
Three-Dimensional Printed Customized Scaffolds Covered with Decellularized Bone Extracellular Matrix for Open-Wedge High-Tibial Osteotomy

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
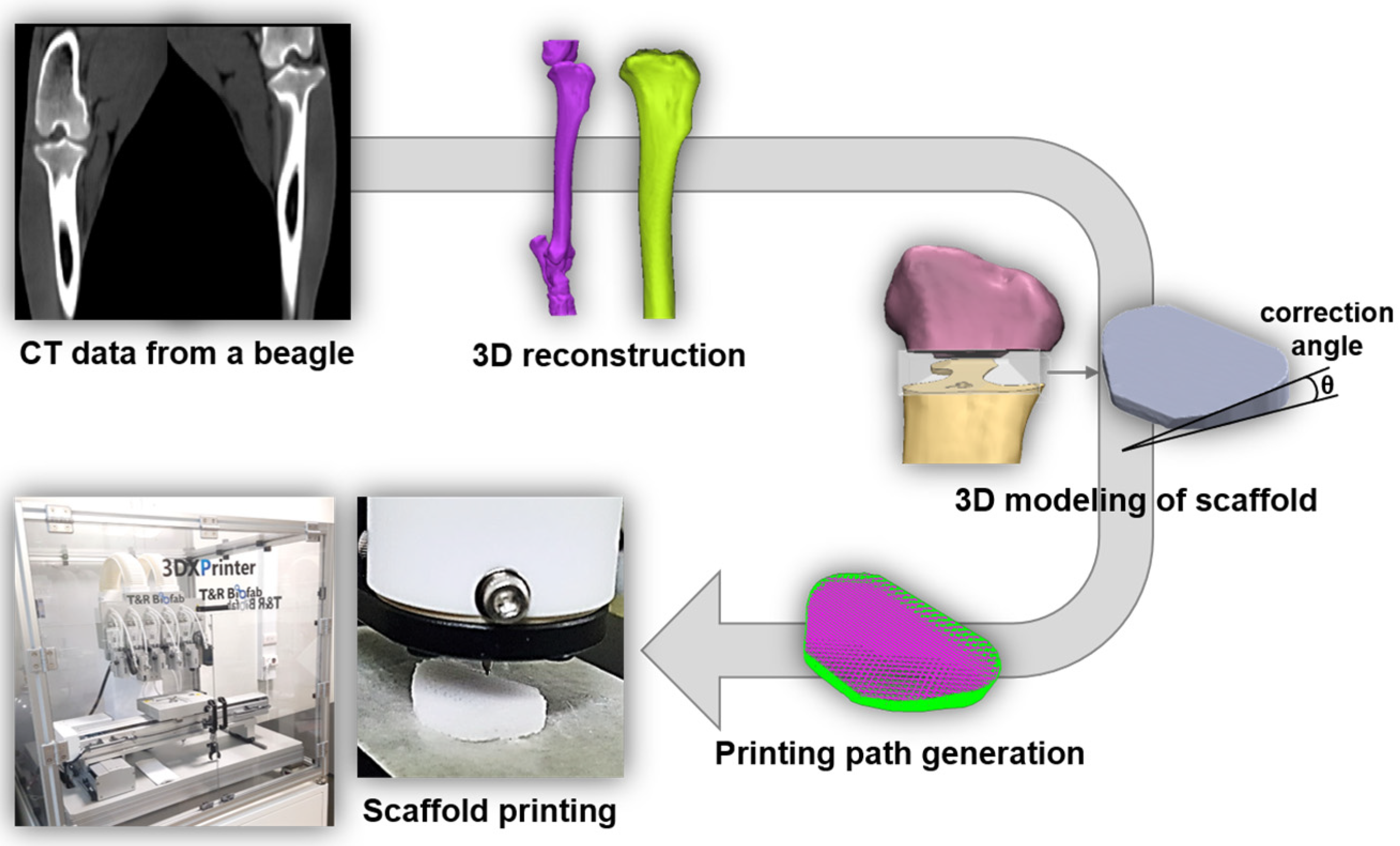
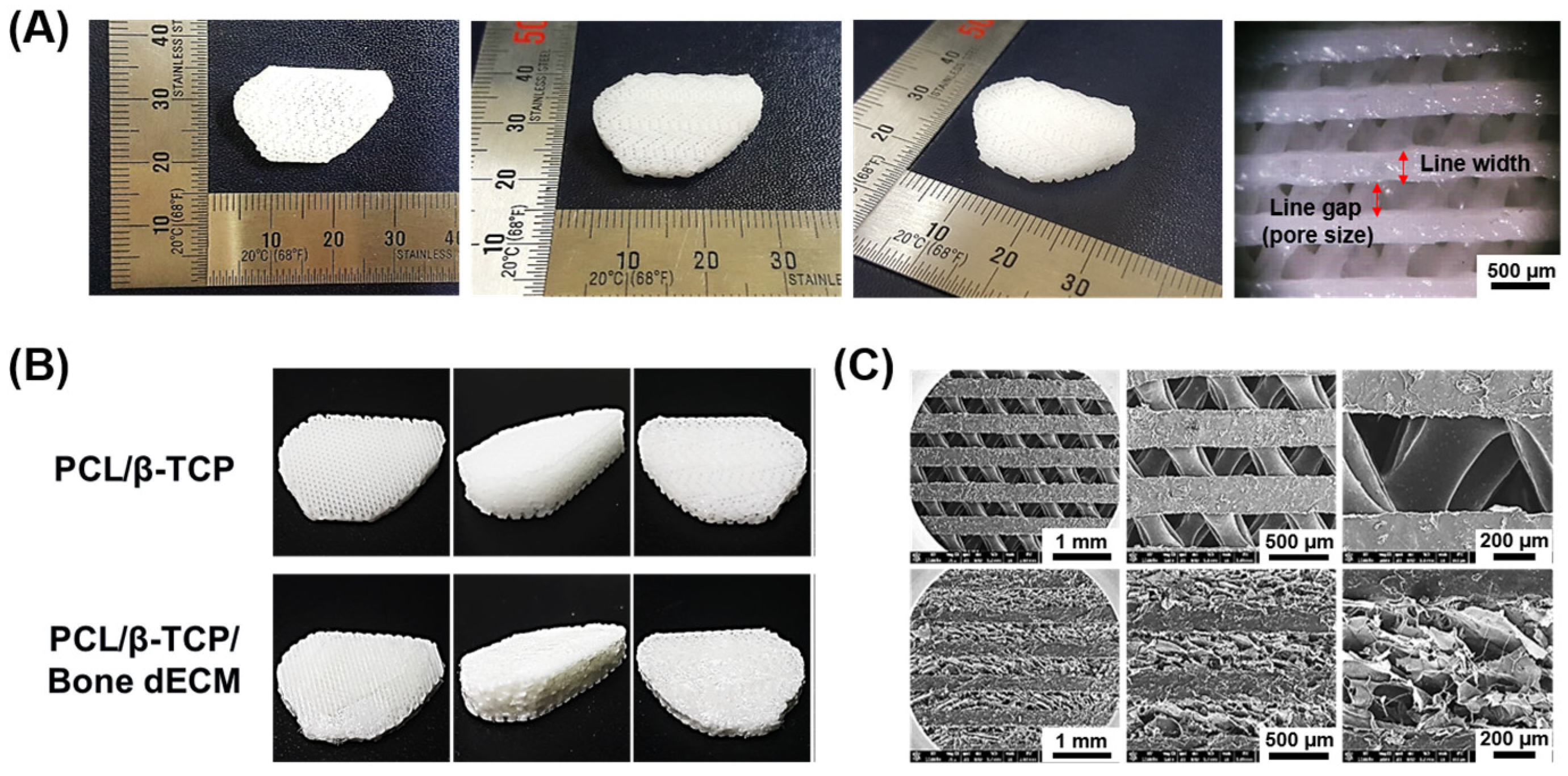
3.1. Characterization of 3D Printed Scaffolds
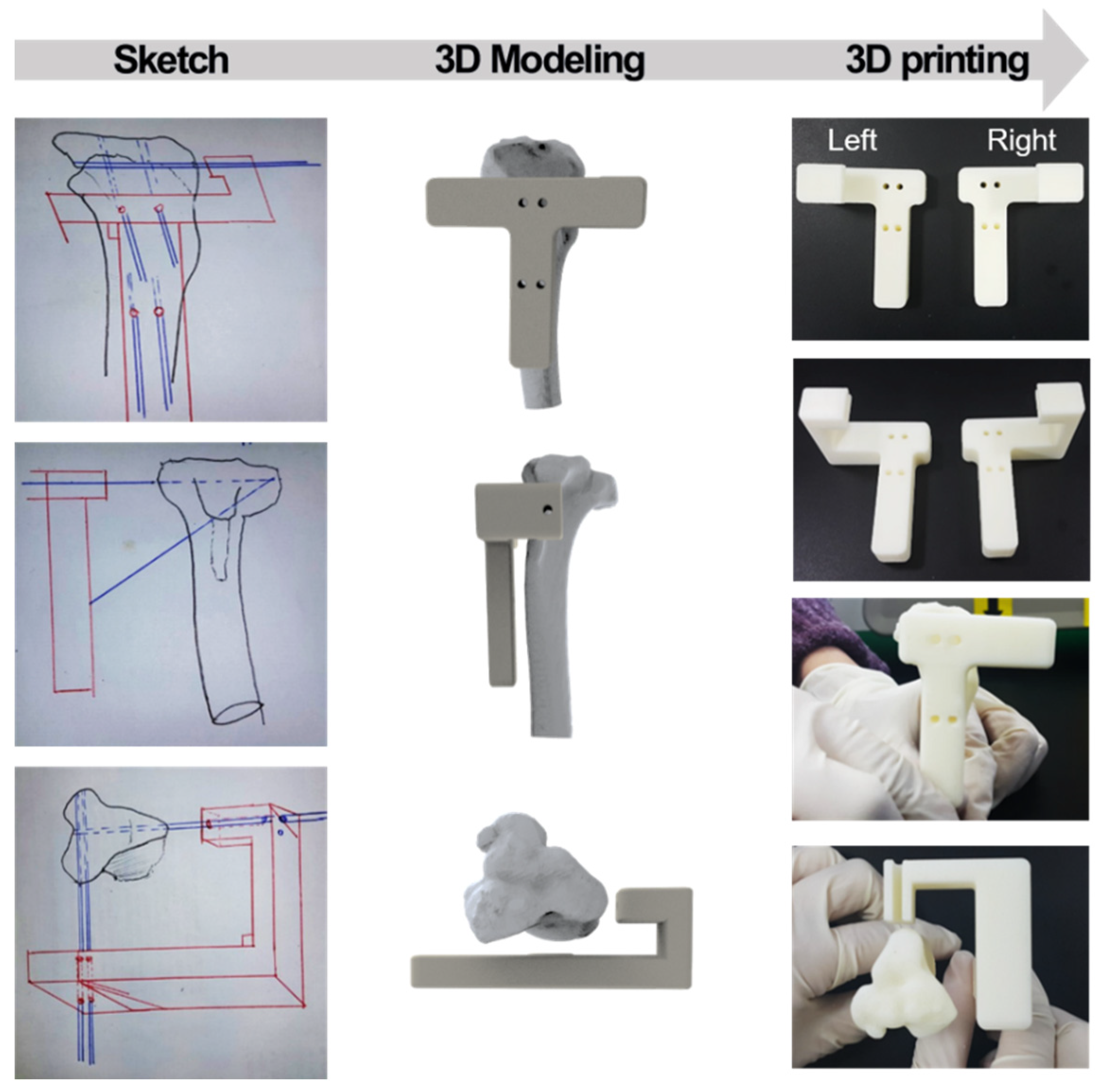
3.2. Characterization of Customized Guide Instrument
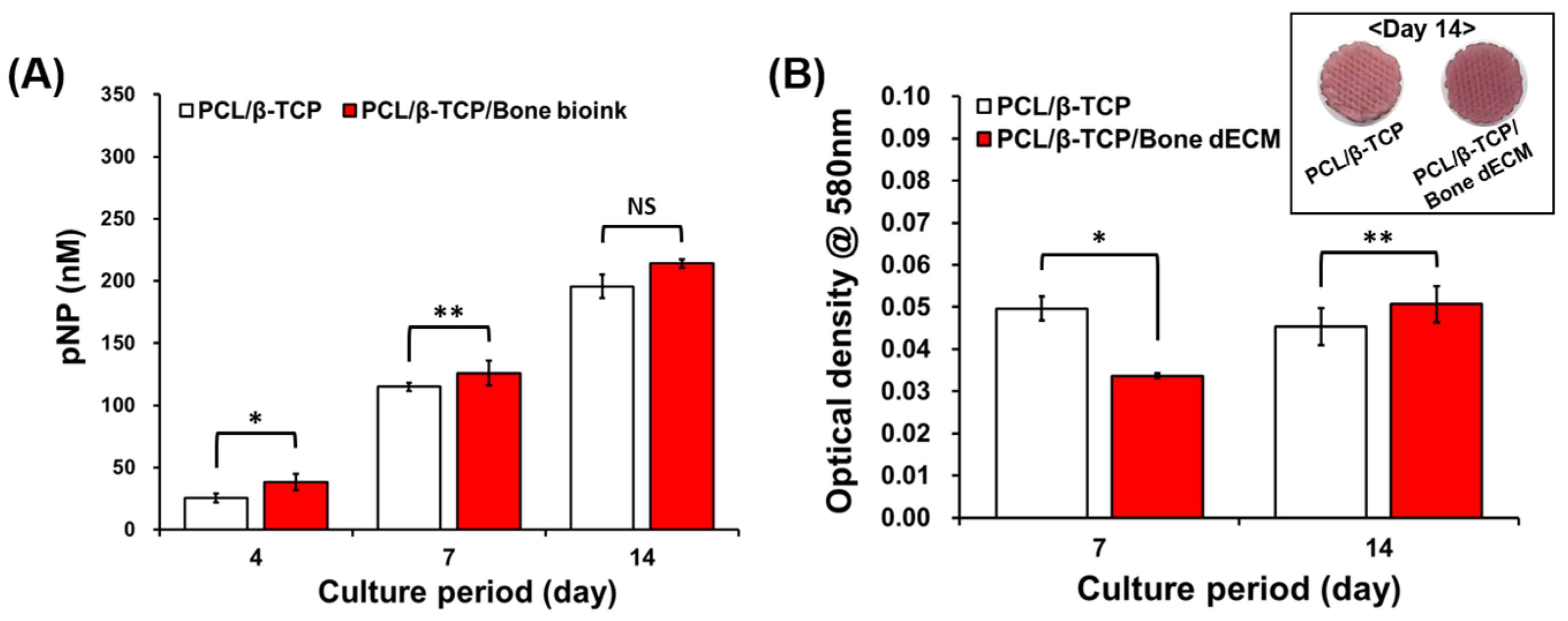
3.3. Cell Seeding Efficiency and Proliferation Results
3.4. Cell Differentiation Results
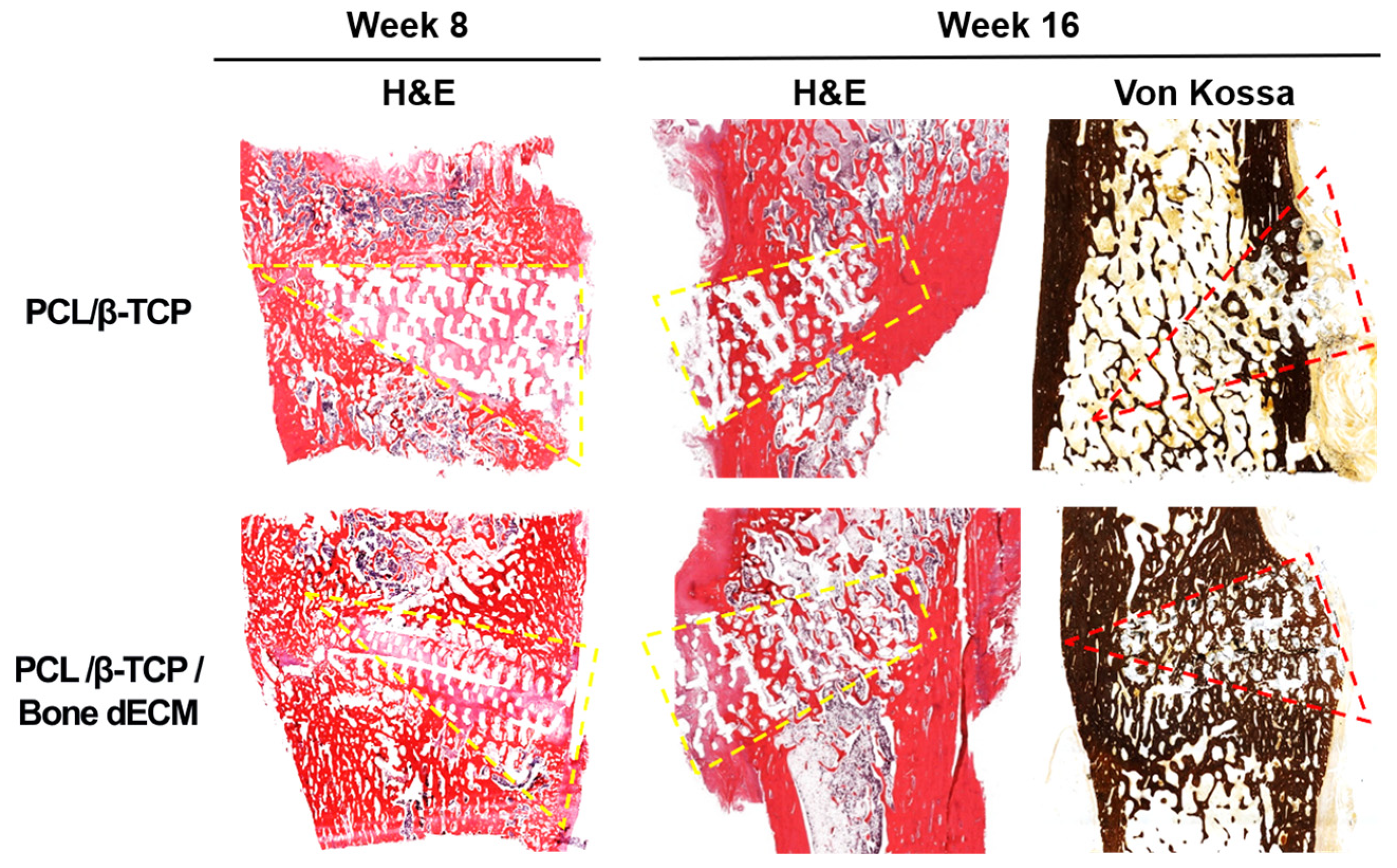
3.5. In Vivo Results
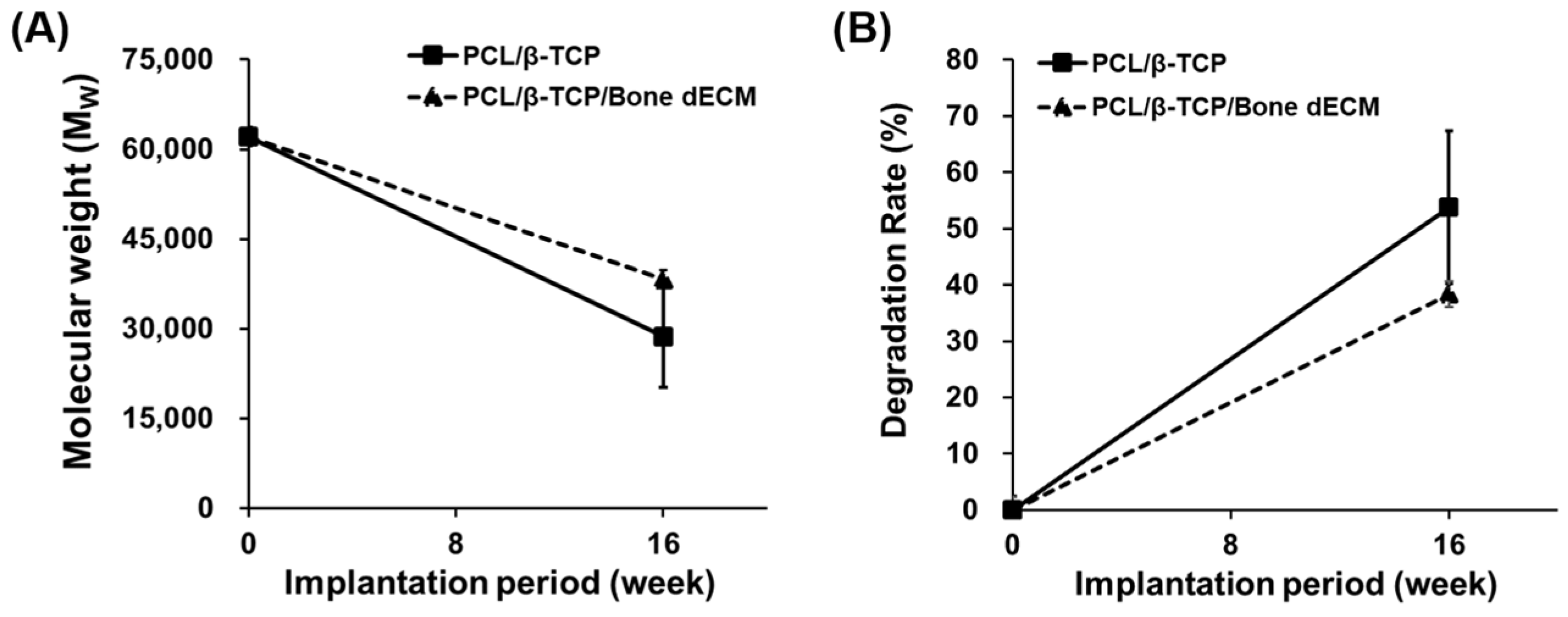
3.6. Degradation Results
3.7. Radiologic Evaluations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahn, G.; Lee, J.S.; Yun, W.S.; Shim, J.H.; Lee, U.L. Cleft Alveolus Reconstruction Using a Three-Dimensional Printed Bioresorbable Scaffold with Human Bone Marrow Cells. J. Craniofacial Surg. 2018, 29, 1880–1883. [Google Scholar] [CrossRef] [PubMed]
- Andriacchi, T.P.; Mundermann, A. The role of ambulatory mechanics in the initiation and progression of knee osteoarthritis. Curr. Opin. Rheumatol. 2006, 18, 514–518. [Google Scholar] [CrossRef] [PubMed]
- Aryee, S.; Imhoff, A.B.; Rose, T.; Tischer, T. Do we need synthetic osteotomy augmentation materials for opening-wedge high tibial osteotomy. Biomaterials 2008, 29, 3497–3502. [Google Scholar] [CrossRef] [PubMed]
