
Prevalence of Dental Malocclusions in Different Geographical Areas: Scoping Review



Abstract
:1. Introduction
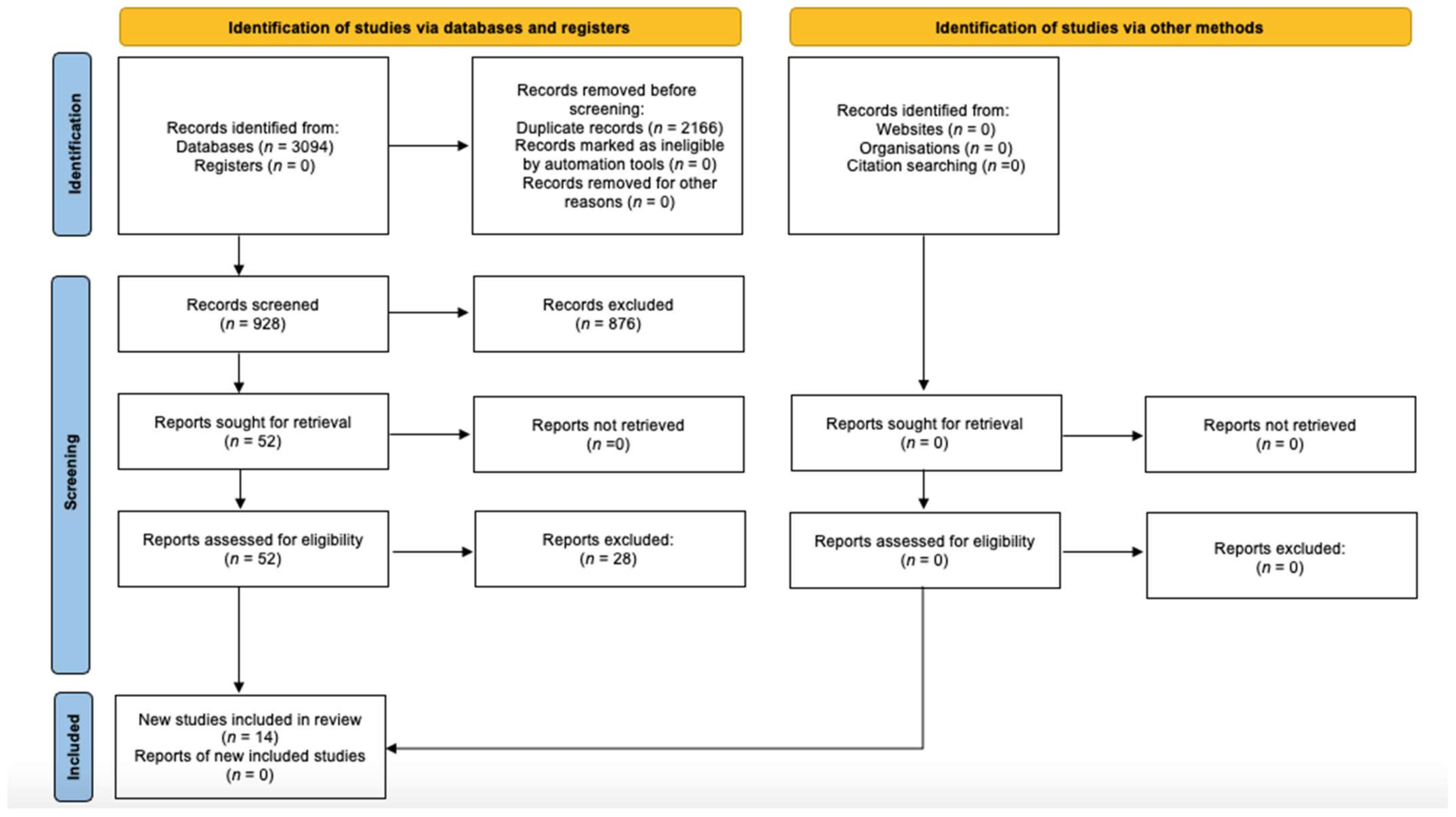
