
Acute Local Spontaneous and Profuse Gingival Hemorrhage during Neoadjuvant Treatment with Paclitaxel and Trastuzumab

 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
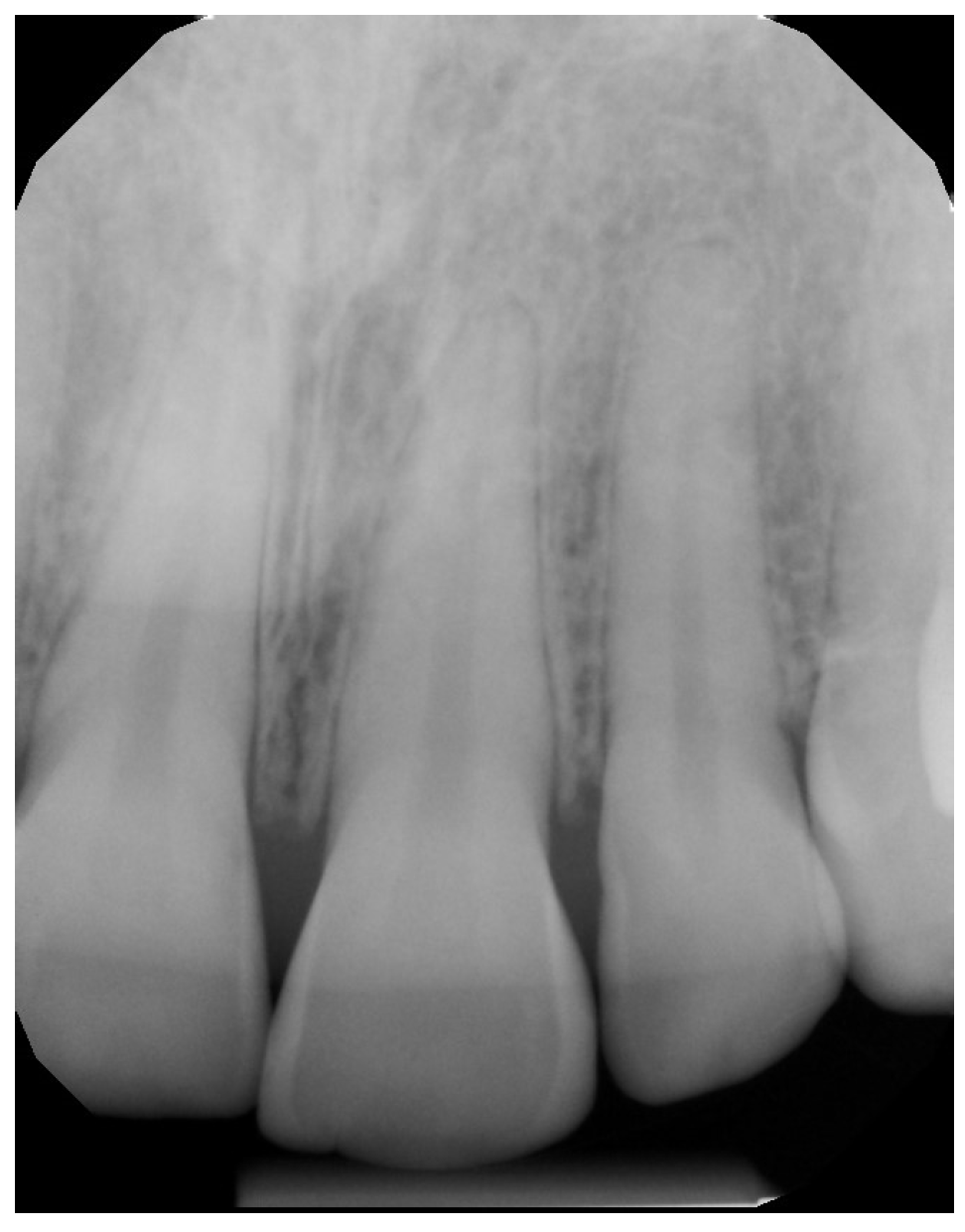
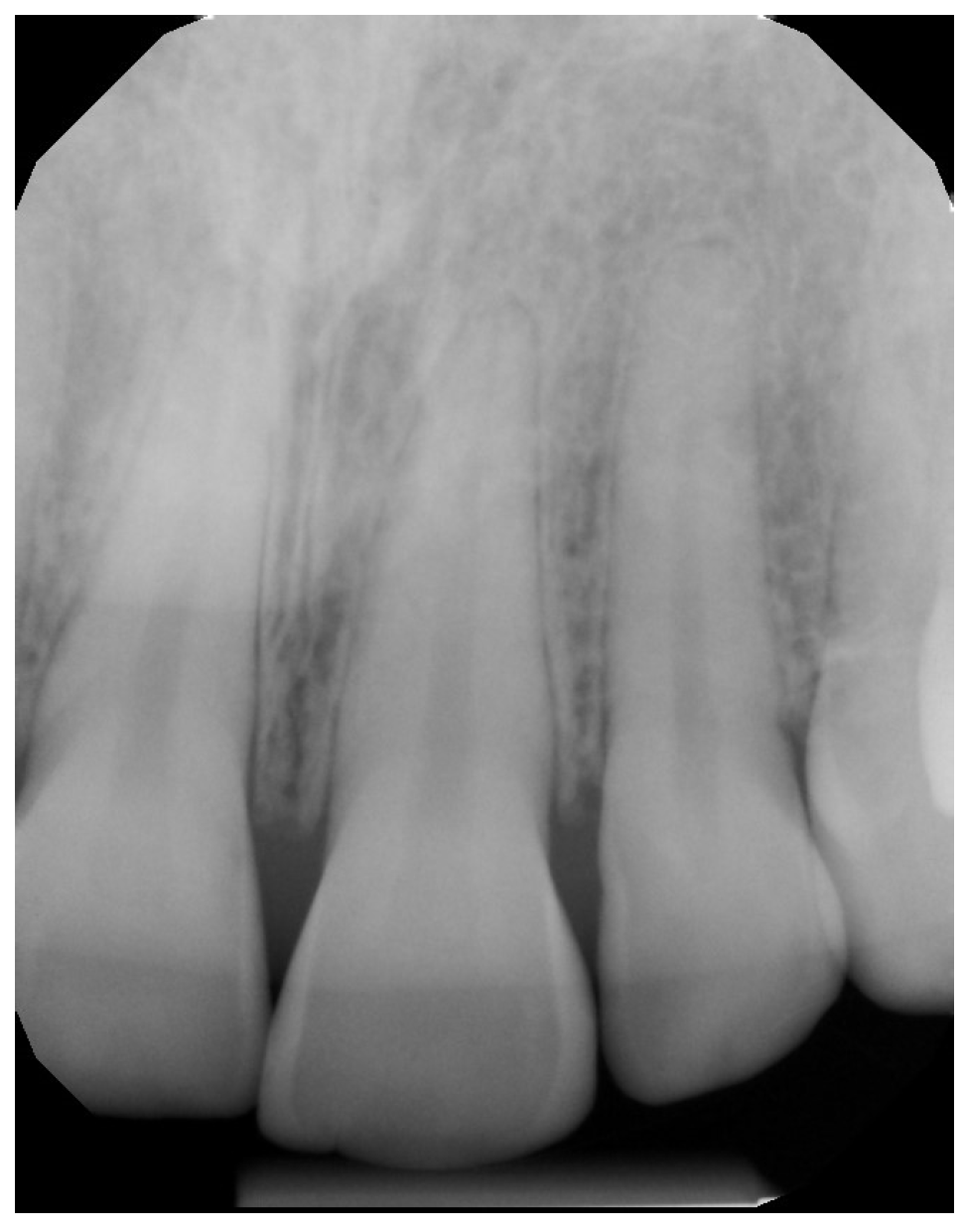
2. Case Presentation
3. Discussion
Author Contributions
Conflicts of Interest
Appendix A


References
- Armitage, G.C. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Armitage, G.C. Periodontal diagnoses and classification of periodontal diseases. Periodontol. 2000 2003, 34, 9–21. [Google Scholar] [CrossRef]
- Linden, G.J.; Lyons, A.; Scannapieco, F. Periodontal systemic associations. Rev. Evid. J. Clin. Periodontol. 2013, 40 (Suppl. 14), 8–19. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.; Bouchard, P. Periodontal diseases and health: Consensus report of the sixth European workshop on periodontology. J. Clin. Periodontol. 2008, 35, 333–337. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Periodontology. Parameter on periodontitis associated with systemic conditions. J. Periodontol. 2000, 71 (Suppl. S5), 876–879. [Google Scholar]
- Pizzo, G.; Guiglia, R.; Lo Russo, L.; Campisi, G. Dentistry and internal medicine: From the focal infection theory to the periodontal medicine concept. Eur. J. Intern. Med. 2010, 21, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Wayne, D.B.; Trajtenberg, C.P.; Hyman, D.J. Tooth and periodontal disease: A review for the primary-care physician. South. Med. J. 2001, 94, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Hudis, C.A. Trastuzumab—Mechanism of action and use in clinical practice. N. Engl. J. Med. 2007, 357, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Gralow, J.R.; Burstein, H.J.; Wood, W.; Hortobagyi, G.N.; Gianni, L.; von Minckwitz, G.; Buzdar, A.U.; Smith, I.E.; Symmans, W.F.; Singh, B.; et al. Preoperative therapy in invasive breast cancer: Pathologic assessment and systemic therapy issues in operable disease. J. Clin. Oncol. 2008, 26, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Advani, P.P.; Ballman, K.V.; Dockter, T.J.; Colon-Otero, G.; Perez, E.A. Long-term cardiac safety analysis of NCCTG N9831 (Alliance) adjuvant trastuzumab trial. J. Clin. Oncol. 2016, 34, 581–587. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarmast, N.D.; Gutierrez Quevedo, M.J.; Wang, H.H.; Gutierrez Herrera, E.R. Acute Local Spontaneous and Profuse Gingival Hemorrhage during Neoadjuvant Treatment with Paclitaxel and Trastuzumab. Dent. J. 2016, 4, 22. https://doi.org/10.3390/dj4030022
Sarmast ND, Gutierrez Quevedo MJ, Wang HH, Gutierrez Herrera ER. Acute Local Spontaneous and Profuse Gingival Hemorrhage during Neoadjuvant Treatment with Paclitaxel and Trastuzumab. Dentistry Journal. 2016; 4(3):22. https://doi.org/10.3390/dj4030022
Chicago/Turabian StyleSarmast, Nima D., Maria J. Gutierrez Quevedo, Howard H. Wang, and Estatio R. Gutierrez Herrera. 2016. "Acute Local Spontaneous and Profuse Gingival Hemorrhage during Neoadjuvant Treatment with Paclitaxel and Trastuzumab" Dentistry Journal 4, no. 3: 22. https://doi.org/10.3390/dj4030022
APA StyleSarmast, N. D., Gutierrez Quevedo, M. J., Wang, H. H., & Gutierrez Herrera, E. R. (2016). Acute Local Spontaneous and Profuse Gingival Hemorrhage during Neoadjuvant Treatment with Paclitaxel and Trastuzumab. Dentistry Journal, 4(3), 22. https://doi.org/10.3390/dj4030022