
Comparative Analysis of Bone Regeneration According to Particle Type and Barrier Membrane for Octacalcium Phosphate Grafted into Rabbit Calvarial Defects

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Material Preparation
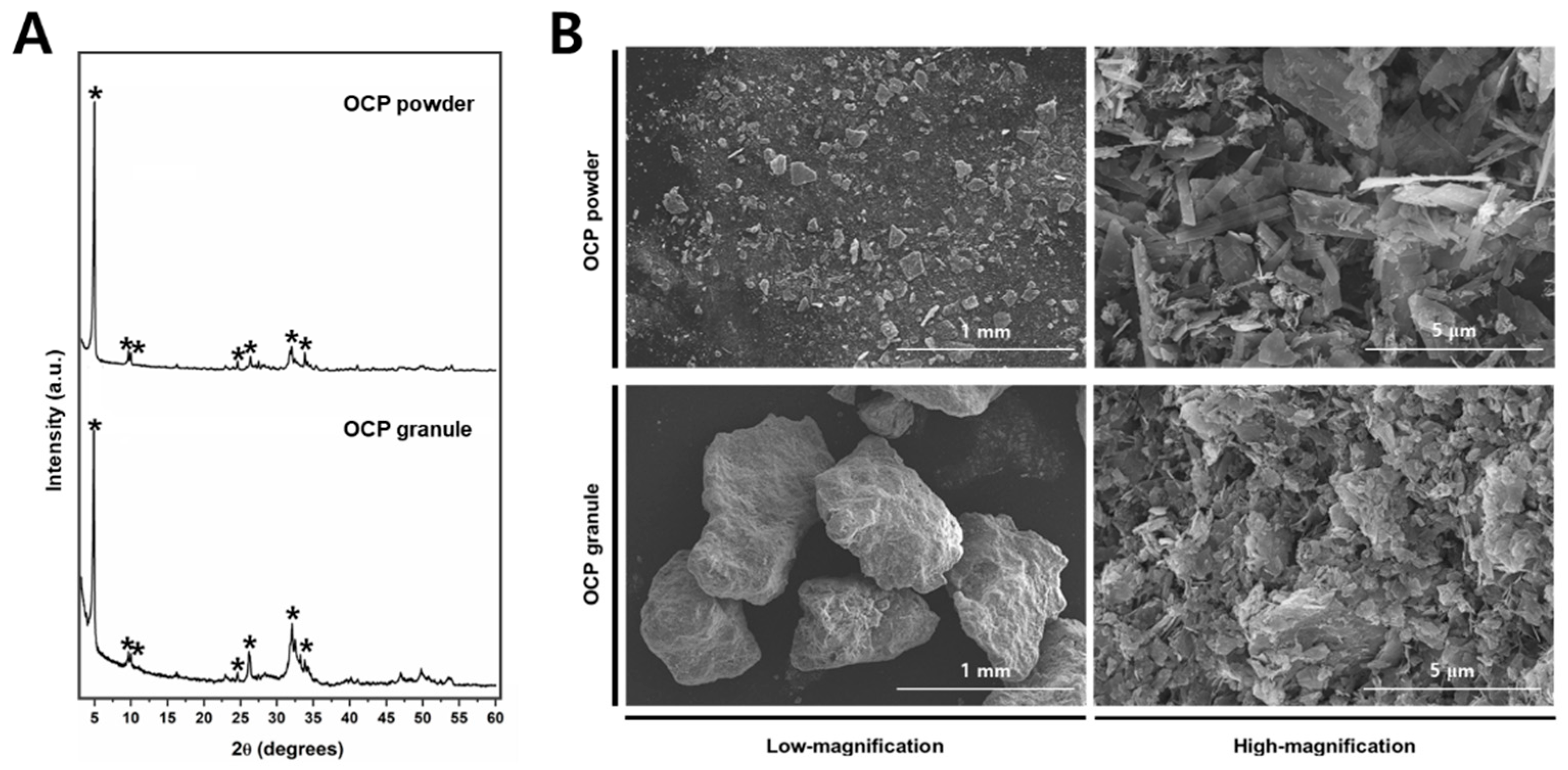