- Blaker, J.J.; Nazhat, S.N.; Maquet, V.; Boccaccini, A.R. Long-term in vitro degradation of PDLLA/bioglass bone scaffolds in acellular simulated body fluid. Acta Biomater. 2011, 7, 829–840. [Google Scholar] [CrossRef]
- Brouwer, R.W.; Huizinga, M.R.; Duivenvoorden, T.; van Raaij, T.M.; Verhagen, A.P.; Bierma-Zeinstra, S.M.; Verhaar, J.A. Osteotomy for treating knee osteoarthritis. Cochrane Database Syst. Rev. 2014, 2014, Cd004019. [Google Scholar] [CrossRef]
- Cai, S.; Xu, G.H.; Yu, X.Z.; Zhang, W.J.; Xiao, Z.Y.; Yao, K.D. Fabrication and biological characteristics of beta-tricalcium phosphate porous ceramic scaffolds reinforced with calcium phosphate glass. J. Mater. Sci. Mater. Med. 2009, 20, 351–358. [Google Scholar] [CrossRef]
- Cheng, C.W.; Solorio, L.D.; Alsberg, E. Decellularized tissue and cell-derived extracellular matrices as scaffolds for orthopaedic tissue engineering. Biotechnol. Adv. 2014, 32, 462–484. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, E.; Saenz de Viteri, V.; Igartua, A.; Martinetti, R.; Dolcini, L.; Barandika, G. Structural characterization and mechanical performance of calcium phosphate scaffolds and natural bones: A comparative study. J. Appl. Biomater. Biomech. JABB 2010, 8, 159–165. [Google Scholar] [CrossRef]
