
Comorbidity Patterns in Patients at Cardiovascular Hospital Admission

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
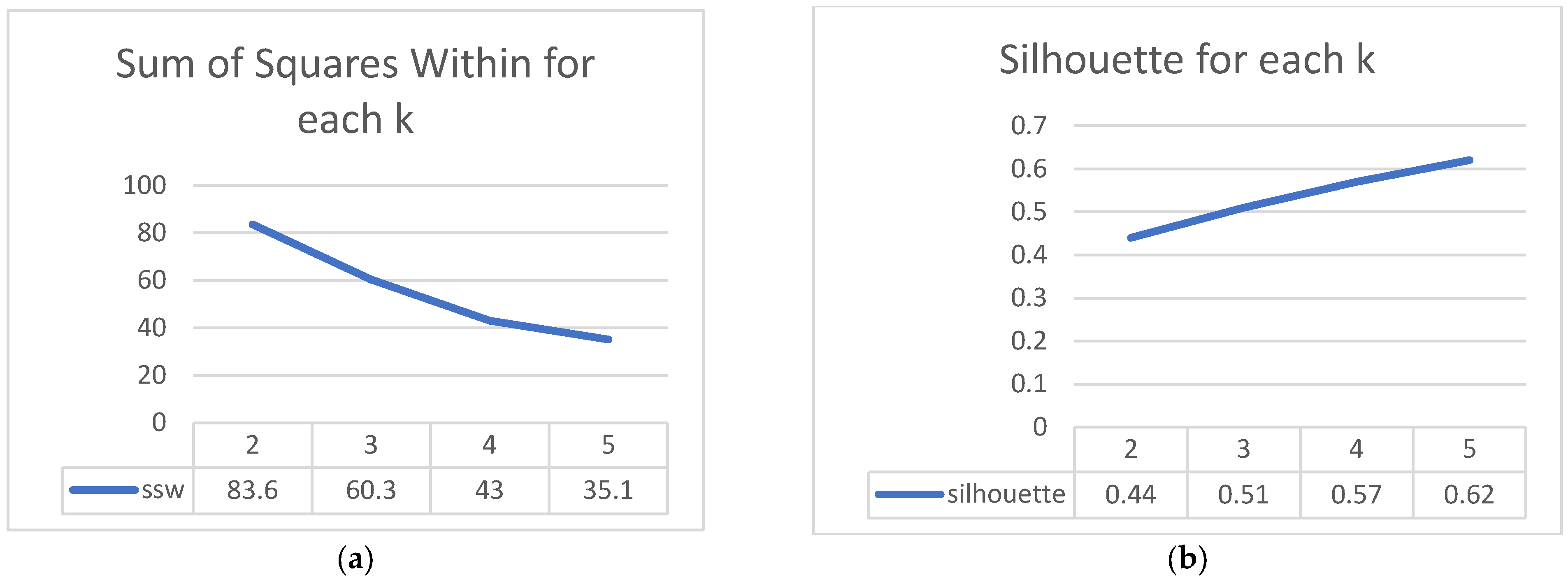
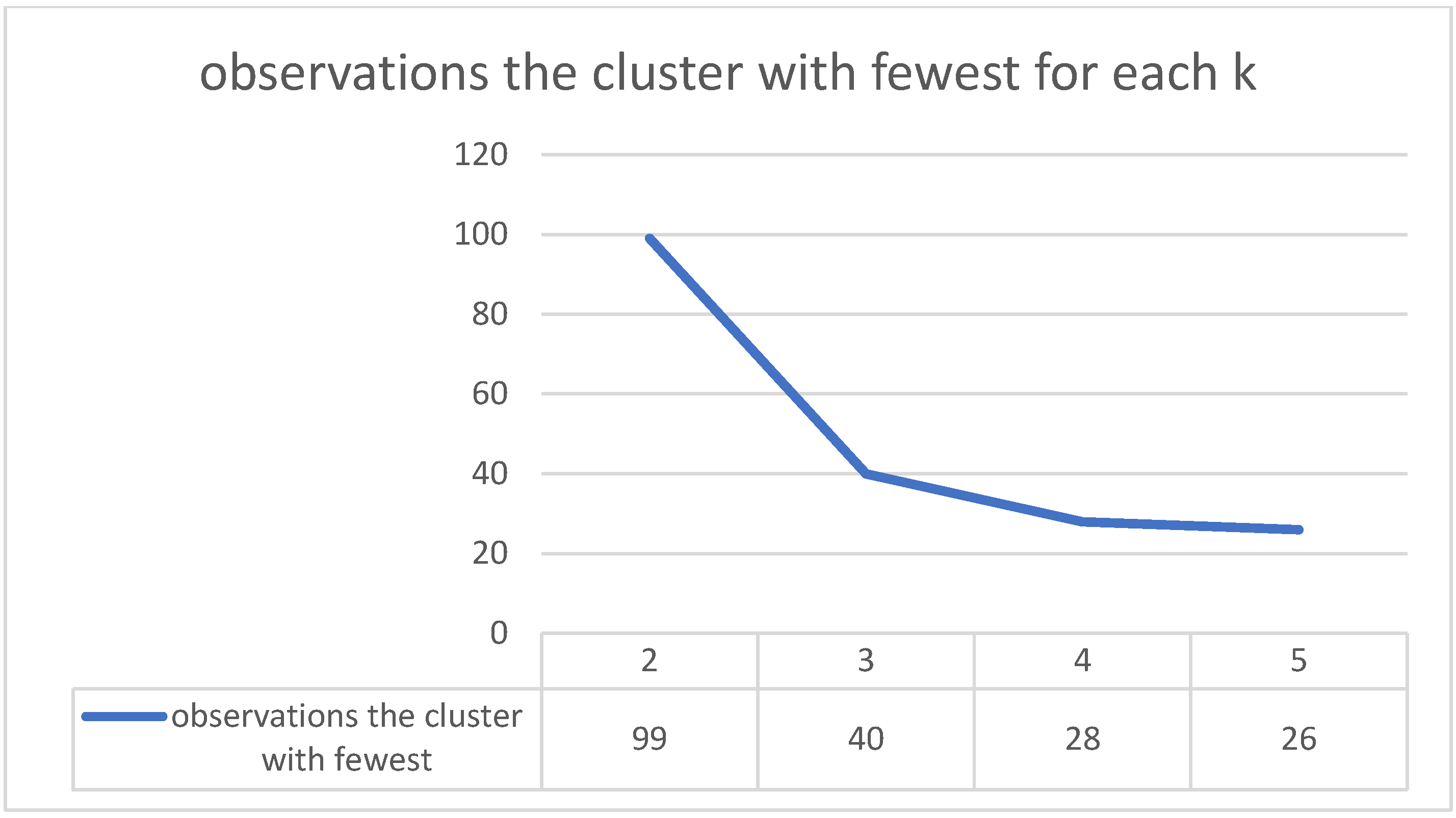