2.2. Material Characterization
2.3. Animals and Surgical Protocol
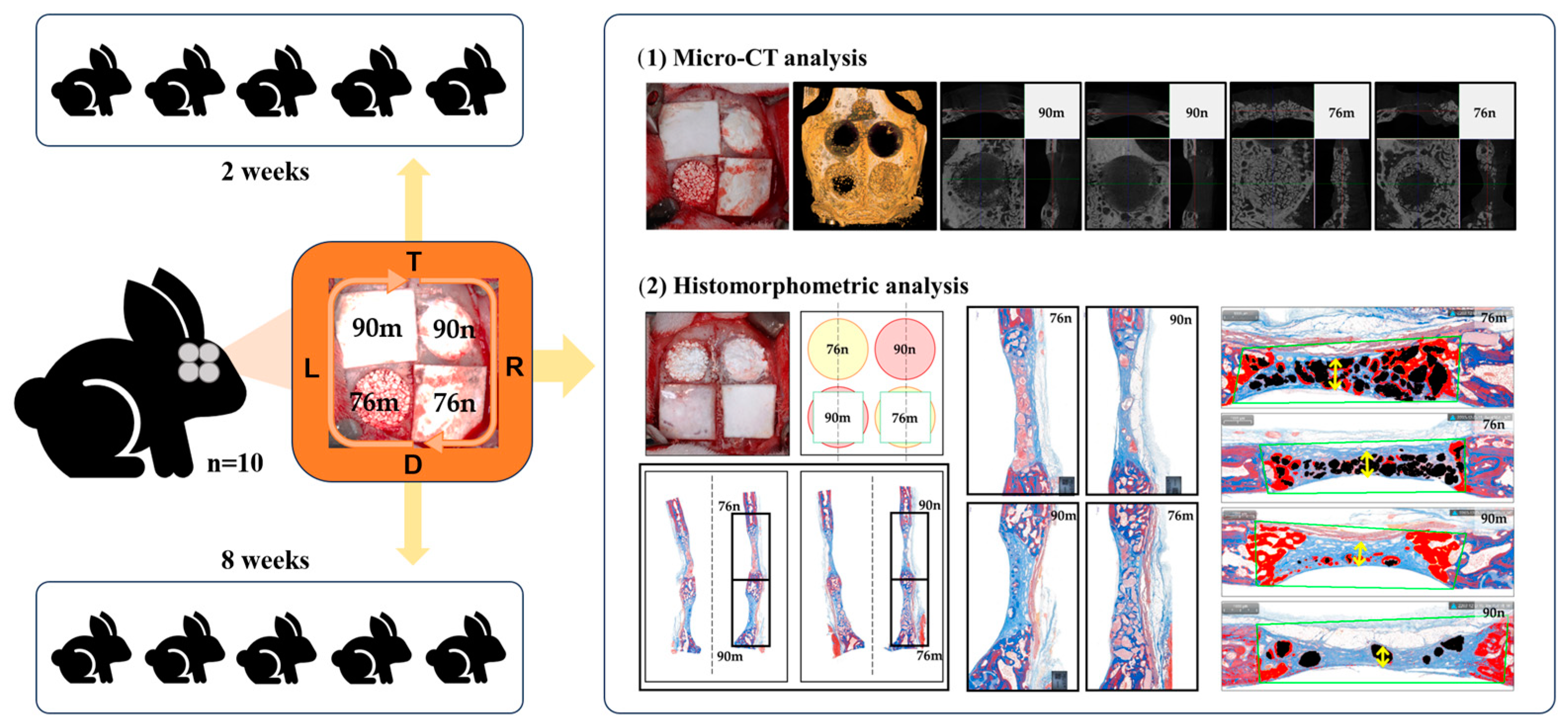
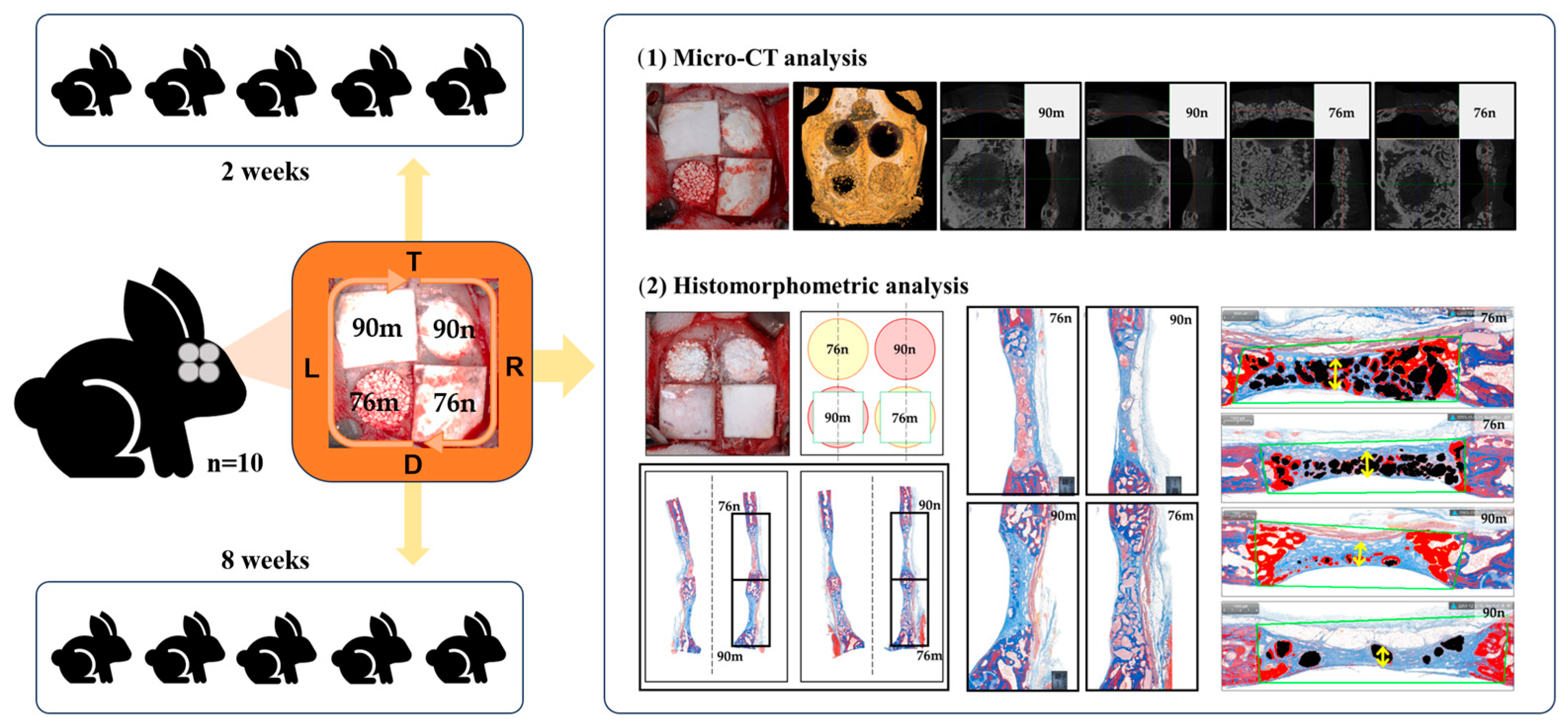
2.4. Study Design
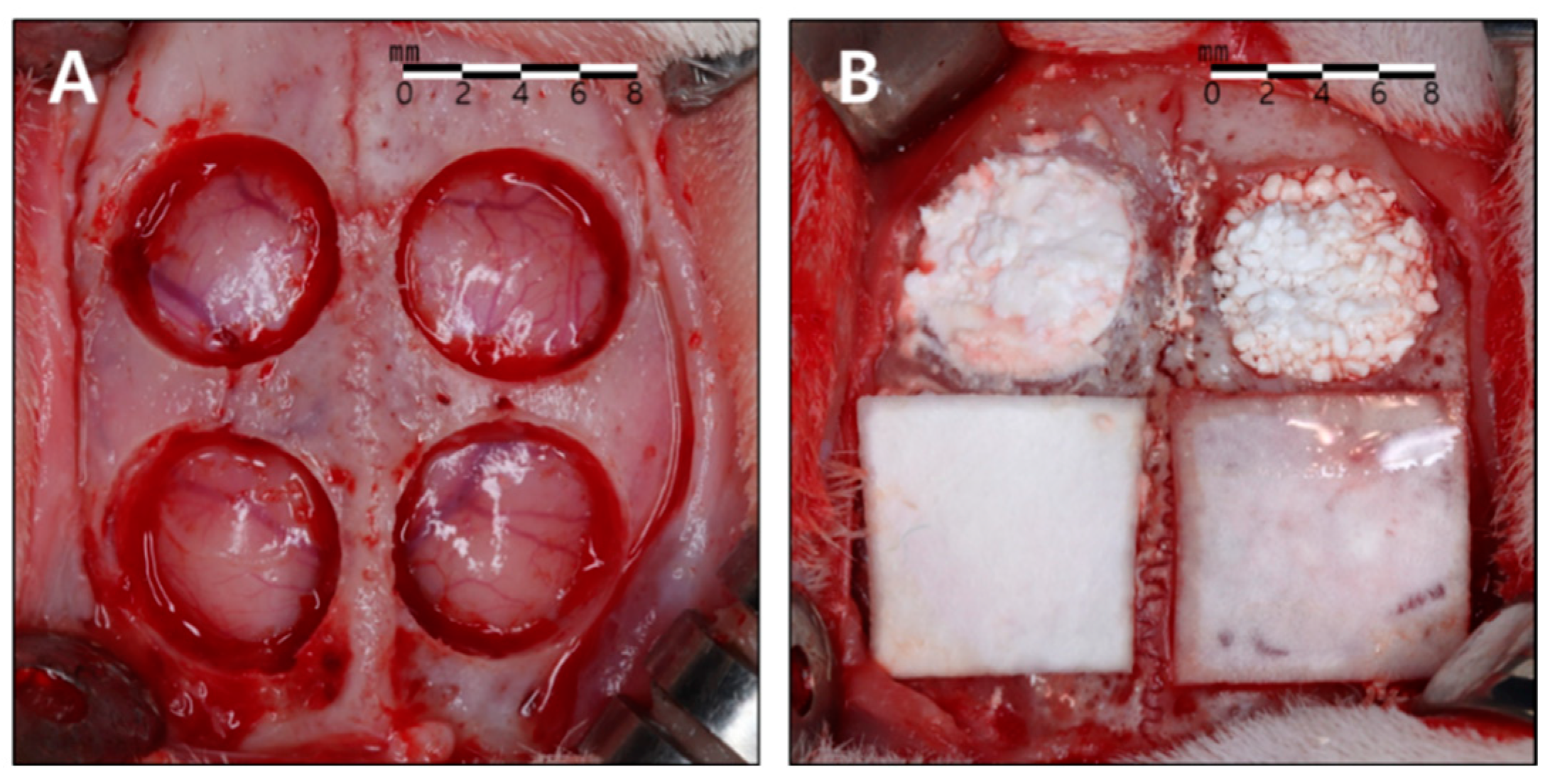
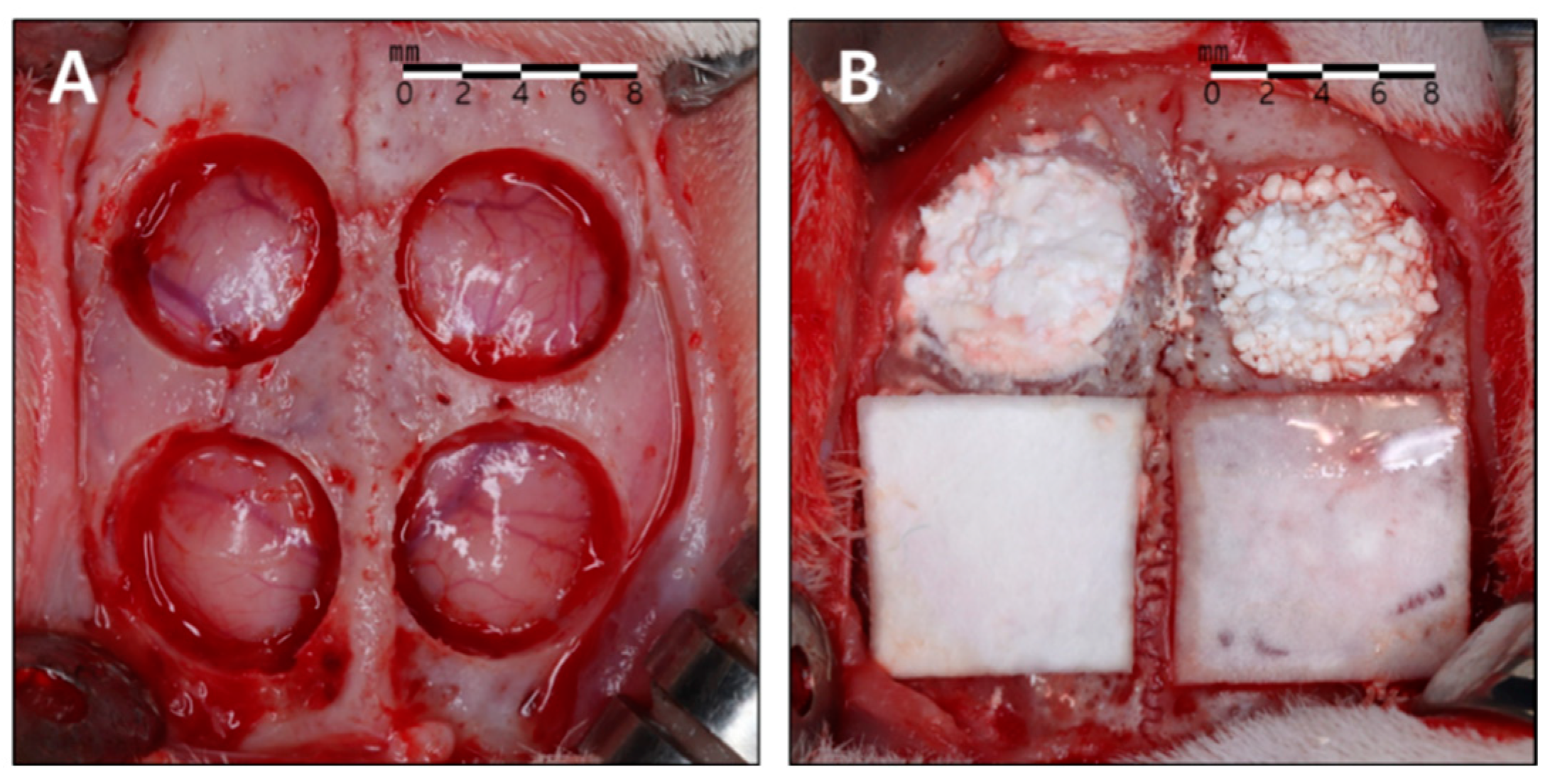
2.5. Surgical Protocol
2.6. Evaluation
- −
- Clinical observations: Animals were meticulously monitored for a duration of 2 to 8 weeks post-surgery, assessing for potential complications such as inflammation, allergic reactions, postoperative bleeding, and infections around the surgical site.
