
Dental Practice Websites in Germany—How Do They Inform about Fluoridation?


Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
2.2. Functional Aspect and Generic Risk of Bias
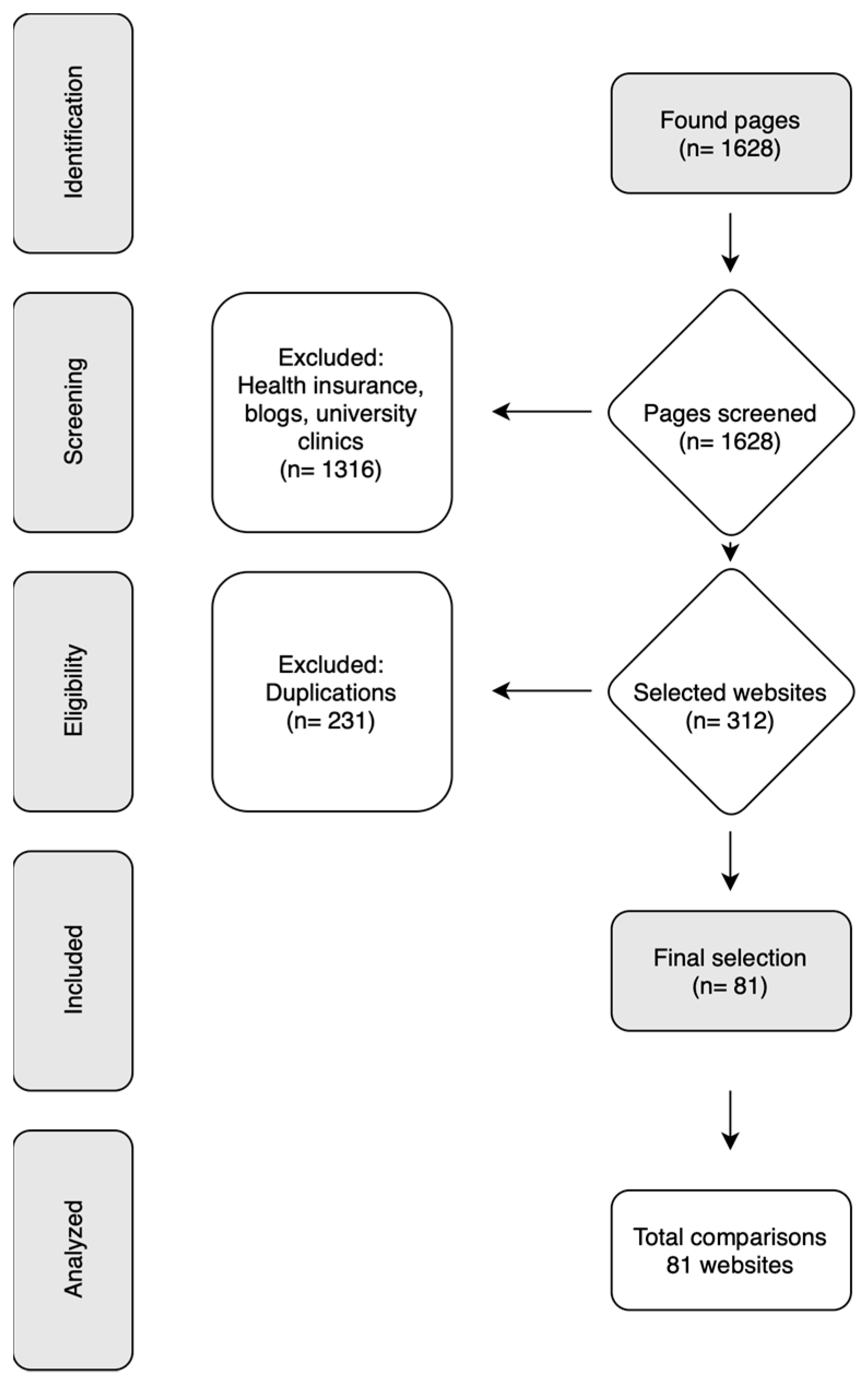
2.3. Search Strategy
2.4. Data Extraction and Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- O’Mullane, D.M.; Baez, R.J.; Jones, S.; Lennon, M.A.; Petersen, P.E.; Rugg-Gunn, A.J.; Whelton, H.; Whitford, G.M. Fluoride and Oral Health. Community Dent. Health 2016, 33, 69–99. [Google Scholar]
- Toumba, K.J.; Twetman, S.; Splieth, C.; Parnell, C.; van Loveren, C.; Lygidakis, N. Guidelines on the use of fluoride for caries prevention in children: An updated EAPD policy document. Eur. Arch. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2019, 20, 507–516. [Google Scholar] [CrossRef]
- Sanz, M.; Beighton, D.; Curtis, M.A.; Cury, J.A.; Dige, I.; Dommisch, H.; Ellwood, R.; Giacaman, R.A.; Herrera, D.; Herzberg, M.C.; et al. Role of microbial biofilms in the maintenance of oral health and in the development of dental caries and periodontal diseases. Consensus report of group 1 of the Joint EFP/ORCA workshop on the boundaries between caries and periodontal disease. J. Clin. Periodontol. 2017, 44 (Suppl. S18), S5–S11. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.; Worthington, H.V.; Glenny, A.M.; Marinho, V.C.; Jeroncic, A. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst. Rev. 2019, 3, CD007868. [Google Scholar] [CrossRef] [PubMed]
- Whelton, H.P.; Spencer, A.J.; Do, L.G.; Rugg-Gunn, A.J. Fluoride Revolution and Dental Caries: Evolution of Policies for Global Use. J. Dent. Res. 2019, 98, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Gouverneur, A.; Bourenane, H.; Chung, A.; Daguerre, C.; Devarieux, M.; Malifarge, L. How people use the internet to find information on medicines? Therapie 2014, 69, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.; Ziade, N.; Jatuworapruk, K.; Caballero-Uribe, C.V.; Khursheed, T.; Gupta, L. The Impact of Social Media on Vaccination: A Narrative Review. J. Korean Med. Sci. 2023, 38, e326. [Google Scholar] [CrossRef] [PubMed]
