
Safety and Evaluation of the Immune Response of Coronavirus Nosode (BiosimCovex) in Healthy Volunteers: A Preliminary Study Extending the Homeopathic Pathogenetic Trial

Abstract
1. Introduction
Objective
2. Materials and Methods
2.1. BiosimCovex (Coronavirus Nosode)
2.2. Study Design
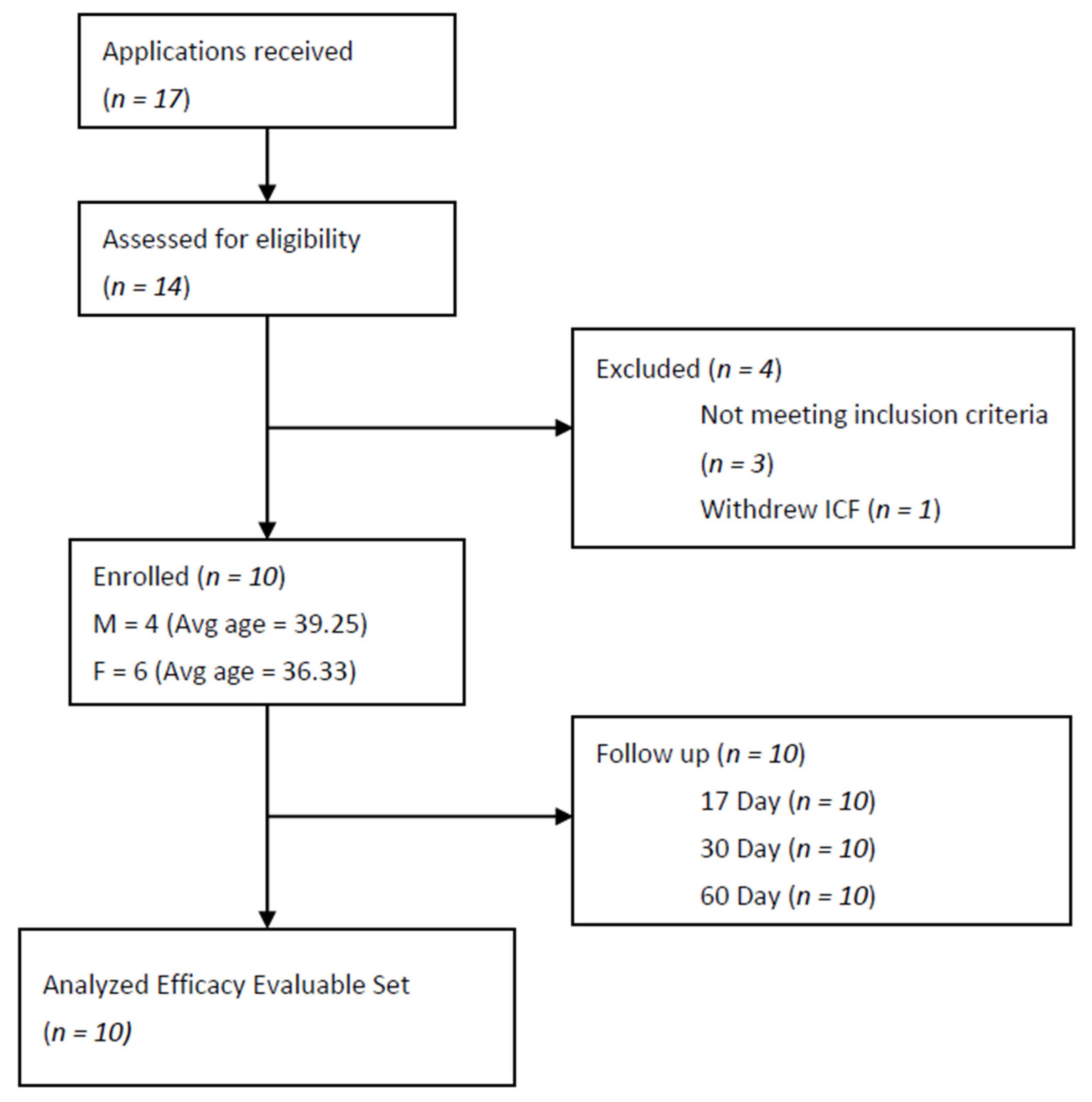
2.3. Study Sample
2.4. Inclusion Criteria
2.5. Exclusion Criteria
2.6. Study Method
2.7. Approvals
2.8. Study End Points and Statistical Assessments
2.9. Safety Assessments
2.10. Safety Parameters
2.11. Immune Response Laboratory Method Parameters
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Masyeni, S.; Iqhrammullah, M.; Frediansyah, A.; Nainu, F.; Tallei, T.; Emran, T.B.; Ophinni, Y.; Dhama, K.; Harapan, H. Molnupiravir: A lethal mutagenic drug against rapidly mutating SARS-CoV-2—A narrative review. J. Med. Vir. 2022, 94, 3006–3016. [Google Scholar] [CrossRef] [PubMed]
- Sharun, K.; Tiwari, R.; Yatoo, M.I.; Natesan, S.; Megawati, D.; Singh, K.P.; Michalak, I.; Dhama, K. A comprehensive review on pharmacologic agents, immunotherapies and supportive therapeutics for COVID-19. Narra J. 2022, 2, e92. [Google Scholar] [CrossRef]
- Hahnemann, S. Materia Medica Pura; Reprinted Ed.; B Jain Publishers Pvt. Ltd.: New Delhi, India, 1986. [Google Scholar]
- Allen, T.F. The Encyclopedia of Pure Materia Medica; B Jain Publishers Pvt. Ltd.: New Delhi, India, 1988; Volume 4, p. v. [Google Scholar]
- Hering, C. Guiding Symptoms of our Materia Medica; Reprint Ed.; B Jain Publishers Pvt. Ltd.: New Delhi, India, 1989; Volume 10. [Google Scholar]
- Homeopathic Pharmacopoeia Convention of the United States. Monograph: Anas Barbariae Hepatis et Cordis Extractum; GIRI: Southeastern, PA, USA, 2012. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5788925/#b10-ceor-10-075 (accessed on 14 February 2019).
- A Ready Reckoner of Medicine in Homeopathic Pharmacopeia; CCRH: New Delhi, India, 2019.
- Government of India. Drugs and Cosmetic Act 1940. Schedule Y. Central Drugs Standard Control Organisation. Available online: https://cdsco.gov.in/opencms/opencms/en/Acts-Rules/ (accessed on 1 November 2022).
