

Esthetic Perception of Different Clinical Situations of Maxillary Lateral Incisor Agenesis According to Populations with Dental and Non-Dental Backgrounds: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. General Aspects
2.2. Search Strategy and Criteria
2.3. Data Extraction and Collection
2.4. Methodological Quality
2.5. Meta-Analysis
3. Results
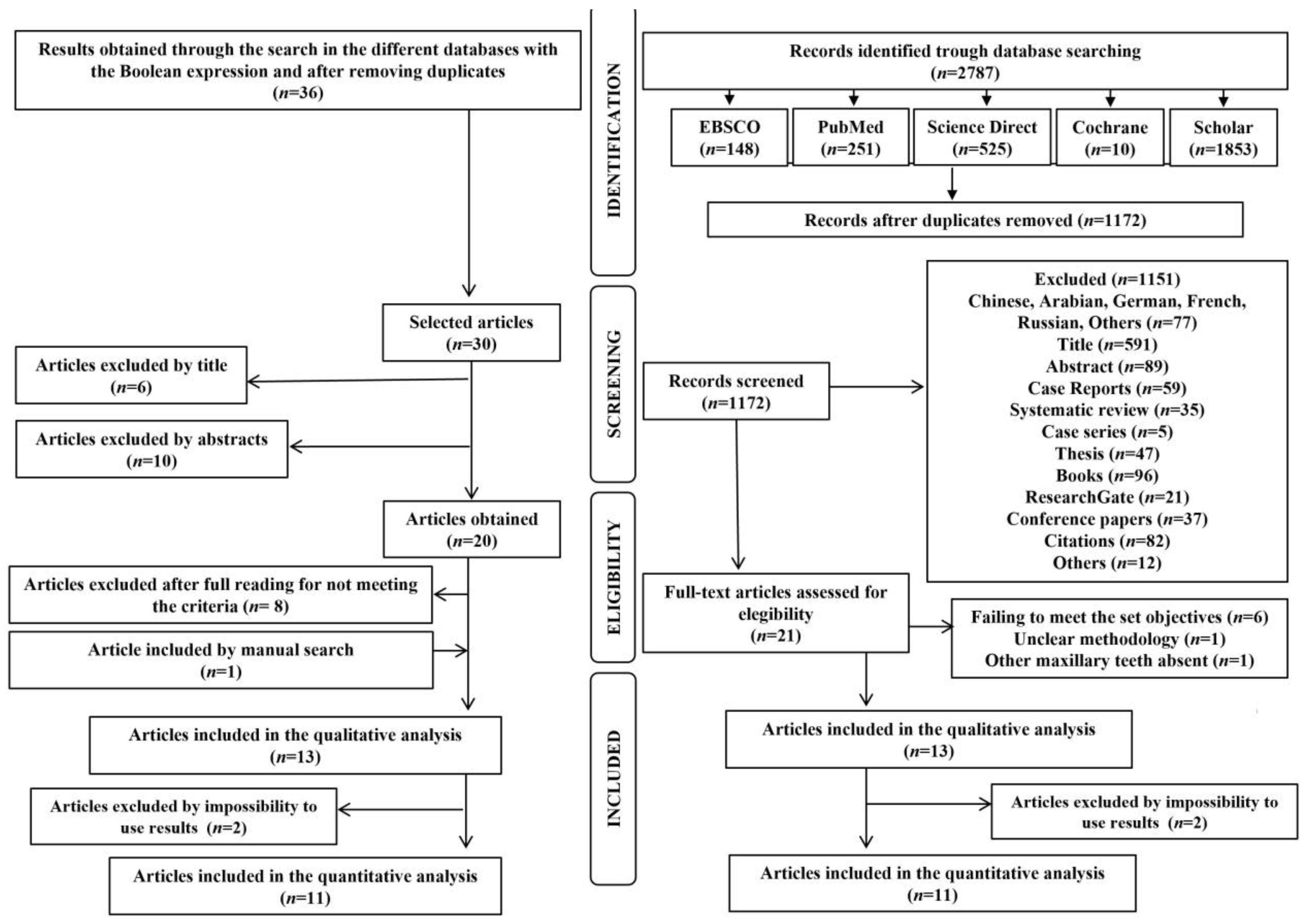
3.1. Study Selection
3.2. Study Characteristics and Descriptive Data Analysis
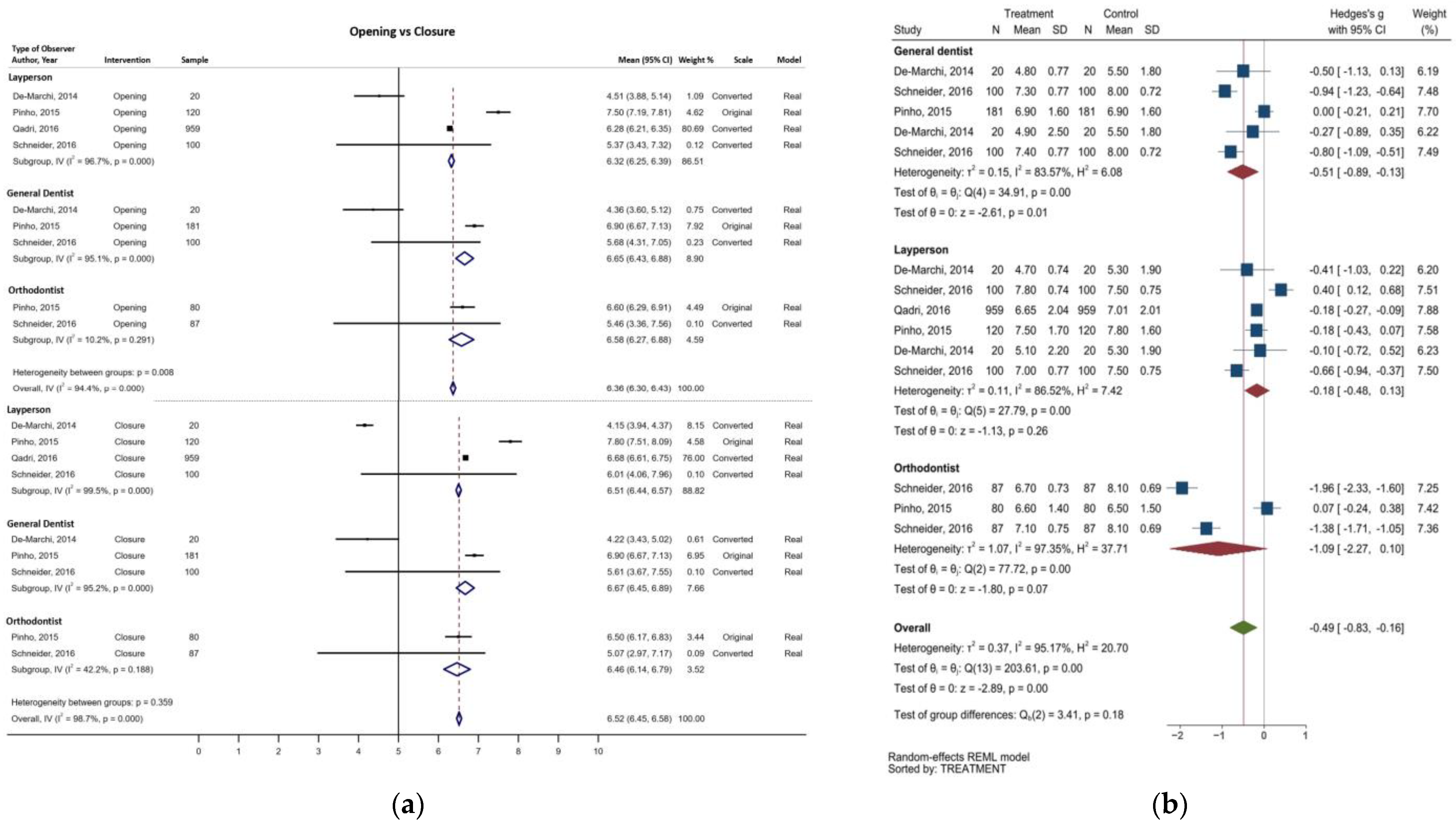
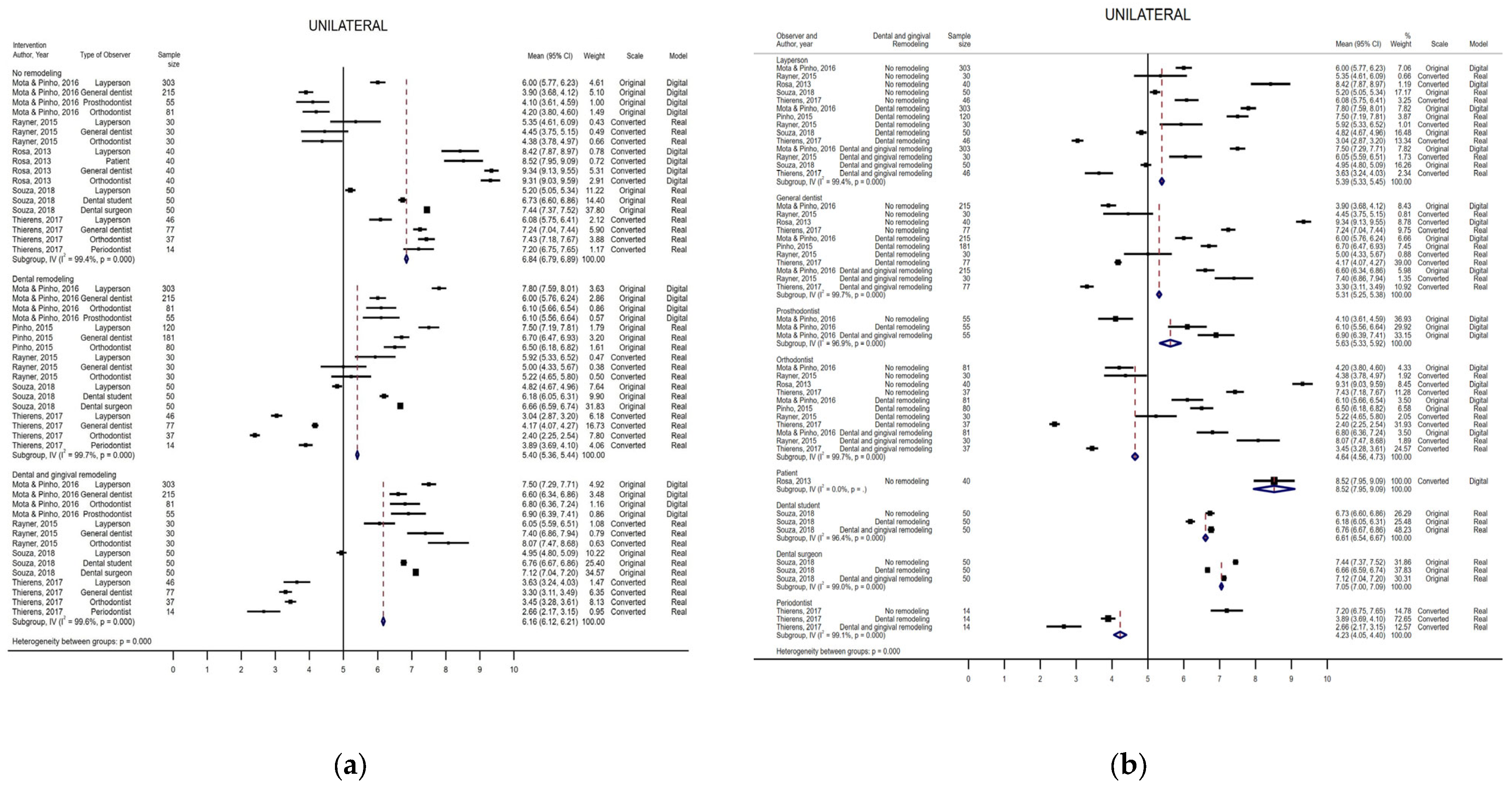
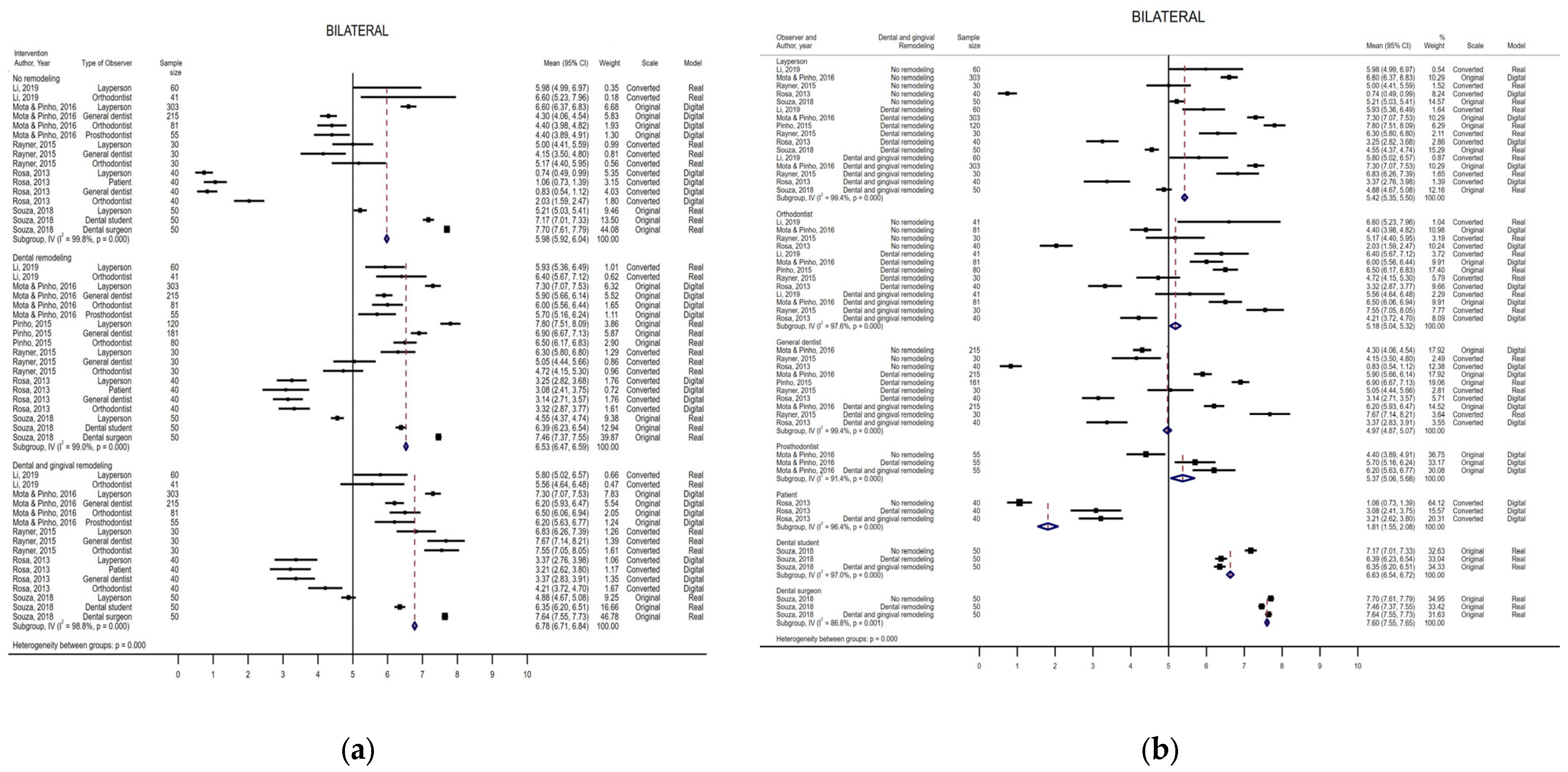
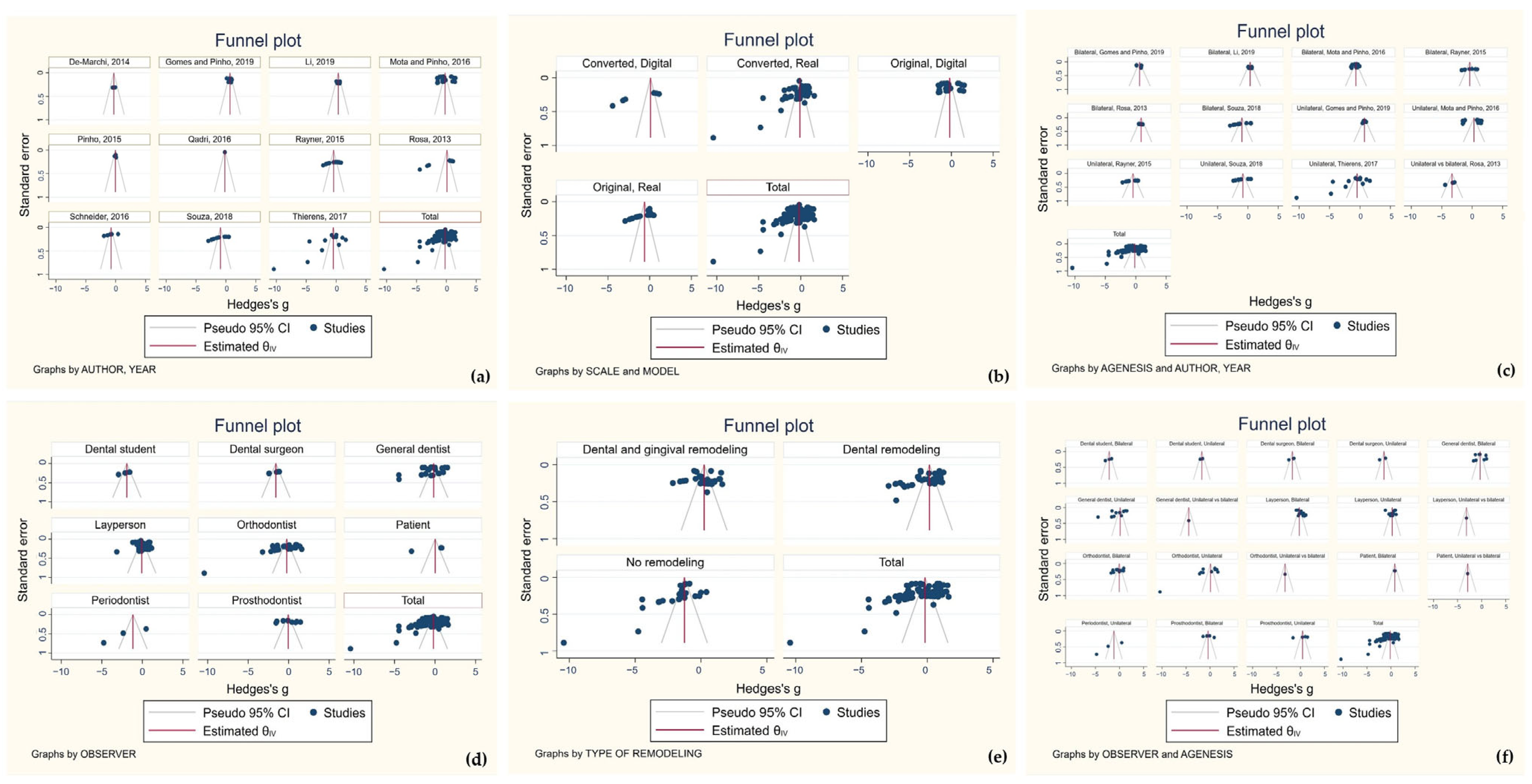
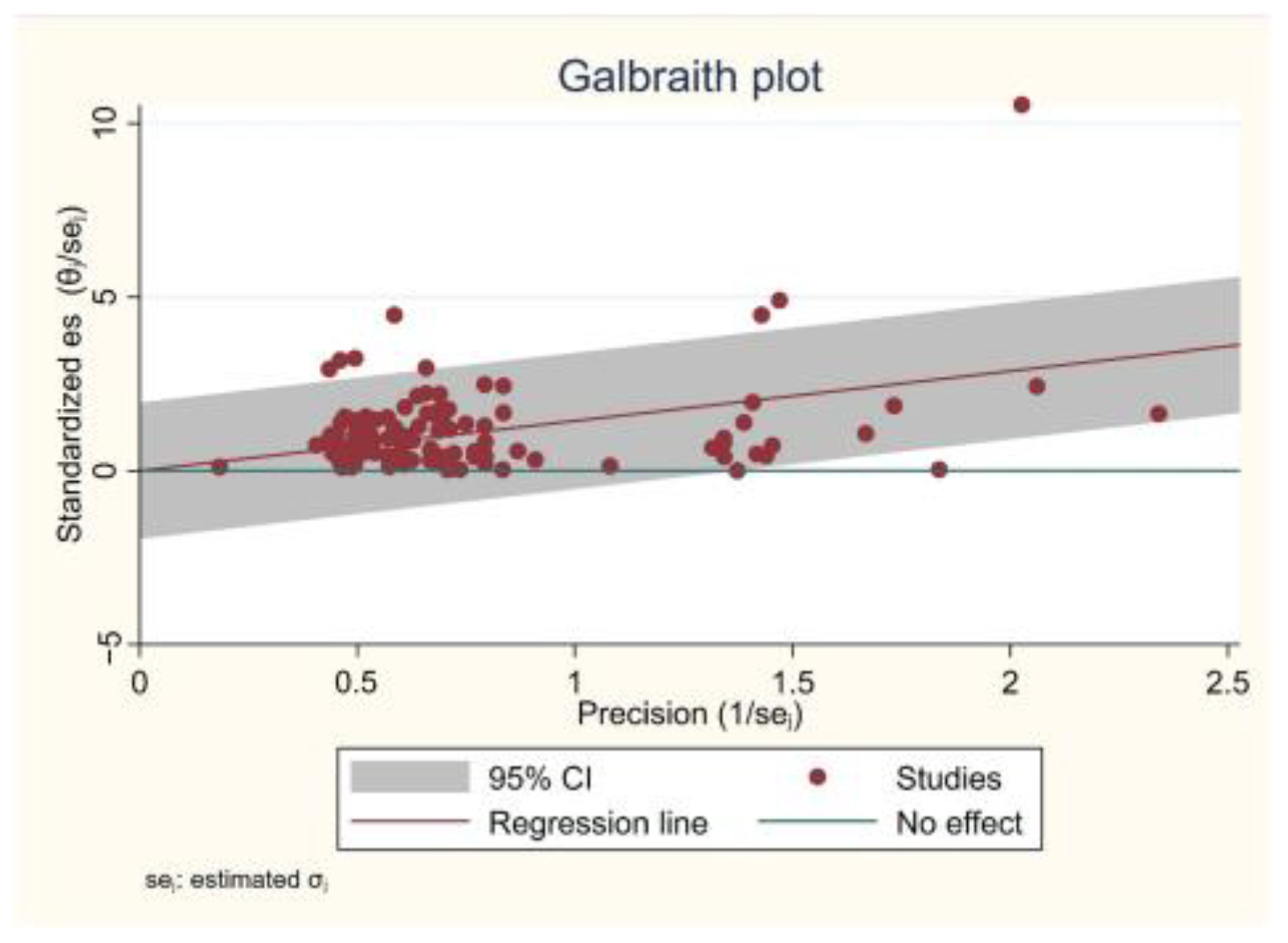
3.3. Meta-Analysis
4. Discussion
4.1. Differentiation Degree among Professionals
4.2. Age and Gender of the Participating Population
4.3. Digital and Real Models
4.4. Rating Scales
4.5. Smile Evaluation
4.6. Canine Morphology
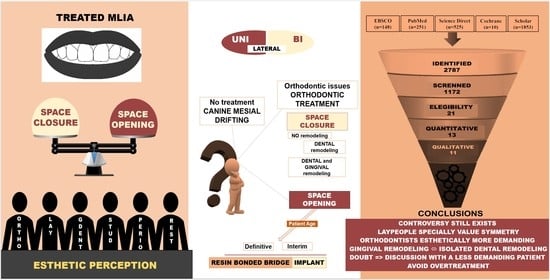
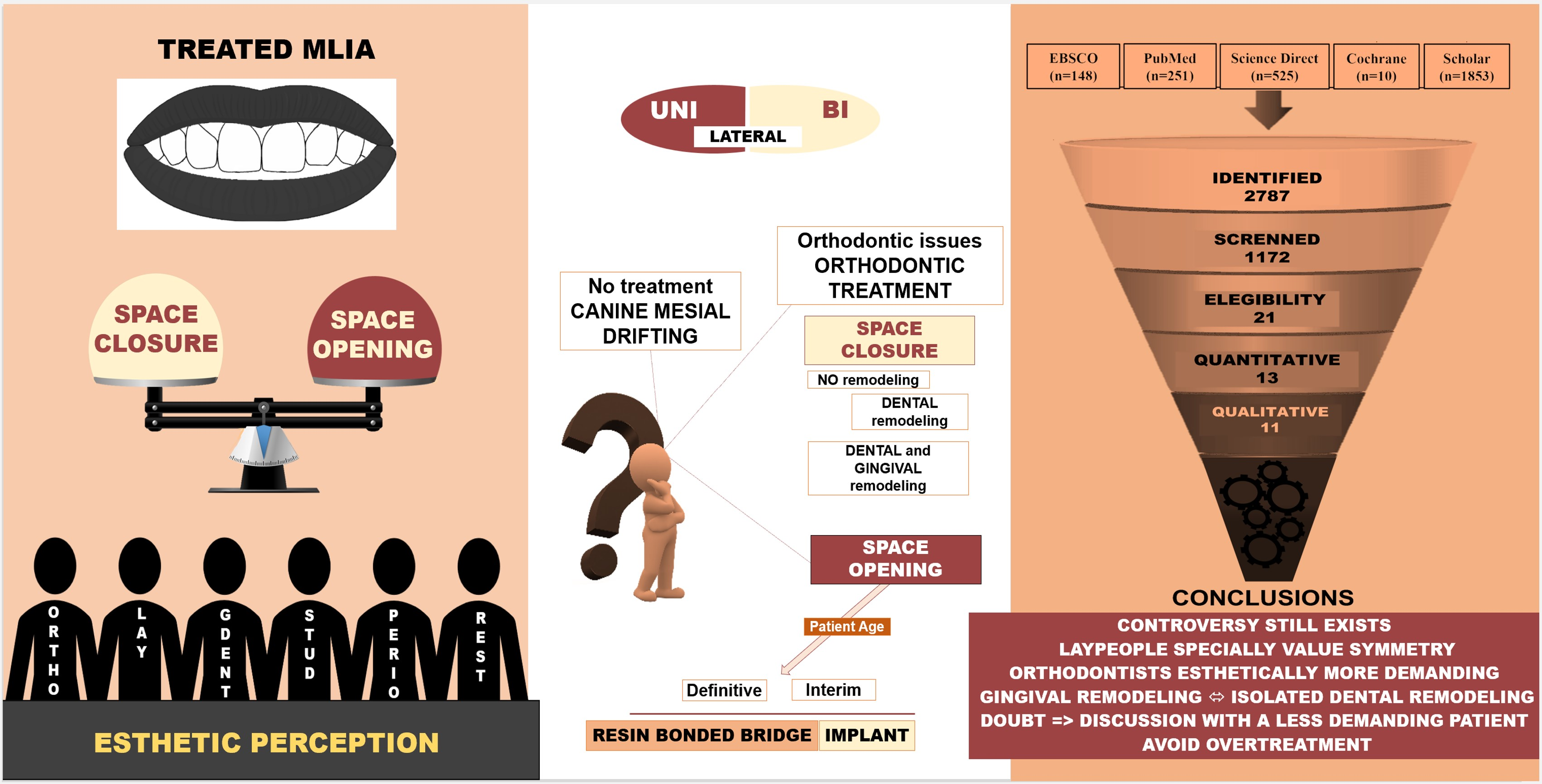
4.7. Different Options for MLIA Management
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Rodrigues, C.D.D.T.; Magnani, R.; Machado, M.S.; Oliveira, O.B. The perception of smile attractiveness. Angle Orthod. 2009, 79, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, P.L.E.; Motta, A.; Pithon, M.; Mucha, J. Details of pleasing smiles. Int. J. Esthet. Dent. 2018, 13, 494–514. [Google Scholar]
- Shamban, A. The signature feature(TM): A new concept in beauty. J. Cosmet. Dermatol. 2019, 18, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Romsics, L.; Segatto, A.; Boa, K.; Becsei, R.; Rózsa, N.; Szántó, I.; Nemes, J.; Segatto, E. Dentofacial mini- and microesthetics as perceived by dental students: A cross-sectional multi-site study. PLoS ONE 2020, 15, e0230182. [Google Scholar] [CrossRef] [PubMed]
- Lukez, A.; Pavlic, A.; Trinajstic Zrinski, M.; Spalj, S. The unique contribution of elements of smile aesthetics to psychosocial well-being. J. Oral Rehabil. 2015, 42, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Brough, E.; Donaldson, A.N.; Naini, F.B. Canine substitution for missing maxillary lateral incisors: The influence of canine morphology, size, and shade on perceptions of smile attractiveness. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 705.E1–705.E9, discussion 705–707. [Google Scholar] [CrossRef]
- De-Marchi, L.M.; Pini, N.I.; Ramos, A.L.; Pascotto, R.C. Smile attractiveness of patients treated for congenitally missing maxillary lateral incisors as rated by dentists, laypersons, and the patients themselves. J. Prosthet. Dent. 2014, 112, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Kokich, V.O.; Kokich, V.G.; Kiyak, H.A. Perceptions of dental professionals and laypersons to altered dental esthetics: Asymmetric and symmetric situations. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Rayner, W.J.; Barber, S.K.; Spencer, R.J. The effect of canine characteristics and symmetry on perceived smile attractiveness when canine teeth are substituted for lateral incisors. J. Orthod. 2015, 42, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Almuzian, M.; Mcintyre, G. Great Expectations of Patients with Missing Lateral Incisors: When are Space Opening and Space Closure Appropriate? Eur. J. Clin. Orthod. 2015, 3, 68–74. [Google Scholar]
