

Automation in Dentistry with Mechanical Drills and Lasers for Implant Osteotomy: A Narrative-Scoping Review

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
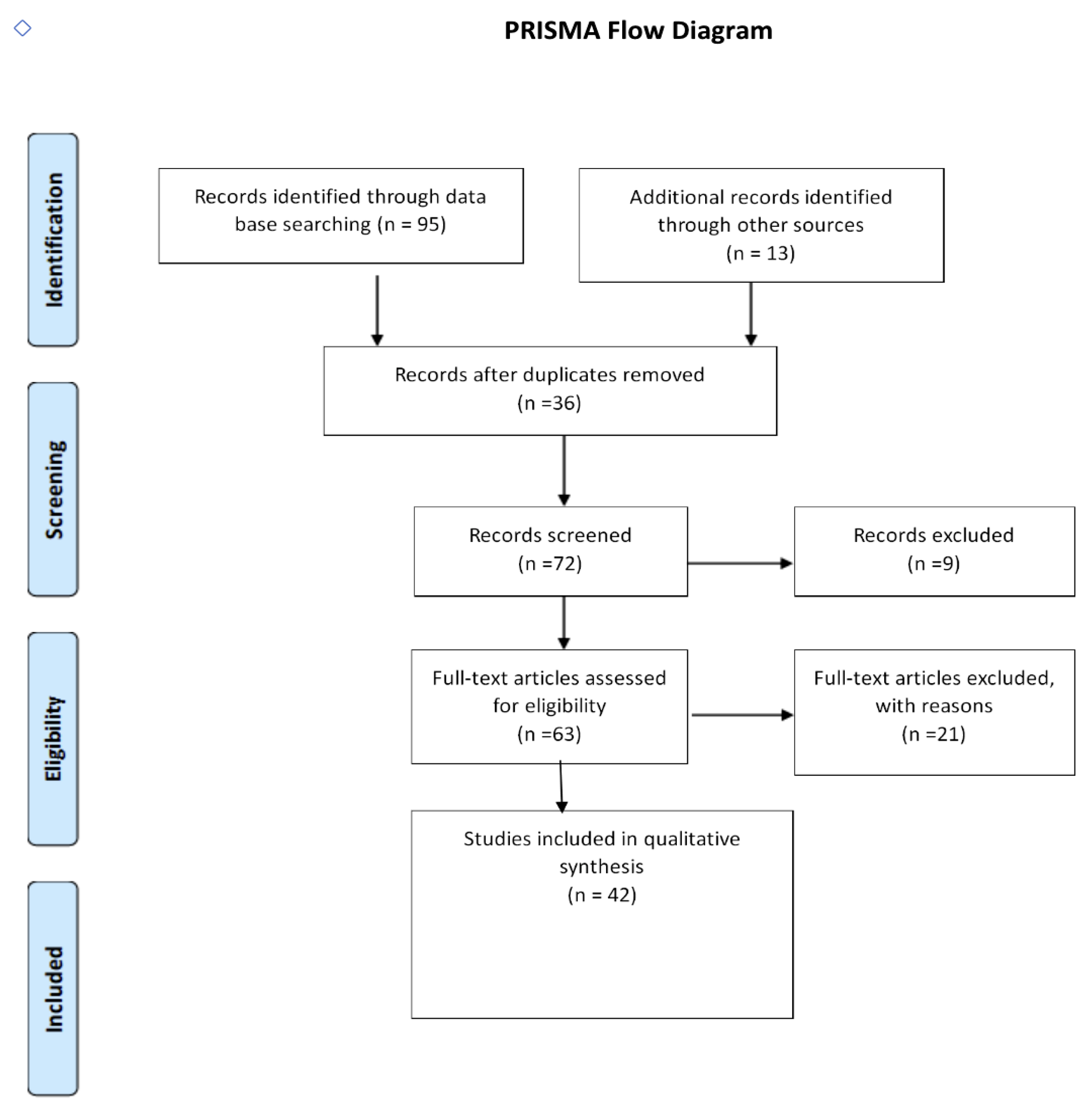
2. Search Methodology and Summary of Results
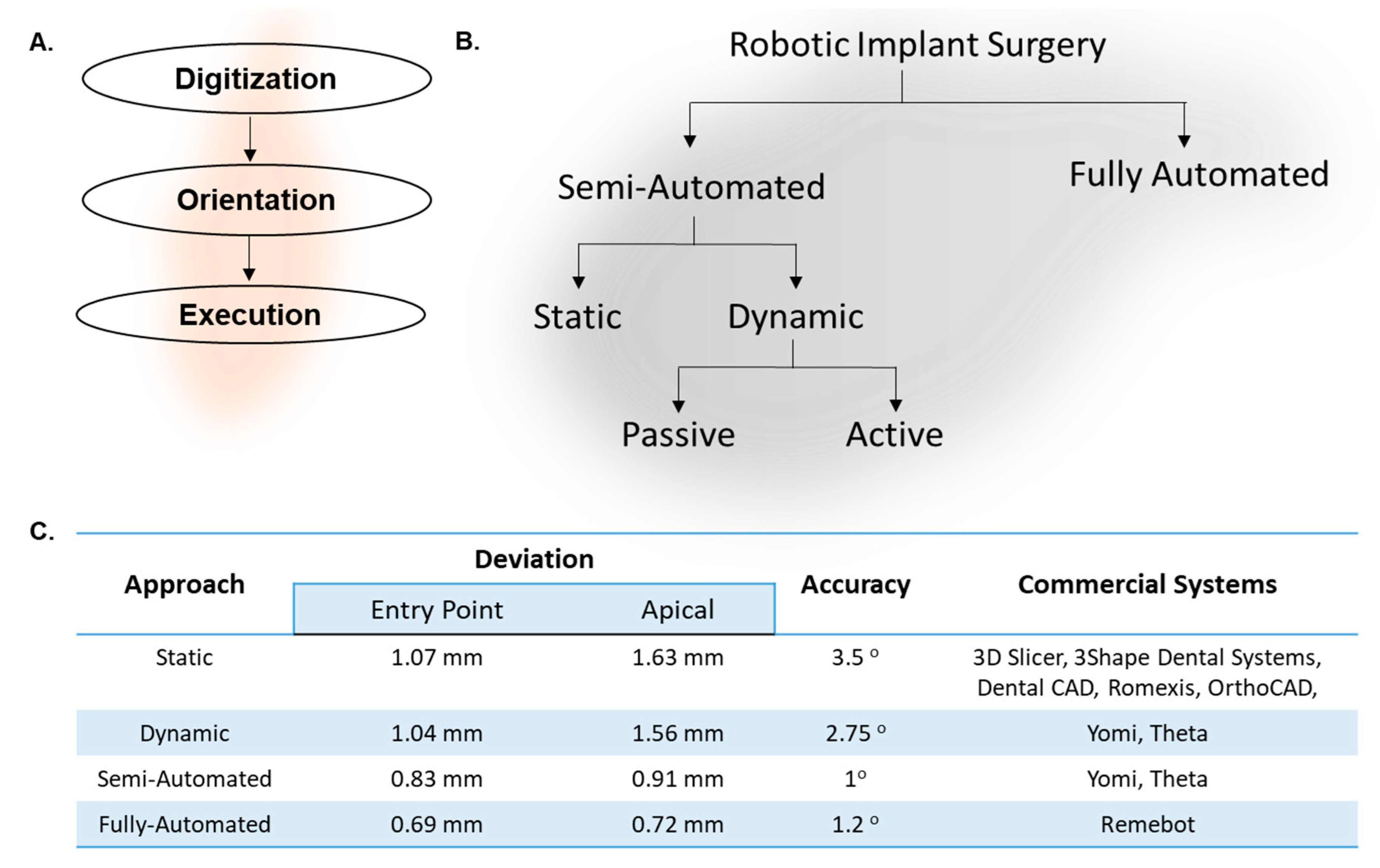
3. Common Features of Robotic or Automated Implant Surgery
4. Static Approach: Computer-Guided Implant Surgery
5. Dynamic Approach: Computer-Navigated Implant Surgery (Active or Passive)
6. Robot-Assisted Implant Surgery (Semi-Automated)
7. Fully-Automated Robotic Implant Surgery
8. Utility of Hard-Tissue Lasers
9. Barriers to Automation in Clinical Dentistry
10. Conclusions and Future Directions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Elagib, M.F.A.; Alqaysi, M.A.H.; Almushayt, M.O.S.; Nagate, R.R.; Gokhale, S.; Chaturvedi, S. Dental implants in growing patients: A systematic review and meta-analysis. Technol. Health Care 2022, 33, 1051–1064. [Google Scholar] [CrossRef] [PubMed]
- Tyrovolas, S.; Koyanagi, A.; Panagiotakos, D.B.; Haro, J.M.; Kassebaum, N.J.; Chrepa, V.; Kotsakis, G.A. Population prevalence of edentulism and its association with depression and self-rated health. Sci. Rep. 2016, 6, 37083. [Google Scholar] [CrossRef] [PubMed]
- Venkat, M.; Janakiram, C.; Ramanarayanan, V. Prevalence of Tooth Mortality among Adults in India: A Systematic Review and Meta-Analysis. Contemp. Clin. Dent. 2021, 12, 339–345. [Google Scholar] [CrossRef]
- Zelig, R.; Goldstein, S.; Touger-Decker, R.; Firestone, E.; Golden, A.; Johnson, Z.; Kaseta, A.; Sackey, J.; Tomesko, J.; Parrott, J.S. Tooth Loss and Nutritional Status in Older Adults: A Systematic Review and Meta-analysis. JDR Clin. Trans. Res. 2022, 7, 4–15. [Google Scholar] [CrossRef]
- Aiquel, L.L.; Pitta, J.; Antonoglou, G.N.; Mischak, I.; Sailer, I.; Payer, M. Does the timing of implant placement and loading influence biological outcomes of implant-supported multiple-unit fixed dental prosthesis-A systematic review with meta-analyses. Clin. Oral Implant. Res. 2021, 32 (Suppl. S21), 5–27. [Google Scholar] [CrossRef] [PubMed]
- Berlin-Broner, Y.; Levin, L. Dental Implant Success and Endodontic Condition of Adjacent Teeth: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2020, 35, e91–e97. [Google Scholar] [CrossRef] [PubMed]
- Hamed, M.T.; Mously, H.A.; Ghulman, M.M.; Naguib, G.H. Impact of dental implant diameter on the efficiency of fatigue: A systematic review analysis. J. Pak. Med. Assoc. 2021, 71, 1648–1654. [Google Scholar] [CrossRef]
