1. Introduction
The human heart exhibits remarkable vitality, beating approximately 100,000 times each day, totaling 30 million beats annually, and a staggering 2.5 billion times over the course of an average lifetime [
1]. Despite being just slightly larger than a clenched fist, it demonstrates incredible efficiency by pumping around 7000 L of blood daily, 2.5 million liters yearly, and 200 million liters throughout an individual’s lifespan [
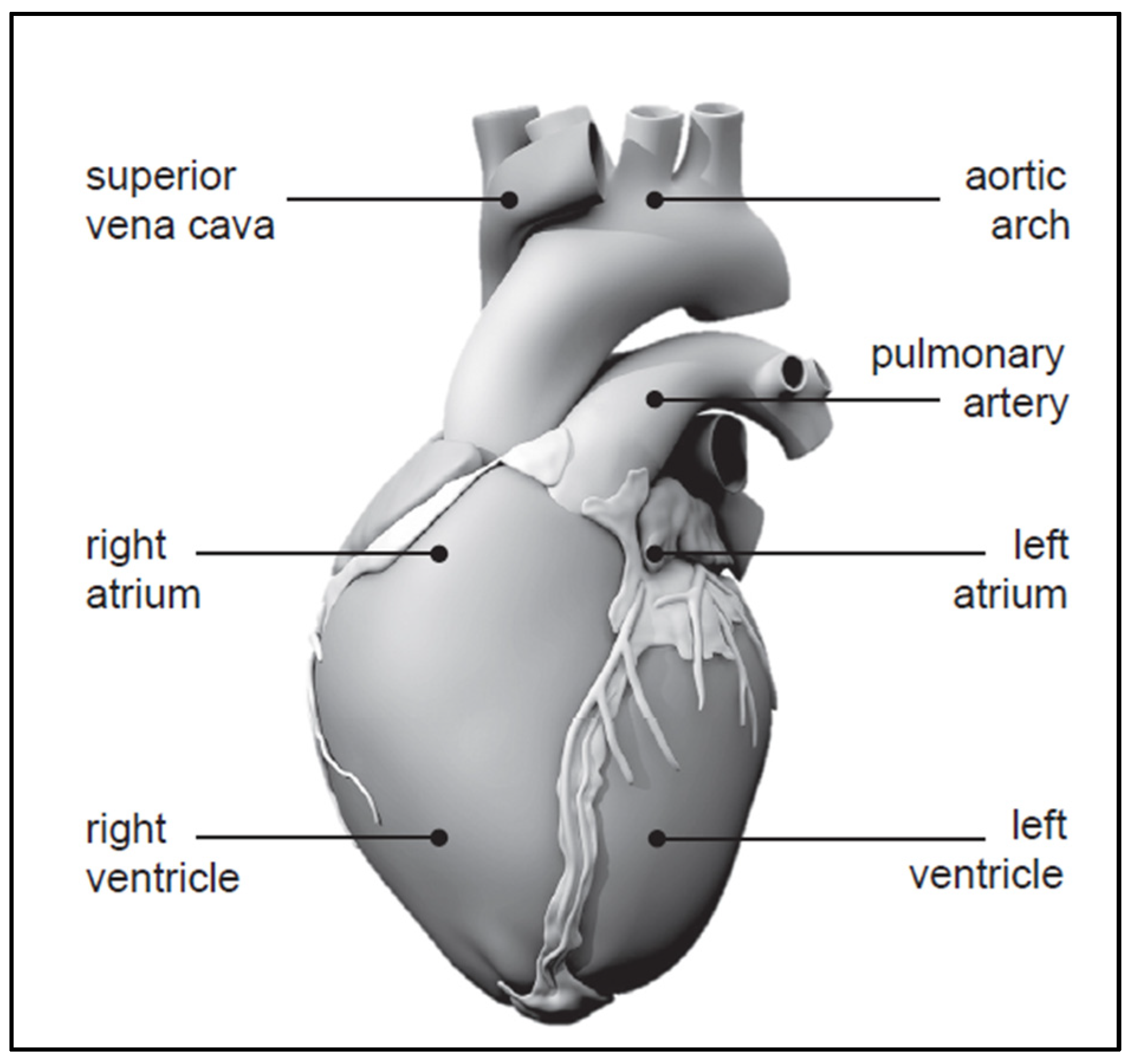
2]. An anatomical model of the human heart, constructed from computer tomography and magnetic resonance images, is depicted in
Figure 1 [
3,
4].
The synchronized opening and closing of these valves, orchestrated by a combination of electrical and mechanical forces, ensures proper chamber filling and ejection. Any disruption, such as valve malfunction or irregular electrical signals, can lead to serious conditions like arrhythmias or heart failure [
5]. Understanding the intricate relationship between electrical impulses and muscular contractions offers valuable insights into these complex cardiac phenomena, with the potential to revolutionize treatment for the millions afflicted by heart disease [
6].
The primary techniques and avenues for modeling cardiac electrophysiology (EP) involve employing mathematical models to replicate the EP dynamics of the myocardium [
7]. During the 1970s and 1980s, EP models predominantly relied on rule-based cellular automata, gradually transitioning to equation-based models encompassing cellular-level and tissue-level equations. At the cellular level, these equations adhere to the Hodgkin and Huxley formalism, characterizing cellular action potential and ionic currents through a system of nonlinear first-order ionic ordinary differential equations. Such equations delineate the kinetics of individual channels, pumps, exchangers, and their electrical interplays. Moreover, there is a growing adoption of Markov-type models to construct more biophysically grounded representations of ion channels. Data from patch-clamp experiments have facilitated the formulation of comprehensive mathematical frameworks for ionic currents, facilitating the development of highly precise EP models. These models are instrumental in simulating electrical activation patterns and conduction velocities of waves within the ventricular myocardium. They can be broadly estimated from electrocardiograms (ECG) or body surface potential maps (BSPM), or locally assessed via electrical activation maps (EAMs). Additionally, extracellular ion concentrations can be approximated and integrated into models based on measurements of blood electrolyte concentrations, albeit recognizing their significant temporal variability.