- Dueled, E.; Gotfredsen, K.; Trab Damsgaard, M.; Hede, B. Professional and patient-based evaluation of oral rehabilitation in patients with tooth agenesis. Clin. Oral. Implant. Res. 2009, 20, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Kokich, V.O., Jr.; Kiyak, H.A.; Shapiro, P.A. Comparing the perception of dentists and lay people to altered dental esthetics. J. Esthet. Dent. 1999, 11, 311–324. [Google Scholar] [CrossRef] [PubMed]
- Pinho, S.; Ciriaco, C.; Faber, J.; Lenza, M.A. Impact of dental asymmetries on the perception of smile esthetics. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 748–753. [Google Scholar] [CrossRef] [PubMed]
- Mota, A.; Pinho, T. Esthetic perception of maxillary lateral incisor agenesis treatment by canine mesialization. Int. Orthod. 2016, 14, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Polder, B.J.; Van’t Hof, M.A.; Van der Linden, F.P.; Kuijpers-Jagtman, A.M. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Commun. Dent. Oral Epidemiol. 2004, 32, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Rosa, M.; Olimpo, A.; Fastuca, R.; Caprioglio, A. Perceptions of dental professionals and laypeople to altered dental esthetics in cases with congenitally missing maxillary lateral incisors. Prog. Orthod. 2013, 14, 34. [Google Scholar] [CrossRef] [PubMed]
- Lupinetti, G.M.; Li, P.; Feagin, K.; MacDougall, M.; Lamani, E. Non-syndromic hypodontia of maxillary lateral incisors and its association with other dental anomalies. Prog. Orthod. 2022, 23, 53. [Google Scholar] [CrossRef]
- Pinho, T.; Bellot-Arcis, C.; Montiel-Company, J.M.; Neves, M. Esthetic Assessment of the Effect of Gingival Exposure in the Smile of Patients with Unilateral and Bilateral Maxillary Incisor Agenesis. J. Prosthodont. 2015, 24, 366–372. [Google Scholar] [CrossRef]
- Armbruster, P.C.; Gardiner, D.M.; Whitley, J.B., Jr.; Flerra, J. The congenitally missing maxillary lateral incisor. Part 1: Esthetic judgment of treatment options. World J. Orthod. 2005, 6, 369–375. [Google Scholar] [PubMed]
- Abdulrahman, N.A.M.; Khalifa, N.; Alhajj, M.N. Dentists’ Preferences in the Treatment of Congenitally Missing Maxillary Lateral Incisors. Braz. Dent. Sci. 2019, 22, 243–251. [Google Scholar] [CrossRef]
- Carlson, H. Suggested treatment for missing lateral incisor cases. Angle Orthod. 1952, 22, 205–216. [Google Scholar]
- Silveira, G.S.; de Almeida, N.V.; Pereira, D.M.; Mattos, C.T.; Mucha, J.N. Prosthetic replacement vs space closure for maxillary lateral incisor agenesis: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 228–237. [Google Scholar] [CrossRef]
- Westgate, E.; Waring, D.; Malik, O.; Darcey, J. Management of missing maxillary lateral incisors in general practice: Space opening versus space closure. Br. Dent. J. 2019, 226, 400–406. [Google Scholar] [CrossRef]
- Seehra, J.; Al-Ali, A.; Pandis, N.; Cobourne, M.T. Space closure versus space opening for bilateral absent upper lateral incisors: What is the duration of orthodontic treatment? Eur. J. Orthod. 2019, 42, 460–465. [Google Scholar] [CrossRef]
- Gomes, A.F.; Pinho, T. Esthetic perception of asymmetric canines treated with space closure in maxillary lateral incisor agenesis. Int. J. Esthet. Dent. 2019, 14, 30–38. [Google Scholar] [PubMed]