- −
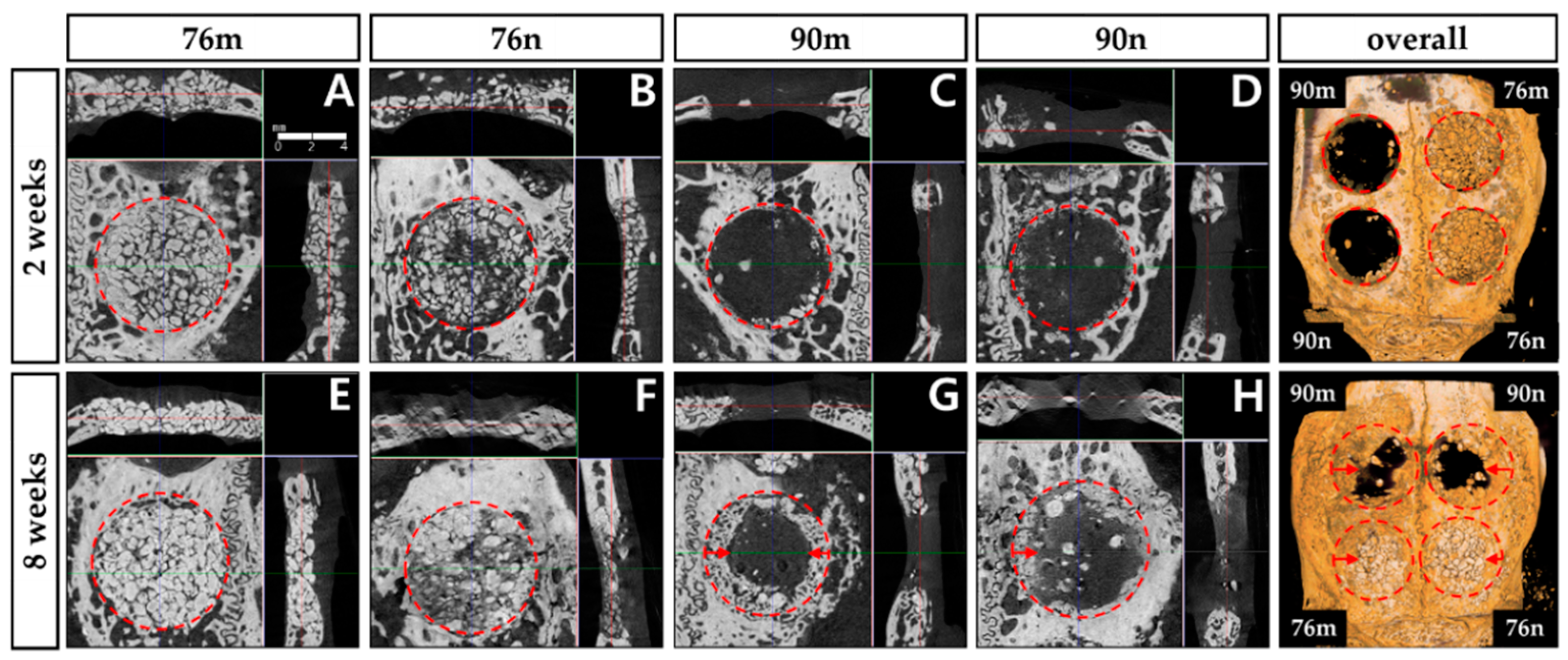
- Micro-computed tomography (micro-CT) analysis: After the animals were sacrificed, the surgical defects and adjacent tissues were removed in a single piece. These samples were rinsed in sterile saline and preserved in 10% buffered formaldehyde solution for 10 days. After rinsing in water, all specimens were scanned using a micro-CT scanner (SkyScan1173;Bruker-CT, Kartuizersweg 3B 2550 Kontich, Belgium). The samples were mounted on a jig using parafilm for precise micro-CT analysis, during which 800 images were captured at a setting of 130 kV tube voltage, 60 µA current, and through a 1.0 mm aluminum filter. Image reconstruction was performed using NRecon software (Ver. 1.7.0.4, Bruker, Kontich, Belgium), with alignment of the cross-sectional images for each specimen achieved through DataViewer software (Ver. 1.5.1.2, Bruker, Kontich, Belgium), and quantitative analysis conducted using CTAn software (Ver. 1.17.7.2, Bruker, Kontich, Belgium). For data analysis, the defect was set as the region of interest, and the threshold was set to 45–90 to analyze the following parameters:
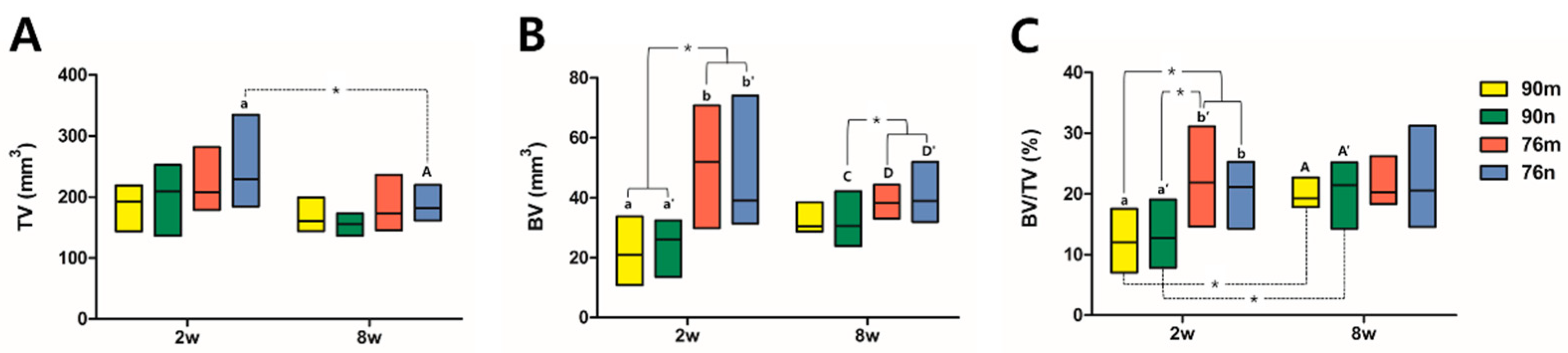
- Total tissue volume (TV; mm3): total augmented volume of the defects.
- New bone volume (BV; mm3): volumetric measurements of the new bone within the defects.
- Bone volume ratio (BV/TV; %): new bone volume to total augmented volume.