As leads used in cardiac implantable electronic devices age, the risk of malfunction increases, with reported malfunction rates reaching 40% after 8 years. This underscores the importance of assessing damage in cardiac devices, given the significant number of patients with cardiovascular diseases and implantable devices. The complexity of these devices presents challenges in damage assessment, but such analyses can provide valuable insights for improving future designs. Salih et al. [
8] examined various damage features of leads such as surface deformation, burnishing, pitting, scratching, discoloration, delamination, insulation defects, coil damage, and abrasion. The study highlights the importance of understanding common damage patterns in cardiac leads to improve future device designs. Salih and Goswami [
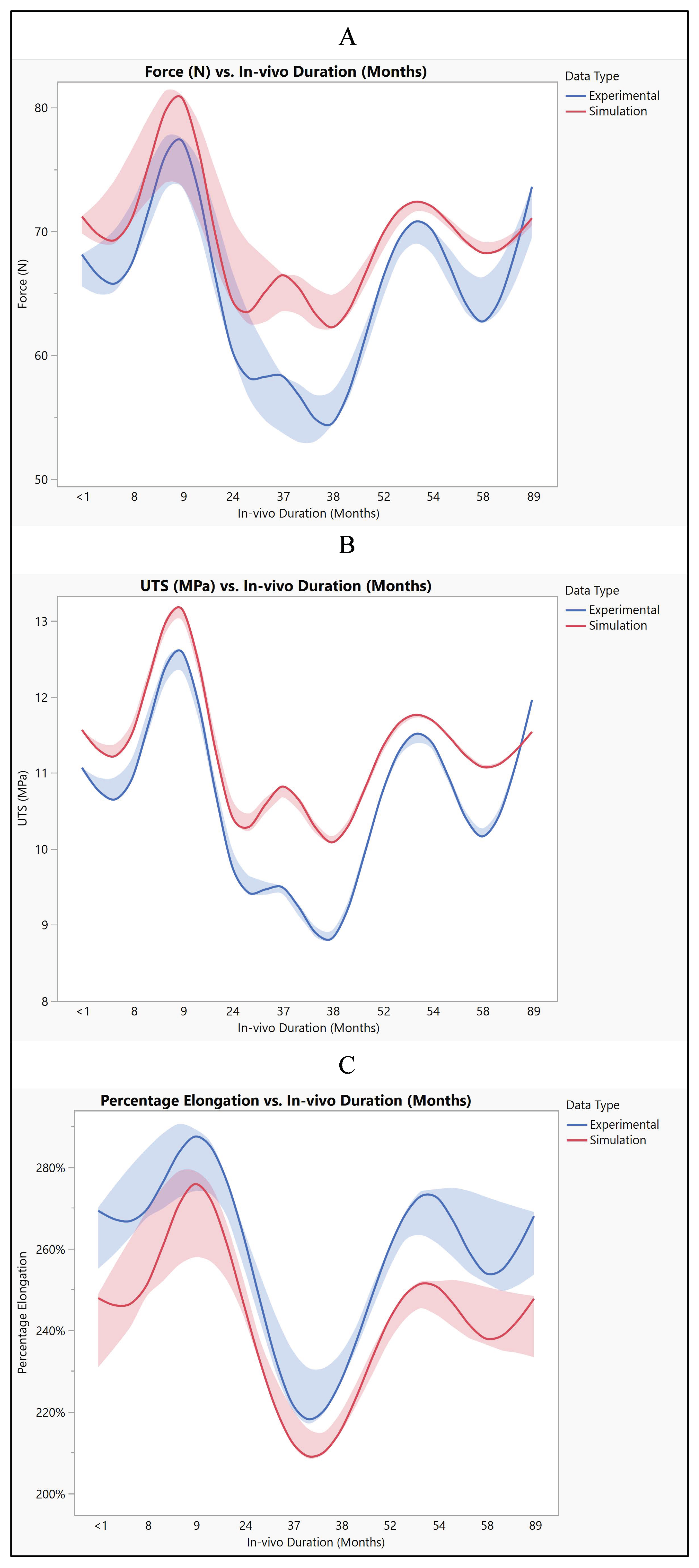
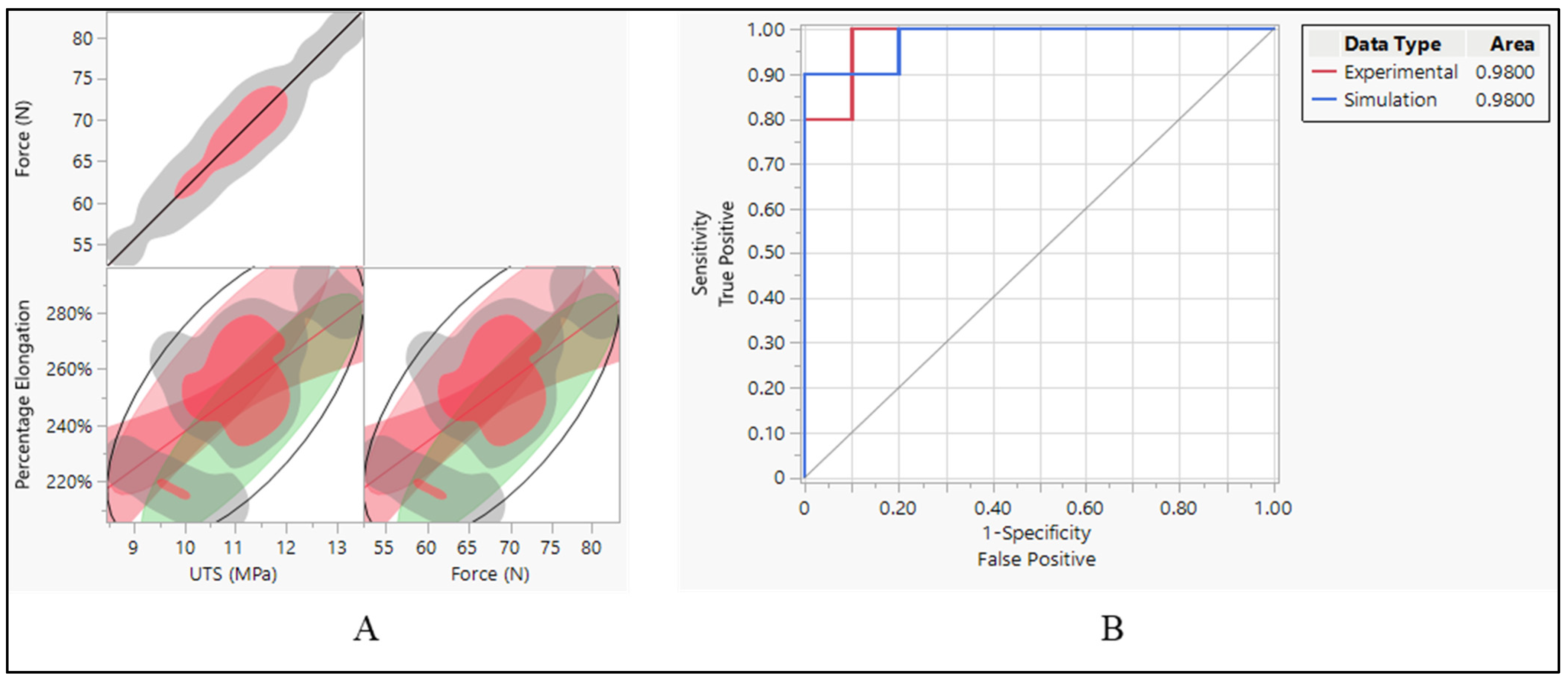
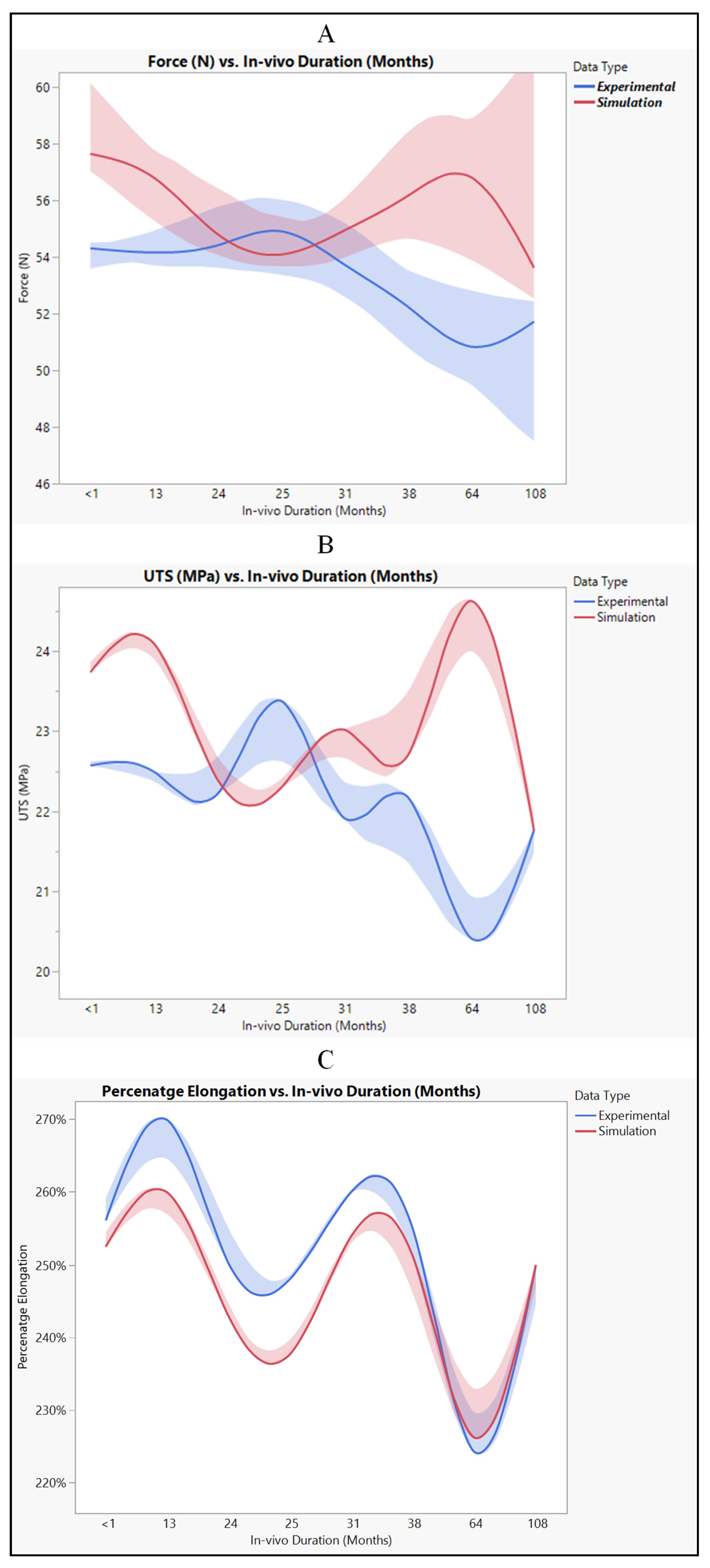
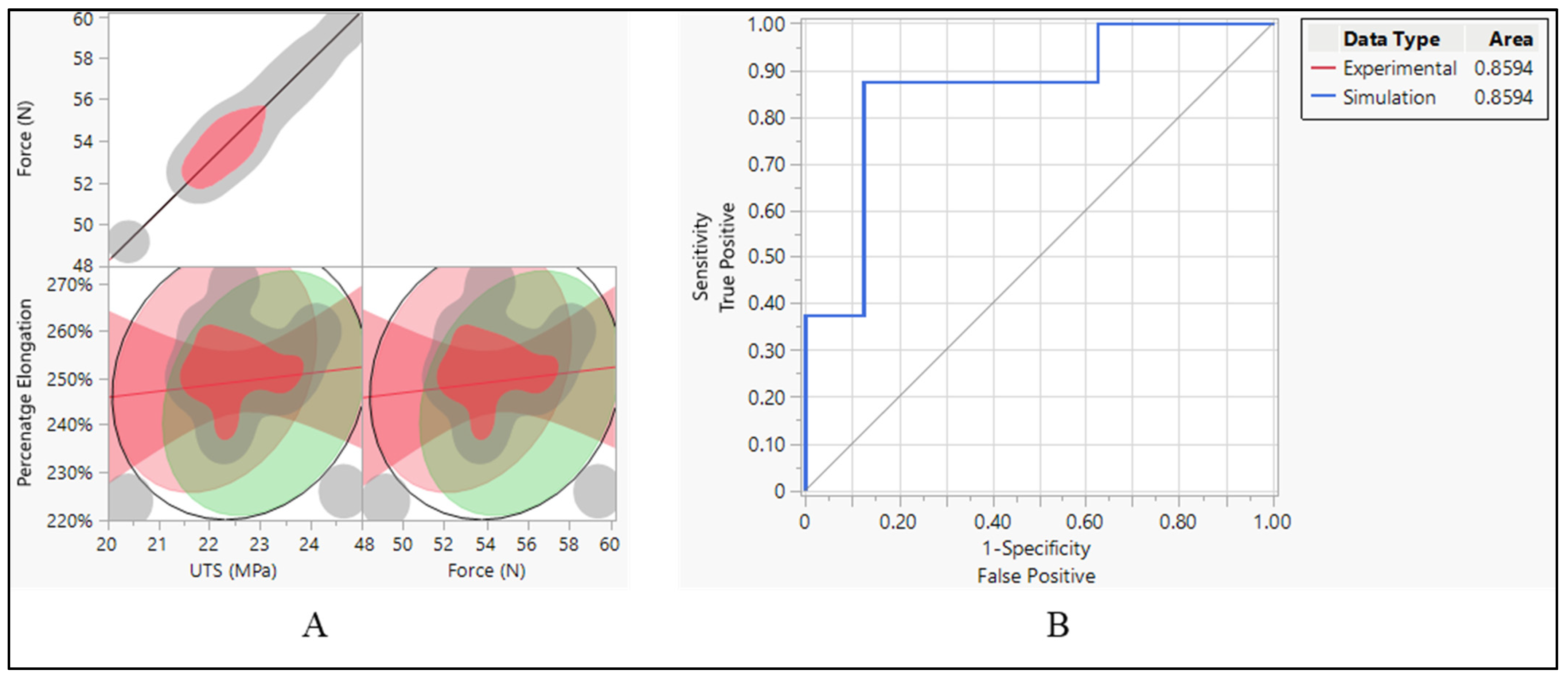
9] investigated the residual properties of silicone leads used in cardiac implantable electronic devices, comparing them with new leads. Results show significant decreases in load to failure, elongation to failure, ultimate tensile strength, and percentage elongation at 5 N after long-term in vivo exposure, while the modulus of elasticity increases over time. Recently, they examined leads using polyurethane and SI-polyimide as insulators, analyzing their mechanical properties after various durations of in vivo implantation [
10]. Results indicate no significant degradation in load to failure, elongation, ultimate tensile strength, or modulus of elasticity over time, except for a significant decrease in the percentage of elongation at 5 N force after 60 months. After experimental work, computational simulation is crucial to complement and enhance the understanding gained. While experiments provide valuable real-world data, they are often limited by factors such as cost, time, and complexity. Computational simulations can fill these gaps by providing a detailed, virtual representation of the system being studied. In the investigation of lead behavior in cardiac devices, computational simulations can help predict long-term performance and assess the impact of different materials and designs, offering insights that may not be feasible through experimentation alone.