- De-Marchi, L.M.; Pini, N.I.; Hayacibara, R.M.; Silva, R.S.; Pascotto, R.C. Congenitally missing maxillary lateral incisors: Functional and periodontal aspects in patients treated with implants or space closure and tooth re-contouring. Open Dent. J. 2012, 6, 248–254. [Google Scholar] [CrossRef]
- Jamilian, A.; Perillo, L.; Rosa, M. Missing upper incisors: A retrospective study of orthodontic space closure versus implant. Prog. Orthod. 2015, 16, 2. [Google Scholar] [CrossRef]
- Rosa, M.; Lucchi, P.; Ferrari, S.; Zachrisson, B.U.; Caprioglio, A. Congenitally missing maxillary lateral incisors: Long-term periodontal and functional evaluation after orthodontic space closure with first premolar intrusion and canine extrusion. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 339–348. [Google Scholar] [CrossRef]
- Schroeder, D.K.; Schroeder, M.A.; Vasconcelos, V. Agenesis of maxillary lateral incisors: Diagnosis and treatment options. Dent. Press. J. Orthod. 2022, 27, e22spe21. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.; Playle, R.; Harris, A.; Tredwin, C.; Addy, L. Does the gender of the subject affect perceived smile aesthetics when varying the dimensions of maxillary lateral incisors? Br. Dent. J. 2018, 225, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Pini, N.I.; De-Marchi, L.M.; Gribel, B.; Ramos, A.L.; Furquim, L.; Pascotto, R.C. Analysis of width/height ratio and gingival zenith in patients with bilateral agenesis of maxillary lateral incisor. Dent. Press. J. Orthod. 2012, 17, 87–93. [Google Scholar] [CrossRef]
- Patusco, V.; Carvalho, C.K.; Lenza, M.A.; Faber, J. Smile prevails over other facial components of male facial esthetics. J. Am. Dent. Assoc. 2018, 149, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, L.; Pinho, T. Esthetic evaluation of dental and gingival asymmetries. Int. Orthod. 2015, 13, 221–231. [Google Scholar] [CrossRef]
- Janson, G.; Branco, N.C.; Fernandes, T.M.; Sathler, R.; Garib, D.; Lauris, J.R. Influence of orthodontic treatment, midline position, buccal corridor and smile arc on smile attractiveness. Angle Orthod. 2011, 81, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Miyoshi, C.S.; Rached, R.N.; Meira, T.M.; Allahham, A.; Saga, A.Y.; Tanaka, O.M. The Eye-Tracking Study of the Impact of the Gingival Margin Height of Maxillary Lateral Incisors. Int. J. Periodontics Restor. Dent. 2020, 40, 261–270. [Google Scholar] [CrossRef]
- Armbruster, P.C.; Gardiner, D.M.; Whitley, J.B., Jr.; Flerra, J. The congenital missing maxillary lateral incisor. Part 2: Assessing dentists’ preferences for treatment. World J. Orthod. 2005, 6, 376–381. [Google Scholar]
- Althagafi, N. Esthetic Smile Perception Among Dental Students at Different Educational Levels. Clin. Cosmet. Investig. Dent. 2021, 13, 163–172. [Google Scholar] [CrossRef]
- Senty, E.L. The maxillary cuspid and missing lateral incisors: Esthetics and occlusion. Angle Orthod. 1976, 46, 365–371. [Google Scholar]
- Kafantaris, S.N.; Tortopidis, D.; Pissiotis, A.L.; Kafantaris, N.M. Factors Affecting Decision-Making For Congenitally Missing Permanent Maxillary Lateral Incisors: A Retrospective Study. Eur. J. Prosthodont. Restor. Dent. 2020, 28, 43–52. [Google Scholar] [CrossRef]
