
Effects of Unpredictable Perturbation Training on a Split-Belt Treadmill on Physical Performance in Older Adults: A Randomized Controlled Trial


Abstract
1. Introduction
2. Materials and Methods
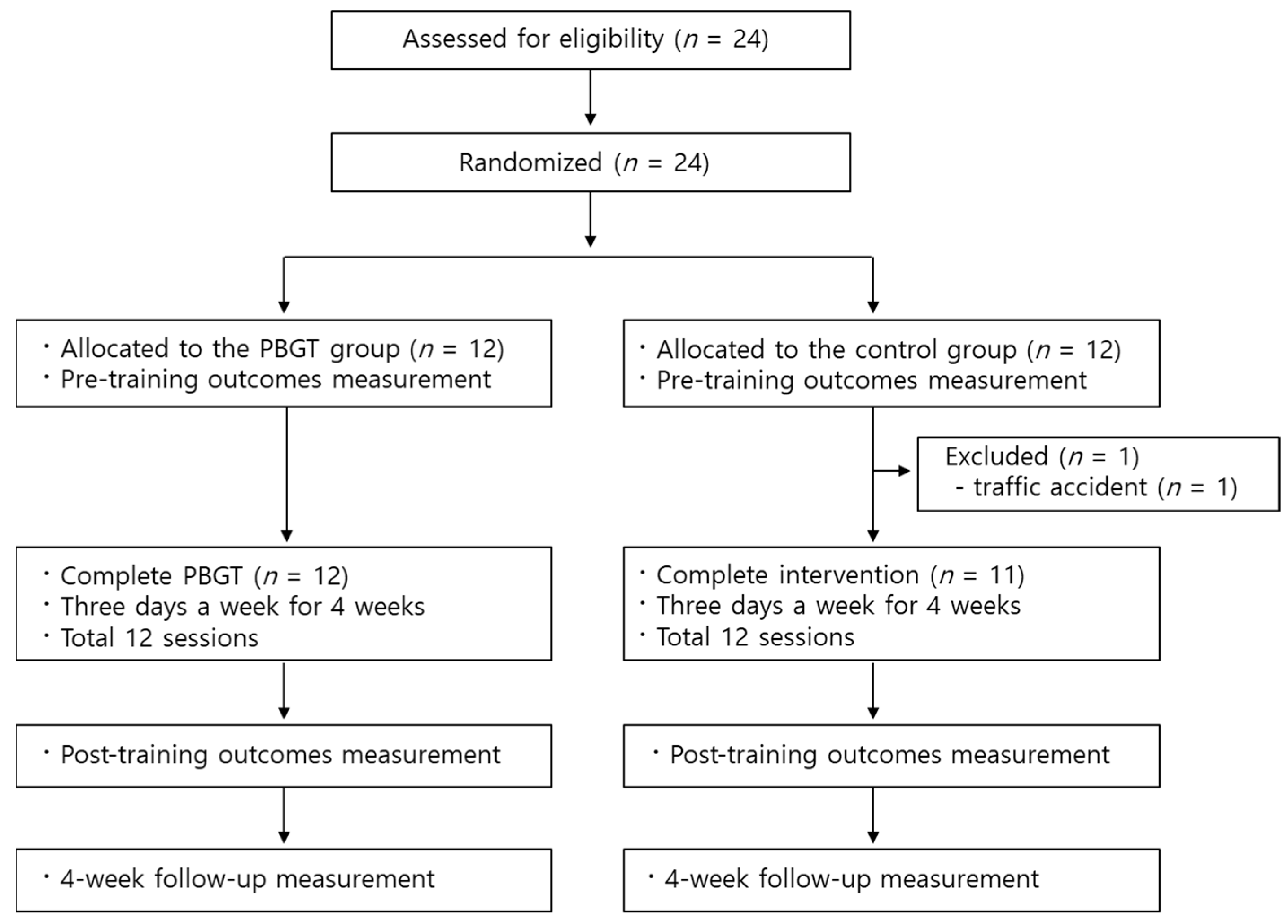
2.1. Study Design
2.2. Participants
2.3. Randomization
2.4. Sample Size
2.5. Intervention
2.6. Outcome Measurement
2.7. Statistical Analysis
3. Results
3.1. Participants
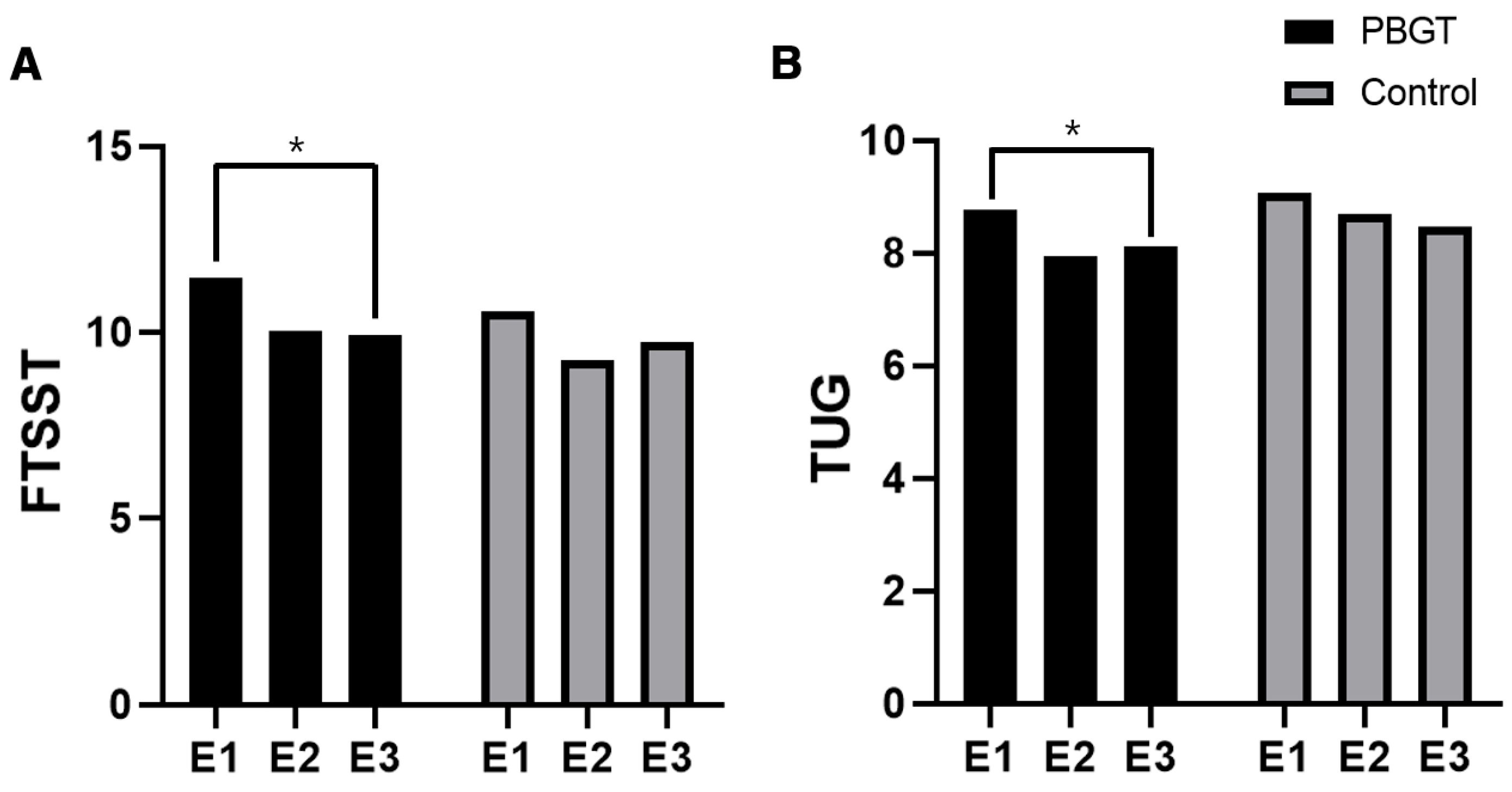
3.2. Outcomes
3.3. Safety Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dellinger, A.M.; Stevens, J.A. The injury problem among older adults: Mortality, morbidity and costs. J. Saf. Res. 2006, 37, 519–522. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk factors for falls among older adults: A review of the literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Auais, M.; Alvarado, B.; Guerra, R.; Curcio, C.; Freeman, E.E.; Ylli, A.; Guralnik, J.; Deshpande, N. Fear of falling and its association with life-space mobility of older adults: A cross-sectional analysis using data from five international sites. Age Ageing 2017, 46, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Florence, C.S.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. Medical costs of fatal and nonfatal falls in older adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Fairhall, N.; Wallbank, G.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S. Exercise for preventing falls in older people living in the community: An abridged Cochrane systematic review. Br. J. Sports Med. 2020, 54, 885–891. [Google Scholar] [CrossRef]
- Sherrington, C.; Michaleff, Z.A.; Fairhall, N.; Paul, S.S.; Tiedemann, A.; Whitney, J.; Cumming, R.G.; Herbert, R.D.; Close, J.C.T.; Lord, S.R. Exercise to prevent falls in older adults: An updated systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1750–1758. [Google Scholar] [CrossRef]
- Sherrington, C.; Fairhall, N.; Kwok, W.; Wallbank, G.; Tiedemann, A.; Michaleff, Z.A.; Ng, C.A.C.M.; Bauman, A. Evidence on physical activity and falls prevention for people aged 65+ years: Systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 144. [Google Scholar] [CrossRef]