2.1. Methodology
2.2. Data
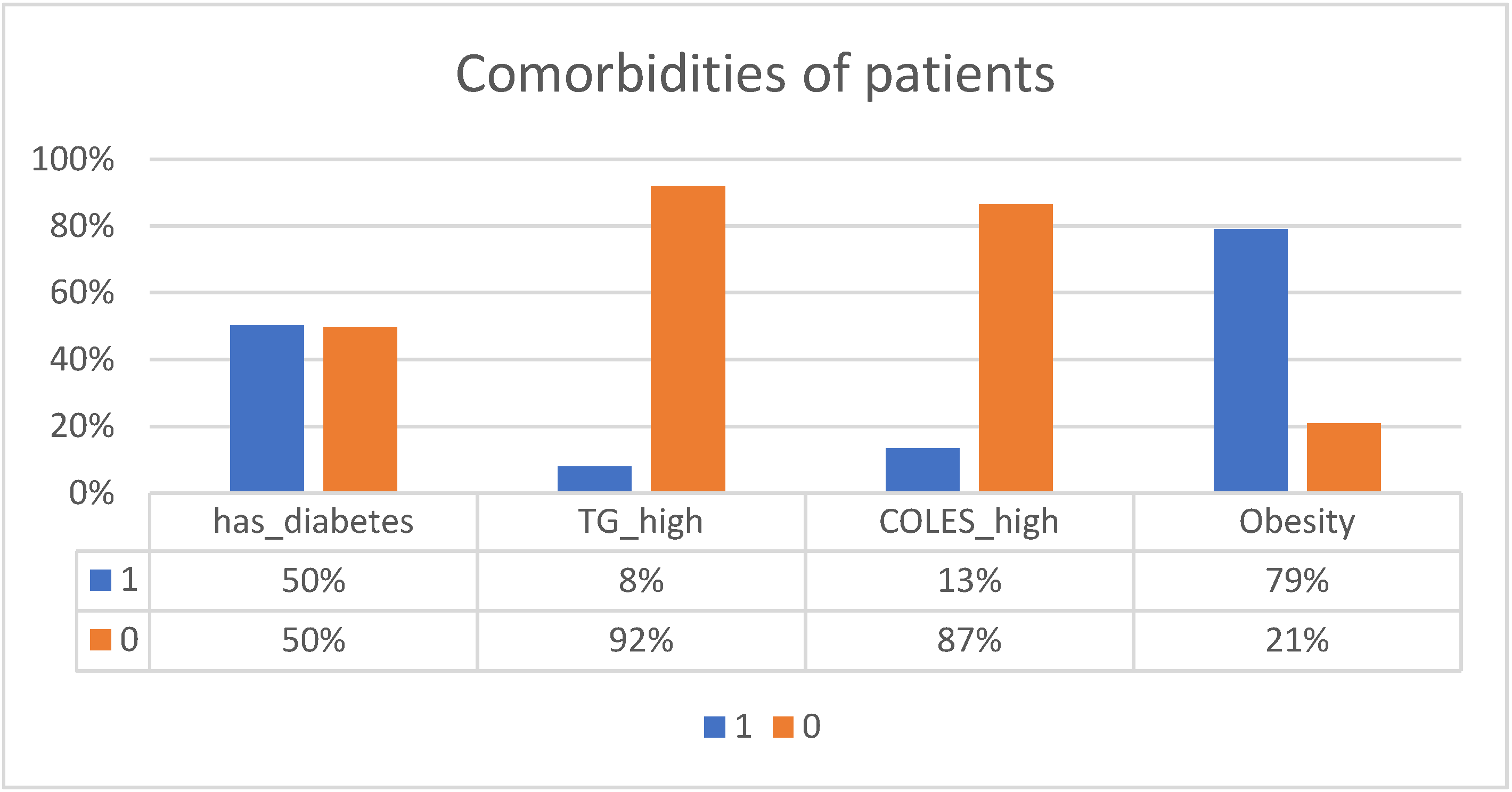
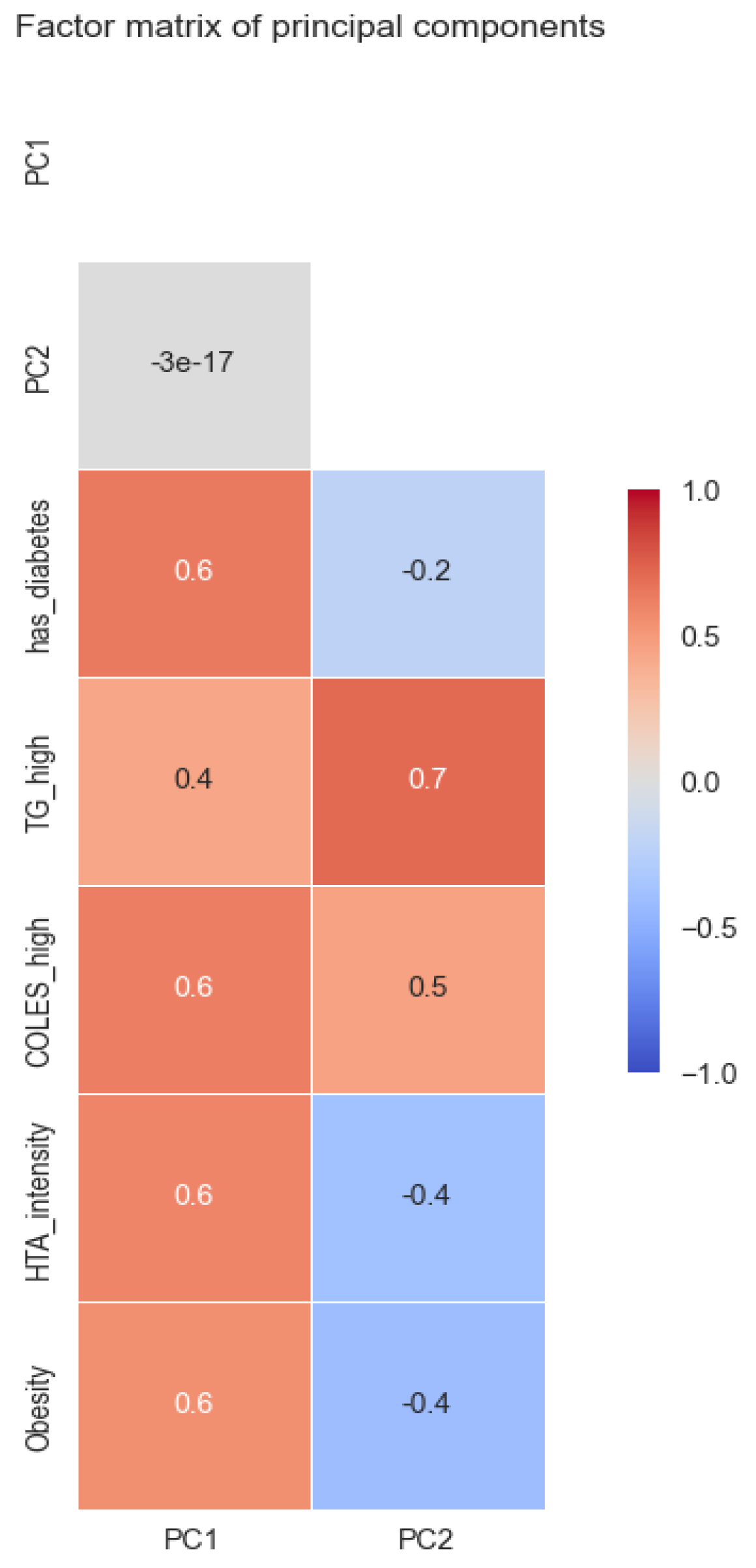
- TG_high: binary variable with 1 when triglycerides are over 200, else 0;