- Guazzi, P.; Grandi, T.; Grandi, G. Implant site preparation using a single bur versus multiple drilling steps: 4-month post-loading results of a multicenter randomised controlled trial. Eur. J. Oral Implant. 2015, 8, 283–290. [Google Scholar]
- Arcuri, L.; Lorenzi, C.; Cecchetti, F.; Germano, F.; Spuntarelli, M.; Barlattani, A. Full digital workflow for implant-prosthetic rehabilitations: A case report. Oral Implant. 2015, 8, 114–121. [Google Scholar] [CrossRef]
- Bolding, S.L.; Reebye, U.N. Accuracy of haptic robotic guidance of dental implant surgery for completely edentulous arches. J. Prosthet. Dent. 2022, 128, 639–647. [Google Scholar] [CrossRef]
- Cheng, K.J.; Kan, T.S.; Liu, Y.F.; Zhu, W.D.; Zhu, F.D.; Wang, W.B.; Jiang, X.F.; Dong, X.T. Accuracy of dental implant surgery with robotic position feedback and registration algorithm: An in-vitro study. Comput. Biol. Med. 2021, 129, 104153. [Google Scholar] [CrossRef]
- Kan, T.S.; Cheng, K.J.; Liu, Y.F.; Wang, R.; Zhu, W.D.; Zhu, F.D.; Jiang, X.F.; Dong, X.T. Evaluation of a custom-designed human-robot collaboration control system for dental implant robot. Int. J. Med. Robot. 2022, 18, e2346. [Google Scholar] [CrossRef]
- Yang, S.; Chen, J.; Li, A.; Li, P.; Xu, S. Autonomous Robotic Surgery for Immediately Loaded Implant-Supported Maxillary Full-Arch Prosthesis: A Case Report. J. Clin. Med. 2022, 11, 6594. [Google Scholar] [CrossRef]
- Tack, P.; Victor, J.; Gemmel, P.; Annemans, L. 3D-printing techniques in a medical setting: A systematic literature review. Biomed. Eng. Online 2016, 15, 115. [Google Scholar] [CrossRef] [PubMed]
- Yan, B.; Zhang, W.; Cai, L.; Zheng, L.; Bao, K.; Rao, Y.; Yang, L.; Ye, W.; Guan, P.; Yang, W.; et al. Optics-guided Robotic System for Dental Implant Surgery. Chin. J. Mech. Eng. 2022, 35, 55. [Google Scholar] [CrossRef]
- Ashforth, S.A.; Oosterbeek, R.N.; Bodley, O.L.C.; Mohr, C.; Aguergaray, C.; Simpson, M.C. Femtosecond lasers for high-precision orthopedic surgery. Lasers Med. Sci. 2020, 35, 1263–1270. [Google Scholar] [CrossRef]
- Rajitha Gunaratne, G.D.; Khan, R.; Fick, D.; Robertson, B.; Dahotre, N.; Ironside, C. A review of the physiological and histological effects of laser osteotomy. J. Med. Eng. Technol. 2017, 41, 1–12. [Google Scholar] [CrossRef]