- Mansfield, A.; Wong, J.S.; Bryce, J.; Knorr, S.; Patterson, K.K. Does perturbation-based balance training prevent falls? Systematic review and meta-analysis of preliminary randomized controlled trials. Phys. Ther. 2015, 95, 700–709. [Google Scholar] [CrossRef]
- Park, J.M.; Kim, Y.W.; Lee, S.J.; Shin, J.C. Robot-assisted gait training in individuals with spinal cord injury: A systematic review and meta-analysis of randomized controlled trials. Ann. Rehabil. Med. 2024, 48, 171–191. [Google Scholar] [CrossRef]
- Lurie, J.D.; Zagaria, A.B.; Pidgeon, D.M.; Forman, J.L.; Spratt, K.F. Pilot comparative effectiveness study of surface perturbation treadmill training to prevent falls in older adults. BMC Geriatr. 2013, 13, 49. [Google Scholar] [CrossRef]
- Patel, P.; Bhatt, T. Adaptation to large-magnitude treadmill-based perturbations: Improvements in reactive balance response. Physiol. Rep. 2015, 3, e12247. [Google Scholar] [CrossRef] [PubMed]
- Darter, B.J.; Labrecque, B.A.; Perera, R.A. Dynamic stability during split-belt walking and the relationship with step length symmetry. Gait Posture 2018, 62, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Altman, A.R.; Reisman, D.S.; Higginson, J.S.; Davis, I.S. Kinematic comparison of split-belt and single-belt treadmill walking and the effects of accommodation. Gait Posture 2012, 35, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Obuchi, S.; Furuna, T.; Suzuki, T. New intervention program for preventing falls among frail elderly people: The effects of perturbed walking exercise using a bilateral separated treadmill. Am. J. Phys. Med. Rehabil. 2004, 83, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.S.; Kim, J.H.; Yong, S.Y.; Lee, Y.H.; Kim, S.H.; Park, J.Y.; Lee, J.K.; Jang, J.Y. Preliminary clinical trial of balance compensation system for improvement of balance in patients with spinocerebellar ataxia. Ann. Rehabil. Med. 2020, 44, 284–291. [Google Scholar] [CrossRef]
