
Health Professional Support for Friends and Family Members of Older People Discharged from Hospital After a Fracture: A Survey Study


Abstract
1. Introduction
Purpose
2. Materials and Methods
2.1. Design
2.2. Participants and Approach
2.3. Potentially Eligible Participants
- Practising health professionals including (but not exclusive to) the following: members of the physiotherapy, occupational therapy or nursing teams, medical practitioners and surgeons.
- Those working in trauma and orthopaedic, musculoskeletal, geriatric/older people’s/frailty or rehabilitation services.
- The aforementioned participants provided informed consent in order to participate in the study.
2.4. Data Collection
2.5. Sample Size
2.6. Data Analysis
3. Results
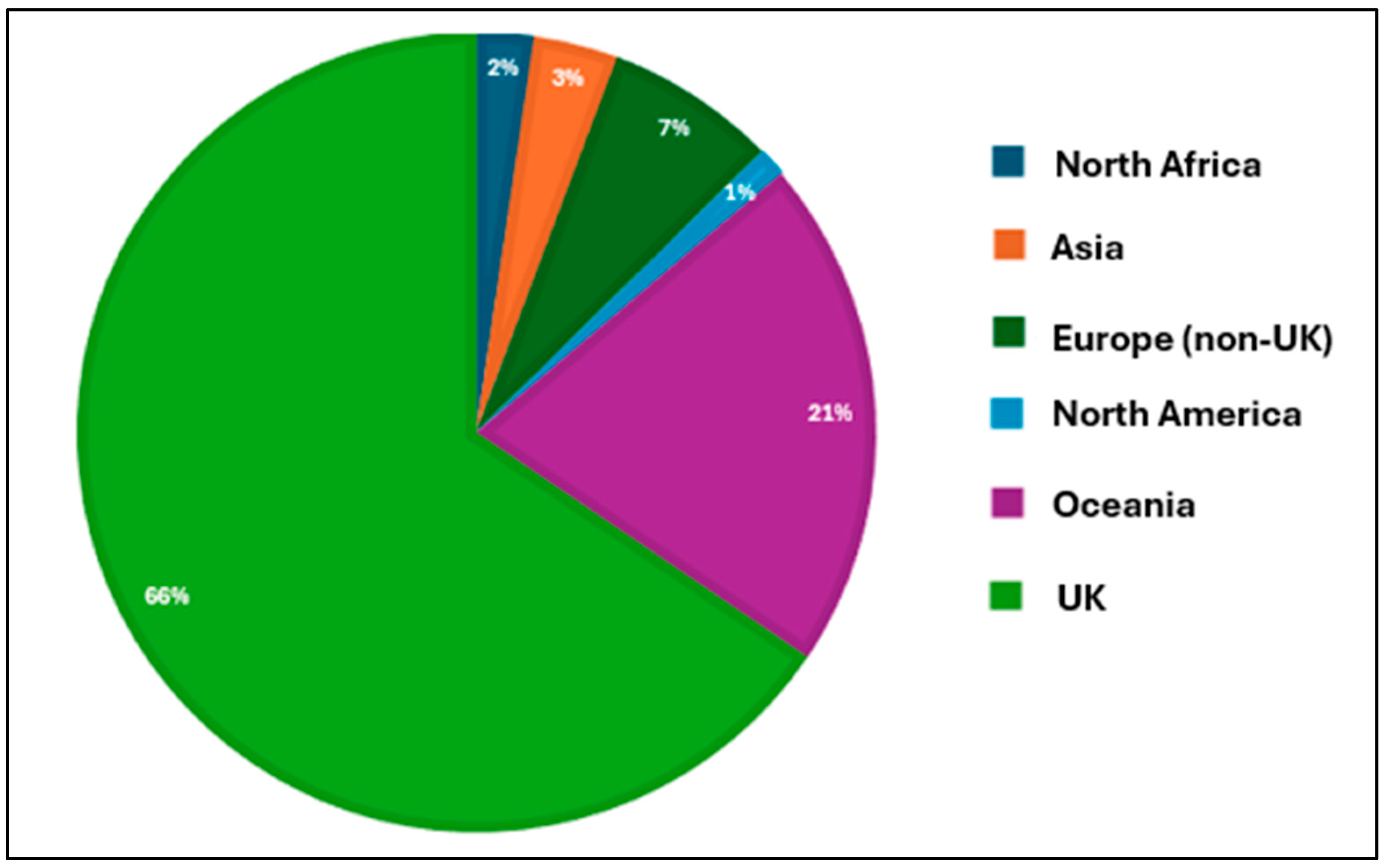
3.1. Respondent Characteristics
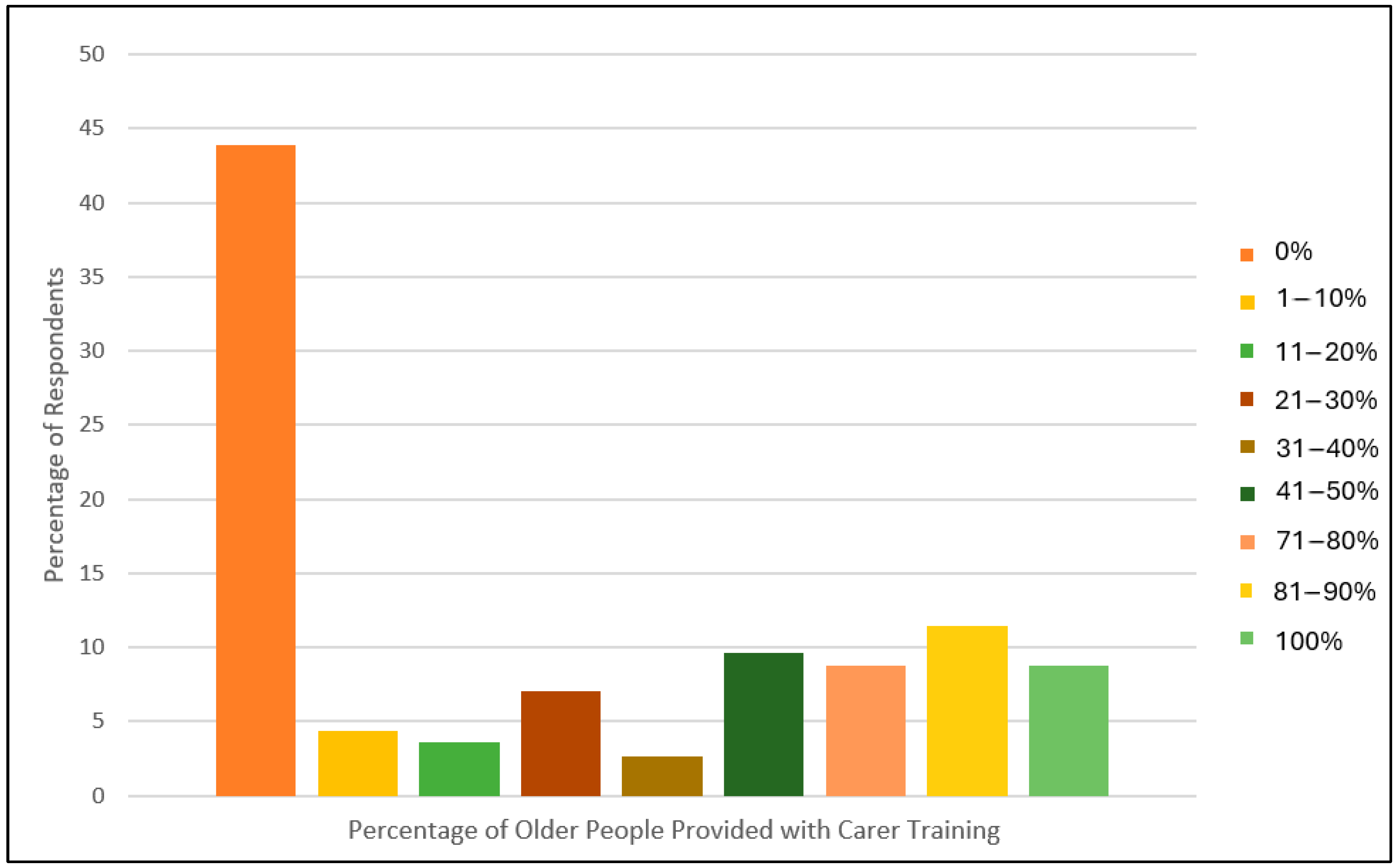
3.2. Delivery of Carer Training for People Following Fracture
3.3. Factors Influencing Implementation
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Department of Health. Office for Health Improvement and Disparities. Guidance: Falls: Applying All Our Health. Updated 25 February 2022. Falls: Applying All Our Health—GOV.UK. Available online: www.gov.uk (accessed on 3 June 2024).