- Gothard, D.; Smith, E.L.; Kanczler, J.M.; Black, C.R.; Wells, J.A.; Roberts, C.A.; White, L.J.; Qutachi, O.; Peto, H.; Rashidi, H.; et al. In Vivo Assessment of Bone Regeneration in Alginate/Bone ECM Hydrogels with Incorporated Skeletal Stem Cells and Single Growth Factors. PLoS ONE 2015, 10, e0145080. [Google Scholar] [CrossRef]
- Han, J.H.; Kim, H.J.; Song, J.G.; Yang, J.H.; Bhandare, N.N.; Fernandez, A.R.; Park, H.J.; Nha, K.W. Is Bone Grafting Necessary in Opening Wedge High Tibial Osteotomy? A Meta-Analysis of Radiological Outcomes. Knee Surg. Relat. Res. 2015, 27, 207–220. [Google Scholar] [CrossRef]
- Han, S.B.; Lee, D.H.; Shetty, G.M.; Chae, D.J.; Song, J.G.; Nha, K.W. A “safe zone” in medial open-wedge high tibia osteotomy to prevent lateral cortex fracture. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2013, 21, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Hollister, S.J. Porous scaffold design for tissue engineering. Nat. Mater. 2005, 4, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Ahn, G.; Kim, C.; Lee, J.-S.; Lee, I.-G.; An, S.-H.; Yun, W.-S.; Kim, S.-Y.; Shim, J.-H. Synergistic Effects of Beta Tri-Calcium Phosphate and Porcine-Derived Decellularized Bone Extracellular Matrix in 3D-Printed Polycaprolactone Scaffold on Bone Regeneration. Macromol. Biosci. 2018, 18, e1800025. [Google Scholar] [CrossRef] [PubMed]