- Cocconi, R.; Rapa, S. Unilateral agenesis of the maxillary lateral incisor: Space closure versus space preservation in growing patients. Semin. Orthod. 2020, 26, 24–32. [Google Scholar] [CrossRef]
- Josefsson, E.; Lindsten, R. Treatment of missing maxillary lateral incisors: A clinical and aesthetic evaluation. Eur. J. Orthod. 2019, 41, 273–278. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Harzing, A.-W.; Alakangas, S. Google Scholar, Scopus and the Web of Science: A longitudinal and cross-disciplinary comparison. Scientometrics 2016, 106, 787–804. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Andrade, D.C.; Loureiro, C.A.; Araujo, V.E.; Riera, R.; Atallah, A.N. Treatment for agenesis of maxillary lateral incisors: A systematic review. Orthod. Craniofac. Res. 2013, 16, 129–136. [Google Scholar] [CrossRef]
- Li, R.; Mei, L.; Wang, P.; He, J.; Meng, Q.; Zhong, L.; Zheng, W.; Li, Y. Canine edge width and height affect dental esthetics in maxillary canine substitution treatment. Prog. Orthod. 2019, 20, 16. [Google Scholar] [CrossRef]
- Qadri, S.; Parkin, N.A.; Benson, P.E. Space closing versus space opening for bilateral missing upper laterals–aesthetic judgments of laypeople: A web-based survey. J. Orthod. 2016, 43, 137–146. [Google Scholar] [CrossRef]
- Schneider, U.; Moser, L.; Fornasetti, M.; Piattella, M.; Siciliani, G. Esthetic evaluation of implants vs canine substitution in patients with congenitally missing maxillary lateral incisors: Are there any new insights? Am. J. Orthod. Dentofac. Orthop. 2016, 150, 416–424. [Google Scholar] [CrossRef]
- Souza, R.A.; Alves, G.N.; Mattos, J.M.; Coqueiro, R.D.S.; Pithon, M.M.; Paiva, J.B. Perception of attractiveness of missing maxillary lateral incisors replaced by canines. Dent. Press. J. Orthod. 2018, 23, 65–74. [Google Scholar] [CrossRef]
- Thierens, L.A.M.; Verhoeven, B.; Temmerman, L.; De Pauw, G.A.M. An esthetic evaluation of unilateral canine substitution for a missing maxillary lateral incisor. J. Esthet. Restor. Dent. 2017, 29, 442–449. [Google Scholar] [CrossRef]
- De-Marchi, L.M.; Pini, N.I.; Pascotto, R.C. The relationship between smile attractiveness and esthetic parameters of patients with lateral agenesis treated with tooth recontouring or implants. Clin. Cosmet. Investig. Dent. 2012, 4, 43–49. [Google Scholar] [CrossRef]
- Sriphadungporn, C.; Chamnannidiadha, N. Perception of smile esthetics by laypeople of different ages. Prog. Orthod. 2017, 18, 8. [Google Scholar] [CrossRef]
- Martinez Florez, D.; Rinchuse, D.; Zullo, T. Influence of maxillary lateral incisor width ratio on perception of smile esthetics among orthodontists and laypersons. J. Esthet. Restor. Dent. 2021, 33, 510–515. [Google Scholar] [CrossRef]
- Rosas, S.; Paço, M.; Lemos, C.; Pinho, T. Comparison between the Visual Analog Scale and the Numerical Rating Scale in the perception of esthetics and pain. Int. Orthod. 2017, 15, 543–560. [Google Scholar] [CrossRef]
- Greta, D.C.; Colosi, H.A.; Gasparik, C.; Dudea, D. Perceptions of Dental Dyschromia by Patients and Dentist. Int. J. Prosthodont. 2021, 34, 154–162. [Google Scholar] [CrossRef]
- Bukhary, S.M.; Gill, D.S.; Tredwin, C.J.; Moles, D.R. The influence of varying maxillary lateral incisor dimensions on perceived smile aesthetics. Br. Dent. J. 2007, 203, 687–693. [Google Scholar] [CrossRef]