- Stubinger, S. Advances in bone surgery: The Er:YAG laser in oral surgery and implant dentistry. Clin. Cosmet. Investig. Dent. 2010, 2, 47–62. [Google Scholar] [CrossRef]
- Pantawane, M.; Dahotre, N. Challenges and Advances in Osteotomy. Ann. Bone Jt. Surg. 2019, 2, 1–4. [Google Scholar] [CrossRef]
- Gulati, M.; Anand, V.; Salaria, S.K.; Jain, N.; Gupta, S. Computerized implant-dentistry: Advances toward automation. J. Indian Soc. Periodontol. 2015, 19, 5–10. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, F.; Fan, S.; Chow, J.K. Robotics in Dental Implantology. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Soundaria Saravanan, C.A.M.; Singaravelu, S.K.; Raju, P.K. Application of digital technology in implant dentistry-an overview. Int. J. Adv. Res. 2020, 8, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Spielau, T.; Hauschild, U.; Katsoulis, J. Computer-assisted, template-guided immediate implant placement and loading in the mandible: A case report. BMC Oral Health 2019, 19, 55. [Google Scholar] [CrossRef] [PubMed]
- Marques, S.; Ribeiro, P.; Falcao, C.; Lemos, B.F.; Rios-Carrasco, B.; Rios-Santos, J.V.; Herrero-Climent, M. Digital Impressions in Implant Dentistry: A Literature Review. Int. J. Environ. Res. Public. Health 2021, 18, 1020. [Google Scholar] [CrossRef]
- Tanna, N.K.; AlMuzaini, A.; Mupparapu, M. Imaging in Orthodontics. Dent. Clin. N. Am. 2021, 65, 623–641. [Google Scholar] [CrossRef] [PubMed]
- Vafaee, F.; Firouz, F.; Mohajeri, M.; Hashemi, R.; Ghorbani Gholiabad, S. In vitro Comparison of the Accuracy (Precision and Trueness) of Seven Dental Scanners. J. Dent. 2021, 22, 8–13. [Google Scholar] [CrossRef]
- Verykokou, S.; Ioannidis, C. An Overview on Image-Based and Scanner-Based 3D Modeling Technologies. Sensors 2023, 23, 596. [Google Scholar] [CrossRef]
- Kernen, F.; Kramer, J.; Wanner, L.; Wismeijer, D.; Nelson, K.; Flugge, T. A review of virtual planning software for guided implant surgery—data import and visualization, drill guide design and manufacturing. BMC Oral Health 2020, 20, 251. [Google Scholar] [CrossRef]
- Vasoglou, G.; Stefanidaki, I.; Apostolopoulos, K.; Fotakidou, E.; Vasoglou, M. Accuracy of Mini-Implant Placement Using a Computer-Aided Designed Surgical Guide, with Information of Intraoral Scan and the Use of a Cone-Beam CT. Dent. J. 2022, 10, 104. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral. Implant. Res. 2018, 29 (Suppl. S16), 416–435. [Google Scholar] [CrossRef]