- Lash, N.J.; Feller, J.A.; Batty, L.M.; Wasiak, J.; Richmond, A.K. Bone grafts and bone substitutes for opening-wedge osteotomies of the knee: A systematic review. Arthroscopy 2015, 31, 720–730. [Google Scholar] [CrossRef]
- Lee, B.H.; Ha, C.W.; Moon, S.W.; Chang, M.; Kim, H.Y.; Park, S.H.; Wang, J.H. Three-dimensional relationships between secondary changes and selective osteotomy parameters for biplane medial open-wedge high tibial osteotomy. Knee 2017, 24, 362–371. [Google Scholar] [CrossRef]
- Lee, O.S.; Lee, K.J.; Lee, Y.S. Comparison of bone healing and outcomes between allogenous bone chip and hydroxyapatite chip grafts in open wedge high tibial osteotomy. J. Mater. Sci. Mater. Med. 2017, 28, 189. [Google Scholar] [CrossRef]
- Lee, S.C.; Jung, K.A.; Nam, C.H.; Jung, S.H.; Hwang, S.H. The short-term follow-up results of open wedge high tibial osteotomy with using an Aescula open wedge plate and an allogenic bone graft: The minimum 1-year follow-up results. Clin. Orthop. Surg. 2010, 2, 47–54. [Google Scholar] [CrossRef]
- Miller, B.S.; Dorsey, W.O.; Bryant, C.R.; Austin, J.C. The effect of lateral cortex disruption and repair on the stability of the medial opening wedge high tibial osteotomy. Am. J. Sports Med. 2005, 33, 1552–1557. [Google Scholar] [CrossRef]
