed using the t-test-dependent statistical method, revealing significant improvements in their well-being and quality of life (See Table 6). The analysis highlighted (1) increased satisfaction with the center’s services, (2) enhanced physical and mental health outcomes, and (3) greater social engagement and reduced feelings of isolation. These findings underscore the critical role of community-driven initiatives in improving elderly care. The lessons learned and positive outcomes demonstrate the potential for replicating this model in other communities to address the comprehensive needs of elderly populations.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Satisfaction with Services at Baan Kho Elderly Daycare Center | n | Mean | SD | Mean Difference | SE | 95% Mean Difference | T | df | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||||
| After the test | 51 | 3.57 | 0.35 | −0.59 | 0.06 | −0.71 | −0.47 | −9.91 | 50 | 0.000 |
| Before the test | 51 | 4.16 | 0.29 | −0.59 | 0.06 | −0.71 | −0.47 | −9.91 | 50 | 0.000 |
4. Discussion
4.1. Lessons Learned from Developing the Daycare Center
- (1)
- The Role of Realistic Cost Assessment in Policy Planning: For policymakers and stakeholders, understanding the financial requirements of an elderly daycare center is critical in determining its feasibility and long-term sustainability. Studies have shown that community-based elder care models can be more cost-effective than institutional care if resources are utilized efficiently. Our study demonstrated that high-quality elderly care services can be provided at a relatively low cost, particularly when leveraging community participation and existing public health infrastructure [8].
- (2)
- Balancing Cost and Service Quality: One challenge in elderly care services is maintaining affordability without compromising quality. A systematic review by Orellana, Manthorpe, and Tinker [9] found that daycare centers significantly improve elderly well-being and reduce healthcare costs by preventing hospitalizations and long-term institutional care. The Ban Kho model achieved this balance by utilizing existing community infrastructure instead of investing in costly new facilities [13]; establishing partnerships with health promotion hospitals, which provided free health check-ups and medical supervision [14]; engaging retired professionals and trained volunteers, which eliminated the need for expensive full-time staff [15]; and offering flexible service packages, allowing local governments to scale services up or down depending on their financial capacity [16]. These approaches ensured that elderly individuals received essential care, social interaction, and health services without imposing unsustainable financial burdens on local governments [17].
- (3)
- The Importance of Public-Private Collaboration: The study highlights that a multi-sectoral funding approach is necessary for financially sustainable elderly care centers [2]. The project was able to maintain operations without charging fees to elderly participants due to diversified funding streams, including public sector investment (local government and public health agencies) [18], private donations (community fundraising, local businesses, and religious organizations) [8], academic grants, supporting training programs and caregiver education [19], and volunteer support, reducing labor costs [13].
- (4)
- Cost-Effectiveness and Scalability for Broader Policy Implementation: For policymakers and stakeholders looking to expand elderly daycare services, the Ban Kho model provides an adaptable framework that can be implemented in other regions [9]. Given that Thailand’s aging population is growing, a cost-effective and scalable model for elderly care must be integrated into national and local policy frameworks [20]. The Ban Kho model’s ability to operate at ~12,416 USD/year PPP-adjusted demonstrates that sustainable elderly care is financially achievable, even in low-resource settings [8,21].
4.2. Outcomes of the Daycare Center
4.3. Impact on the Community and Stakeholders
4.4. Impact on Geriatric Health
- (1)
- Government Funding: ongoing financial support from local administrative organizations and public health programs.
- (2)
- Community Contributions: a combination of local fundraising, voluntary donations, and Corporate Social Responsibility (CSR) initiatives.