The use of the finite element method (FEM) and computational fluid dynamics (CFD) modeling in cardiovascular device design and development is well-established. These methods enable engineers to simulate the behavior of cardiovascular devices in a controlled virtual environment, providing insights into their performance and helping to optimize their design. However, previous studies have limitations that our work addresses, making it important in the field.
Morris et al. [
11] highlighted the significance of computational fluid dynamics modeling in cardiovascular medicine, emphasizing its role in improving device safety and effectiveness. While their work advanced the understanding of cardiovascular device behavior, it may have been limited in addressing specific device design challenges. Tourek et al. [
12] reviewed cardiac pacemaker lead designs for computational models in a VR environment, showcasing the impact of FEM modeling on pacemaker design optimization. However, their focus may have been more on the virtual reality aspect rather than on the comprehensive analysis of lead performance over time, which is a critical factor in device durability and patient safety.
Additionally, Morris et al. [
13] demonstrated the utility of virtual fractional flow reserve from coronary angiography in modeling the significance of coronary lesions, indicating the potential of FEM and CFD modeling in optimizing coronary artery bypass graft surgery planning. Their work contributed to understanding the hemodynamic effects of coronary lesions, but it may not have fully explored the intricacies of device–tissue interactions that our study addresses. Furthermore, Gasser et al. [
14] proposed a novel strategy to translate the biomechanical rupture risk of abdominal aortic aneurysms to their equivalent diameter risk, highlighting the role of FEM and CFD modeling in aneurysm treatment planning. While their approach was innovative, it might not have delved deeply into the detailed analysis of device performance and material behavior, a key aspect that needed to be investigated.
Simon et al. [
15] conducted simulations of the three-dimensional hinge flow fields of a bi-leaflet mechanical heart valve (BMHV) under aortic conditions, focusing on the detrimental stresses on blood elements caused by these flows. Their study aimed to characterize these flows to identify underlying causes for thromboembolic complications associated with BMHVs. While their work contributed to improving heart valve design, particularly in understanding the flow patterns around the hinge, it may not have addressed the broader scope of device–organ interaction that our study encompasses. Jiménez and Davies [
16] demonstrated the hemodynamically driven stent strut design, emphasizing FEM modeling’s role in stent design optimization. However, their focus may have been more on stent geometry rather than on the comprehensive analysis of material properties and long-term performance.
Chiu et al. [
17] compared the thromboresistance of different ventricular assist devices (VADs), highlighting the impact of FEM and CFD modeling on blood pump design optimization. While their study contributed to improving blood pump design, particularly in understanding thrombogenic potential, it may not have fully explored the dynamic behavior of devices within the cardiovascular system. Chen et al. [
18] analyzed the fluid–structure interaction in a model of an L-Type Mg alloy stent-stenosed coronary artery system, demonstrating the use of FEM analysis in stent design optimization. While their study advanced stent design, it may not have addressed the comprehensive analysis of the device–tissue interaction.
In this study, three-dimensional models of cardiac leads and the heart were created using SolidWorks and MIMICS 25.0, while ANSYS Workbench 2022R1 was utilized for simulations. The cardiac leads were inserted into the heart 3D model, and simulations were run to investigate changes in lead behavior over time, ranging from new leads to more than 100 months of in vivo exposure. This work provides insights into the long-term performance of cardiac leads in vivo, comparing our findings with previous experimental work to enhance the robustness of our results and highlight the evolution of lead behavior under in vivo conditions. This comparative analysis adds depth to our understanding of lead performance and underscores the importance of our work in advancing the field of cardiac device design and optimization.
The objectives of this research endeavor encompass the development and validation of finite element models of cardiac device leads, aiming to create accurate representations of their mechanical behavior under various loading and stretching conditions. Through computational simulations, we seek to investigate the long-term performance of these leads in vivo, simulating the effects of in vivo implantation and physiological conditions to assess their durability and reliability. A crucial aspect involves comparing simulated results with experimental data to validate the accuracy of our computational models, thus ensuring their fidelity in representing real-world scenarios. Furthermore, we aim to optimize the design of cardiac devices for improved performance, leveraging insights gained from computational simulations to identify design enhancements and material optimizations. By exploring the impact of material properties on the mechanical behavior of cardiac device leads, we aim to enhance our understanding of their interaction with heart tissue and contribute to the advancement of cardiac device technology, ultimately striving to develop safer, more reliable, and longer-lasting cardiac device leads.
2. Materials and Methods
2.1. Computational Simulations
In our study, we employed advanced software tools to develop detailed three-dimensional models of both cardiac leads and the heart. Using SolidWorks, we constructed intricate models of cardiac leads, including a silicon pacing lead, a Polyurethane ICD lead, and a Polyurethane CRT lead. These models were designed to accurately represent the geometry and material properties of the leads used in cardiac implantable electronic devices.
Simultaneously, we utilized MIMICS 25.0 to create a three-dimensional model of the heart, incorporating its various components such as the myocardium, valves, chambers, and vessels. This detailed heart model was essential for simulating the interaction between the leads and the heart tissue realistically.
For conducting simulations, we employed ANSYS Workbench 2022R1, a powerful finite element analysis software. The heart model was meshed as nonlinear and quadratic to capture its complex mechanical behavior accurately. This meshing approach allowed us to simulate large deformations and material nonlinearity characteristic of soft tissues like the heart, ensuring the fidelity of our simulations.
The cardiac leads were then inserted into the heart model, and simulations were run to investigate how the leads behaved over time. By analyzing changes in lead behavior, we gained valuable insights into the long-term performance of cardiac leads in vivo. This aspect of our study is crucial for understanding how leads interact with the heart tissue and how their mechanical properties may change over time, providing valuable information for improving the design and durability of cardiac implantable electronic devices.