- Miyazaki, T.; Wada, M.; Kawahara, H.; Sato, M.; Baba, H.; Shimada, S. Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann. Rheum. Dis. 2002, 61, 617–622. [Google Scholar] [CrossRef]
- Nha, K.W.; Oh, S.M.; Ha, Y.W.; Nikumbha, V.P.; Seo, J.H.; Oh, M.J.; Lim, C.O.; Kim, J.G. A Retrospective Comparison of Union Rates After Open Wedge High Tibial Osteotomies With and Without Synthetic Bone Grafts (Hydroxyapatite and beta-tricalciumphosphate) at 2 Years. Arthroscopy 2018, 34, 2621–2630. [Google Scholar] [CrossRef]
- Rangavittal, N.; Landa-Canovas, A.R.; Gonzalez-Calbet, J.M.; Vallet-Regi, M. Structural study and stability of hydroxyapatite and beta-tricalcium phosphate: Two important bioceramics. J. Biomed. Mater. Res. 2000, 51, 660–668. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.M.; Park, J.W.; Na, H.D.; Shon, O.J. High Tibial Osteotomy versus Unicompartmental Knee Arthroplasty for Medial Compartment Arthrosis with Kissing Lesions in Relatively Young Patients. Knee Surg. Relat. Res. 2018, 30, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Santic, V.; Tudor, A.; Sestan, B.; Legovic, D.; Sirola, L.; Rakovac, I. Bone allograft provides bone healing in the medial opening high tibial osteotomy. Int. Orthop. 2010, 34, 225–229. [Google Scholar] [CrossRef]
