1. Introduction
Aging is a slow, progressive, and uneven process that depends on the physical, psychological, genetic, and environmental variability of each person. While older people experience “successful” or “typical” aging, others will progressively lose autonomy.
Described since the 70s, frailty syndrome is a dynamic and evolving geriatric concept involving numerous dimensions of everyday life and leading to the risk of developing a loss of autonomy. It corresponds to a precarious state of equilibrium linked to the reduction of physiological reserves due to aging and is responsible for the inability to respond to physical, psychological, or social stress. Its management requires medical, social, and psychological interventions [
1].
Regardless of the models used for estimating the aging of the French population, the results converge: the percentage of people aged 65 and over will increase sharply until 2040. Two causes have been well identified: The Baby Boom generation reaching this age group and the increase in life expectancy. By 2016, life expectancy will reach 85.3 years for women and 79.3 years for men, respectively. This represents an increase of 1.2 years for women and 2.2 years for men compared to 2006 [
2]. According to INSEE (Institut National de la Statistique et des Études Économiques) demographic projections, one out of four inhabitants will be 65 or over in 2040, compared with 18% in 2013 [
3].
In contrast, life expectancy in good health at age 65, as determined by the number of years without disability, remains stable. As of 2016, it stands at 10.5 years for women and 9.4 years for men. As a result, the rate of dependent elderly people has increased: in 2012, there were 1.2 million dependent people, and this rate will continue to increase, reaching at least two million people by 2040 [
4]. Expenditures related to dependent elderly care has also increased, totaling 23.7 billion euros in 2014 versus 21.1 billion in 2011 [
5].
Considering the aging of the French population, the increasing dependency of elderly persons, and the resulting health and economic consequences, frailty seems to be a major public health issue and a target for preventive medicine.
Frailty is not a spontaneously resolving process, but it might be reversible in cases of early and targeted intervention [
6]. Screening for frailty in primary care, combined with the intervention of a geriatric team if needed, has been proven to limit or even stop the development of frailty syndrome [
7].
The general practitioner plays an important role in the detection and prevention of frailty in elderly individuals through early screening. However, frailty remains difficult to assess in primary care due to the multitude of conflicting definitions and the diagnostic tools available. Moreover, not all of these instruments have been validated in the context of general medicine, and their implementation is not systematically adapted for general practitioners [
8].
Ideally, as with any screening tool, these frailty detection scores should be sensitive enough to identify as many frail individuals as possible, but also specific enough to avoid conducting a standardized geriatric test that is not very useful or efficient for those who are not frail. These scores must be validated by comparing them to benchmark tools. Finally, to be useful, a frailty detection score must be relevant for all health practitioners (whether or not they are doctors), which means we need a simple and reproducible set of criteria in order to avoid a lengthy training period beforehand. A tool with these characteristics should be easy to use.
There is no consensus regarding frailty diagnostic criteria. The prevalence of frailty depends on the tool used. In the European SHARE study, the prevalence of frailty varied from 6% to 43% depending on the eight tools used [
1,
2,
3,
4,
5,
6,
7,
8,
9]. These tools were validated by international cohort studies for diagnosing frailty, but appear difficult to use in general medical practice. Due to this, we developed a tool for identifying frailty in general medicine for independent subjects over 65 years old that is intended to be quick and easy to use. It takes into account the various factors related to the risk of frailty (social, cognitive, nutritional, iatrogenic, and falls).
The objective of our study was to determine the performance of the “Zulfiqar Frailty Scale” (ZFS) tool to detect frailty (as defined by Fried’s criteria) in this ambulatory population and to compare it to other scales such as the Gerontopole Frailty Screening Tool (GFST), the modified Short Emergency Geriatric Assessment (mSEGA) Grid A, and the comprehensive geriatric assessment (CGA). Its secondary objectives were to evaluate the feasibility and acceptability of our “ZFS” tool in the setting of a primary care consultation and to evaluate the prevalence of each element of the “ZFS” composite tool in a population of older subjects seeing general practitioners.
3. Results
3.1. Characteristics of the Study Population
During our study, we offered the screening to 102 patients.
A total of 102 patients were included with a mean age of 82 years. There were 55 women (53.8%) and 47 men (see
Table 2).
3.3. Use of the ZFS Scale
In scoring the ZFS scale, each positive response was given a score of one point, for a maximum of six points per patient evaluation. The average score for our scale was 3.32 ± 1.55. The item “Weight loss ≥ 5% in 6 months” was found in 17 patients (16.7%); a positive response for “Fall risk according to monopodal support test” was found in 69 patients (67.6%); 40 patients responded positively (39.2%) to feeling “Lonely”; the presence of home assistance was noted in 46 subjects (45.1%); “Complaints of memory problems” was found in 67 subjects (65.7%); and 74 patients (72.5%) were positive with respect to “≥5 therapeutic classes”. An elderly patient was considered fragile when the ZFS score was ≥3. As a result, 76 subjects (74.5%) were classified as frail. The average completion time for the analysis was 109.62 s ± 9.24.