- Saffarpour, A.; Ghavam, M.; Saffarpour, A.; Dayani, R.; Fard, M.J. Perception of Laypeople and Dental Professionals of Smile Esthetics. J. Dent. (Tehran) 2016, 13, 85–91. [Google Scholar]
- Chandra Pani, S.; Fernandez, R.A.; Ihsan Kudsi, R.; Elkhawly, F.F.; AlBatran, A.N.; Nasser, M.A. The Impact of Lateral Incisor Dimensions on Smile Perception—A Study of Patients Tolerance for Deviation from the Ideal. Periodontics Prosthodont. 2016, 2, 5. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Size Calculation | Selection Description | Dropout | Valid methodology | Confounding Variables | Blind Measurements | Adequate Statistics Analysis | Qualitative Scoring | |
|---|---|---|---|---|---|---|---|---|
| Armbruster et al. 2005 [19] | - | ? | + | + | - | + | + | Moderate |
| Brough et al. 2010 [6] | - | + | + | + | + | + | + | High |
| De-Marchi et al. 2014 [7] | - | ? | + | + | - | + | + | Moderate |
| Gomes & Pinho 2019 [25] | - | + | + | + | + | + | + | High |
| Li et al. 2019 [48] | - | ? | + | + | + | + | + | High |
| Mota & Pinho 2016 [14] | + | + | + | + | + | + | + | High |
| Pinho et al. 2015 [18] | - | ? | + | + | + | - | + | Moderate |
| Qadri et al. 2016 [49] | + | + | + | + | + | - | + | High |
| Rayner et al. 2015 [9] | + | + | + | + | + | + | + | High |
| Rosa et al. 2013 [16] | + | ? | + | + | + | + | + | High |
| Schneider et al. 2016 [50] | - | ? | + | + | - | + | + | Moderate |
| Souza et al. 2018 [51] | + | + | + | + | + | + | + | High |
| Thierens et al. 2017 [52] | - | + | + | + | + | + | + | High |
| Author, Year | Type of Observer | Sample |
|---|---|---|
| Armbruster et al. (2005) [19] | General dentist | 140 |
| Layperson | 60 | |
| Orthodontist | 40 | |
| Dental specialists | 29 | |
| Brough et al. (2010) [6] | General dentist | 40 |
| Layperson | 40 | |
| Orthodontist | 40 | |
| De-Marchi et al. (2014) [7] | Orthodontist | 20 |
| Periodontists | 20 | |
| Gomes and Pinho (2016) [25] | General dentist | 141 |
| Layperson | 142 | |
| Orthodontist | 100 | |
| Periodontists | 51 | |
| Li et al. (2019) [48] | Layperson | 60 |
| Orthodontist | 41 | |
| Mota and Pinho (2016) [14] | General dentist | 215 |
| Layperson | 303 | |
| Orthodontist | 81 | |
| Prosthodontist | 55 | |
| Pinho et al. (2015) [18] | General dentist | 181 |
| Layperson | 120 | |
| Orthodontist | 80 | |
| Qadri et al. (2016) [49] | Layperson | 959 |
| Rayner et al. (2015) [9] | General dentist | 30 |
| Layperson | 30 | |
| Orthodontist | 30 | |
| Rosa et al. (2013) [16] | General dentist | 40 |
| Layperson | 40 | |
| Orthodontist | 40 | |
| Patient | 40 | |
| Schneider et al. (2016) [50] | General dentist | 100 |
| Orthodontist | 87 | |
| Souza et al. (2018) [51] | Dental student | 50 |
| Dental surgeon | 50 | |
| Layperson | 50 | |
| Thierens et al. (2017) [52] | General dentist | 77 |
| Layperson | 46 | |
| Orthodontist | 37 | |
| Periodontists | 14 |
| Study | Population | Interventions | Objectives | Parameters | Outcome | Validity of Methods | Confounding Variables | Study Design |
|---|---|---|---|---|---|---|---|---|