- Sawkins, M.J.; Bowen, W.; Dhadda, P.; Markides, H.; Sidney, L.; Taylor, A.; Rose, F.; Badylak, S.; Shakesheff, K.; White, L. Hydrogels derived from demineralized and decellularized bone extracellular matrix. Acta Biomater. 2013, 9, 7865–7873. [Google Scholar] [CrossRef]
- Schroter, S.; Ateschrang, A.; Ihle, C.; Stöckle, U.; Konstantinidis, L.; Döbele, S. Lateral hinge fractures in open wedge high tibial osteotomy. Der Orthop. 2014, 43, 1000–1007. [Google Scholar]
- Shim, J.H.; Jeong, J.H.; Won, J.Y.; Bae, J.-H.; Ahn, G.; Jeon, H.; Yun, W.-S.; Bae, E.-B.; Choi, J.-W.; Lee, S.-H.; et al. Porosity effect of 3D-printed polycaprolactone membranes on calvarial defect model for guided bone regeneration. Biomed. Mater. 2017, 13, 015014. [Google Scholar] [CrossRef]
- Shim, J.H.; Won, J.Y.; Park, J.H.; Bae, J.H.; Ahn, G.; Kim, C.H.; Lim, D.H.; Cho, D.W.; Yun, W.S.; Bae, E.B.; et al. Effects of 3D-Printed Polycaprolactone/beta-Tricalcium Phosphate Membranes on Guided Bone Regeneration. Int. J. Mol. Sci. 2017, 18, 899. [Google Scholar] [CrossRef]
- Slevin, O.; Ayeni, O.R.; Hinterwimmer, S.; Tischer, T.; Feucht, M.J.; Hirschmann, M.T. The role of bone void fillers in medial opening wedge high tibial osteotomy: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2016, 24, 3584–3598. [Google Scholar] [CrossRef]