- Eggenberger, P.; Theill, N.; Holenstein, S.; Schumacher, V.; de Bruin, E.D. Multicomponent physical exercise with simultaneous cognitive training to enhance dual-task walking of older adults: A secondary analysis of a 6-month randomized controlled trial with 1-year follow-up. Clin. Interv. Aging 2015, 10, 1711–1732. [Google Scholar] [CrossRef]
- Lord, S.R.; Murray, S.M.; Chapman, K.; Munro, B.; Tiedemann, A. Sit-to-stand performance depends on sensation, speed, balance, and psychological status in addition to strength in older people. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M539–M543. [Google Scholar] [CrossRef]
- Whitney, S.L.; Wrisley, D.M.; Marchetti, G.F.; Gee, M.A.; Redfern, M.S.; Furman, J.M. Clinical measurement of sit-to-stand performance in people with balance disorders: Validity of data for the five-times-sit-to-stand test. Phys. Ther. 2005, 85, 1034–1045. [Google Scholar] [CrossRef]
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional reach: A new clinical measure of balance. J. Gerontol. 1990, 45, M192–M197. [Google Scholar] [CrossRef]
- Chiaramonte, R.; D’Amico, S.; Caramma, S.; Grasso, G.; Pirrone, S.; Ronsisvalle, M.G.; Bonfiglio, M. The effectiveness of goal-oriented dual task proprioceptive training in subacute stroke: A retrospective observational study. Ann. Rehabil. Med. 2024, 48, 31–41. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the probability for falls in community-dwelling older adults using the timed UP & go test. Phys. Ther. 2000, 80, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Psych, A.P. A systematic review of the effects of perturbation training on preventing falls. N. Z. J. Physiother. 2017, 45, 31–49. [Google Scholar]
- McCrum, C.; Gerards, M.H.; Karamanidis, K.; Zijlstra, W.; Meijer, K. A systematic review of gait perturbation paradigms for improving reactive stepping responses and falls risk among healthy older adults. Eur. Rev. Aging Phys. Act. 2017, 14, 3. [Google Scholar] [CrossRef] [PubMed]
- Pai, Y.C.; Bhatt, T.S. Repeated-slip training: An emerging paradigm for prevention of slip-related falls among older adults. Phys. Ther. 2007, 87, 1478–1491. [Google Scholar] [CrossRef]