| Armbruster et al. (2005) [19] | 40 (L) 140 (GDPs) 43 (O) 29 specialists (SP) (9 PT, 11 END, 3 SUR, 4 OD, and 2 P) | Direct visual observation. Observers blinded for treatment options. | Esthetic appearance of various treatment options of treated MLIA cases. | MLIA treated with Maryland bridges (MB), dental implants (IP), orthodontic canine reposition (CR), or no-MLIA (control)(NT). 1 (more) to 5 (less attractive). | (O) NT > CR > MB > I (GDPs)-NT = CR > MB = I (SP)-NT = CR > MB = I (L)–CR > NT > MB > I (p < 0.001). | YES real model | YES multiple variables | N-RCT CI |
| Brough et al. (2010) [6] | 40 (L) 40 (GDPs) 40 (O) | Direct visual ranking of images digitally manipulated from original photography. Blind and random evaluation. | Smile attractiveness in patients with MLIA vs. natural whole dentition. | Gradual increment of canine width, crown height and morphology, and gingival margin height. No quantitative measures. | (All) Dark, large canines, gingival margin >0.5 mm above central incisive-unattractive. Narrow canines–better rank. (GDPs)-natural tones; (O)-slightly brighter tones. (L)-brighter tones; (O)-cusps < 1.0 mm; (L)-cusps 1.0–1.5 mm. | YES digital model | NO same teeth same gum | N-RCT NCI |
| De-Marchi et al. (2014) [7] | 20 (L) (10M,10F) and 20 (GDPs) > 4 years practice (10M,10F) | Direct visual observation of 68 photographs 26 (SC + R) 20 (SO + IP) 22 (no-MLIA). | Attractiveness of smiles in patients with MLIA vs. natural whole dentition. | Controlled photographic protocol. Unpleasant: 0 to 50.99 mm. Nice: 51–100 mm | (Male GDPs)-most critical Volunteers -control group–very pleased with their smiles. Patient satisfaction SC +R > SOI; more satisfied than control group (p < 0.002). | YES real model | YES different lips different teeth | N-RCT CI |
| Gomes & Pinho (2019) [25] | 142 (L) 141 (GDPs) 100 (O) 51 (PT) | Quiz. Numerical Valuation. Ranking in ascending order. Anonymous. | Esthetic perception of asymmetric MLIA treated with SC and canine mesialization. | Space closure of MLIA with asymmetric canines. 2 symmetric simulations. Digital manipulation (smile 1—smaller canines) (smile 2—larger canines). Visual analog scale (VAS) (0–10). | Pretreatment image-least esthetic. Orthodontic treatment- improvement. Symmetric canines–most esthetic. Larger canines–more esthetic. Differences between (GDPs and L) regarding the most and least esthetic approach(p < 0.05). (L) more impressed than professionals; dental specialists more demanding (p < 0.05). | YES real model | NO same parameters same model | N-RTC NC |
| Li et al. (2019) [48] | 60 (L) 41 (O) | Direct visual photo observation. Ranking of images digitally manipulated from original photography. 140 | Canine edge width and height affect in dental esthetics in canine mesialization. | 127 closure treatments. Top 5 most pleasant cases, digitally manipulated; 140 images with canine edge widths ((0, 12.5, 25, 37.5, 50, 62.5 and 75% of the central incisor width) and heights (−0.5, 0, 0.5 and 1.0 mm relative to central incisor edge)). | Most esthetic canine shape-canine edge-62.5% of the central incisor width and −0.5 mm gingival to the central incisor edge (p < 0.005). Canine edge width (p = 0.003) and height (p < 0.001) affect esthetics in canine substitutions. | YES Digital model | NO same gingiva same teeth | N-RTC NCI |