- COLES_high: binary variable with 1 when cholesterol is over 240, else 0;
- Obesity: binary variable with 1 when the patient has any stages of obesity (BMI over 30), else 0;
- Has_diabetes: binary variable with 1 when patient has diabetes, else 0;
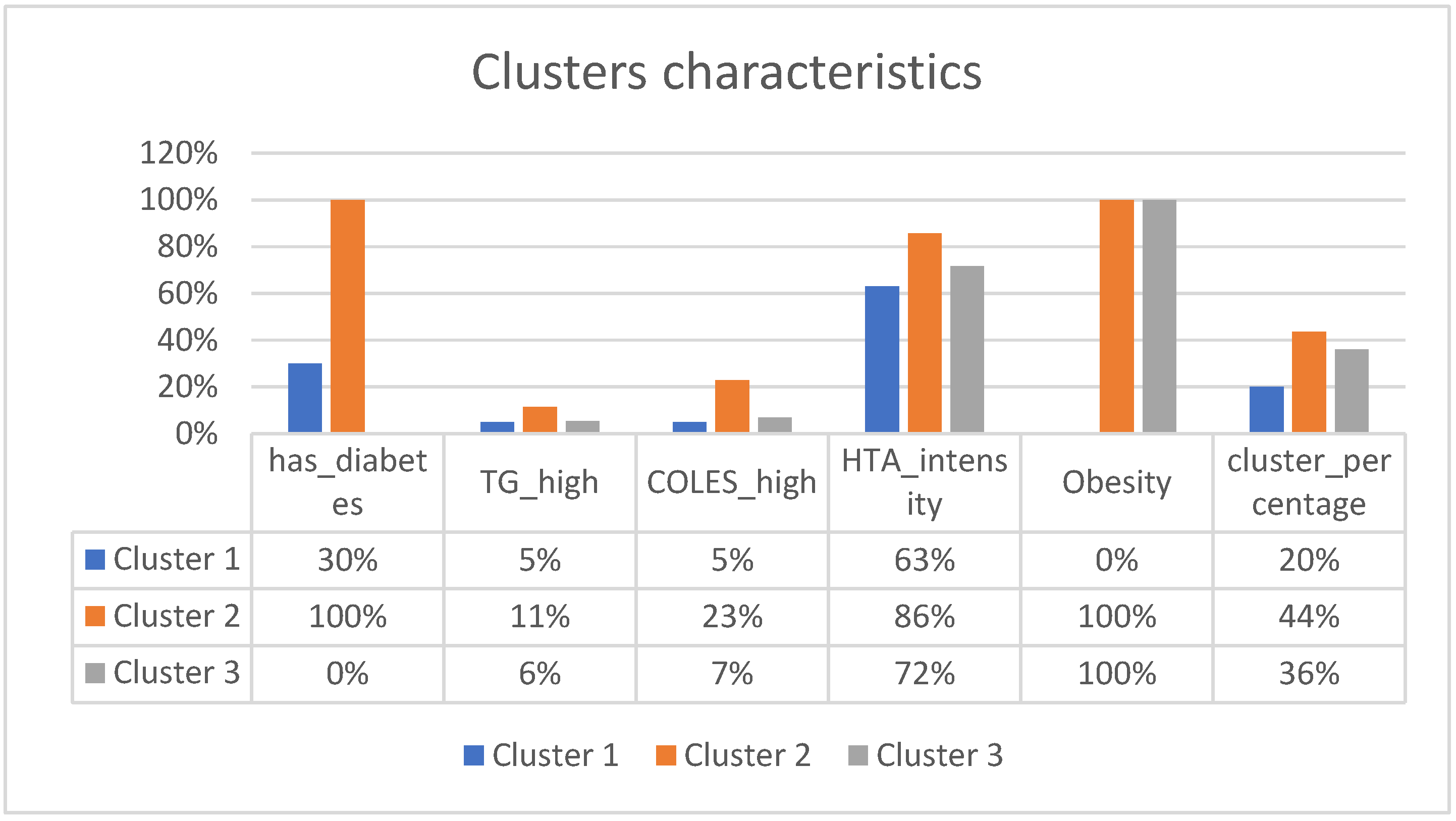
- HTA_intensity: ordinal variable for hypertension. This reflects the hypertension intensity and is made based on hypertension stages; no hypertension has a value of 0, stage 1 has a value of 0.33, stage 2 has a value of 0.66, and stage 3 has a value of 1.