- (3)
- Public–Private Partnerships: collaboration with private healthcare providers and non-profit organizations to co-fund operational expenses.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Olimid, A.P.; Olimid, D.A. Societal challenges, population trends and human security: Evidence from the public governance within the United Nations publications (2015-2019). Rev. Stiinte Politice 2019, 64, 53–64. [Google Scholar]
- Bloom, D.E.; Canning, D.; Fink, G. The greying of the global population and its macroeconomic consequences. Twenty-First Century Soc. 2010, 5, 233–242. [Google Scholar] [CrossRef]
- Teerawichitchainan, B. Older persons in Thailand: An update from a recent national survey. Asian Popul. Stud. 2020, 16, 243–247. [Google Scholar]
- Anantanasuwong, D. Population Ageing in Thailand: Critical Issues in the Twenty-First Century. In Education for the Elderly in the Asia Pacific (Education in the Asia-Pacific Region: Issues, Concerns and Prospects); Narot, P., Kiettikunwong, N., Eds.; Springer: Singapore, 2021. [Google Scholar]
- Knodel, J.; Chayovan, N. Intergenerational relationships and family care and support for Thai elderly. Ageing Int. 2008, 33, 15–27. [Google Scholar] [CrossRef]
- World Health Organization. Universal Health Coverage Partnership Annual Report 2021: Health Systems Strengthening and Health Emergencies Beyond COVID-19; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- Razavi, S. Making the right to social security a reality for all workers. Indian J. Labour Econ. 2022, 65, 269–294. [Google Scholar] [CrossRef] [PubMed]
- Knodel, J.E.; Prachuabmoh, V.; Chayovan, N. The Changing Well-Being of Thai Elderly: An Update from the 2011 Survey of Older Persons in Thailand; HelpAge International: Chiang Mai, Thailand, 2013. [Google Scholar]
- Orellana, K.; Manthorpe, J.; Tinker, A. Day centres for older people: A systematically conducted scoping review of literature about their benefits, purposes and how they are perceived. Ageing Soc. 2020, 40, 73–104. [Google Scholar] [CrossRef] [PubMed]
- Yamane, T. Statistics: An Introductory Analysis; Harper & Row: New York, NY, USA, 1973. [Google Scholar]
- Hair, J.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis; Prentice Hall: Hoboken, NJ, USA, 2009. [Google Scholar]
- Lincoln, Y.S.; Guba, E. Naturalistic Inquiry; Sage: Los Angeles, CA, USA, 1985; Volume 75. [Google Scholar]
- Suwan, P.R.; Hardnaulee, D. Social welfare programs for elderly people and women in Thailand. Asia Pac. J. Relig. Cult. 2022, 6, 130–140. [Google Scholar]
- Pilayon, B.; Tanukit, P.; Rueangworaboon, S.; Inchaiya, C.; Dumrongpakapakorn, P. Can Family Carer Groups Help People with Intellectual Disabilities? Applying Focused Ethnography Methods in Community Contexts of Northeastern Thailand. Malays. J. Med. Health Sci. 2022, 18, 76–82. [Google Scholar]
- Laver, K.; Cumming, R.G.; Dyer, S.M.; Agar, M.R.; Anstey, K.J.; Beattie, E.; Brodaty, H.; Broe, T.; Clemson, L.; Crotty, M.; et al. Clinical practice guidelines for dementia in Australia. Med. J. Aust. 2016, 204, 191–193. [Google Scholar] [PubMed]
- Ross, A.; Arnold, J.; Gormley, A.; Locke, S.; Shanske, S.; Tardiff, C. Care coordination in pediatric health care settings: The critical role of social work. Soc. Work. Health Care 2019, 58, 1–13. [Google Scholar] [PubMed]
- Ong, S.; Woo, J.; Parikh, P.; Chan, R.; Sun, J.; Mun, C.Y.; Wee, S.L.; Thu, N.N.; Thang, P.; Setiati, S.; et al. Addressing nutritional requirements of ageing consumers in Asia-recommendations from an expert workshop. Asia Pac. J. Clin. Nutr. 2019, 28, 204–213. [Google Scholar] [PubMed]
- Bolton, L. Innovative Financing Methods for Social Protection; Institute of Development Studies: Brighton, UK, 2017. [Google Scholar]
- Wendimagegn, N.F.; Bezuidenhout, M.C. Integrating promotive, preventive, and curative health care services at hospitals and health centers in Addis Ababa, Ethiopia. J. Multidiscip. Healthc. 2019, 12, 243–255. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Long-Term Care Financing: Lessons for Low-and Middle-Income Settings. Brief 8. Ensuring Financial Sustainability in Long-Term Care; World Health Organization: Geneva, Switzerland, 2024. [Google Scholar]
- Chand, M. Aging in South Asia: Challenges and opportunities. South Asian J. Bus. Stud. 2018, 7, 189–206. [Google Scholar] [CrossRef]

| Cost Category | Estimated Amount (THB) | PPP-Adjusted (USD) | Funding Source |