- Aydemir, C.A.; Arisan, V. Accuracy of dental implant placement via dynamic navigation or the freehand method: A split-mouth randomized controlled clinical trial. Clin. Oral Implant. Res. 2020, 31, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Roessler, K.; Winter, F.; Wilken, T.; Pataraia, E.; Mueller-Gerbl, M.; Dorfer, C. Robotic Navigated Laser Craniotomy for Depth Electrode Implantation in Epilepsy Surgery: A Cadaver Lab Study. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2021, 82, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Talwar, N.; Chand, P.; Singh, B.P.; Rao, J.; Pal, U.S.; Ram, H. Evaluation of the efficacy of a prosthodontic stent in determining the position of dental implants. J. Prosthodont. 2012, 21, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Tao, B.; Feng, Y.; Fan, X.; Zhuang, M.; Chen, X.; Wang, F.; Wu, Y. Accuracy of dental implant surgery using dynamic navigation and robotic systems: An in vitro study. J. Dent. 2022, 123, 104170. [Google Scholar] [CrossRef] [PubMed]
- Houssiau, F.A.; Devogelaer, J.P.; Van Damme, J.; de Deuxchaisnes, C.N.; Van Snick, J. Interleukin-6 in synovial fluid and serum of patients with rheumatoid arthritis and other inflammatory arthritides. Arthritis Rheum. 1988, 31, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, P.; Alam, M.K.; Aldajani, A.; Alahmari, A.; Alanazi, A.; Stoddart, M.; Sghaireen, M.G. Dental Robotics: A Disruptive Technology. Sensors 2021, 21, 3308. [Google Scholar] [CrossRef]
- Apostolopoulos, A.P.; Angelis, S.; Kaitatzi, M.; Kareliotis, G.; Tsiotsias, A.; Maris, S.J.; Filippou, D.K.; Makropoulou, M. The Facts and Myths for the Use of Lasers in Orthopedic Surgery. J. Long. Term. Eff. Med. Implant. 2021, 31, 55–69. [Google Scholar] [CrossRef]
- Romanos, G.E.; Gupta, B.; Yunker, M.; Romanos, E.B.; Malmstrom, H. Lasers use in dental implantology. Implant Dent. 2013, 22, 282–288. [Google Scholar] [CrossRef]
- Xue, V.W.; Zhao, I.S.; Yin, I.X.; Niu, J.Y.; Lo, E.C.M.; Chu, C.H. Effects of 9300 nm Carbon Dioxide Laser on Dental Hard Tissue: A Concise Review. Clin. Cosmet. Investig. Dent. 2021, 13, 155–161. [Google Scholar] [CrossRef]
- Heyder, M.; Sigusch, B.; Hoder-Przyrembel, C.; Schuetze, J.; Kranz, S.; Reise, M. Clinical effects of laser-based cavity preparation on class V resin-composite fillings. PLoS ONE 2022, 17, e0270312. [Google Scholar] [CrossRef]