- Lawler, K.; Taylor, N.F.; Shields, N. Involving family members in physiotherapy for older people transitioning from hospital to the community: A qualitative analysis. Disabil. Rehabil. 2015, 37, 2061–2069. [Google Scholar] [CrossRef]
- Dyer, S.M.; Crotty, M.; Fairhall, N.; Magaziner, J.S.; Beaupre, L.A.; Cameron, I.; Sherrington, C. A critical review of the long-term disability outcomes following hip fracture. BMC Geriatr. 2016, 16, 158. [Google Scholar] [CrossRef] [PubMed]
- Parsons, N.; Griffin, X.L.; Achten, J.; Costa, M.L. Outcome assessment after hip fracture: Is EQ-5D the answer? Bone Jt. Res. 2014, 3, 69–75. [Google Scholar] [CrossRef]
- Bökberg, C.; Lindhardt, T.; Björkman, E.; Ahlström, G. Caring and health of close family members of frail older persons recently discharged from acute hospital care: A comparative cross-sectional study. Nurs. Rep. 2024, 14, 901–912. [Google Scholar] [CrossRef]
- PHFSA. Recovering After a Hip Fracture: Helping People Understand Physiotherapy in the NHS. Physiotherapy ‘Hip Spirit’ Audit Report 2017. PHFSA201802w1.pdf. Available online: https://fffap.org.uk/ (accessed on 13 June 2024).
- Blackburn, J.; Yeowell, G. Patients’ perceptions of rehabilitation in the community following hip fracture surgery. A qualitative thematic synthesis. Physiotherapy 2020, 108, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Ariza-Vega, P.; Ortiz-Piña, M.; Kristensen, M.T.; Castellote-Caballero, Y.; Jiménez-Moleón, J.J. High perceived caregiver burden for relatives of patients following hip fracture surgery. Disabil. Rehabil. 2019, 41, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Wimo, A.; Karlsson, G.; Jönsson, B.; Winblad, B. (Eds.) Evaluation of the resource utilization and caregiver time in Anti-dementia drug trials—A quantitative battery. In The Health Economics of Dementia; Wiley’s: London, UK, 1998. [Google Scholar]
- Smith, T.O.; Langford, S.; Ward, K.; Gray, R. Unpaid caregiving for people following hip fracture: Longitudinal analysis from the English Longitudinal Study of Ageing. Eur. Geriatr. Med. 2023, 14, 1249–1260. [Google Scholar] [CrossRef]
- Office for National Statistics. Living Longer: Caring in Later Working Life. Living Longer—Office for National Statistics. 2019. Available online: https://ons.gov.uk (accessed on 6 June 2024).