- Aimeur, E.; Amri, S.; Brassard, G. Fake news, disinformation and misinformation in social media: A review. Soc. Netw. Anal. Min. 2023, 13, 30. [Google Scholar] [CrossRef] [PubMed]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5, e004206. [Google Scholar] [CrossRef]
- Dietrich Leurer, M.; Vandenberg, H.; Cameron, D. Risk Communication in Public Health: Lessons from a Historic Fluoridation Debate in Saskatchewan. Health Commun. 2023, 38, 3124–3134. [Google Scholar] [CrossRef]
- Armfield, J.M. When public action undermines public health: A critical examination of antifluoridationist literature. Aust. N. Z. Health Policy 2007, 4, 25. [Google Scholar] [CrossRef]
- Ko, A.; Chi, D.L. Fluoride hesitancy: A mixed methods study on decision-making about forms of fluoride. Community Dent. Oral Epidemiol. 2023, 51, 997–1008. [Google Scholar] [CrossRef]
- Lotto, M.; Zakir Hussain, I.; Kaur, J.; Butt, Z.A.; Cruvinel, T.; Morita, P.P. Analysis of Fluoride-Free Content on Twitter: Topic Modeling Study. J. Med. Internet Res. 2023, 25, e44586. [Google Scholar] [CrossRef] [PubMed]
- Terrasse, M.; Gorin, M.; Sisti, D. Social Media, E-Health, and Medical Ethics. Hastings Cent. Rep. 2019, 49, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Lotto, M.; Sa Menezes, T.; Zakir Hussain, I.; Tsao, S.F.; Ahmad Butt, Z.; Morita, P.P.; Cruvinel, T. Characterization of False or Misleading Fluoride Content on Instagram: Infodemiology Study. J. Med. Internet Res. 2022, 24, e37519. [Google Scholar] [CrossRef] [PubMed]
- Kanzow, P.; Buttcher, A.F.; Wiegand, A.; Schwendicke, F. Quality of Information Regarding Repair Restorations on Dentist Websites: Systematic Search and Analysis. J. Med. Internet Res. 2020, 22, e17250. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Stange, J.; Stange, C.; Graetz, C. German dentists’ websites on periodontitis have low quality of information. BMC Med. Inform. Decis. Mak. 2017, 17, 114. [Google Scholar] [CrossRef]
- Minervation. The LIDA Instrument: Minervation Validation Instrument for Health Care Web Sites, Version 1.2. Available online: http://www.minervation.com/wp-content/uploads/2011/04/Minervation-LIDA-instrument-v1-2.pdf (accessed on 2 December 2022).