2.3. Descriptive Statistics
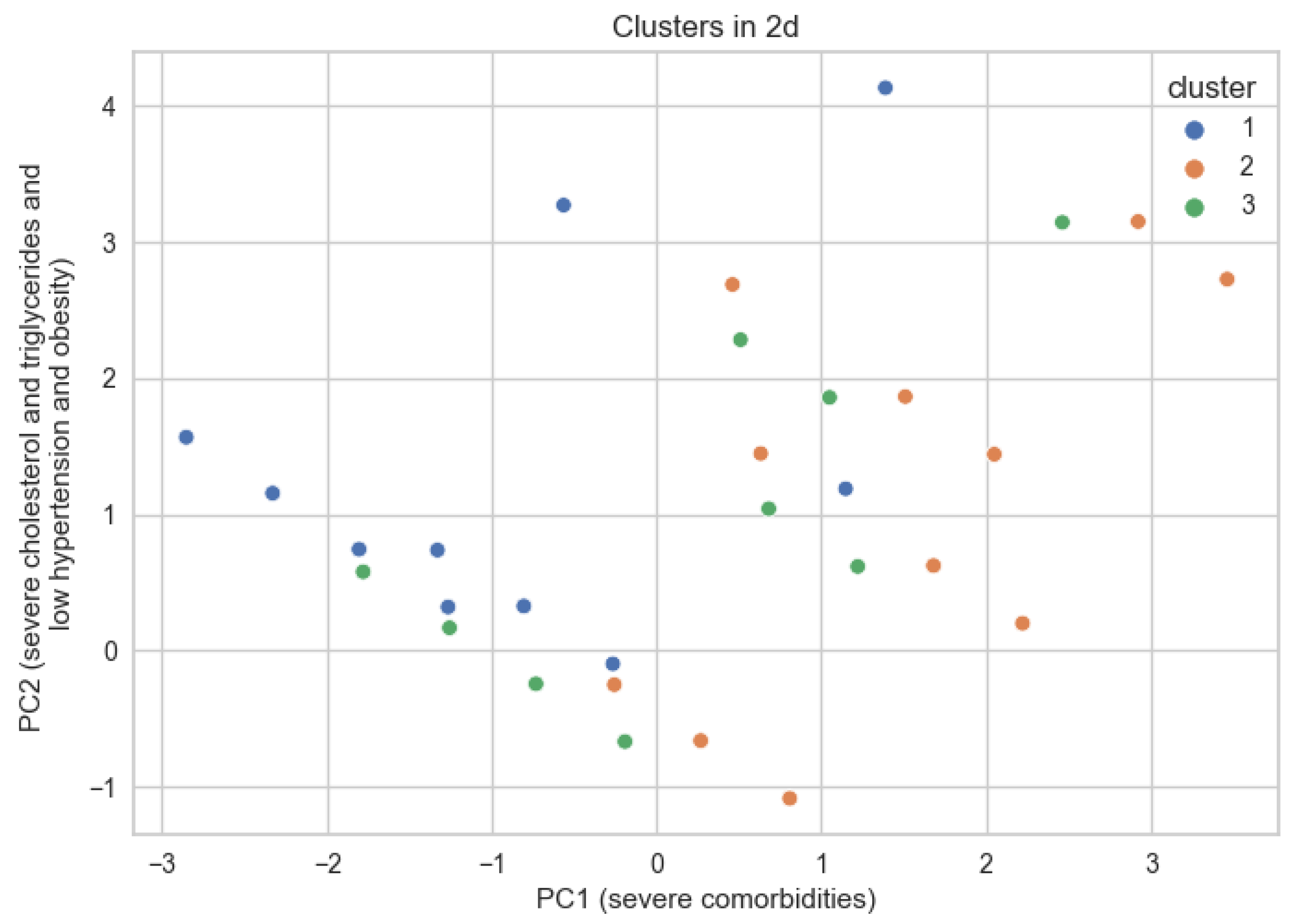
Comorbidity Dimensions
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases (CVDs) Fact Sheet. Available online: https://www.who.int/en/newsroom/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 1 January 2022).