- −
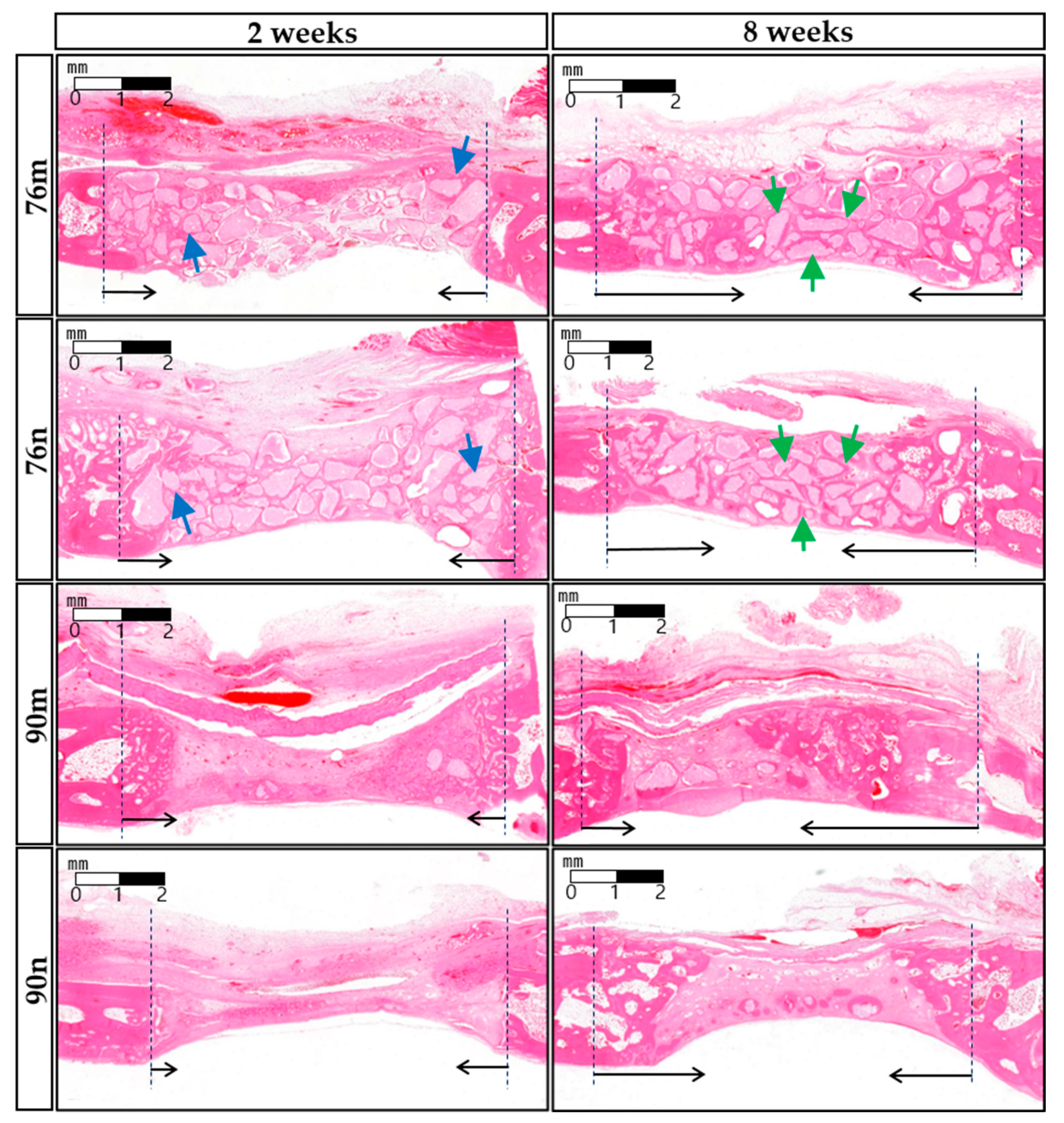
- Histologic and histomophometric analysis: Following micro-CT scanning, the specimens underwent a 14-day decalcification process in 5% formic acid and were subsequently embedded in paraffin. Serial 5 μm thick sections were obtained from the central region of each calvarial defect. The central sections from each block were subjected to hematoxylin and eosin (H&E) and Masson trichrome staining for histological and histometric analyses. One blinded examiner conducted examinations using a microscope (DM LB, Leica Microsystems, Wetzlar, Germany) equipped with a camera (DC300F, Leica Microsystems). The slide images were saved as digital files, and computer-aided histometric measurements were performed using an automated image analysis system (Image-Pro Plus; Media Cybernetics, Silver Spring, MD, USA). The assessment of bone healing and regeneration involved measuring the following parameters in each histological section corresponding to the defect areas:
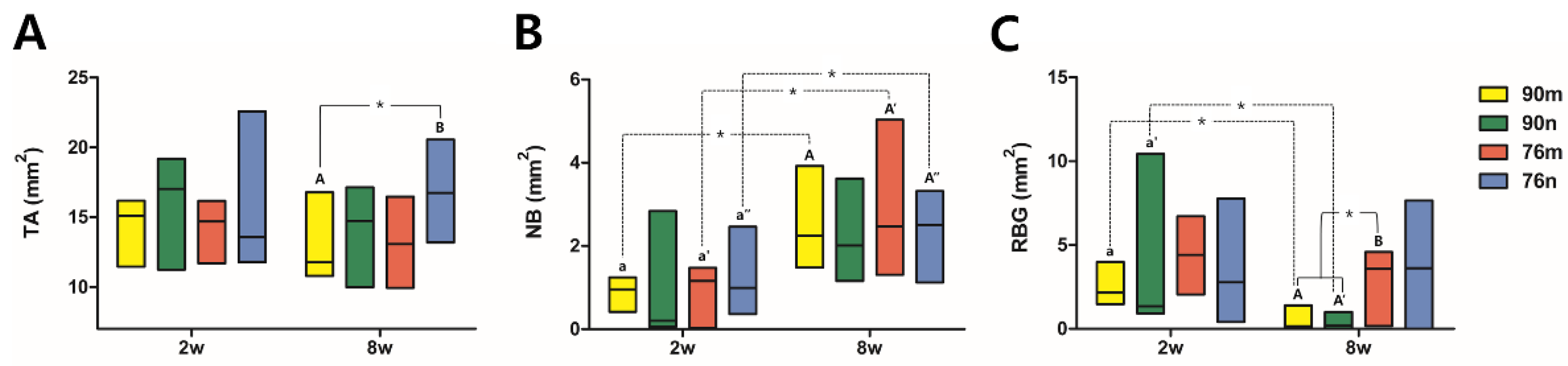
- Total augmented area (TA; mm2): Total sum of the area of new bone, residual particles, connective tissue, adipose tissue, blood vessels within the defect area.
- New bone area (NB; mm2) and its ratio (%NB): Area of the newly formed bone within the defect, and ratio of NB to TA.
- Residual bone graft area (RG; mm2) and its ratio (%RG): Area of the residual material within the defect, and ratio of RG to TA.