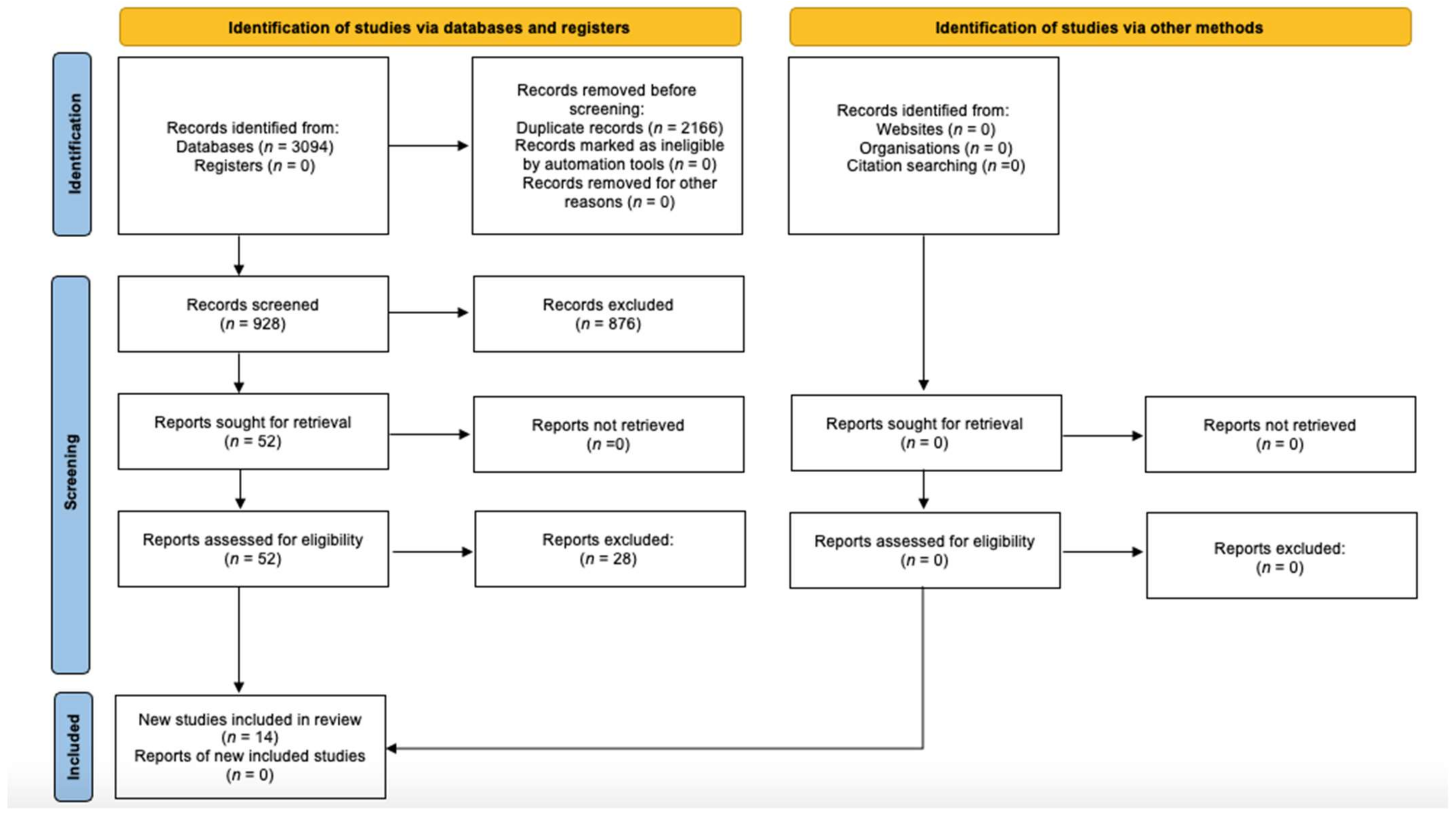
2. Materials and Methods
- -
- Studies whose patients presented an age range of 7 to 20 years.