2.2. Geometry Creation
Three-dimensional models of the cardiac leads: silicon pacing lead (d = 2 mm), Polyurethane ICD lead (d = 2.8 mm), and Polyurethane CRT lead (d = 1.75 mm) were constructed using SolidWorks (Dassault Systèmes SolidWorks Corp., Concord, MA, USA) and imported in ANSYS Workbench 2022R1 (ANSYS Inc., Canonsburg, PA, USA) to simulate the loading conditions and regions of stress development. The heart and its attached vessels were modeled as well. Firstly, imaging data of a healthy heart and its surrounding vessels were taken from DICOM Image Library [
19]. Secondly, MIMICS 25.0 program was employed to convert the imaging data into a 3D model, following the same procedure used in our previous modeling [
20], allowing for the differentiation between the various components of the heart, including the myocardium, mitral valve, tricuspid valve, aortic valve, pulmonary valve, left atrium, right atrium, left ventricle, right ventricle, ascending aorta, aortic arch, descending aorta, pulmonary artery, superior vena cava, inferior vena cava, and coronary arteries, as shown in
Figure 2. This process involved segmenting the different structures based on their densities and anatomical features [
21]. By segmenting the different structures based on their densities and anatomical features, we were able to create a detailed and realistic 3D model that accurately represented the complex geometry of the heart and its associated vasculature. This detailed model was essential for conducting accurate simulations and investigating the behavior of the cardiac leads in vivo. Finally, the 3D model was refined and optimized using SolidWorks. This step allowed for the incorporation of finer details and adjustments to ensure the model accurately represented the structure and mechanical properties of the heart and its attached vessels. The final model would therefore include both the external features of the heart and vessels as well as internal structures in the myocardium and the layers of the vessel walls. After constructing the models, the leads were inserted into the heart model, as shown in
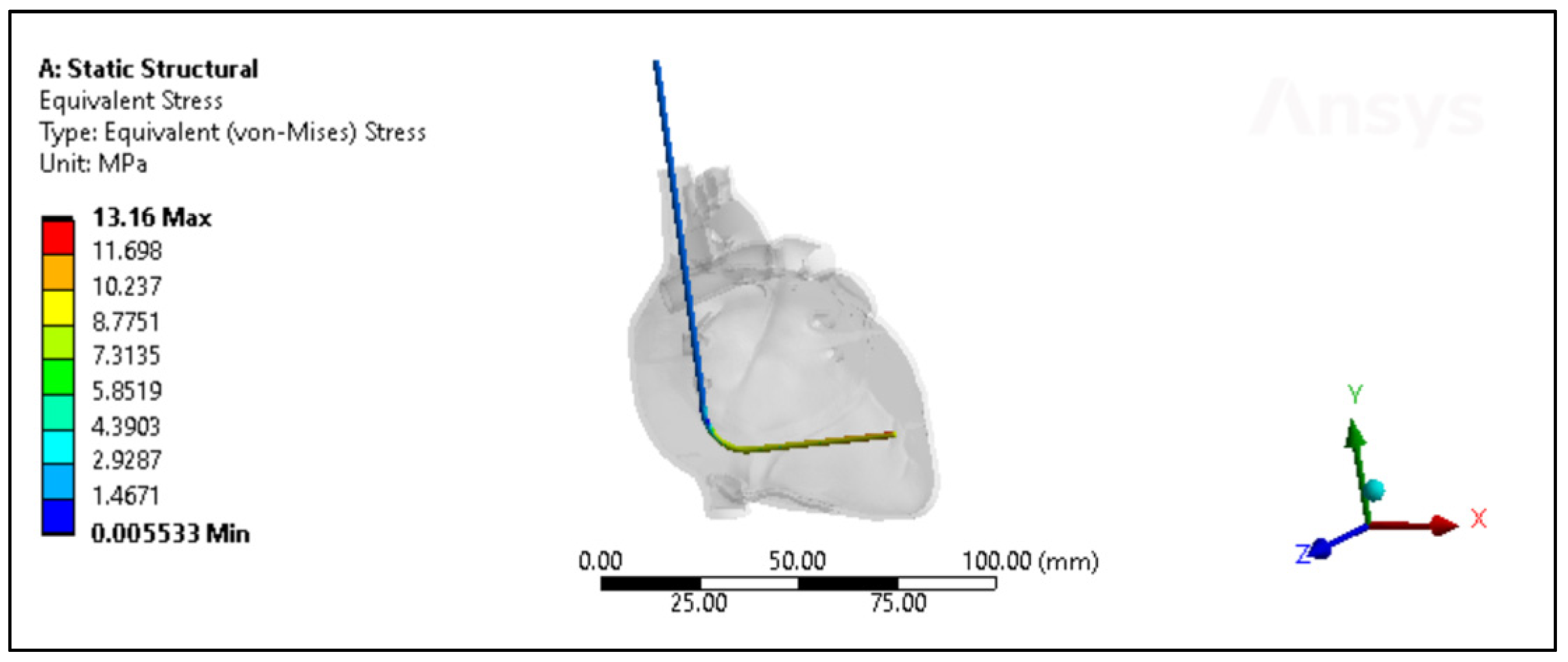
Figure 3. The lead is then inserted into the right ventricle and the tip of the lead was fixed near the septal area near the apex, as shown in
Figure 4.
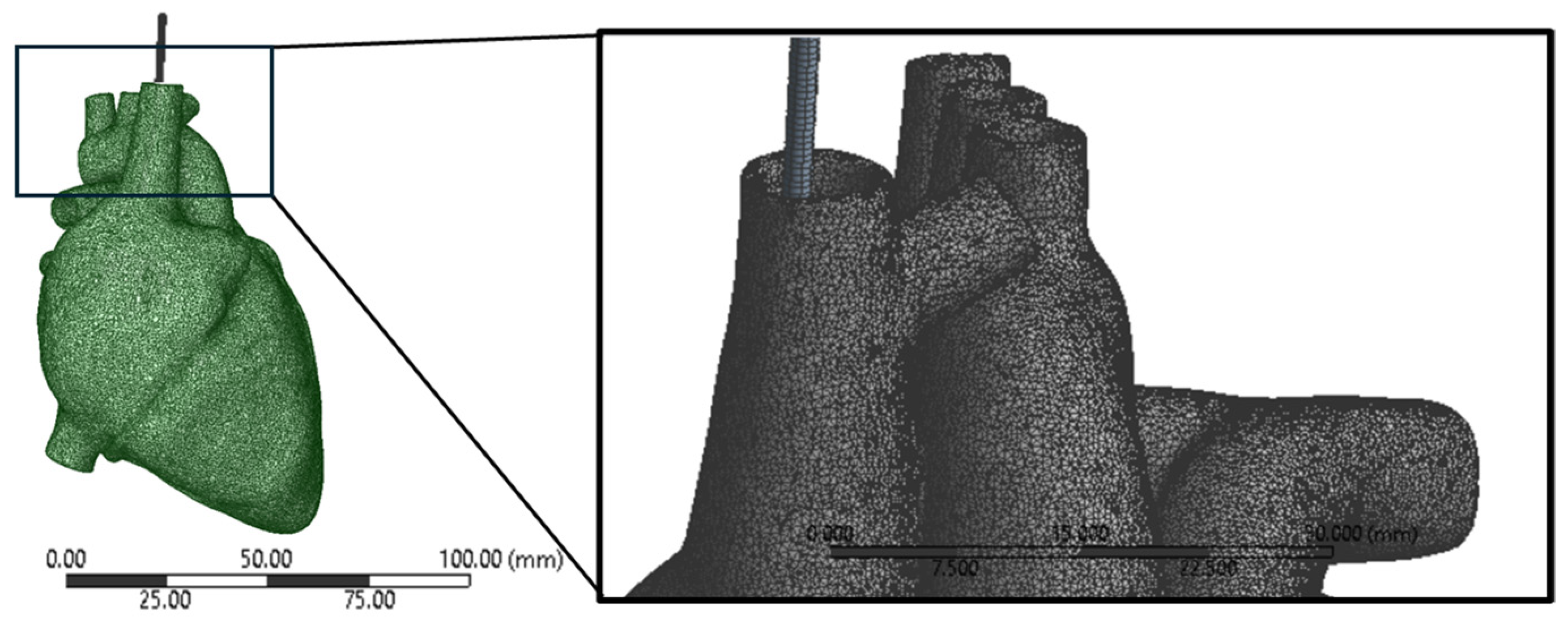
2.3. Finite Element Meshing
The mesh of the heart was configured as nonlinear and quadratic. This setup was chosen to accurately capture the complex behavior of the heart tissue under various loading conditions. Nonlinear elements allow for the simulation of large deformations and material nonlinearity, which are characteristic of soft tissues like the heart. The quadratic mesh type enhances the accuracy of the simulation by using higher-order interpolation functions for the elements, providing a more detailed representation of the geometry, and reducing numerical errors. This combination of nonlinear and quadratic meshing ensured that the simulation accurately captured the mechanical response of the heart tissue, enhancing the reliability and precision of the results. A mesh size of 0.5 mm was selected for both the heart and lead geometry as shown in
Figure 5. This choice aimed to strike a balance between accuracy and computational efficiency. Each element in the mesh had a characteristic size of 0.5 mm, enabling the capture of complex geometrical features while maintaining manageable computational costs. A smaller mesh size would have provided more detailed geometry representation but at a higher computational expense. Conversely, a larger mesh size would have reduced computational costs but could have led to less accurate results, particularly in regions with intricate geometry or high stress gradients. By using the 0.5 mm mesh size, the simulation could accurately depict the behavior of the lead within the heart, ensuring meaningful and reliable results.