- Charnock, D.; Shepperd, S. Learning to DISCERN online: Applying an appraisal tool to health websites in a workshop setting. Health Educ. Res. 2004, 19, 440–446. [Google Scholar] [CrossRef]
- Charnock, D.; Shepperd, S.; Needham, G.; Gann, R. DISCERN: An instrument for judging the quality of written consumer health information on treatment choices. J. Epidemiol. Community Health 1999, 53, 105–111. [Google Scholar] [CrossRef]
- Blizniuk, A.; Furukawa, S.; Ueno, M.; Kawaguchi, Y. Evaluation of English Websites on Dental Caries by Using Consumer Evaluation Tools. Oral Health Prev. Dent. 2016, 14, 363–369. [Google Scholar] [CrossRef]
- Akan, B.; Dindaroglu, F.C. Content and Quality Analysis of Websites as a Patient Resource for Temporomandibular Disorders. Turk. J. Orthod. 2020, 33, 203–209. [Google Scholar] [CrossRef]
- Patel, A.; Cobourne, M.T. The design and content of orthodontic practise websites in the UK is suboptimal and does not correlate with search ranking. Eur. J. Orthod. 2015, 37, 447–452. [Google Scholar] [CrossRef]
- Kumar, S.; Chhabra, V.; Mehra, M.; Saranya, K.; Kumar, B.H.; Shenoy, S.; Swamy, R.S.; Murti, K.; Pai, K.S.R.; Kumar, N. The fluorosis conundrum: Bridging the gap between science and public health. Toxicol. Mech. Methods 2023, 34, 214–235. [Google Scholar] [CrossRef]
- Wang, Y.; McKee, M.; Torbica, A.; Stuckler, D. Systematic Literature Review on the Spread of Health-related Misinformation on Social Media. Soc. Sci. Med. 2019, 240, 112552. [Google Scholar] [CrossRef] [PubMed]
- Eliacik, B.K. Topical Fluoride Applications Related Posts Analysis on Twitter Using Natural Language Processing. Oral Health Prev. Dent. 2021, 19, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Basch, C.H.; Milano, N.; Hillyer, G.C. An assessment of fluoride related posts on Instagram. Health Promot. Perspect. 2019, 9, 85–88. [Google Scholar] [CrossRef]
- Basch, C.H.; Blankenship, E.B.; Goff, M.E.; Yin, J.; Basch, C.E.; DeLeon, A.J.; Fung, I.C. Fluoride-related YouTube videos: A cross-sectional study of video contents by upload sources. J. Dent. Hyg. JDH Am. Dent. Hyg. Assoc. 2018, 92, 47–53. [Google Scholar]
- Burgette, J.M.; Dahl, Z.T.; Yi, J.S.; Weyant, R.J.; McNeil, D.W.; Foxman, B.; Marazita, M.L. Mothers’ Sources of Child Fluoride Information and Misinformation from Social Connections. JAMA Netw. Open 2022, 5, e226414. [Google Scholar] [CrossRef] [PubMed]
- Lisboa, S.O.; Assuncao, C.M.; Drumond, C.L.; Serra-Negra, J.M.C.; Machado, M.G.P.; Paiva, S.M.; Ferreira, F.M. Association between Level of Parental Oral Health Literacy and the Rational Use of Fluoride for Children from 0 to 4 Years of Age after Instruction: An Intervention Trial. Caries Res. 2022, 56, 535–545. [Google Scholar] [CrossRef]
- Aguirre, P.E.A.; Coelho, M.M.; Rios, D.; Machado, M.; Cruvinel, A.F.P.; Cruvinel, T. Evaluating the Dental Caries-Related Information on Brazilian Websites: Qualitative Study. J. Med. Internet Res. 2017, 19, e415. [Google Scholar] [CrossRef] [PubMed]