- -
- Studies whose patients presented mixed or permanent dentition.
- -
- Recent studies performed from 2005 to the present.
- -
- Studies that analysed at least two spatial dimensions.
- -
- Exclusion of studies performed in the same geographical areas with overlapping results.
- -
- Exclusion of systematic reviews and meta-analyses.
- -
- Exclusion of studies whose titles correlated the prevalence of malocclusion with other problems such as temporomandibular disorders, sleep apnoea and bruxism.
2.1. Study Characteristics
2.2. Study Results
3. Results
3.1. Angle Classes
3.1.1. Class I
3.1.2. Class II
3.1.3. Class III
3.2. Vertical Dimension
3.2.1. Openbite
3.2.2. Deepbite
3.2.3. Overjet
3.2.4. Crowding
3.2.5. Spacing
3.2.6. Crossbite
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dos Santos, R.R.; Nayme, J.G.; Garbin, A.J.; Saliba, N.; Garbin, C.A.; Moimaz, S.A. Prevalence of malocclusion and related oral habits in 5-to 6-year-old children. Oral Health Prev. Dent. 2012, 10, 311–318. [Google Scholar] [PubMed]
- Mtaya, M.; Brudvik, P.; Astrøm, A.N. Prevalence of malocclusion and its relationship with socio- demographic factors, dental caries, and oral hygiene in 12- to 14-year-old Tanzanian schoolchildren. Eur. J. Orthod. 2009, 31, 467–476. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.; Fida, M. Assessment of psychosocial impact of dental aesthetics. J. Coll. Physicians Surg. Pak. 2008, 18, 559–564. [Google Scholar] [PubMed]
- Lew, K.K.; Foong, W.C.; Loh, E. Malocclusion prevalence in an ethnic Chinese population. Aust. Dent. J. 1993, 38, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Gelgör, I.E.; Karaman, A.I.; Ercan, E. Prevalence of malocclusion among adolescents in central anatolia. Eur. J. Dent. 2007, 1, 125–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garbin, A.J.ĺ.; Perin, P.C.P.; Garbin, C.A.S.; Lolli, L.F. Malocclusion prevalence and comparison between the Angle classification and the Dental Aesthetic Index in scholars in the interior of São Paulo state Brazil. Dent. Press J. Orthod. 2010, 15, 94–102. [Google Scholar] [CrossRef] [Green Version]
- Maspero, C.; Galbiati, G.; Giannini, L.; Guenza, G.; Farronato, M. Class II division 1 malocclusions: Comparisons between one- and two-step treatment. Eur. J. Paediatr. Dent. 2018, 19, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Farronato, G.; Maspero, C.; Chimenti, C.; Festa, F.; Giannì, A.B.; Alvaro, C.M.; Perillo, L. Ortognatodonzia, 1st ed.; Edi-Ermes: Milan, Italy, 2013; Volume 1, pp. 190–200. [Google Scholar]
- Fernandez, C.C.A.; Pereira, C.V.C.A.; Luiz, R.R.; Vieira, A.R.; De Castro Costa, M. Dental anomalies in different growth and skeletal malocclusion patterns. Angle Orthod. 2017, 88, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Masucci, C.; Oueiss, A.; Maniere-Ezvan, A.; Orthlieb, J.D.; Casazza, E. What is a malocclusion? L’Orthodontie Française 2020, 91, 57–67. [Google Scholar] [CrossRef]
- Battaglia, D. Malocclusioni: La Diagnosi in Ortodonzia Comincia Con L’analisi Dentale; Il Dentista Moderno: Milan, Italy, 2016. [Google Scholar]
- Lanteri, V.; Maspero, C.; Cavone, P.; Marchio, V.; Farronato, M. Relationship between molar deciduous teeth infraocclusion and mandibular growth: A case-control study. Eur. J. Paediatr. Dent. 2020, 21, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Maspero, C.; Begnoni, G.; Magnani, A.; Farronato, M.; Khomchyna, N.; Dellavia, C. Rapid Maxillary Expander and Eruption Guidance Appliance therapy in skeletal Class II: Cephalometric considerations. Eur. J. Paediatr. Dent. 2019, 20, 280–284. [Google Scholar] [CrossRef]