- Loeb, M.; Russell, M.L.; Neupane, B.; Thanabalan, V.; Singh, P.; Newton, J.; Pullenayegum, E. A randomized, blinded, placebo-controlled trial comparing antibody responses to homeopathic and conventional vaccines in university students. Vaccine 2018, 36, 7423–7429. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Talele, G. An open-label, exploratory documentation of proving-symptoms of CVN01 (Coronavirus nosode from the clinical sample) in healthy volunteers. Int. J. High Dilution Res. 2021, 20, 44–50. [Google Scholar] [CrossRef]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef] [PubMed]
- Talele, G.; Chowdhary, A.; Vaidya, S.; Deshmukh, R.; Rawal, R.; Shah, R. Preparation of Coronavirus Nosodes Sourced from a Clinical Sample of SARS-Cov-2 Positive Patient, Inactivated Strain, and Spike Glycoprotein. Int. J. High Dilution Res. 2020, 19, 02–09. [Google Scholar] [CrossRef]
- Homeopathic Pharmacopeia of India, 1st ed.; Ministry of Health Government of India: New Delhi, India, 1983; Volume IV, pp. 136–137.
- Shah, R. Scientific method of preparing homeopathic nosodes. Indian J. Res. Homoeopath. 2014, 8, 166–174. [Google Scholar] [CrossRef]
- Allen, H.C. The Materia Medica of the Nosodes with Provings of the X-ray; Jain Publishers: New Delhi, India, 1988. [Google Scholar]
- Marot, S.; Calvez, V.; Louet, M.; Marcelin, A.; Burrel, S. Interpretation of SARS-CoV-2 replication according to RT-PCR crossing threshold value. Clin. Microbiol Infect. 2021, 27, 1056–1057. [Google Scholar] [CrossRef]
- Allen, T.F. The Encyclopedia of Pure Materia Medica; B. Jain Publishers: New Delhi, India, 1988; Volume 8, p. 164. [Google Scholar]
- Kent, J.T. Lectures on Homeopathic Materia Medica; Reprint; Jain Publishing Company: New Delhi, India, 1980; p. 1001. [Google Scholar]
- Clarke, J.H. A Dictionary of Practical Materia Medica; Salvator Apotheke: Mödling, Austria, 2014; Available online: http://www.materiamedica.info/en/materia-medica/john-henry-clarke/carcinosinum (accessed on 1 November 2022).