- Saletti-Cuesta, L.; Tutton, E.; Langstaff, D.; Willett, K. Understanding informal carers’ experiences of caring for older people with a hip fracture: A systematic review of qualitative studies. Disabil. Rehabil. 2018, 40, 740–750. [Google Scholar] [CrossRef]
- Lin, P.C.; Hung, S.H.; Liao, M.H.; Sheen, S.Y.; Jong, S.Y. Care needs and level of care difficulty related to hip fractures in geriatric populations during the post-discharge transition period. J. Nurs. Res. 2006, 14, 251–260. [Google Scholar] [CrossRef]
- Wu, L.C.; Chou, M.Y.; Liang, C.K.; Lin, Y.T.; Ku, Y.C.; Wang, R.H. Association of home care needs and functional recovery among community-dwelling elderly hip fracture patients. Arch. Gerontol. Geriatr. 2013, 57, 383–388. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. Improving the quality of web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Mou, H.; Lam, S.K.K.; Chien, W.T. The effects of a family-focused dyadic psychoeducational intervention for stroke survivors and their family caregivers: A randomised controlled trial. Int. J. Nurs. Stud. 2023, 143, 104504. [Google Scholar] [CrossRef]
- van der Velde, M.Y.; Aerden, L.A.M.; van Oort, A.; Bodde, K.; Rambaran Mishre, R.; Oosterveer, D.M. Caregiver strain and fatigue are independent determinants of anxiety among patients early after stroke. Neuropsychol. Rehabil. 2023, 33, 428–439. [Google Scholar] [CrossRef]
- Wang, J.; Liu, J.; Li, L.; Man, J.; Yue, S.; Liu, Z. Effect of education and muscle relaxation program on anxiety, depression and care burden in caregivers of acute stroke survivors: A randomized, controlled study. Medicine 2021, 100, e24154. [Google Scholar] [CrossRef] [PubMed]
- Jammal, M.; Kolt, G.S.; Liu, K.P.Y.; Dennaoui, N.; George, E.S. The impact of caregiving on the roles and valued activities of stroke carers: A systematic review of qualitative studies. PLoS ONE 2024, 19, e0304501. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Wu, T.T.; Cai, H.; He, J.Y.; Wang, T.Y.; Lin, X.X.; Li, H. Effects of Wab-WPPEP on post-intensive care syndrome-family in family caregivers of heart valve replacement patients: A randomized controlled trial. Intensive Crit. Care Nurs. 2024, 86, 103817. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Zhang, X.; Li, Y.; Lv, Q.; Gao, X.; Lin, M.; Zang, X. Advanced heart failure patients and family caregivers health and function: Randomised controlled pilot trial of online dignity therapy. BMJ Support. Palliat. Care 2023, in press. [Google Scholar] [CrossRef]
- Reichman, M.; Grunberg, V.A.; Presciutti, A.M.; Foster, K.T.; Vranceanu, A.M.; Creutzfeldt, C.J. Peer-delivered interventions for caregivers in the ICU with a focus on severe acute brain injury: A scoping review. Neurocrit. Care 2024, in press. [Google Scholar] [CrossRef]
- Smith, T.O.; Khoury, R.; Hanson, S.; Welsh, A.; Grant, K.; Clark, A.B.; Ashford, P.-A.; Hopewell, S.; Pfeiffer, K.; Logan, P.; et al. Hospital-based caregiver intervention for people following hip fracture surgery (HIP HELPER): Multicentre randomised controlled feasibility trial with embedded qualitative study in England. BMJ Open 2023, 13, e073611. [Google Scholar] [CrossRef]