The distribution of each category is shown in
Table 7, and we studied the internal consistency of our questionnaire (see
Table 8 and
Table 9).
3.4. Comprehensive Geriatric Assessment (CGA)
After a comprehensive geriatric assessment, frailty syndrome was found in 57 patients (55.9%).
3.5. Concordance Study
Concordance with the comprehensive geriatric assessment (CGA) is shown in
Table 10.
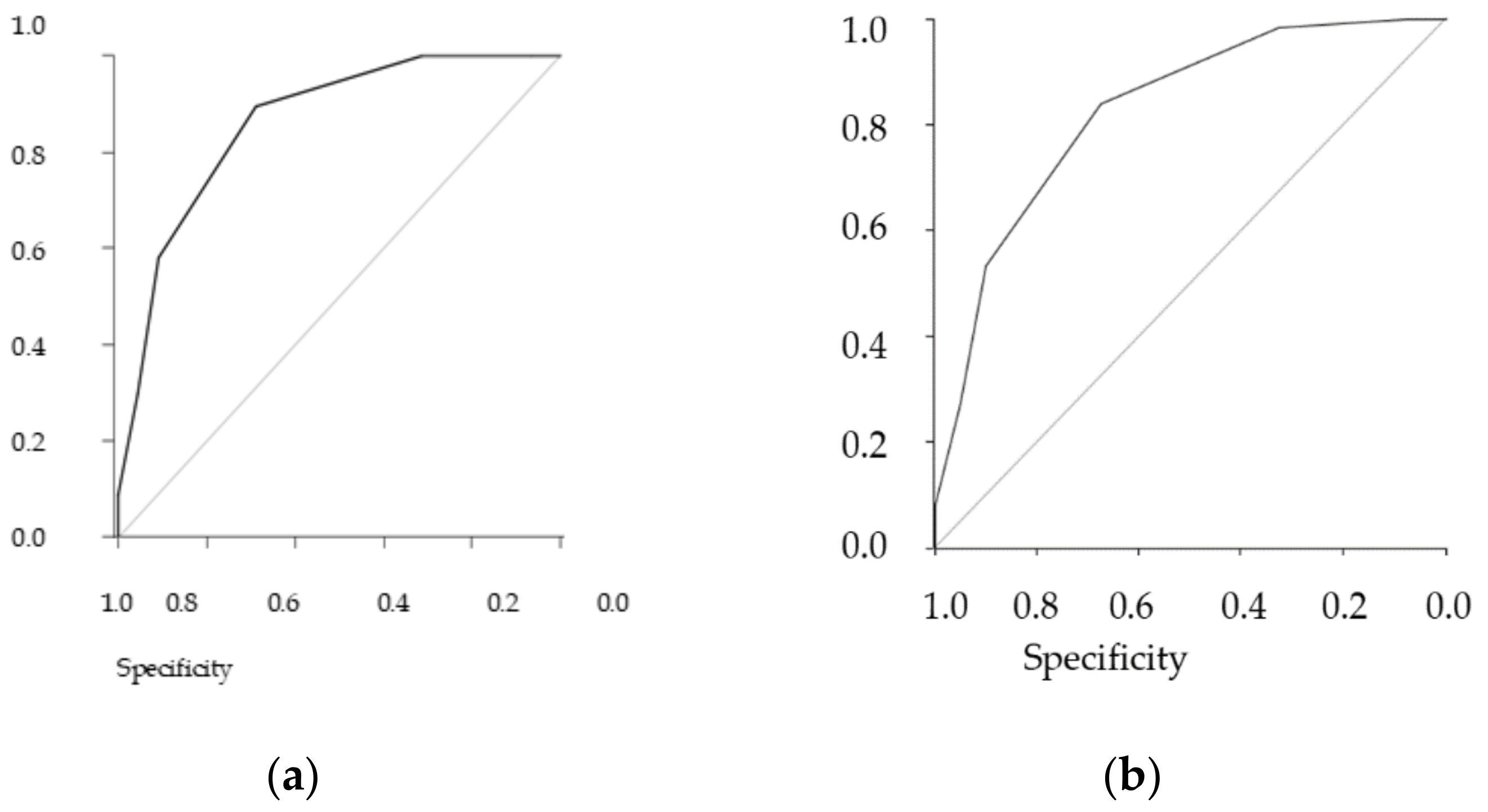
The table shows the results stratified by three different definitions of frailty, the performance of the GFST, and the ZFS. The gold standard is the comprehensive geriatric assessment (CGA), and we added the Fried scale as an additional reference standard (see
Figure 1 (
Figure 1a,b).
In general, both scales showed solid performance, and differences between them in the sample were minimal. As the CGA showed a prevalence of frailty of 55.9%, a similar prevalence threshold for the ZFS (i.e., 64% at the threshold ≥3) could be assessed (see
Table 11 and
Table 12 for analyses of concordance).