- Capewell, S.; O’Flaherty, M. Rapid mortality falls after risk-factor changes in populations. Lancet 2011, 378, 752–753. [Google Scholar] [CrossRef] [PubMed]
- Hunt, S.A.; Abraham, W.T.; Chin, M.H.; Feldman, A.M.; Francis, G.S.; Ganiats, T.G.; Jessup, M.; Konstam, M.A.; Mancini, D.M.; Michl, K.; et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult. Circulation 2005, 112, e154–e235. [Google Scholar] [CrossRef]
- Swedberg, K.; Cleland, J.; Dargie, H.; Drexler, H.; Follath, F.; Komajda, M.; Tabazzi, L.; Smiseth, O.A.; Gavazzi, A.; Haverich, A.; et al. Guidelines for the diagnosis and treatment of chronic heart failure: Executive summary (update 2005). Eur. Heart J. 2005, 26, 1115–1140. [Google Scholar] [CrossRef]
- Mosterd, A.; Hoes, A.W. Clinical epidemiology of heart failure. Heart 2007, 93, 1137–1146. [Google Scholar] [CrossRef]
- Cowie, M. Incidence and aetiology of heart failure; a population-based study. Eur. Heart J. 1999, 20, 421–428. [Google Scholar] [CrossRef]
- Ather, S.; Chan, W.; Bozkurt, B.; Aguilar, D.; Ramasubbu, K.; Zachariah, A.A.; Wehrens, X.H.T.; Deswal, A. Impact of noncardiac comorbidities on morbidity and mortality in a predominantly male population with heart failure and preserved versus reduced ejection fraction. J. Am. Coll. Cardiol. 2012, 59, 998–1005. [Google Scholar] [CrossRef]
- Cheitlin, M.D. Clinical presentation, management, and in-hospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: A report from the Acute Decompensated Heart Failure National Registry (adhere) database. Yearb. Cardiol. 2007, 2007, 329–330. [Google Scholar] [CrossRef]
- Braunstein, J.B.; Anderson, G.F.; Gerstenblith, G.; Weller, W.; Niefeld, M.; Herbert, R.; Wu, A.W. Noncardiac comorbidity increases preventable hospitalizations and mortality among Medicare beneficiaries with chronic heart failure. J. Am. Coll. Cardiol. 2003, 42, 1226–1233. [Google Scholar] [CrossRef]
- Eckel, R.H.; Jakicic, J.M.; Ard, J.D.; de Jesus, J.M.; Houston Miller, N.; Hubbard, V.S.; Lee, I.M.; Lichtenstein, A.H.; Loria, C.M.; Millen, B.E.; et al. 2013 AHA/ACC guideline on Lifestyle Management to reduce cardiovascular risk. J. Am. Coll. Cardiol. 2014, 63, 2960–2984. [Google Scholar] [CrossRef]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Noel Bairey Merz, C.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation 2014, 129, S1–S45. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults. Circulation 2014, 129 (Suppl. 2), S102–S138. [Google Scholar] [CrossRef]
- Fields, L.E.; Burt, V.L.; Cutler, J.A.; Hughes, J.; Roccella, E.J.; Sorlie, P. The burden of adult hypertension in the United States 1999 to 2000. Hypertension 2004, 44, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Stamler, J. Blood pressure, systolic and diastolic, and cardiovascular risks. US Population Data. Arch. Intern. Med. 1993, 153, 598–615. [Google Scholar] [CrossRef] [PubMed]
- Vasan, R.S.; Beiser, A.; Seshadri, S.; Larson, M.G.; Kannel, W.B.; D’Agostino, R.B.; Levy, D. Residual lifetime risk for developing hypertension in middle-aged women and men. JAMA 2002, 287, 1003–1010. [Google Scholar] [CrossRef]
- He, J.; Ogden, L.G.; Bazzano, L.A.; Vupputuri, S.; Loria, C.; Whelton, P.K. Risk factors for congestive heart failure in US men and women. Arch. Intern. Med. 2001, 161, 996. [Google Scholar] [CrossRef]
- Kannel, W.B. Diabetes and cardiovascular disease. JAMA 1979, 241, 2035. [Google Scholar] [CrossRef]
- Arnold, J.M.O.; Yusuf, S.; Young, J. Prevention of heart failure in patients in the Heart Outcomes Prevention Evaluation (HOPE) study. ACC Curr. J. Rev. 2003, 12, 57. [Google Scholar] [CrossRef]
- Lewis, E.F.; Moye, L.A.; Rouleau, J.L. Predictors of late development of heart failure in stable survivors of myocardial infarction. the care study. ACC Curr. J. Rev. 2004, 13, 32. [Google Scholar] [CrossRef]