- Geiken, A.; Holtmann, L.; Splieth, C.H.; Conrad, J.; Doerfer, C.E.; Graetz, C. Are the Dental Guidelines for Early Dental Visits and Fluoridation Measures Supported by Pediatricians, and What Are Their Caries Prevention Efforts? J. Clin. Med. 2022, 11, 1159. [Google Scholar] [CrossRef] [PubMed]
- Geiken, A.; Holtmann, L.; Doerfer, C.E.; Schwarz, C.; Graetz, C. Attitude of Midwives towards Fluoride Recommendations and Oral Prevention in Infants and Young Children. Children 2022, 9, 1135. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable and Attribute | Value (n (%)) |
|---|---|
| Practice location | |
| Rural | 7 (9%) |
| City | 41 (50%) |
| Large city | 33 (41%) |
| Practice setting | |
| Single practice | 24 (30%) |
| Multi-practice | 55 (67%) |
| Chain practice | 2 (3%) |
| Age | |
| Young | 9 (11%) |
| Middle-aged | 32 (39%) |
| Older | 28 (35%) |
| No information | 12 (15%) |
| Specializations | |
| Pediatric dentistry | 3 (4%) |
| Any specializations | 17 (17%) |
| No information | 62 (79%) |
| Item | Median (IQR a; Min–Max b) |
|---|---|
| 1.1 Accessibility | |
| • Is the information available full text without registration, log-in or subscription? | 2 (0; 2–2) |
| 1.2 Usability | |
| • Is there a clear statement of who this website is for? | 2 (0; 1–2) |
| • Is the level of detail appropriate to their level of knowledge? Is the layout of the main block of information clear and readable? | 2 (0; 1–2) |
| • Is the navigation clear and well structured? | 2 (0; 0–2) |
| • Can you always tell your current location on the site? | 2 (0; 1–2) |
| • Do navigational links have a consistent function? | 2 (0; 0–2) |
| • Does the site provide an effective search function? | 2 (0; 0–2) |
| • Can you use the site without third party plugins? | 0 (0; 0–2) |
| • Can the user make an effective judgment of whether the site applies to them? | 1 (0; 0–2) |
| • Is the website interactive? | 2 (0; 1–2) |
| • Does the website integrate non textual media? | 1 (0; 0–2) |
| 1.3 Reliability | |
| • Can users submit comments on specific content? | 0 (0; 0–0) |
| • Is site content updated at an appropriate interval? | 2 (0; 1–2) |
| • Is it clear who runs the site? | 2 (0; 0–2) |
| • Is it clear who pays for the site? | 1 (0; 1–2) |
| • Can the information be checked from original sources? | 2 (0; 1–2) |
| Item | Median (IQR a; Min–Max b) |
|---|---|
| 2.1 Reliability | |
| • Are the aims clear? | 2 (0; 1–2) |
| • Is it clear what sources of information were used to compile the publication? | 0 (0; 0–2) |
| • Is it clear when the information used or reported in the publication was produced? | 2 (0; 0–2) |
| • Is it balanced and unbiased? | 1 (0; 0–2) |
| • Does it provide details of additional sources of support and information? | 1 (0; 0–2) |
| • Does it refer to areas of uncertainty? | 0 (0; 0–1) |
| 2.2 Quality | |
| • Does it describe how each treatment works? | 2 (0; 0–2) |
| • Does it describe the benefits of each treatment? | 2 (0; 0–2) |
| • Does it describe the risks of each treatment? | 0 (0; 0–2) |
| • Does it describe what would happen if no treatment is used? | 1 (0; 0–2) |
| • Does it describe how the treatment choices affect overall quality of life? | 1 (0; 0–2) |