- Pai, Y.C.; Bhatt, T.; Yang, F.; Wang, E. Perturbation training can reduce community-dwelling older adults’ annual fall risk: A randomized controlled trial. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 1586–1594. [Google Scholar] [CrossRef]
- Lee, A.; Bhatt, T.; Pai, Y.C. Generalization of treadmill perturbation to overground slip during gait: Effect of different perturbation distances on slip recovery. J. Biomech. 2016, 49, 149–154. [Google Scholar] [CrossRef]
- Nørgaard, J.E.; Andersen, S.; Ryg, J.; Stevenson, A.J.; Andreasen, J.; Oliveira, A.S.; Danielsen, M.B.; Jorgensen, M.G. Effect of treadmill perturbation-based balance training on fall rates in community-dwelling older adults: A randomized clinical trial. JAMA Netw. Open 2023, 6, e238422. [Google Scholar] [CrossRef]
- McCrum, C.; Vaes, A.W.; Delbressine, J.M.; Koopman, M.; Liu, W.Y.; Willems, P.; Meijer, K.; Spruit, M.A. A pilot study on the feasibility and effectiveness of treadmill-based perturbations for assessing and improving walking stability in chronic obstructive pulmonary disease. Clin. Biomech. 2022, 91, 105538. [Google Scholar] [CrossRef]
- Moreland, J.D.; Richardson, J.A.; Goldsmith, C.H.; Clase, C.M. Muscle weakness and falls in older adults: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2004, 52, 1121–1129. [Google Scholar] [CrossRef]
- Ahn, B.R.; Kang, H.J.; Choi, E.J.; Jang, S.W.; Chung, H.S.; Jeon, K.S. Correlation of the Korean version of falls efficacy scale-international with quantitative balance and gait parameters through exercise program in elderly men. Ann. Rehabil. Med. 2019, 43, 195–203. [Google Scholar] [CrossRef]
- Smith, C.; Seematter-Bagnoud, L.; Santos-Eggimann, B.; Krief, H.; Bula, C.J. Executive function and prospective falls: A 6-year longitudinal study in community-dwelling older adults. BMC Geriatr. 2023, 23, 140. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Control Group a (n = 11) | PBGT Group a (n = 12) | p-Value | |
|---|---|---|---|
| Age | 73.00 ± 3.29 | 74.08 ± 3.55 | 0.458 b |
| Sex (male:female) | 6:5 | 5:7 | 0.537 c |