- Kratzel, A.; Todt, D.; V’kovski, P.; Steiner, S.; Gultom, M.; Thao, T.T.N.; Ebert, N.; Holwerda, M.; Steinmann, J.; Niemeyer, D.; et al. Inactivation of Severe Acute Respiratory Syndrome Coronavirus 2 by WHO-Recommended Hand Rub Formulations and Alcohols. Emerg Infect. Dis. 2020, 26, 1592–1595. [Google Scholar] [CrossRef]
- Rose-John, S.; Winthrop, K.; Calabrese, L. The role of IL-6 in the host defense against infections: Immunobiology and clinical implications. Nat. Rev. Rheumatol. 2017, 13, 399–409. Available online: https://www.nature.com/articles/nrrheum.2017.83 (accessed on 1 November 2022). [CrossRef]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef]
- Kishimoto, M.; Narazaki, T. The Two-Faced Cytokine IL-6 in the Host Defense and Diseases. Int J. Mol. Sci. 2018, 19, 3528. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6274717/ (accessed on 1 November 2022).
- Vatansever, H.S.; Becer, E. Relationship between IL-6 and COVID-19: To be considered during treatment. Future Virol. 2020, 15, 817–822. [Google Scholar] [CrossRef]
- Gadotti, A.C.; de Castro Deus, M.; Telles, J.P.; Wind, R.; Goes, M.; Ossoski, R.G.C.; de Padua, A.M.; de Noronha, L.; Moreno-Amaral, A.; Baena, C.P.; et al. IFN-γ is an independent risk factor associated with mortality in patients with moderate and severe COVID-19 infection. Virus Res. 2020, 289, 198171. [Google Scholar] [CrossRef] [PubMed]
- De Bruin, S.; Bos, L.D.; van Roon, M.A.; Tuip-de Boer, A.M.; Schuurman, A.R.; Koel-Simmelinck, M.J.; Bogaard, H.J.; Tuinman, P.R.; van Agtmael, M.A.; Hamann, J.; et al. Clinical features and prognostic factors in COVID-19: A prospective cohort study. EBioMedicine 2021, 67, 103378. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Herscu, P. Provings, Volume I. How Understanding Provings Offers an Essential Foundation to Successful Patient Care—With a Proving of Alcoholus; New England School of Homeopathy: Amherst, MA, USA, 2002; pp. 39–116. [Google Scholar]
- Mohanty, S.; Joshi, S.R.; Ueda, I.; Wilson, J.; Blevins, T.P.; Siconolfi, B.; Meng, H.; Devine, L.; Raddassi, K.; Tsang, S.; et al. Prolonged proinflammatory cytokine production in monocytes modulated by interleukin 10 after influenza vaccination in the older adults. J. Infect. Dis. 2015, 211, 1174–1184. Available online: https://pubmed.ncbi.nlm.nih.gov/25367297/ (accessed on 1 November 2022). [CrossRef]
- Dienz, O.; Rincon, M. The effects of IL-6 on CD4 T cell responses. Clin. Immunol. 2009, 130, 27–33. [Google Scholar] [CrossRef]
- Del Giudice, M.; Gangestad, S.W. Rethinking IL-6 and CRP: Why they are more than inflammatory biomarkers, and why it matters. Brain Behav. Immun. 2018, 70, 61–75. [Google Scholar] [CrossRef]
- Pérez-Galarza, J.; Prócel, C.; Cañadas, C.; Aguirre, D.; Pibaque, R.; Bedón, R.; Sempértegui, F.; Drexhage, H.; Baldeón, L. Immune Response to SARS-CoV-2 Infection in Obesity and T2D: Literature Review. Vaccines 2021, 9, 102. [Google Scholar] [CrossRef]