- Domke, M.; Wick, S.; Laible, M.; Rapp, S.; Huber, H.P.; Sroka, R. Ultrafast dynamics of hard tissue ablation using femtosecond-lasers. J. Biophotonics 2018, 11, e201700373. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, H.; Beltran Bernal, L.M.; Hamidi, A.; Droneau, A.; Canbaz, F.; Guzman, R.; Jacques, S.L.; Cattin, P.C.; Zam, A. Combined Nd:YAG and Er:YAG lasers for real-time closed-loop tissue-specific laser osteotomy. Biomed. Opt. Express 2020, 11, 1790–1807. [Google Scholar] [CrossRef] [PubMed]
- Nalcaci, R.; Cokakoglu, S. Lasers in orthodontics. Eur. J. Dent. 2013, 7, S119–S125. [Google Scholar] [CrossRef]
- Honigmann, P.; Hofer, M.; Hirsch, S.; Morawska, M.; Muller-Gerbl, M.; Thieringer, F.M.; Coppo, E. Cold ablation robot-guided laser osteotomy in hand, wrist and forearm surgery-A feasibility study. Int. J. Med. Robot. 2022, 18, e2438. [Google Scholar] [CrossRef] [PubMed]
- Moslemi, N.; Shahnaz, A.; Masoumi, S.; Torabi, S.; Akbari, S. Laser-Assisted Osteotomy for Implant Site Preparation: A Literature Review. Implant. Dent. 2017, 26, 129–136. [Google Scholar] [CrossRef]
- Arora, A.; Upadhyaya, V.; Munjal, D.; Malik, D.; Parashar, D. Lasers—A Benefaction to Implant Dentistry. IOSR J. Dent. Med. Sci. 2017, 16, 119–125. [Google Scholar] [CrossRef]
- Chery, J.; Freitas, V.; Saman, D.M.; Gupta, A. Comparison of Cavity Preparation Times Using Conventional High-Speed Handpiece Versus Er, Cr:YSGG Laser: A Pilot Study with Pediatric Dental Residents. Pediatr. Dent. 2022, 44, 90–94. [Google Scholar]
- Stubinger, S.; Landes, C.; Seitz, O.; Sader, R. Er:YAG laser osteotomy for intraoral bone grafting procedures: A case series with a fiber-optic delivery system. J. Periodontol. 2007, 78, 2389–2394. [Google Scholar] [CrossRef]
- Nguendon Kenhagho, H.; Canbaz, F.; Gomez Alvarez-Arenas, T.E.; Guzman, R.; Cattin, P.; Zam, A. Machine Learning-Based Optoacoustic Tissue Classification Method for Laser Osteotomes Using an Air-Coupled Transducer. Lasers Surg. Med. 2021, 53, 377–389. [Google Scholar] [CrossRef]
- Chan, K.S.; Kwan, J.R.; Shelat, V.G. Awareness, perception, knowledge, and attitude toward robotic surgery in a general surgical outpatient clinic in Singapore, Asia. J. Clin. Transl. Res. 2022, 8, 224–233. [Google Scholar]