| FTSST | 11.46 ± 2.90 | 10.55 ± 3.60 | 0.512 d |
| KFES-I | 18.17 ± 1.03 | 17.36 ± 0.67 | 0.064 b |
| TUG | 8.77 ± 1.61 | 9.06 ± 1.86 | 0.693 d |
| FRT | 17.56 ± 6.52 | 21.28 ± 5.92 | 0.168 b |
| PBGT a | Control a | PBGT vs. Control b | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| E1 | E2 | E3 | p c (d) d | E1 | E2 | E3 | p (d) | Time p (d) | Group p (d) | Time × Group p (d) | |
| FTSST | 11.46 ± 2.90 | 10.06 ± 2.07 | 9.94 ± 2.03 | <0.001 (0.504) | 10.55 ± 3.60 | 9.24 ± 1.72 | 9.73 ± 2.85 | 0.255 (0.128) | 0.004 (0.230) | 0.515 (0.020) | 0.659 (0.020) |
| KFES-I | 18.17 ± 1.03 | 17.67 ± 1.37 | 17.50 ± 1.09 | 0.061 e (0.255) f | 17.36 ± 0.67 | 17.00 ± 1.18 | 16.64 ± 1.03 | 0.087 e (0.204) f | – | – | – |
| TUG | 8.77 ± 1.61 | 7.94 ± 0.99 | 8.11 ± 1.08 | 0.011 (0.335) | 9.06 ± 1.86 | 8.69 ± 1.17 | 8.47 ± 1.49 | 0.679 (0.092) | 0.021 (0.169) | 0.366 (0.039) | 0.593 (0.025) |
| FRT | 17.56 ± 6.52 | 19.33 ± 6.39 | 17.35 ± 5.95 | 0.242 (0.123) | 21.28 ± 5.92 | 20.68 ± 5.62 | 20.40 ± 5.14 | 0.768 (0.026) | 0.442 (0.038) | 0.247 (0.063) | 0.387 (0.044) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, K.-S.; Ko, M.-H. Effects of Unpredictable Perturbation Training on a Split-Belt Treadmill on Physical Performance in Older Adults: A Randomized Controlled Trial. Geriatrics 2025, 10, 23. https://doi.org/10.3390/geriatrics10010023
Han K-S, Ko M-H. Effects of Unpredictable Perturbation Training on a Split-Belt Treadmill on Physical Performance in Older Adults: A Randomized Controlled Trial. Geriatrics. 2025; 10(1):23. https://doi.org/10.3390/geriatrics10010023
Chicago/Turabian StyleHan, Kap-Soo, and Myoung-Hwan Ko. 2025. "Effects of Unpredictable Perturbation Training on a Split-Belt Treadmill on Physical Performance in Older Adults: A Randomized Controlled Trial" Geriatrics 10, no. 1: 23. https://doi.org/10.3390/geriatrics10010023
APA StyleHan, K.-S., & Ko, M.-H. (2025). Effects of Unpredictable Perturbation Training on a Split-Belt Treadmill on Physical Performance in Older Adults: A Randomized Controlled Trial. Geriatrics, 10(1), 23. https://doi.org/10.3390/geriatrics10010023