- Lewis, E.F.; Solomon, S.D.; Jablonski, K.A.; Murguia Rice, M.; Clemenza, F.; Hsia, J.; Maggioni, A.P.; Zabalgoitia, M.; Huynh, T.; Cuddy, T.E.; et al. Predictors of heart failure in patients with stable coronary artery disease. Circ. Heart Fail. 2009, 2, 209–216. [Google Scholar] [CrossRef]
- Ingelsson, E.; Sundström, J.; Ärnlöv, J.; Zethelius, B.; Lind, L. Insulin resistance and risk of congestive heart failure. JAMA 2005, 294, 334. [Google Scholar] [CrossRef]
- Matsushita, K.; Blecker, S.; Pazin-Filho, A.; Bertoni, A.; Chang, P.P.; Coresh, J.; Selvin, E. The Association of Hemoglobin a1c with incident heart failure among people without diabetes: The atherosclerosis risk in communities study. Diabetes 2010, 59, 2020–2026. [Google Scholar] [CrossRef]
- Alexander, J.K. Obesity and the heart. Curr. Probl. Cardiol. 1980, 5, 1–41. [Google Scholar] [CrossRef]
- Alpert, M.A.; Terry, B.E.; Mulekar, M.; Cohen, M.V.; Massey, C.V.; Fan, T.M.; Panayiotou, H.; Mukerji, V. Cardiac morphology and left ventricular function in normotensive morbidly obese patients with and without congestive heart failure, and effect of weight loss. Am. J. Cardiol. 1997, 80, 736–740. [Google Scholar] [CrossRef]
- Seide, M.J. Heart failure due to extreme obesity. N. Engl. J. Med. 1957, 257, 1227–1230. [Google Scholar] [CrossRef] [PubMed]
- Kenchaiah, S.; Evans, J.C.; Levy, D.; Wilson, P.W.F.; Benjamin, E.J.; Larson, M.G.; Kannel, W.B.; Vasan, R.S. Obesity and the risk of heart failure. N. Engl. J. Med. 2002, 347, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Pekkanen, J.; Linn, S.; Heiss, G.; Suchindran, C.M.; Leon, A.; Rifkind, B.M.; Tyroler, H.A. Ten-year mortality from cardiovascular disease in relation to cholesterol level among men with and without preexisting cardiovascular disease. N. Engl. J. Med. 1990, 322, 1700–1707. [Google Scholar] [CrossRef]
- Kannel, W.B.; Belanger, A.J. Epidemiology of Heart Failure. Am. Heart J. 1991, 121, 951–957. [Google Scholar] [CrossRef] [PubMed]
- O’Flaherty, M.; Buchan, I.; Capewell, S. Contributions of treatment and lifestyle to declining CVD mortality: Why have CVD mortality rates declined so much since the 1960s? Heart 2012, 99, 159–162. [Google Scholar] [CrossRef]
- Koopman, C.; Bots, M.L.; van Dis, I.; Vaartjes, I. Shifts in the age distribution and from acute to chronic coronary heart disease hospitalizations. Eur. J. Prev. Cardiol. 2014, 23, 170–177. [Google Scholar] [CrossRef]
- Feinstein, A.R. Clinical Judgment; Williams & Wilkins: New York, NY, USA, 1967. [Google Scholar]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and Medical Education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Vos, R.; van den Akker, M.; Boesten, J.; Robertson, C.; Metsemakers, J. Trajectories of multimorbidity: Exploring patterns of multimorbidity in patients with more than ten chronic health problems in life course. BMC Fam. Pract. 2015, 16, 2. [Google Scholar] [CrossRef] [PubMed]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soysaler, C.-A.; Andrei, C.L.; Ceban, O.; Sinescu, C.-J. Comorbidity Patterns in Patients at Cardiovascular Hospital Admission. Medicines 2023, 10, 26. https://doi.org/10.3390/medicines10040026
Soysaler C-A, Andrei CL, Ceban O, Sinescu C-J. Comorbidity Patterns in Patients at Cardiovascular Hospital Admission. Medicines. 2023; 10(4):26. https://doi.org/10.3390/medicines10040026
Chicago/Turabian StyleSoysaler, Cezara-Andreea, Cătălina Liliana Andrei, Octavian Ceban, and Crina-Julieta Sinescu. 2023. "Comorbidity Patterns in Patients at Cardiovascular Hospital Admission" Medicines 10, no. 4: 26. https://doi.org/10.3390/medicines10040026
APA StyleSoysaler, C.-A., Andrei, C. L., Ceban, O., & Sinescu, C.-J. (2023). Comorbidity Patterns in Patients at Cardiovascular Hospital Admission. Medicines, 10(4), 26. https://doi.org/10.3390/medicines10040026