- Welsh, A.; Hanson, S.; Pfeiffer, K.; Khoury, R.; Clark, A.; Grant, K.; Ashford, P.A.; Hopewell, S.; Logan, P.A.; Crotty, M.; et al. Facilitating the transition from hospital to home after hip fracture surgery: A qualitative study from the HIP HELPER trial. BMC Geriatr. 2024, 24, 948. [Google Scholar] [CrossRef] [PubMed]
- Welsh, A.; Hanson, S.; Pfeiffer, K.; Khoury, R.; Clark, A.; Ashford, P.A.; Hopewell, S.; Logan, P.; Crotty, M.; Costa, M.; et al. Perspectives of informal caregivers who support people following hip fracture surgery: A qualitative study embedded within the HIP HELPER feasibility trial. BMJ Open 2023, 13, e074095. [Google Scholar] [CrossRef]
- Brown, K.; Cameron, I.D.; Keay, L.; Coxon, K.; Ivers, R. Functioning and health-related quality of life following injury in older people: A systematic review. Injury Prev. 2017, 23, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Rafferty, M.; Stoff, L.; Smith, J.D.; Hansen, P.; Briody, M.; Diaz, C.; O’Donnell, L.; Heinemann, A.W.; Brown, C.H.; Lieber, R.L. Promoting evidence-based practice: The influence of novel structural change to accelerate translational rehabilitation. Arch. Phys. Med. Rehabil. 2023, 104, 1289–1299. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Always | Sometimes | Never | N | |
|---|---|---|---|---|
| Which health professionals provided training for the respondents? | ||||
| Nursing Team | 7 (14.3) | 29 (59.2) | 13 (26.5) | 49 |
| Physiotherapy Team | 44 (77.2) | 13 (22.8) | 0 (0.0) | 57 |
| Occupational Therapy Team | 16 (30.8) | 31 (59.6) | 5 (9.6) | 52 |
| General Multidisciplinary Team | 10 (21.3) | 30 (63.8) | 7 (14.9) | 47 |
| Social Workers | 1 (2.3) | 17 (39.5) | 25 (58.1) | 43 |
| Physicians | 3 (7.0) | 24 (55.8) | 16 (37.2) | 43 |
| Surgeons | 2 (4.7) | 19 (44.2) | 22 (51.2) | 43 |
| Other: Nursing Assistant, Pharmacist, Volunteer | 1 (3.8) | 4 (15.4) | 21 (80.8) | 26 |
| What type of patients did the carers receive training for? | ||||
| Hip fracture | 27 (54.0) | 21 (42.0) | 2 (4.0) | 50 |
| Other lower limb fracture (non-hip) | 18 (36.0) | 31 (62.0) | 1 (2.0) | 50 |
| Spinal fracture | 21 (42.0) | 25 (50.0) | 4 (8.0) | 50 |
| Upper limb fracture | 16 (32.0) | 32 (64.0) | 2 (4.0) | 50 |
| Major trauma fracture | 22 (45.8) | 21 (43.8) | 5 (10.4) | 48 |
| Patients who live at home with identified carer | 27 (56.3) | 19 (39.6) | 2 (4.2) | 48 |
| Other: Caregivers, Care home carers, Rib fractures | 2 (10.0) | 8 (40.0) | 10 (50.0) | 20 |
| Where is training provided? | ||||
| In hospital | 15 (37.5) | 18 (45.0) | 7 (17.5) | 40 |
| Out of hospital | 17 (45.9) | 17 (45.9) | 3 (8.1) | 37 |
| In and out of hospital | 9 (24.3) | 21 (56.8) | 7 (18.9) | 37 |
| How is training provided? | ||||
| Face-to-face | 34 (70.8) | 13 (27.1) | 1 (2.1) | 48 |
| Virtual (telephone or online) | 1 (2.5) | 22 (55.0) | 17 (42.5) | 40 |
| Hybrid (face-to-face AND virtual) | 0 (0.0) | 15 (40.5) | 22 (59.5) | 37 |
| What is provided in the carer training? | ||||
| Discussion on recovery expectations | 31 (68.9) | 13 (28.9) | 1 (28.9) | 45 |
| Practice manual handling (transfers/walking practice) | 24 (51.1) | 22 (46.8) | 1 (46.8) | 47 |