- Zou, J.; Meng, M.; Law, C.S.; Rao, Y.; Zhou, X. Common dental diseases in children and malocclusion. Int. J. Oral Sci. 2018, 10, 1–7. [Google Scholar] [CrossRef]
- Marcomini, L.; Lucato, A.S.; dos Santos, J.L.B.; Tubel, C.A.M. Prevalence of malocclusion and its relationship with functional changes in the breathing and in the swallowing. Braz. Dent. Sci. 2010, 13, 52–58. [Google Scholar] [CrossRef]
- Abate, A.; Cavagnetto, D.; Fama, A.; Maspero, C.; Farronato, G. Relationship between Breastfeeding and Malocclusion: A Systematic Review of the Literature. Nutrients 2020, 12, 3688. [Google Scholar] [CrossRef] [PubMed]
- Germeç, D.; Taner, T.U. Lower lip sucking habit treated with a lip bumper appliance. Angle Orthod. 2005, 75, 1071–1076. [Google Scholar] [PubMed]
- Muñoz, I.C.L.; Orta, P.B. Comparison of cephalometric patterns in mouth breathing and nose breathing children. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 1167–1172. [Google Scholar] [CrossRef]
- Johal, A.; Cheung, M.Y.H.; Marcenes, W. The impact of two different malocclusion traits on quality of life. Br. Dent. J. 2007, 202, E6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siluvai, S.; Kshetrimayum, N.; Reddy, C.V.; Siddanna, S.; Manjunath, M.; Rudraswamy, S. Malocclusion and related quality of life among 13- to 19-year-old students in Mysore City—A cross-sectional study. Oral Health Prev. Dent. 2015, 13, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Bourzgui, F.; Sebbar, M.; Hamza, M.; Lazrak, L.; Abidine, Z.; El Quars, F. Prevalence of malocclusions and orthodontic treatment need in 8-to 12-year-old schoolchildren in Casablanca, Morocco. Prog. Orthod. 2012, 13, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Aikins, E.A.; Onyeaso, C.O. Prevalence of malocclusion and occlusal traits among adolescents and young adults in Rivers State, Nigeria. Odontostomatol. Trop. 2014, 37, 5–12. [Google Scholar]
- Ferro, R.; Besostri, A.; Olivieri, A.; Stellini, E. Prevalence of occlusal traits and orthodontic treatment need in 14 year-old adolescents in Northeast Italy. Eur. J. Paediatr. Dent. 2016, 17, 36–42. [Google Scholar]
- Sundareswaran, S.; Kizhakool, P. Prevalence and gender distribution of malocclusion among 13–15-year-old adolescents of Kerala, South India. Indian J. Dent. Res. 2019, 30, 455–461. [Google Scholar] [CrossRef]
- Alhaija, E.S.J.A.; Al-Khateeb, S.N.; Al-Nimri, K.S. Prevalence of malocclusion in 13–15 year-old North Jordanian school children. Community Dent. Health 2005, 22, 266–271. [Google Scholar]
- Alvarado, K.; López, L.; Hanke, R.; Picón, F.; Rivas-Tumanyan, S. Prevalence of malocclusion and distribution of occlusal characteristics in 13-to 18-year-old adolescents attending selected high schools in the municipality of San Juan, PR (2012–2013). Puerto Rico Health Sci. J. 2017, 36, 61–66. [Google Scholar]
- Perrotta, S.; Bucci, R.; Simeon, V.; Martina, S.; Michelotti, A.; Valletta, R. Prevalence of malocclusion, oral parafunctions and temporomandibular disorder-pain in Italian schoolchildren: An epidemiological study. J. Oral Rehabil. 2019, 46, 611–616. [Google Scholar] [CrossRef]