- Warden, S.J.; Morris, H.G.; Crossley, K.M.; Brukner, P.D.; Bennell, K.L. Delayed- and non-union following opening wedge high tibial osteotomy: Surgeons’ results from 182 completed cases. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2005, 13, 34–37. [Google Scholar] [CrossRef]
- Won, J.Y.; Park, C.Y.; Bae, J.H.; Ahn, G.; Kim, C.; Lim, D.H.; Cho, D.W.; Yun, W.S.; Shim, J.H.; Huh, J.B. Evaluation of 3D printed PCL/PLGA/beta-TCP versus collagen membranes for guided bone regeneration in a beagle implant model. Biomed. Mater. 2016, 11, 055013. [Google Scholar] [CrossRef]
- Yacobucci, G.N.; Cocking, M.R. Union of medial opening-wedge high tibial osteotomy using a corticocancellous proximal tibial wedge allograft. Am. J. Sports Med. 2008, 36, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Yoo, M.J.; Shin, Y.E. Open Wedge High Tibial Osteotomy and Combined Arthroscopic Surgery in Severe Medial Osteoarthritis and Varus Malalignment: Minimum 5-Year Results. Knee Surg. Relat. Res. 2016, 28, 270–276. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grouping According to LHF | Nonlateral Group (N = 10) | LHF Group (N = 8) | p Value |
|---|---|---|---|