Sensibility was 89.5% (CI95: 78.5% to 96%), while specificity was 68.9% (CI95: 53.4% to 81.8%). The positive predictive value was 78.5% (CI95: 66.5 % to 87.7%), and the negative predictive value was 83.8% (CI95: 68% to 93.8%).
Sensibility was 83.9% (CI95% (confidence interval): 72.3 to 92%), while specificity was 67.5% (CI95%: 50.9 to 81.4%). The positive predictive value was 80% (CI95%: 68.2 to 88.9%), and the negative predictive value was 73% (CI95%: 55.9 to 86.2%).
Whether comparing the concordance of the ZFS with the Fried or CGA scores, the results were the same.
The Pearson correlations between the geriatric scores are shown in
Table 13.
3.6. Feasibility of the “ZFS” Tool in General Medicine
On average, it took 109.62 s ± 9.24.
Our tool was very well-received by patients, with an acceptability rating of 9.8/10 using the visual analog scale.
4. Discussion
General practitioners are usually best suited to screen for frailty due to their frequent contact with elderly patients and the influence they can have on patients’ futures through their coordination of care with other health, medical, paramedical, and social service professionals. Fried’s criteria are the worldwide standard for frailty screening among elderly patients, particularly during comprehensive geriatric assessments conducted by geriatricians. However, the use of a dynamometer makes it difficult to apply these frailty screening criteria in the context of primary care. The Fried scale is widely known [
10], but its inclusion in measurements is not routinely used for patient assessment. Additionally, there are no psychosocial components in the Fried scale.
The Gerontopole Frailty Screening Tool (GFST) consists of two parts: a questionnaire conducted first, and the clinician’s assessment of frailty [
11,
12]. A limitation of this scale is that it does not provide specific guidance for clinicians regarding the identification of frailty. Moreover, most of the items are subjective.
The seven-item Program of Research to Integrate the Services for the Maintenance of Autonomy (PRISMA-7) scale contains seven simple self-reported components. A total score ≥3 is considered frail [
16]. It has a high level of accuracy in identifying frailty in community-dwelling older people [
17], but has a tendency to over-screen for frailty [
18].
The Frailty Index (FI) of Cumulative Deficits (FI-CD) was proposed by Rockwood and Mitninski. It has been well validated and has a higher predictive ability of adverse clinical events than other frailty measurements in both hospital and community settings [
19,
20], but it has some limitations and is time consuming. There is also a Frailty Index derived from the comprehensive geriatric assessment (CGA). It is used as a clinical standard for frailty assessment and has been found to be highly correlated with the FI-CD [
21]. It is also time consuming.
The proportion of frail individuals in our sample was similar to that obtained through the Fried and SEGA grid A scale: 63.7% in our scale, 67.7% in the SEGA grid A, 75.5% in the GFST, and 60.8% for Fried’s criteria (if at least three criteria were present). The ZFS was easy to implement and showed an appropriate level of sensitivity and negative predictive value in our study group. The tool detects frailty if at least three criteria are met. The purpose of this tool is to identify frailty in outpatients and to refer them to a geriatric team for a standardized geriatric evaluation so that they can establish a personalized plan of care (PPC). In the identification of frailty in outpatients, our scale was no less discriminating than the Fried scale. Other scales used in geriatric evaluation such as the G8 [
22] have been shown to have a sensitivity similar to ours (87% for G8).
The ZFS has several advantages. It does not require previous training on the part of caregivers, and it is not time consuming, an advantage for medical consultation in elderly people. The time estimated for consultation in general medicine in France is approximately 15 min [
23]. With our scale, frailty screening can be assessed in 2 min, which is similar to the GFST scale. The time is longer for the Fried scale and for the SEGA grid A (from 6 to 10 min) [
6], making them more difficult for general practitioners to apply during consultation. A practical tool should require a minimum of time to complete, similar to ours. In contrast to the Fried scale, the ZFS does not require additional equipment such as a dynamometer for the determination of the isometric contraction. This is a real advantage in the context of wide-scale screening. Another advantage of the ZFS compared to the GFST scale is its higher level of objectivity for its selected criteria. Indeed, the GFST scale contains questions that are more subjective, while our tool is more objective and easy to assess. It is a quick tool that requires no prior training and no specific equipment or facilities, making it a feasible screening tool suitable for general practice. Our tool has the advantage of requiring no equipment whatsoever, making it perfectly suitable for primary care. It can be used by general practitioners, in addition to other health professionals such as nurses, physiotherapists, and occupational therapists.
Limitations
Our study sample was small. To be validated for the purpose of studying its reproducibility, our tool will need to be tested in multiple primary care clinics, in both urban and rural areas, and across a larger sample with many types of practitioners (doctors, nurses, physical therapists, occupational therapists, etc.). The prediction of pathological events (falls, hospitalization, and morbidity-mortality) was not studied in this research. This will begin in March 2021 for an 18-month period. The cognitive question remains difficult to understand with a rapid detection score such as ours. The question “Does the person complain of memory problems?” is still subjective and requires, as we have done, a response confirmed by the patient’s family.





{kind=link}