- Traebert, E.; Martins, L.G.T.; Pereira, K.C.R.; Costa, S.X.S.; Lunardelli, S.E.; Lunardelli, A.N.; Traebert, J. Malocclusion in Brazilian schoolchildren: High prevalence and low impact. Oral Health Prev. Dent. 2018, 16, 163–167. [Google Scholar] [CrossRef]
- Sidlauskas, A.; Lopatiene, K. The prevalence of malocclusion among 7–15-year-old Lithuanian schoolchildren. Medicina 2009, 45, 147. [Google Scholar] [CrossRef] [Green Version]
- Almalky, N.M.; Elattar, H.M. Prevalence of different types of malocclusion among school children in Makkah Governorate of Saudi Arabia. Int. J. Dent. Oral Sci. 2018, 5, 645–648. [Google Scholar]
- Gudipaneni, R.K.; Aldahmeshi, R.F.; Patil, S.R.; Alam, M.K. The prevalence of malocclusion and the need for orthodontic treatment among adolescents in the northern border region of Saudi Arabia: An epidemiological study. BMC Oral Health 2018, 18, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Kaur, H.; Pavithra, U.S.; Abraham, R. Prevalence of malocclusion among adolescents in South Indian population. J. Int. Soc. Prev. Community Dent. 2013, 3, 97. [Google Scholar] [CrossRef] [Green Version]
- Lombardo, G.; Vena, F.; Negri, P.; Pagano, S.; Barilotti, C.; Paglia, L.; Colombo, S.; Orso, M.; Cianetti, S. Worldwide prevalence of malocclusion in the different stages of dentition- A systematic review and meta-analysis. Eur. J. Paediatr. Dent. 2020, 21, 115–123. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Authors | Title | Periodical and Year | Population |
|---|---|---|---|
| Prevalence of malocclusions and orthodontic treatment need in 8- to 12-year-old schoolchildren in Casablanca, Morocco | Progress in Orthodontics 2012 | 1000 subjects between 8 and 12 years old |
| Prevalence of malocclusion and occlusal traits among adolescents and young adults in Rivers State, Nigeria | Odontostomatol Trop 2014 | 620 subjects between 13 and 20 years old |
| Prevalence of occlusal traits and orthodontic treatment needed in 14 year-old adolescents in Northeast Italy | European Journal Pediatric Dentistry 2016 | 444 subjects of 14 years old |
| Prevalence and gender distribution of malocclusion among 13–15-year-old adolescents of Kerala, South India | Indian Journal of Dental Research 2019 | 1554 subjects between 13 and 15 years old |
| Prevalence of malocclusion in 13–15 year-old North Jordanian school children | Community Dental Health 2005 | 1003 subjects between 13 and 15 years old |
| Prevalence of Malocclusion and Distribution of Occlusal Characteristics in 13- to 18-year-old Adolescents Attending Selected High Schools in the Municipality of San Juan, PR | Puerto Rico Health Science Journal 2017 | 155 subjects between 13 and 18 years old |
| Prevalence of malocclusion, oral parafunctions and temporomandibular disorder pain in Italian school children: an epidemiological study. | Journal of Oral Rehabilitation 2019 | 700 subjects between 9 and 11 years old |
| Malocclusion in Brazilian Schoolchildren: High Prevalence and Low Impact | Oral Health and Preventive Dentistry 2015 | 389 subjects between 10 and 15 years old |
| The prevalence of malocclusion among 7–15-year-old Lithuanian schoolchildren | Medicina (Kaunas) 2009 | 1681 subjects between 7 and 15 years old |
| Prevalence Of Different Types of Malocclusion Among School Children In Makkah Governorate of Saudi Arabia | International Journal of Dentistry and Oral Science 2018 | 289 subjects between 14 and 17 years old |