| Mota & Pinho (2016) [14] | 303 (L) 215 (GDPs) 81 (O) 55 (PT) | Online survey. Digital manipulation. | Perception of smile attractiveness in MLIA cases treated with canine mesialization. | 9 digital photos of MLIA treatment involving space closure. Unilateral and bilateral. Numeric scale (1–10) (least to most attractive) >5-attractive <5-unattractive. | (L)-better scored all cases/other groups. (All)–ideal smile = smile with lateral incisors. (All)–canine remodeling-more attractive. GDPs/O/PT- favor canine remodeling + gingival remodeling. | YES digital model | NO | N-RCT CI |
| Pinho et al. (2015) [18] | 120 (L) 181 (GDPs) 80 (O) | Online survey. Esthetic perception preferences. Pre-and post-treatment evaluations. | Smile esthetic perception in patients with MLIA with respect to gingival exposure. | 4 clinical cases. 24 smile photos. Numerical scale 0–10. | All photos score- O < GDPs < L. Males- highest scores. Symmetric cases and medium smile- higher scored. Gingival exposure- significant influence on the esthetic perception in post-treatment cases (p < 0.001). | YES real model | YES same lips different teeth | N-RCT NCI |
| Qadri et al. (2016) [49] | 959 (DSt) and University staff F/M (76%/24%) 5 (O) 5 (RD) | Online survey. 959 completed responses with 9590 judgments. 4 pairs of photos. BILATERAL | Esthetic perception concerning the outcome of bilateral MLIA treatment patients with SC, SO, or IP. | 21 patients (11 SC/10 PR). 10 specialist dentists (O + RD) ranked the photos. Most attractive (1)-least attractive (22). Only bilaterally MLIA included in this study. | SC-more attractive/PR (p < 0.001). Females and staff-higher ratings. Females/males-preferred SC/PR = 3/1 (p < 0.001). Space closure more attractive than space opening by (L). | YES Real morphed model Photo size standardization | YES multiple variables | N-RCT NCI Cross-sectional |
| Rayner et al. (2015) [9] | 30 (L) 30 (GDPs) 30 (O) | Direct visual observation. Digital manipulation. (average female face image based on frontal photos of 4 female volunteers). | Effect of canine characteristics and symmetry on perceived smile attractiveness, in MLIA treated with canine mesialization. | 1 ideal image. 6 morphed images (canine with lateral incisor-unilateral and bilateral). 3 types of canine created using software. Variations in shape, length, and color. | (O, GDPs)-space closure with canine significantly less attractive/ideal smile unless replaced by ideal canines(p < 0.001). (L)-lateral incisors replaced with canines different from ideal smile, but not clinically significant. (All)– unilateral replacement not significantly less attractive than bilateral replacement. | YES real model | NO same face same teeth same smile | N-RCT CI |
| Rosa et al. (2013) [16] | 40 (L) 40 (OP) 40 (GDPs) 40 (O) | Quiz. Digital model of an ideal smile. Ranking (descriptive analysis). Numerical valuation. | Valuation of esthetic perception in altered smiles due to MLIA with or without treatment. | 12 simulations. Visual analog scale (VAS) 0 to 100. | Significant differences–(All professionals) and (L) (p < 0.005). Orthodontic treatment, absence of diastema, symmetry-higher valued by all groups. | YES digital model | NO same parameters same model | N-RCT NCI |