- Talele, G.; Vaidhya, S.; Chowdhary, A.; Herscu, P.; Shah, R. Randomized double-blind, placebo-controlled feasibility study, evaluating the efficacy of homeopathic medicines in the prevention of COVID-19 in a quarantined population. Homeopathy 2022, 111, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Jonas, W.B. Do homeopathic nosodes protect against infection? An experimental test. Altern. Ther. Health Med. 1999, 5, 36–40. [Google Scholar] [PubMed]
- Dhama, K.; Nainu, F.; Frediansyah, A.; Yatoo, M.I.; Mohapatra, R.K.; Chakraborty, S.; Zhou, H.; Islam, M.R.; Mamada, S.S.; Kusuma, H.I.; et al. Global emerging Omicron variant of SARS-CoV-2: Impacts, challenges and strategies. J. Infect. Public Health 2022, 16, 4–14. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Subject No. | Gender (M.F) | Age (Yrs) | Weight (Kg) | WBC (4.00–10.00) 103/µL) | RBC (3.50–5.50) 106/uL | HGB (11.0–16.0) g/dL | PLT (100–300) 103/uL | Alkaline Phosphatase (53–128) U/L | Bilirubin Direct (0.00–0.20) mg/dL | Bilirubin Total (0.00–2.00) mg/dL | Total Protein (6.40–8.30) g/dL | Albumin (3.5–5.20) g/dL | AST/GOT (0.0–35.0) U/L | ALT/GPT (0.0–45.0) U/L | C-Reactive Protein (0.0–6.0) mg/dL | Ferritin (21.81–274.66) ng/mL |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 22 | 53 | 6.57 | 5.18 | 14 | 275 | 92 | 0.13 | 0.22 | 7.82 | 4.41 | 19.6 | 27.7 | 0.4 | 13.87 |
| 2 | F | 48 | 70.5 | 8.31 | 4.52 | 13.2 | 274 | 81 | 0.18 | 0.5 | 7.79 | 4.18 | 16.9 | 15.3 | 1.2 | 15.54 |
| 3 | F | 40 | 57.3 | 10.16 | 4.8 | 12 | 360 | 107 | 0.09 | 0.22 | 7.57 | 4.22 | 18.5 | 13.6 | 1.1 | 20.25 |
| 4 | F | 32 | 60 | 7.1 | 4.38 | 11.8 | 252 | 61 | 0.27 | 0.72 | 6.96 | 4.31 | 15.6 | 11.6 | 0.8 | 16.69 |
| 5 | F | 35 | 69 | 8.17 | 4.31 | 12.4 | 290 | 79 | 0.14 | 0.32 | 7.21 | 4.2 | 14.3 | 17.6 | 1.4 | 20.45 |
| 6 | F | 36 | 61 | 8.69 | 4.44 | 12 | 299 | 77 | 0.12 | 0.24 | 7.39 | 3.99 | 14.7 | 9.2 | 4.9 | 17.09 |
| 7 | M | 46 | 78 | 5.83 | 4.97 | 13.3 | 237 | 64 | 0.23 | 0.34 | 7.24 | 4.11 | 17.8 | 11.6 | 0.7 | 105.52 |
| 8 | M | 49 | 101.3 | 6.26 | 4.39 | 13.3 | 310 | 61 | 0.12 | 0.18 | 7.11 | 4.06 | 16.7 | 28.4 | 1.2 | 119.41 |
| 9 | M | 40 | 59.7 | 5.83 | 4.84 | 14.9 | 294 | 113 | 0.3 | 0.73 | 7.21 | 4.4 | 23.9 | 20.8 | 1.7 | 51.1 |
| 10 | F | 28 | 68 | 5.42 | 4.69 | 12.8 | 331 | 79 | 0.14 | 0.3 | 7.61 | 4.15 | 35.4 | 54.1 | 0.6 | 11.84 |
| Mean | 36.59 | 66.67 | 7.09 | 4.64 | 12.94 | 290.21 | 79.68 | 0.16 | 0.34 | 7.39 | 4.20 | 18.64 | 18.21 | 1.10 | 26.84 | |
| SD | 8.80 | 13.89 | 1.54 | 0.29 | 0.98 | 36.15 | 18.05 | 0.07 | 0.20 | 0.29 | 0.14 | 6.29 | 13.38 | 1.29 | 40.32 |
| Sr No. | Blood Parameters | Baseline | Day 17 | p Value |
|---|---|---|---|---|
| 1 | WBC (4.00–10.00) 103/µL) | 7.234 | 7.529 | 0.2801 |
| 2 | RBC (3.50–5.50) 106/uL | 4.652 | 4.208 | 0.2834 |
| 3 | HGB (11.0–16.0) g/dL | 12.97 | 12.97 | 1 |
| 4 | PLT (100–300)103/uL | 292.2 | 276.4 | 0.0724 |