| The prevalence of malocclusion and the need for orthodontic treatment among adolescents in the northern border region of Saudi Arabia: an epidemiological study | BMC Oral Health 2018 | 500 subjects between 14 and 18 years old |
| Prevalence of malocclusion and its relationship with socio-demographic factors, dental caries, and oral hygiene in 12- to 14-year-old Tanzanian schoolchildren | The European Journal of Orthodontics 2009 | 1601 subjects between 12 and 14 years old |
| Prevalence of malocclusion among adolescents in South Indian population | Journal of International Societ of Preventive and Community Dentistry 2013 | 2400 subjects between 13 and 17 years old |
| Prevalence of malocclusion among adolescents in Central Anatolia | European Journal of Dentistry 2017 | 2329 subjects between 12 and 17 years old |
| I Class | II Class | III Class | Overjet | Openbite | |
|---|---|---|---|---|---|
| 1 | 61.4% | 24% | 10% | 63.8% 1–4 mm 17.2% 4–6 mm 10% > 6 mm | * |
| 2 | 80.3% | 6.3% (3.9% I° division, 2.4% II° division) | 1.6% | 30% (increased 15.6%; reduced 15.2%) | 7.1% |
| 3 | 86.3% | 19.50% | 3.9% | increased 48% | 1.4% |
| 4 | 64.3% | 17.6% | 8% | increased 11.8% | 1.6% |
| 5 | 55.3% | 18.8% | 1.4% | increased 24.7%, reduced nell’1.8% | 2.9% |
| 6 | 73% | 7.10% | 19.4% | increased 63% | 1.9% |
| 7 | 46.8% | 32.6% (19% divisions) | 1.6% | increased 14.1%, reduced 2.2% | 18% |
| 8 | 42.7% | 15.9% | 14.1% | 30.90% | 2.6% |
| 9 | 68.4% | 27.7% | 2.8% | increased 21.09%, reduced 0.4% | 3.46% |
| 10 | 67.13% | I division 14.53%, II division 10.7% | 7.61% | increased 25.6%, reduced 17% | 21.1% |
| 11 | 52.8% | 31.8% | 15.4% | increased 22.2% reduced 11.4% | 4.6% |
| 12 | 93.6% | 4.4% | 2% | * | 16.1% |
| 13 | 89.45% | 8.37% | 2.14% | Increased 33.71% reduced 18.07% | 35.97% |
| 14 | 34.9% | I division 40% II division 4.7% | 10.3% | increased 25.1% reduced 10.4% | 8.2% |
| Deepbite | Crowding | Spacing | Crossbite | |
|---|---|---|---|---|
| 1 | * | anterior 50%, posterior 2.5% | * | * |
| 2 | * | 14.4% | 60% | 17.1% |
| 3 | * | 30% | * | anterior 4%, posterior 5% |
| 4 | * | 66.6% | 15.3% | anterior 27.5% posterior 5.1% |
| 5 | 16.9% | 50.4% | 26.7% | 6.80% |
| 6 | * | * | * | * |
| 7 | 2% | * | * | 12% |
| 8 | * | * | * | * |
| 9 | 14.46% | upper 44.1%, lower 40.3% | * | 8.8% |
| 10 | 26.3% | 63.3% | * | anterior 17%, posterior 21.4% |
| 11 | * | * | * | anterior 4.8% posterior 9.4% |
| 12 | * | * | 21.9% | * |
| 13 | 14.15% | 58.12% | * | anterior 8.48% posterior 0.99% |
| 14 | 14.4% | * | * | 9.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cenzato, N.; Nobili, A.; Maspero, C. Prevalence of Dental Malocclusions in Different Geographical Areas: Scoping Review. Dent. J. 2021, 9, 117. https://doi.org/10.3390/dj9100117
Cenzato N, Nobili A, Maspero C. Prevalence of Dental Malocclusions in Different Geographical Areas: Scoping Review. Dentistry Journal. 2021; 9(10):117. https://doi.org/10.3390/dj9100117
Chicago/Turabian StyleCenzato, Niccoló, Anna Nobili, and Cinzia Maspero. 2021. "Prevalence of Dental Malocclusions in Different Geographical Areas: Scoping Review" Dentistry Journal 9, no. 10: 117. https://doi.org/10.3390/dj9100117
APA StyleCenzato, N., Nobili, A., & Maspero, C. (2021). Prevalence of Dental Malocclusions in Different Geographical Areas: Scoping Review. Dentistry Journal, 9(10), 117. https://doi.org/10.3390/dj9100117