2.7. Statistical Analysis
3. Results
3.1. Phase Analysis Using X-ray Diffration
3.2. Clinical Findings
3.3. Micro-CT Analysis
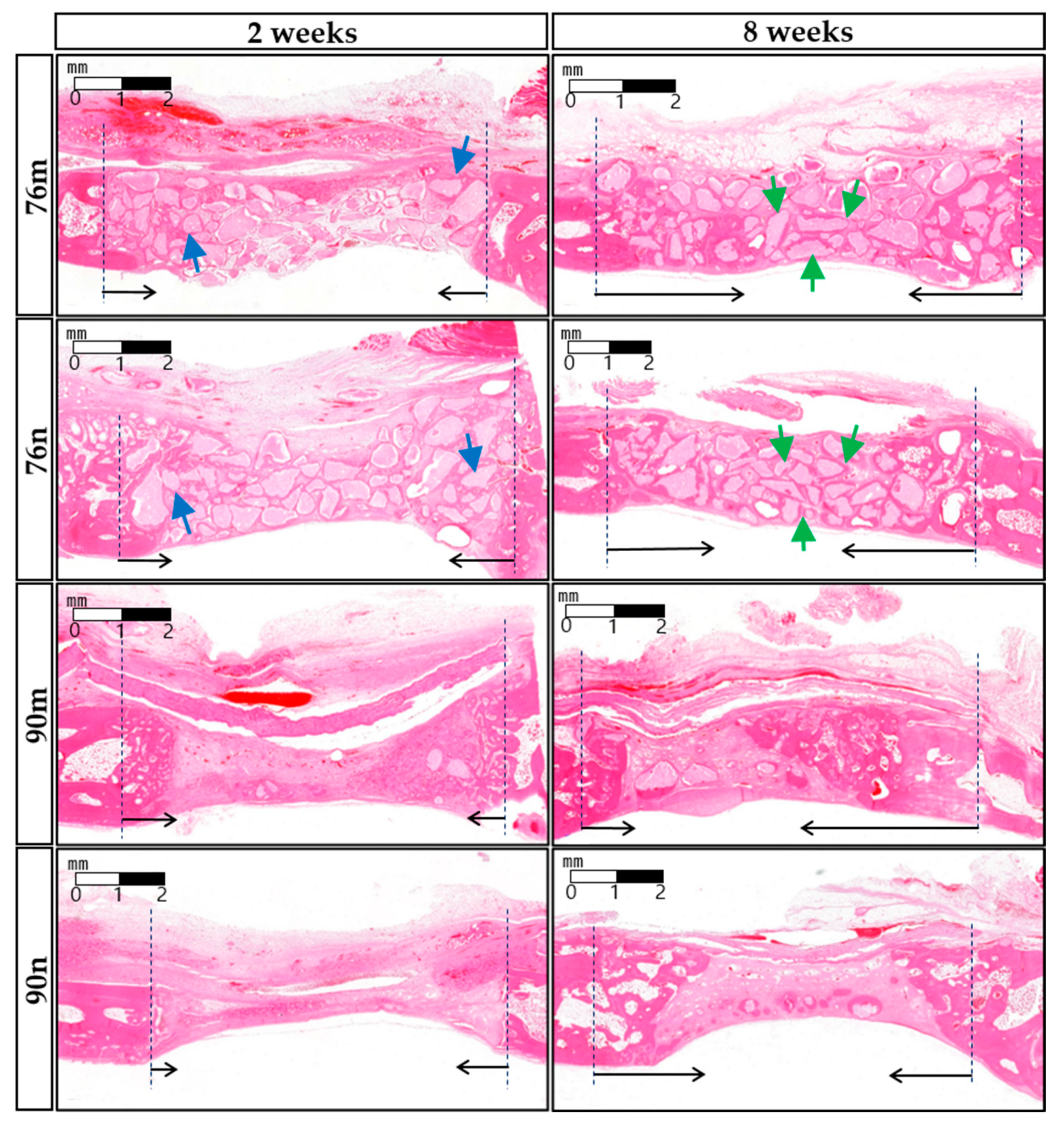
3.4. Histological Analysis
3.5. Histomorphometric Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haugen, H.J.; Lyngstadaas, S.P.; Rossi, F.; Perale, G. Bone grafts: Which is the ideal biomaterial? J. Clin. Periodontol. 2019, 46 (Suppl. 21), 92–102. [Google Scholar] [CrossRef]
- Kim, J.; Kim, S.; Song, I. Biomimetic Octacalcium Phosphate Bone Has Superior Bone Regeneration Ability Compared to Xenogeneic or Synthetic Bone. Materials 2021, 14, 5300. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-S.; Jang, T.-S.; Kim, S.-Y.; Lee, W.-P. Octacalcium Phosphate Bone Substitute (Bontree®): From Basic Research to Clinical Case Study. Appl. Sci. 2021, 11, 7921. [Google Scholar] [CrossRef]
- Bucholz, R.W. Nonallograft osteoconductive bone graft substitutes. Clin. Orthop. Relat. Res. 2002, 395, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Bohner, M.; Santoni, B.L.G.; Döbelin, N. β-tricalcium phosphate for bone substitution: Synthesis and properties. Acta Biomater. 2020, 113, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Arinzeh, T.L.; Tran, T.; McAlary, J.; Daculsi, G. A comparative study of biphasic calcium phosphate ceramics for human mesenchymal stem-cell-induced bone formation. Biomaterials 2005, 26, 3631–3638. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, M.; Botelho, M.G.; Dorozhkin, S.V. Biphasic calcium phosphates bioceramics (HA/TCP): Concept, physicochemical properties and the impact of standardization of study protocols in biomaterials research. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 71, 1293–1312. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Tanuma, Y.; Matsui, K.; Suzuki, O.; Takahashi, T.; Kamakura, S. Clinical safety and efficacy of implantation of octacalcium phosphate collagen composites in tooth extraction sockets and cyst holes. J. Tissue Eng. 2016, 7, 2041731416670770. [Google Scholar] [CrossRef]
- Fowler, B.O.; Moreno, E.C.; Brown, W.E. Infra-red spectra of hydroxyapatite, octacalcium phosphate and pyrolysed octacalcium phosphate. Arch. Oral. Biol. 1966, 11, 477–492. [Google Scholar] [CrossRef]
- LeGeros, R.Z. Properties of osteoconductive biomaterials: Calcium phosphates. Clin. Orthop. Relat. Res. 2002, 395, 81–98. [Google Scholar] [CrossRef]
- Detsch, R.; Hagmeyer, D.; Neumann, M.; Schaefer, S.; Vortkamp, A.; Wuelling, M.; Ziegler, G.; Epple, M. The resorption of nanocrystalline calcium phosphates by osteoclast-like cells. Acta Biomater. 2010, 6, 3223–3233. [Google Scholar] [CrossRef]
- Honda, Y.; Anada, T.; Kamakura, S.; Morimoto, S.; Kuriyagawa, T.; Suzuki, O. The effect of microstructure of octacalcium phosphate on the bone regenerative property. Tissue Eng. Part A 2009, 15, 1965–1973. [Google Scholar] [CrossRef] [PubMed]
- Miyatake, N.; Kishimoto, K.N.; Anada, T.; Imaizumi, H.; Itoi, E.; Suzuki, O. Effect of partial hydrolysis of octacalcium phosphate on its osteoconductive characteristics. Biomaterials 2009, 30, 1005–1014. [Google Scholar] [CrossRef] [PubMed]
- Murakami, Y.; Honda, Y.; Anada, T.; Shimauchi, H.; Suzuki, O. Comparative study on bone regeneration by synthetic octacalcium phosphate with various granule sizes. Acta Biomater. 2010, 6, 1542–1548. [Google Scholar] [CrossRef] [PubMed]
- Tanuma, Y.; Anada, T.; Honda, Y.; Kawai, T.; Kamakura, S.; Echigo, S.; Suzuki, O. Granule size-dependent bone regenerative capacity of octacalcium phosphate in collagen matrix. Tissue Eng. Part A 2012, 18, 546–557. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Webster, T.J. Nanomedicine for implants: A review of studies and necessary experimental tools. Biomaterials 2007, 28, 354–369. [Google Scholar] [CrossRef] [PubMed]
- Eliaz, N.; Metoki, N. Calcium Phosphate Bioceramics: A Review of Their History, Structure, Properties, Coating Technologies and Biomedical Applications. Materials 2017, 10, 334. [Google Scholar] [CrossRef]
- Wang, H.L.; Boyapati, L. “PASS” principles for predictable bone regeneration. Implant. Dent. 2006, 15, 8–17. [Google Scholar] [CrossRef]
- Sbricoli, L.; Guazzo, R.; Annunziata, M.; Gobbato, L.; Bressan, E.; Nastri, L. Selection of Collagen Membranes for Bone Regeneration: A Literature Review. Materials 2020, 13, 786. [Google Scholar] [CrossRef]
- Bunyaratavej, P.; Wang, H.L. Collagen membranes: A review. J. Periodontol. 2001, 72, 215–229. [Google Scholar] [CrossRef]