| • Is it clear that there may be more than one possible treatment choice? | 2 (0; 0–2) |
| • Does it provide support for shared decision making? | 1 (0; 0–2) |
| Item | Median (IQR a; Min–Max b) |
|---|---|
| • Is the word fluoridation mentioned at all? | 2 (0; 0–2) |
| • Is there an extra item that gives information only on fluoridation? | 0 (0; 0–2) |
| • Is there a pro/con point of view? | 2 (0; 0–2) |
| • Is fluoride explained in complete sentences? | 0 (0; 0–2) |
| • Is fluoridation defined in complete sentences? | 0 (0; 0–2) |
| • Is syst. and loc. fluoridation explained in more detail? | 0 (0; 0–2) |
| • Is the mode of action explained in more detail? | 0 (0; 0–2) |
| • Are the risks of non-administration explained? | 0 (0; 0–2) |
| • Are the risks of excessive administration explained? | 0 (0; 0–2) |
| • Is it divided into basic and intensive prophylaxis? | 0 (0; 0–2) |
| • Is basis prophylaxis mentioned in more detail? | 0 (0; 0–0) |
| • Is intensive prophylaxis mentioned in more detail? | 0 (0; 0–0) |
| • Is information provided about the age at which fluoride should be taken? | 0 (0; 0–2) |
| • Are fluoride sources mentioned? | 0 (0;0–2) |
| • Are instructions for taking fluoride given? | 0 (0; 0–2) |
| • Is information provided on the correct amount to take? | 0 (0; 0–2) |
| • Are the advantages of early administration mentioned? | 0 (0; 0–2) |
| • Are the disadvantages of not taking fluoride mentioned? | 0 (0; 0–2) |
| Factor | Beta (Mean Quality Score) | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Constant | 15.3 | 12.8 to 18.0 | <0.001 |
| Chained practice (ref.: multi-practice) | 0.8 | −1.7 to 3.4 | 0.52 |
| Single practice (ref.: multi-practice) | 0.1 | −0.8 to 1.04 | 0.8 |
| No information on specialization (ref.: pediatric dentistry) | −0.3 | −2.8 to 2.3 | 0.84 |
| Any specialization (ref.: pediatric dentistry) | 0.2 | −2.4 to 2.72 | 0.89 |
| Rural (ref.: big city) | −0.34 | −1.7 to 1.1 | 0.64 |
| City (ref.: big city) | 0.022 | −0.8 to 0.8 | 0.96 |
| Age of dentists (cont., per year) | 0.4 | −0.04 to 0.75 | 0.08 |
| Number of dentists (cont.) | 0.035 | 1.98 to 3.7 | 0.72 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geiken, A.; Kock, M.; Banz, L.; Schwendicke, F.; Graetz, C. Dental Practice Websites in Germany—How Do They Inform about Fluoridation? Dent. J. 2024, 12, 65. https://doi.org/10.3390/dj12030065
Geiken A, Kock M, Banz L, Schwendicke F, Graetz C. Dental Practice Websites in Germany—How Do They Inform about Fluoridation? Dentistry Journal. 2024; 12(3):65. https://doi.org/10.3390/dj12030065
Chicago/Turabian StyleGeiken, Antje, Mirja Kock, Lisa Banz, Falk Schwendicke, and Christian Graetz. 2024. "Dental Practice Websites in Germany—How Do They Inform about Fluoridation?" Dentistry Journal 12, no. 3: 65. https://doi.org/10.3390/dj12030065
APA StyleGeiken, A., Kock, M., Banz, L., Schwendicke, F., & Graetz, C. (2024). Dental Practice Websites in Germany—How Do They Inform about Fluoridation? Dentistry Journal, 12(3), 65. https://doi.org/10.3390/dj12030065