- McDermott, H.; Choudhury, N.; Lewin-Runacres, M.; Aemn, I.; Moss, E. Gender differences in understanding and acceptance of robot-assisted surgery. J. Robot. Surg. 2020, 14, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.; Salmon, B.; Codari, M.; Hassan, B.; Bornstein, M.M. Cone beam computed tomography in implant dentistry: Recommendations for clinical use. BMC Oral Health 2018, 18, 88. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Shi, M.; Liu, X.; Shi, Y. Uncertainty optimization of dental implant based on finite element method, global sensitivity analysis and support vector regression. Proc. Inst. Mech. Eng. Part H 2019, 233, 232–243. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Fan, L.; Zhang, S.; Zhao, J.; Gu, Y. Deep learning based dental implant failure prediction from periapical and panoramic films. Quant. Imaging Med. Surg. 2023, 13, 935–945. [Google Scholar] [CrossRef]
- Chen, H.; Li, H.; Sun, Y.; Wang, Y.; Lu, P. Femtosecond laser for cavity preparation in enamel and dentin: Ablation efficiency related factors. Sci. Rep. 2016, 6, 20950. [Google Scholar] [CrossRef]
- Chung, S.H.; Mazur, E. Surgical applications of femtosecond lasers. J. Biophotonics 2009, 2, 557–572. [Google Scholar] [CrossRef]
- Rapp, L.; Madden, S.; Brand, J.; Maximova, K.; Walsh, L.J.; Spallek, H.; Zuaiter, O.; Habeb, A.; Hirst, T.R.; Rode, A.V. Investigation of laser wavelength effect on the ablation of enamel and dentin using femtosecond laser pulses. Sci. Rep. 2023, 13, 20156. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ganta, G.K.; Mosca, R.C.; Varsani, R.; Murthy, V.R.; Cheruvu, K.; Lu, M.; Arany, P.R. Automation in Dentistry with Mechanical Drills and Lasers for Implant Osteotomy: A Narrative-Scoping Review. Dent. J. 2024, 12, 8. https://doi.org/10.3390/dj12010008
Ganta GK, Mosca RC, Varsani R, Murthy VR, Cheruvu K, Lu M, Arany PR. Automation in Dentistry with Mechanical Drills and Lasers for Implant Osteotomy: A Narrative-Scoping Review. Dentistry Journal. 2024; 12(1):8. https://doi.org/10.3390/dj12010008
Chicago/Turabian StyleGanta, Gopala Krishna, Rodrigo Crespo Mosca, Ridham Varsani, Venkata Ramana Murthy, Kamala Cheruvu, Michael Lu, and Praveen R. Arany. 2024. "Automation in Dentistry with Mechanical Drills and Lasers for Implant Osteotomy: A Narrative-Scoping Review" Dentistry Journal 12, no. 1: 8. https://doi.org/10.3390/dj12010008
APA StyleGanta, G. K., Mosca, R. C., Varsani, R., Murthy, V. R., Cheruvu, K., Lu, M., & Arany, P. R. (2024). Automation in Dentistry with Mechanical Drills and Lasers for Implant Osteotomy: A Narrative-Scoping Review. Dentistry Journal, 12(1), 8. https://doi.org/10.3390/dj12010008