|---|---|---|---|
| Infrastructure Setup and Renovation | 150,000 | ~9804 | Local Government and Community Fundraising |
| Equipment and Materials (furniture, kitchen, recreational materials) | 50,000 | ~3268 | Local Government and Donations |
| Health Services (screenings, basic medical supplies) | 30,000/year | ~1961/year | Public Health Center and Volunteers |
| Daily Operations and Staff Support | 100,000/year | ~6536/year | Local Administrative Organization (SAO) |
| Community and Educational Activities (workshops, training, recreational programs) | 40,000/year | ~2614/year | Public and Private Donations |
| Volunteer and Support Incentives | 20,000/year | ~1307/year | Local Health and Social Welfare Budget |
| Miscellaneous Expenses (transportation, maintenance) | 20,000 B/year | ~1307/year | Local Government |
| Characteristics | N (%) |
|---|---|
| Male | 71 (33.81) |
| Female | 139 (66.19) |
| Age | |
| Young old (60–69 years old) | 304 (56.93) |
| Middle old (70–79 years old) | 175 (32.77) |
| Very old (80 years old and above) | 54 (10.11) |
| Nonelderly (Under 60 years of age) | 1 (0.19) |
| Marital status | |
| Single | 7 (3.33) |
| Marriage | 119 (56.67) |
| Widowed | 78 (37.14) |
| Divorce | 6 (2.86) |
| Education | |
| Bachelor’s degree | 1 (0.48) |
| Secondary education | 4 (1.90) |
| Primary education | 195 (92.86) |
| Not educate | 10 (4.76) |
| Occupation | |
| Farmer | 153 (72.86) |
| Owner business | 14 (6.67) |
| Unemployed | 39 (18.57) |
| Not specified | 4 (1.90) |
| Income per Month (THB) | Equivalent in PPP USD | Comparison with Global Standards | N (%) |
|---|---|---|---|
| Less than 1000 | ~65 | Below extreme poverty line (USD 2.15/day) | 130 (61.90) |
| 1001–3000 | 65–196 | Near/below lower-middle-income threshold | 71 (33.81) |
| 3100–5000 | ~203–327 | Low income, but above extreme poverty | 6 (2.86) |
| 5001–10,000 | ~327–654 | Comparable to low–middle income | 2 (0.95) |
| More than 10,000 | >654 | Closer to global lower-middle income | 1 (0.48) |
| Issues | Health Problem | Health Needs of the Elderly | ||
|---|---|---|---|---|
| Mean (SD) | Interpretation | Mean (SD) | Interpretation | |
| Physical | 1.61 (0.85) | Very Low | 4.33 (0.90) | High |
| Mental | 1.57 (0.76) | Very Low | 4.21 (0.90) | High |
| Social and Economic | 2.77 (1.49) | Low | 4.27 (0.94) | High |
| Spiritual | 1.67 (0.84) | Very Low | - | - |
| Housing and Environment | 1.32 (0.60) | Very Low | 4.18 (0.89) | High |
| Overall Questionnaire | 1.79 (0.90) | Very Low | 4.25 (0.91) | High |
| Daycare Service Needs | Mean | Standard Deviation | Interpretation |
|---|---|---|---|
| Need for Daycare Center Establishment | 4.47 | 0.77 | High |
| Service Needs | 4.33 | 0.82 | High |
| Facility Needs | 4.20 | 0.87 | High |
| Overall Questionnaire | 4.33 | 0.82 | High |
| Health Data Before and After | Mean Difference | S.D. | t-Value | df | Sig. |
|---|---|---|---|---|---|
| Weight | 0.64 | 1.18 | 3.83 | 49 | 0.00 |
| Body Mass Index (BMI) | 0.28 | 0.50 | 3.94 | 49 | 0.00 |
| Ability to perform daily living activities (Barthel ADL index) | −0.20 | 0.61 | −2.33 | 49 | 0.02 |
| Dementia status | −4.66 | 2.98 | −11.06 | 49 | 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pilayon, B.; Chueaduangpui, K.; Saentho, J.; Kongmant, R.; Turnbull, N. Development of an Adult Daycare Center Service Model for the Elderly Through Community Participation: An Action Research Approach. Geriatrics 2025, 10, 55. https://doi.org/10.3390/geriatrics10020055
Pilayon B, Chueaduangpui K, Saentho J, Kongmant R, Turnbull N. Development of an Adult Daycare Center Service Model for the Elderly Through Community Participation: An Action Research Approach. Geriatrics. 2025; 10(2):55. https://doi.org/10.3390/geriatrics10020055
Chicago/Turabian StylePilayon, Benjayamas, Kanin Chueaduangpui, Juthaluck Saentho, Ruchakron Kongmant, and Niruwan Turnbull. 2025. "Development of an Adult Daycare Center Service Model for the Elderly Through Community Participation: An Action Research Approach" Geriatrics 10, no. 2: 55. https://doi.org/10.3390/geriatrics10020055
APA StylePilayon, B., Chueaduangpui, K., Saentho, J., Kongmant, R., & Turnbull, N. (2025). Development of an Adult Daycare Center Service Model for the Elderly Through Community Participation: An Action Research Approach. Geriatrics, 10(2), 55. https://doi.org/10.3390/geriatrics10020055