| Exercise prescription and progression advice | 26 (55.3) | 20 (42.6) | 1 (42.6) | 47 |
| Signposting to other post-discharge services | 13 (27.7) | 32 (68.1) | 2 (68.1) | 47 |
| Education on potential post-discharge complications | 20 (42.6) | 25 (53.2) | 2 (53.2) | 47 |
| Pacing and behaviour modification advice | 20 (42.6) | 23 (48.9) | 4 (48.9) | 47 |
| Advice on stress and anxiety management for caregivers | 9 (19.1) | 27 (57.4) | 11 (57.4) | 47 |
| Provision of contact details for further support | 20 (42.6) | 24 (51.1) | 3 (51.1) | 47 |
| Provision of written information/materials or online links | 19 (40.4) | 25 (53.2) | 3 (53.2) | 47 |
| Duration of carer training provided | ||||
| Inpatient only | 16 (45.7) | 15 (42.9) | 4 (11.4) | 35 |
| Up to 2 weeks post-hospital discharge | 12 (30.8) | 18 (46.2) | 9 (23.1) | 39 |
| Up to 4 weeks post-hospital discharge | 9 (23.1) | 20 (51.3) | 10 (25.6) | 39 |
| Up to 6 weeks post-hospital discharge | 10 (24.4) | 19 (46.3) | 12 (29.3) | 41 |
| Longer than 6 weeks post-hospital discharge | 8 (18.2) | 21 (47.7) | 15 (34.1) | 44 |
| Strongly Agree | Agree | Neutral | Disagree | Strongly Disagree | N | |
|---|---|---|---|---|---|---|
| Patients living alone | 2 (33.3) | 1 (16.7) | 3 (50.0) | 0 (0.0) | 0 (0.0) | 6 |
| Patients living with an unpaid carer | 4 (66.7) | 1 (16.7) | 1 (16.7) | 0 (0.0) | 0 (0.0) | 6 |
| Patients living in a care home/care facility | 2 (33.3) | 1 (16.7) | 2 (33.3) | 1 (16.7) | 0 (0.0) | 6 |
| Patients following hip fracture | 3 (50.0) | 2 (33.3) | 1 (16.7) | 0 (0.0) | 0 (0.0) | 6 |
| Patients following lower limb fracture (non-hip) | 3 (50.0) | 1 (16.7) | 2 (33.3) | 0 (0.0) | 0 (0.0) | 6 |
| Patients following spinal fracture | 2 (33.3) | 3 (50.0) | 1 (16.7) | 0 (0.0) | 0 (0.0) | 6 |
| Patients following multiple fractures | 3 (60.0) | 1 (20.0) | 1 (20.0) | 0 (0.0) | 0 (0.0) | 5 |
| Major trauma patients | 4 (66.7) | 1 (16.7) | 1 (16.7) | 0 (0.0) | 0 (0.0) | 6 |
| Any patient who has experienced a fracture | 3 (50.0) | 1 (16.7) | 2 (33.3) | 0 (0.0) | 0 (0.0) | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, T.O.; Arnold, S.; Baxter, M. Health Professional Support for Friends and Family Members of Older People Discharged from Hospital After a Fracture: A Survey Study. Geriatrics 2025, 10, 36. https://doi.org/10.3390/geriatrics10020036
Smith TO, Arnold S, Baxter M. Health Professional Support for Friends and Family Members of Older People Discharged from Hospital After a Fracture: A Survey Study. Geriatrics. 2025; 10(2):36. https://doi.org/10.3390/geriatrics10020036
Chicago/Turabian StyleSmith, Toby O., Susanne Arnold, and Mark Baxter. 2025. "Health Professional Support for Friends and Family Members of Older People Discharged from Hospital After a Fracture: A Survey Study" Geriatrics 10, no. 2: 36. https://doi.org/10.3390/geriatrics10020036
APA StyleSmith, T. O., Arnold, S., & Baxter, M. (2025). Health Professional Support for Friends and Family Members of Older People Discharged from Hospital After a Fracture: A Survey Study. Geriatrics, 10(2), 36. https://doi.org/10.3390/geriatrics10020036