In this study, mesh convergence checks were performed to assess the sensitivity of the simulation results to changes in the mesh density. The number of elements and nodes in the mesh directly impacts the accuracy of the simulation, with finer meshes generally providing more accurate results but requiring more computational resources. The total number of elements and nodes for each model, including the heart with different leads, was carefully determined to ensure that the results were consistent within a five percent margin. This meant that further refinement of the mesh did not lead to significant changes in the results, indicating that the chosen mesh density was sufficient to capture the behavior of the system accurately. After performing mesh convergence checks, the total number of elements for the heart model with the pacing lead was 2,287,865, with 3,619,097 nodes. For the pacing lead itself, there were 4872 elements and 24,411 nodes. Correspondingly, the heart model alone consisted of 2,282,993 elements and 3,594,686 nodes. The total number of elements for the heart model with the ICD lead was 2,289,083, with 3,625,200 nodes. For the ICD lead itself, there were 6090 elements and 30,514 nodes. The total number of elements for the heart model with the CRT lead was 2,286,647, with 3,612,994 nodes. For the CRT lead itself, there were 3654 elements and 18,308 nodes, as shown in
Table 1. By refining the mesh using a smaller increment size, the simulation was able to accurately depict the complex interactions between the leads and the heart tissue, providing valuable insights into the long-term performance of the cardiac leads in vivo. The meticulous meshing process ensured that the models were robust and capable of providing meaningful and reliable results for further analysis and interpretation.
Table 2 shows the mesh convergence within a five percent margin for the polyurethane ICD lead inside the heart model with less than a month of in vivo exposure.
2.4. Material Assignment
The material properties of the new leads were assigned according to the ASTM standards D 1708-02a [
22] and D 412-06a [
23], which provide guidelines for determining the tensile properties of plastics and elastomers, respectively. These standards ensure that the material properties used in the simulation are based on well-established testing methodologies.
In contrast, the residual properties of the leads after in vivo exposure were derived from our previous experimental investigations [
9,
10]. These data were crucial for modeling the long-term behavior of the leads, as they reflects the actual performance of the leads after being implanted in patients for varying durations.
The in vivo implantation durations varied among the leads, ranging from new leads to 132 months. For pacing leads, the average in vivo duration was 55 ± 49 months, while for CRT leads, it ranged from less than a month to 108 months, with an average duration of 41 ± 31 months. ICD leads had in vivo durations ranging from less than a month to 89 months, with an average duration of 41 ± 27 months. These varying durations reflect the real-world conditions under which the leads are exposed to physiological stresses, and incorporating these data into the simulation ensures that the models accurately represent the behavior of the leads over time. The mechanical properties of cardiac muscle were crucial for accurately modeling its behavior under various mechanical loads and conditions in the ANSYS software 2022 R1. These properties were defined based on specific values: a Young’s elastic modulus of 80 kPa [
24], which represents the stiffness and resistance to deformation of the muscle; an ultimate tensile strength of 110 kPa [
24,
25], indicating the maximum stress the muscle can withstand before failure; and a Poisson’s ratio of 0.4 [
26], which shows the muscle’s tendency to contract laterally when stretched longitudinally. These properties were determined based on established values from the literature, ensuring that the model accurately represents the mechanical response of cardiac muscle. Incorporating these properties into the simulation allows for a more realistic representation of the behavior of the muscle under different loading conditions, providing valuable insights into its mechanical function and performance.