- Jeong, C.H.; Kim, J.; Kim, H.S.; Lim, S.Y.; Han, D.; Huser, A.J.; Lee, S.B.; Gim, Y.; Ji, J.H.; Kim, D.; et al. Acceleration of bone formation by octacalcium phosphate composite in a rat tibia critical-sized defect. J. Orthop. Transl. 2022, 37, 100–112. [Google Scholar] [CrossRef]
- Bergerhoff, G.; Hundt, R.; Sievers, R.; Brown, I.D. The inorganic crystal structure data base. J. Chem. Inf. Comput. Sci. 1983, 23, 66–69. [Google Scholar] [CrossRef]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving bioscience research reporting: The arrive guidelines for reporting animal research. J. Pharmacol. Pharmacother. 2010, 1, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Pae, H.C.; Kang, J.H.; Cha, J.K.; Lee, J.S.; Paik, J.W.; Jung, U.W.; Kim, B.H.; Choi, S.H. 3d-printed polycaprolactone scaffold mixed with β-tricalcium phosphate as a bone regenerative material in rabbit calvarial defects. J. Biomed. Mater. Res. Part B Appl. Biomater. 2019, 107, 1254–1263. [Google Scholar] [CrossRef] [PubMed]
- Kamal, M.; Andersson, L.; Al-Asfour, A.; Bartella, A.K.; Gremse, F.; Rosenhain, S.; Gabato, S.; Hölzle, F.; Kessler, P.; Lethaus, B. Bone regeneration in rabbit calvarial critical-sized defects filled with composite in situ formed xenogenic dentin and biphasic tricalcium phosphate/hyroxyapatite mixture. J. Biomed. Mater. Res. Part B Appl. Biomater. 2019, 107, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Lin, K.; Wang, Z.; Chang, J.; Wang, L.; Lu, J.; Ning, C. Reconstruction of calvarial defect of rabbits using porous calcium silicate bioactive ceramics. Biomaterials 2008, 29, 2588–2596. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; McBride, S.; Fulmer, M.; Harten, R.; Garza, Z.; Dean, D.D.; Sylvia, V.L.; Doll, B.; Wolfgang, T.L.; Gruskin, E. Fiber-reinforced calcium phosphate cement formulations for cranioplasty applications: A 52-week duration preclinical rabbit calvaria study. J. Biomed. Mater. Res. Part B Appl. Biomater. 2012, 100, 1170–1178. [Google Scholar] [CrossRef] [PubMed]
- Sohn, J.-Y.; Park, J.-C.; Um, Y.-J.; Jung, U.-W.; Kim, C.-S.; Cho, K.-S.; Choi, S.-H. Spontaneous healing capacity of rabbit cranial defects of various sizes. J. Periodontal Implant. Sci. 2010, 40, 180–187. [Google Scholar] [CrossRef]
- Guastaldi, F.P.S.; Matheus, H.R.; Faloni, A.P.D.S.; de Almeida-Filho, E.; Cominotte, M.A.; Moretti, L.A.C.; Verzola, M.H.A.; Marcantonio, E., Jr.; de Almeida, J.M.; Guastaldi, A.C. A new multiphase calcium phosphate graft material improves bone healing—An in vitro and in vivo analysis. J. Biomed. Mater. Res. Part B Appl. Biomater. 2022, 110, 2686–2704. [Google Scholar] [CrossRef]
- Suzuki, O.; Shiwaku, Y.; Hamai, R. Octacalcium phosphate bone substitute materials: Comparison between properties of biomaterials and other calcium phosphate materials. Dent. Mater. J. 2020, 39, 187–199. [Google Scholar] [CrossRef]
- Daculsi, G. Biphasic calcium phosphate concept applied to artificial bone, implant coating and injectable bone substitute. Biomaterials 1998, 19, 1473–1478. [Google Scholar] [CrossRef]
- Daculsi, G.; LeGeros, R.Z.; Nery, E.; Lynch, K.; Kerebel, B. Transformation of biphasic calcium phosphate ceramics in vivo: Ultrastructural and physicochemical characterization. J. Biomed. Mater. Res. 1989, 23, 883–894. [Google Scholar] [CrossRef]
- Daculsi, G.; LeGeros, R.Z.; Mitre, D. Crystal dissolution of biological and ceramic apatites. Calcif. Tissue Int. 1989, 45, 95–103. [Google Scholar] [CrossRef]
- Gauthier, O.; Bouler, J.M.; Aguado, E.; Pilet, P.; Daculsi, G. Macroporous biphasic calcium phosphate ceramics: Influence of macropore diameter and macroporosity percentage on bone ingrowth. Biomaterials 1998, 19, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Kamakura, S.; Sasaki, K.; Homma, T.; Honda, Y.; Anada, T.; Echigo, S.; Suzuki, O. The primacy of octacalcium phosphate collagen composites in bone regeneration. J. Biomed. Mater. Res. A 2007, 83, 725–733. [Google Scholar] [CrossRef]
- Jung, Y.; Kim, W.H.; Lee, S.H.; Ju, K.W.; Jang, E.H.; Kim, S.O.; Kim, B.; Lee, J.H. Evaluation of New Octacalcium Phosphate-Coated Xenograft in Rats Calvarial Defect Model on Bone Regeneration. Materials 2020, 13, 4391. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Matsui, K.; Ezoe, Y.; Kajii, F.; Suzuki, O.; Takahashi, T.; Kamakura, S. Efficacy of Octacalcium Phosphate Collagen Composite for Titanium Dental Implants in Dogs. Materials 2018, 11, 229. [Google Scholar] [CrossRef]