| Correction angle (°) | 10.6 ± 0.7 | 9.8 ± 1.0 | 0.087 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, G.; Kim, J.-Y.; Shim, J.-H.; An, S.-H.; Kim, J.; Kim, C.; Lee, I.-G.; Shin, J.-M.; Lee, B. Three-Dimensional Printed Customized Scaffolds Covered with Decellularized Bone Extracellular Matrix for Open-Wedge High-Tibial Osteotomy. Bioengineering 2024, 11, 1129. https://doi.org/10.3390/bioengineering11111129
Ahn G, Kim J-Y, Shim J-H, An S-H, Kim J, Kim C, Lee I-G, Shin J-M, Lee B. Three-Dimensional Printed Customized Scaffolds Covered with Decellularized Bone Extracellular Matrix for Open-Wedge High-Tibial Osteotomy. Bioengineering. 2024; 11(11):1129. https://doi.org/10.3390/bioengineering11111129
Chicago/Turabian StyleAhn, Geunseon, Jun-Young Kim, Jin-Hyung Shim, Sang-Hyun An, Junsik Kim, Changhwan Kim, In-Gyu Lee, Jung-Min Shin, and Byunghoon Lee. 2024. "Three-Dimensional Printed Customized Scaffolds Covered with Decellularized Bone Extracellular Matrix for Open-Wedge High-Tibial Osteotomy" Bioengineering 11, no. 11: 1129. https://doi.org/10.3390/bioengineering11111129
APA StyleAhn, G., Kim, J.-Y., Shim, J.-H., An, S.-H., Kim, J., Kim, C., Lee, I.-G., Shin, J.-M., & Lee, B. (2024). Three-Dimensional Printed Customized Scaffolds Covered with Decellularized Bone Extracellular Matrix for Open-Wedge High-Tibial Osteotomy. Bioengineering, 11(11), 1129. https://doi.org/10.3390/bioengineering11111129