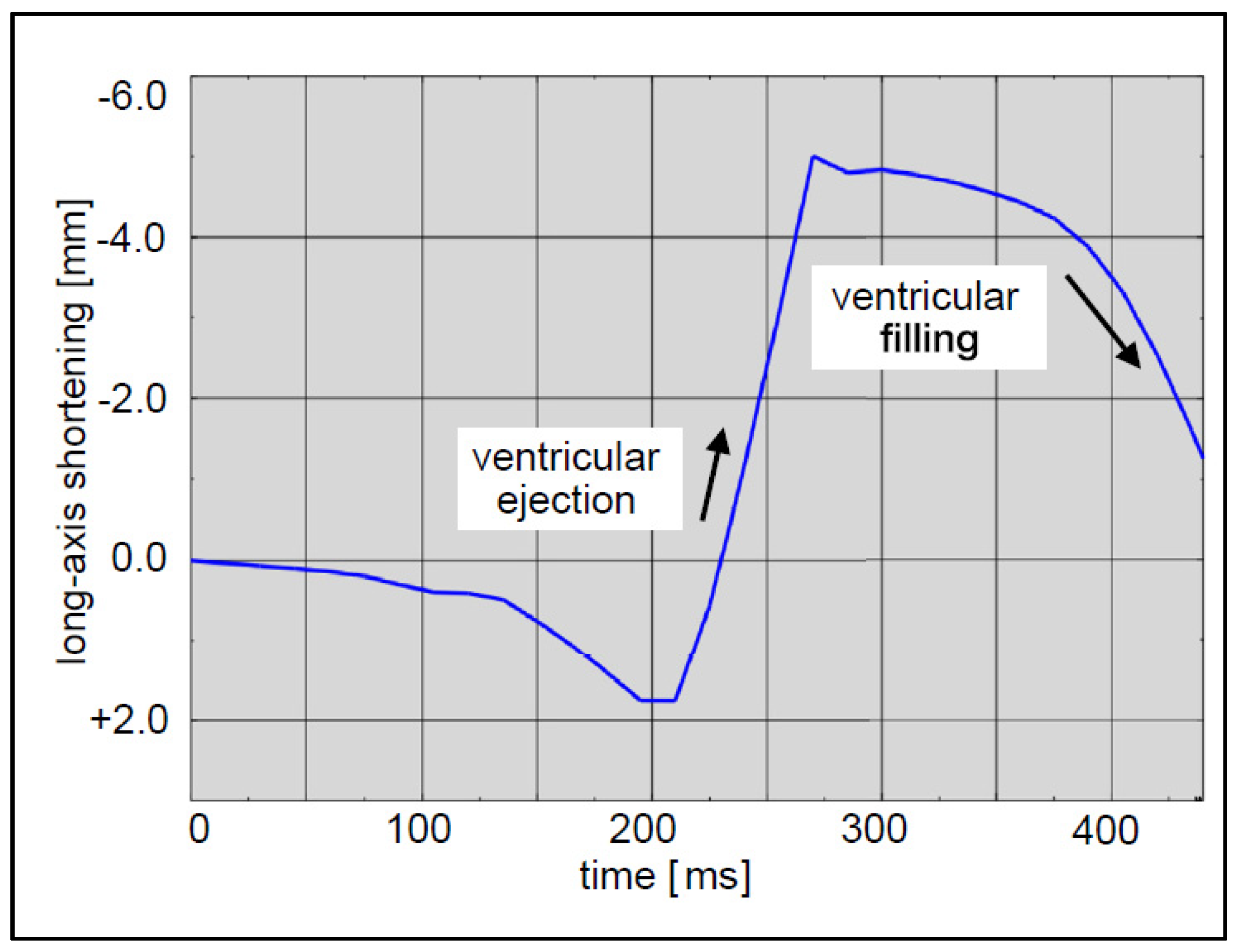
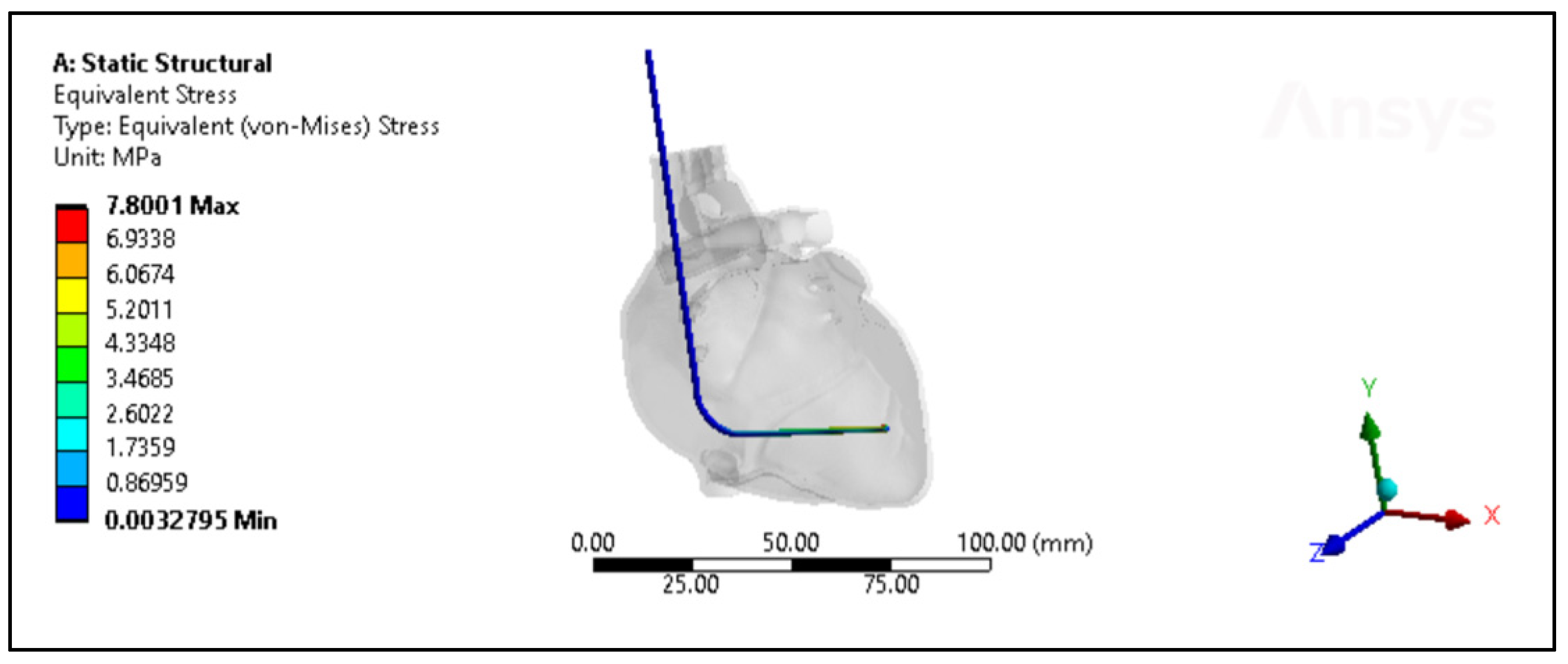
2.5. Loads and Boundary Conditions
In the simulation, the lead was fixed at its entry point into the heart to prevent unrealistic movement, representing its anchoring in reality. Other parts of the heart not in direct contact with the lead were also fixed to simulate the anchoring effect of surrounding tissues. To simulate the heartbeat, a displacement boundary condition was applied to the heart. This displacement was defined based on the expected motion of the heart during a cardiac cycle (
Figure 6), incorporating the dynamics of the heart’s long axis. During ventricular ejection, the distance between the apex and base decreased rapidly, and the ventricles shortened by approximately 7 mm. This shortening plateaued towards the end systole to ensure enough blood was ejected. During ventricular filling, the long axis gradually returned to its initial length as the heart muscle relaxed.
The interaction between the lead and heart tissue was defined using a frictional contact formulation to handle potential nonlinear behavior. Contact properties, with a friction coefficient = 0.5, were specified to represent the contact between lead and heart tissue. A fine mesh, approximately 0.1 mm near the contact interface, was used to capture the contact behavior accurately. The contact interface was carefully aligned with the tissue surface to prevent unrealistic contact behavior. Solver settings were adjusted to ensure proper resolution of the contact interactions, with a convergence criterion and monitoring of contact forces and displacements. The contact model was validated by comparing simulation results with experimental data or the published literature to verify the accuracy of the contact forces and displacements predicted by the simulation.