- Suzuki, O.; Hamai, R.; Sakai, S. The material design of octacalcium phosphate bone substitute: Increased dissolution and osteogenecity. Acta Biomater. 2023, 158, 1–11. [Google Scholar] [CrossRef]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.L.; Strider, J.; Hall, C.; Ferguson, H.W.; Armstrong, K.L.; Runner, R.R.; Baur, D.A. Distraction osteogenesis in irradiated rabbit mandibles with adjunctive hyperbaric oxygen therapy. J. Oral. Maxillofac. Surg. 2006, 64, 589–593. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Week | Group | TV | BV | BV/TV | ||||
|---|---|---|---|---|---|---|---|---|
| 2 weeks (n = 5) | 90m | 192.563 (144.331–219.075) | 21.038 (10.813–33.831) a |  |  | 12.004 (7.051–17.569) a |  | |
| 90n | 209.308 (136.747–252.565) | 26.084 (13.647–32.505) a′ | 12.787 (7.859–19.074) a′ | |||||
| 76m | 208.007 (179.307–281.868) | 52.035 (29.927–70.808) b | 21.899 (14.640–31.131) b′ | |||||
| 76n |  | 229.541 (184.888–334.893) a | 39.112 (31.501–74.109) b′ | 21.154 (14.334–25.276) b | ||||
| Overall | 208.657 (136.747–334.893) | 32.401 (10.813–74.109) | 15.688 (7.051–31.131) | |||||
| 8 weeks (n = 5) | 90m | 161.167 (144.422–199.540) | 30.565 (28.767–38.564) | 19.327 (17.849–22.715) A | ||||
| 90n | 155.934 (136.747–173.027) | 30.685 (23.884–42.150) C |  | 21.449 (14.324–25.173) A′ | ||||
| 76m | 173.027 (145.817–236.518) | 38.200 (33.107–44.354) D | 20.279 (18.388–26.197) | |||||
| 76n | 181.749 (161.864–219.773) A | 39.009 (32.037–52.048) D′ | 20.592 (14.577–31.214) | |||||
| Overall | 166.051 (136.747–236.518) | 34.318 (23.884–52.048) | 20.533 (14.324–31.214) | |||||
| Week | Group | TA | NB | %NB | RBG | %RBG | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 weeks (n = 5) | 90m | 15.090 (11.450–16.170) |  | 0.960 (0.420–1.240) a |  | 5.937 (3.368–8.217) a |  | 2.150 (1.470–3.990) a |  | 14.515 (12.838–26.441) a | |||
| 90n | 17.010 (11.240–19.170) | 0.200 (0.060–2.840) | 1.779 (0.495–15.477) | 1.340 (0.920–10.430) a′ | 11.744 (7.302–54.408) a′ | ||||||||
| 76m | 14.690 (11.680–16.160) | 1.160 (0.030–1.470) a′ | 7.612 (0.257–10.007) a′ | 4.400 (2.050–6.720) | 29.952 (14.012–43.664) | ||||||||
| 76n | 13.560 (11.780–22.560) | 0.990 (0.360–2.460) a′′ | 6.033 (3.056–10.904) a′′ | 2.780 (0.400–7.770) | 20.501 (3.040–34.441) | ||||||||
| Overall | 14.890 (11.240–22.560) | 0.975 (0.030–2.840) | 5.985 (0.257–15.477) | 2.405 (0.400–10.430) | 15.300 (3.040–54.408) | ||||||||
| 8 weeks (n = 5) | 90m |  | 11.755 (10.790–16.770) A | 2.245 (1.480–3.920) A | 19.840 (12.726–27.625) A | 0.155 (0.000–1.390) A |  | 1.196 (0.000–9.796) A |  | ||||
| 90n | 14.735 (9.970–17.130) | 2.015 (1.160–3.620) | 15.691 (8.033–21.133) | 0.180 (0.000–1.010) A′ | 1.087 (0.000–6.994) A′ | ||||||||
| 76m | 13.070 (9.940–16.450) | 2.465 (1.310–5.030) A′ | 16.479 (11.313–50.604) A′ | 3.580 (0.170–4.580) B | 24.323 (1.468–32.068) B | ||||||||
| 76n | 16.720 (13.190–20.550) B | 2.505 (1.120–3.320) A′′ | 15.688 (7.349–16.831) A′′ | 3.615 (0.000–7.650) | 21.968 (0.000–37.226) | ||||||||
| Overall | 14.315 (9.940–20.550) | 2.290 (1.120–5.030) | 16.128 (7.349–50.604) | 0.800 (0.000–7.650) | 6.034 (0.000–37.226) | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pyo, S.-W.; Paik, J.-W.; Lee, D.-N.; Seo, Y.-W.; Park, J.-Y.; Kim, S.; Choi, S.-H. Comparative Analysis of Bone Regeneration According to Particle Type and Barrier Membrane for Octacalcium Phosphate Grafted into Rabbit Calvarial Defects. Bioengineering 2024, 11, 215. https://doi.org/10.3390/bioengineering11030215
Pyo S-W, Paik J-W, Lee D-N, Seo Y-W, Park J-Y, Kim S, Choi S-H. Comparative Analysis of Bone Regeneration According to Particle Type and Barrier Membrane for Octacalcium Phosphate Grafted into Rabbit Calvarial Defects. Bioengineering. 2024; 11(3):215. https://doi.org/10.3390/bioengineering11030215
Chicago/Turabian StylePyo, Se-Wook, Jeong-Won Paik, Da-Na Lee, Young-Wook Seo, Jin-Young Park, Sunjai Kim, and Seong-Ho Choi. 2024. "Comparative Analysis of Bone Regeneration According to Particle Type and Barrier Membrane for Octacalcium Phosphate Grafted into Rabbit Calvarial Defects" Bioengineering 11, no. 3: 215. https://doi.org/10.3390/bioengineering11030215
APA StylePyo, S.-W., Paik, J.-W., Lee, D.-N., Seo, Y.-W., Park, J.-Y., Kim, S., & Choi, S.-H. (2024). Comparative Analysis of Bone Regeneration According to Particle Type and Barrier Membrane for Octacalcium Phosphate Grafted into Rabbit Calvarial Defects. Bioengineering, 11(3), 215. https://doi.org/10.3390/bioengineering11030215