| 5 | Alkaline Phosphatase (53–128) U/L | 81.4 | 80.4 | 0.5897 |
| 6 | Bilirubin Direct (0.00–0.20) mg/dL | 0.172 | 0.231 | 0.0994 |
| 7 | Bilirubin Total (0.00–2.00) mg/dL | 0.377 | 0.573 | 0.0658 |
| 8 | Total Protein (6.40–8.30) g/dL | 7.391 | 7.28 | 0.1193 |
| 9 | Albumin (3.5–5.20) g/dL | 4.203 | 4.255 | 0.1920 |
| 10 | AST/GOT (0.0–35.0) U/L | 19.34 | 17.09 | 0.1679 |
| 11 | ALT/GPT (0.0–45.0) U/L | 20.99 | 16.74 | 0.2398 |
| 12 | C-Reactive Protein (0.0–6.0) mg/dL | 1.4 | 1.61 | 0.4992 |
| 13 | Ferritin (21.81–274.66) ng/mL | 39.176 | 38.803 | 0.9009 |
| Test (Unit) | Visit | Statistics | n = 10 | p-Value |
|---|---|---|---|---|
| IL- 6 (0.00–7.00 pg/mL) | Visit 1 (Baseline) | Mean (SD) | 2.022 (0.794) | 0.00094 |
| Min, Max | 1.5, 3.7 | |||
| Visit 2 (Day 17) | Mean (SD) | 6.077 (2.845) | ||
| Min, Max | 2.65, 12 | |||
| Visit 3 (Day 34) | Mean (SD) | 29.032 (12.774) | 0.00008 | |
| Min, Max | 9.12, 44.6 | |||
| Visit 4 (Day 60) | Mean (SD) | 5.829 (6.771) | 0.11934 | |
| Min, Max | 1.5, 24.26 |
| Test (Unit) | Visit | Statistics | n = 10 | p-Value |
|---|---|---|---|---|
| Absolute Lymphocyte count (990.00–3150.00)/uL | Visit 3 (Day 34) | Mean (SD) | 2198.7 (526.201) | 0.25587 |
| Min, Max | 1563, 2854 | |||
| Visit 4 (Day 60) | Mean (SD) | 2287.9 (502.911) | ||
| Min, Max | 1699, 3004 | |||
| Absolute CD4 (424.00–1509.00)/uL | Visit 3 (Day 34) | Mean (SD) | 833.5 (280.553) | 0.026799 |
| Min, Max | 505, 1453 | |||
| Visit 4 (Day 60) | Mean (SD) | 900.8 (328.806) | ||
| Min, Max | 526, 1520 | |||
| Absolute CD8 (169.00–955.00)/uL | Visit 3 (Day 34) | Mean (SD) | 652.3 (272.316) | 0.2373 |
| Min, Max | 300, 1046 | |||
| Visit 4 (Day 60) | Mean (SD) | 687.7 (293.047) | ||
| Min, Max | 351, 1153 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herscu, P.; Talele, G.; Vaidya, S.; Shah, R. Safety and Evaluation of the Immune Response of Coronavirus Nosode (BiosimCovex) in Healthy Volunteers: A Preliminary Study Extending the Homeopathic Pathogenetic Trial. Medicines 2023, 10, 8. https://doi.org/10.3390/medicines10010008
Herscu P, Talele G, Vaidya S, Shah R. Safety and Evaluation of the Immune Response of Coronavirus Nosode (BiosimCovex) in Healthy Volunteers: A Preliminary Study Extending the Homeopathic Pathogenetic Trial. Medicines. 2023; 10(1):8. https://doi.org/10.3390/medicines10010008
Chicago/Turabian StyleHerscu, Paul, Gitanjali Talele, Shashikant Vaidya, and Rajesh Shah. 2023. "Safety and Evaluation of the Immune Response of Coronavirus Nosode (BiosimCovex) in Healthy Volunteers: A Preliminary Study Extending the Homeopathic Pathogenetic Trial" Medicines 10, no. 1: 8. https://doi.org/10.3390/medicines10010008
APA StyleHerscu, P., Talele, G., Vaidya, S., & Shah, R. (2023). Safety and Evaluation of the Immune Response of Coronavirus Nosode (BiosimCovex) in Healthy Volunteers: A Preliminary Study Extending the Homeopathic Pathogenetic Trial. Medicines, 10(1), 8. https://doi.org/10.3390/medicines10010008