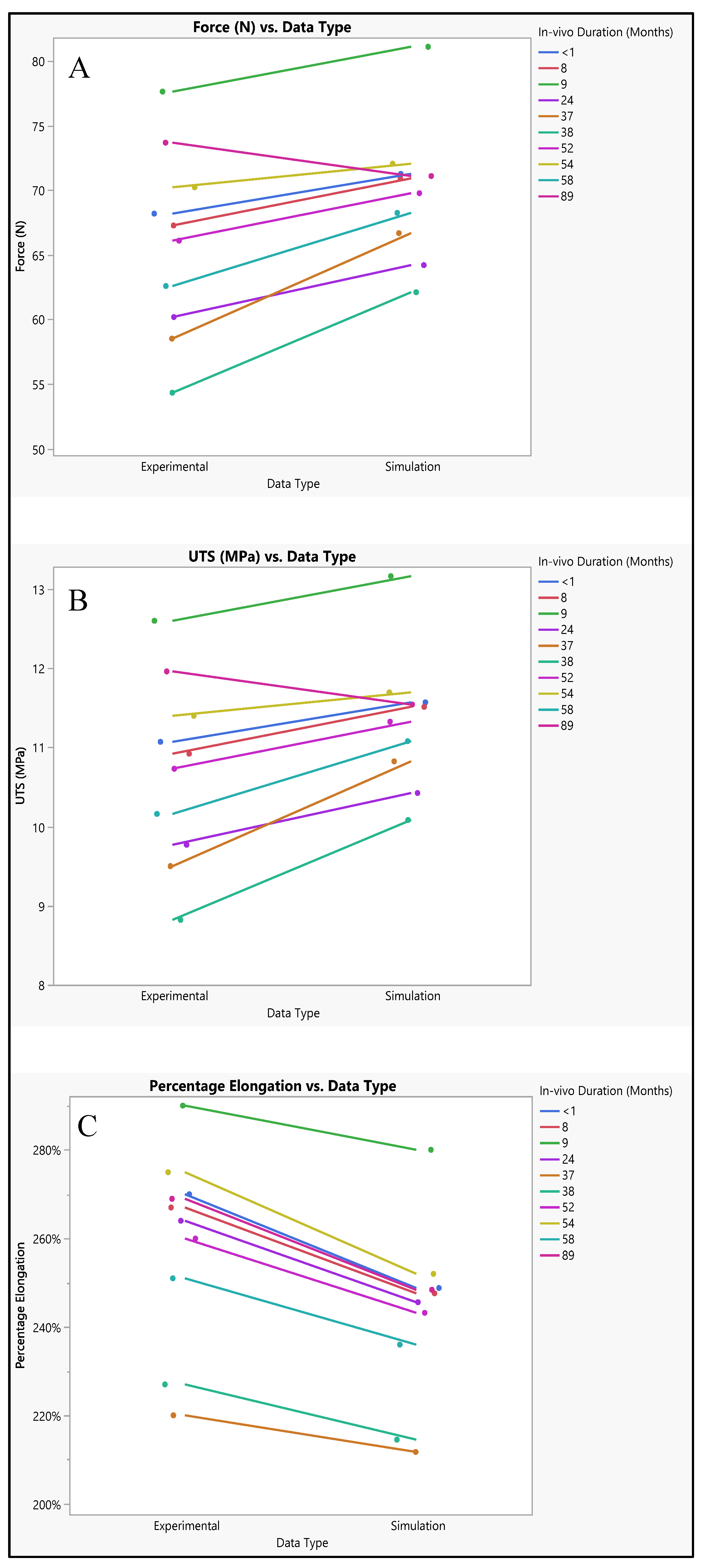
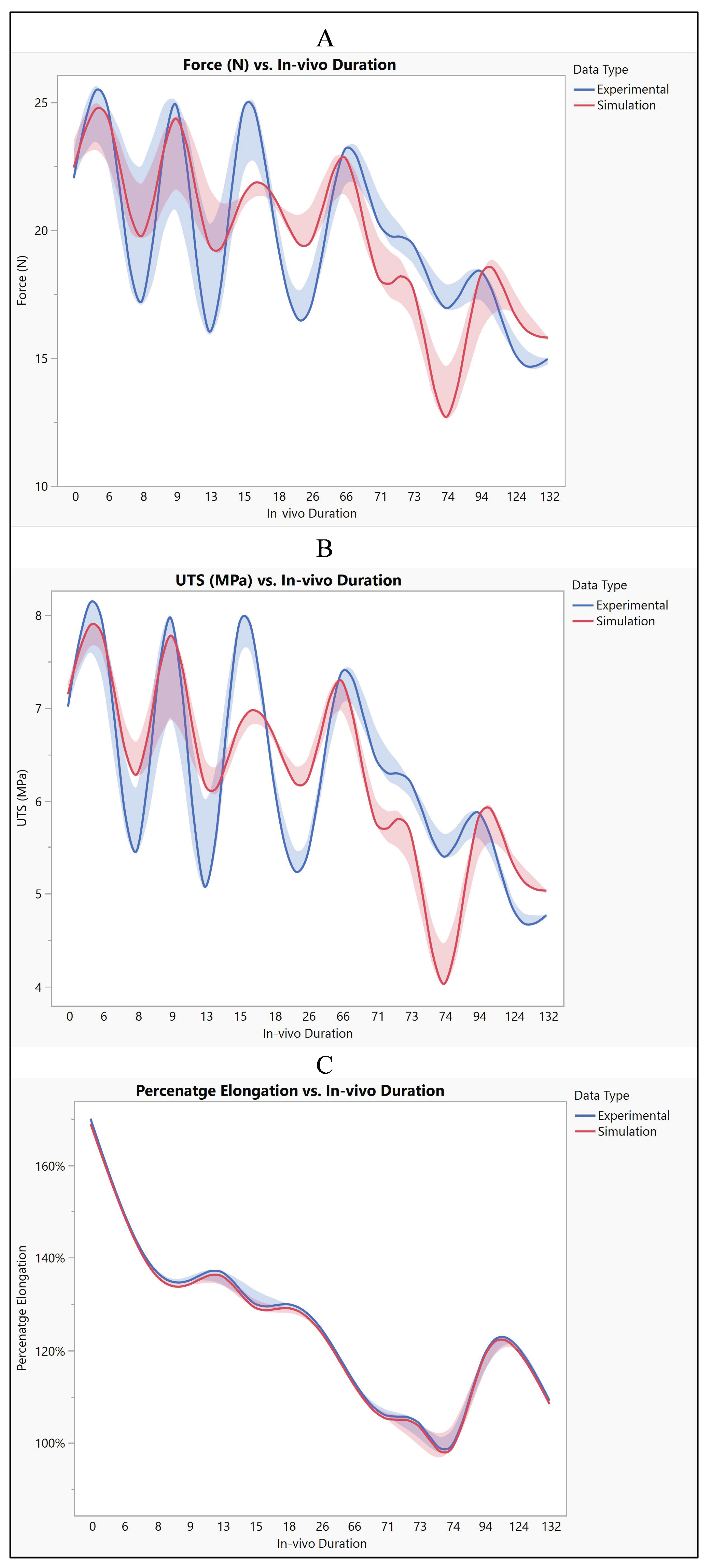
Multiple simulations were then performed on these models to investigate the change in the residual properties with respect to the in vivo implantation period of the leads. This involved applying the defined loads and boundary conditions to simulate the interaction between the leads and the heart tissue over time. The simulations aimed to analyze how the mechanical properties of the leads changed over time due to the effects of in vivo implantation, providing insights into the long-term performance and durability of the leads in a realistic physiological environment.















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}