| Schneider et al. (2016) [50] | 100 (L) 100 (GDPs) 87 (O) Blinded observers | Direct visual photo observation. 9 frontal photos 3-SC + R 3-SO + IP 3-no-MLIA | Esthetic evaluation of implants vs canine substitution in patients with MLIA. | 7 pairs of bipolar adjectives. Smiles classified from 1–5 (less-more attractive). | O/GDPs-no-MLIA more attractive than SC + R > SO + IP (Non-significant). L-SC + R > no-MLIA > SP + IP. L/GDPs-Better scores for SC + R. All groups-Worst scores for SO + IP (Nonsignificant). | YES Real Model Best photo preselection by orthodontists | YES multiple variables Mixed cases | N-RCT CI |
| Souza et al. (2018) [51] | (L) (GDPs) (DSt) 150 (22 and 40 y) Similar socioeconomic status | Direct visual observation. Digital manipulation. SC UNILATERAL BILATERAL (R + G) (R + B + G) ® (R + C + G) (R + B) | Perception of the attractiveness of MLIA replaced with canine mesialization. | Extraoral photograph. 20-year-old woman-normal occlusion. Software manipulation of original photograph. Mandibular arch without modifications. Various compositions with different sizes and proportions of height and width of the teeth to simulate repositioning of the canine on the left, right, or both sides. VAS 0 to 10, (less to more esthetic). | Original image–highest acceptance by (All). Lowest acceptance–left side alterations. Bilateral R + G-highest scores from (L). R + C-lowest score from (GDPs). (DSt)-least attractive–bilateral alterations Globally–(L)-lowest scores/other groups Least acceptable–(All) groups-bleaching (L)-attractive—bleached mesialized canines without treatment. (GDPs and DSt)- notice more differences than (L). (L)-cannot detect some interventions. | YES Real Digitally manipulated Model | NO same teeth same gum same mandibular teeth | N-RCT CI |
| Thierens et al. (2017) [52] | 46 (L) 77 (GDPs) 37 (O) 14 (P) (age, experience, and gender, except the mean age of (O) to (L)) Female: Male (ratio 1.5:1) | Direct visual observation. Digital manipulation. Ranking by attractiveness. UNILATERAL | Size, morphology, and color of the substitute canine influence on dento-gingival attractiveness perceived by dental professionals and laypeople. | Standard image. Five series (width, color, gingival margin height, canine crown tip, and gingival margin height of the neighboring first premolar). Image most deviated from the standard/each parameter combined into a final series. | Dark canine and pronounced tip of a substituted canine-most unattractive to (All) professionals and (L). Gingival height of the neighboring premolar-least unattractive–(All) groups of examiners. | YES Real Digitally manipulated model | NO same teeth same gum same mandibular teeth | N-RCT CI |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calheiros-Lobo, M.J.; Calheiros-Lobo, M.; Pinho, T. Esthetic Perception of Different Clinical Situations of Maxillary Lateral Incisor Agenesis According to Populations with Dental and Non-Dental Backgrounds: A Systematic Review and Meta-Analysis. Dent. J. 2023, 11, 105. https://doi.org/10.3390/dj11040105
Calheiros-Lobo MJ, Calheiros-Lobo M, Pinho T. Esthetic Perception of Different Clinical Situations of Maxillary Lateral Incisor Agenesis According to Populations with Dental and Non-Dental Backgrounds: A Systematic Review and Meta-Analysis. Dentistry Journal. 2023; 11(4):105. https://doi.org/10.3390/dj11040105
Chicago/Turabian StyleCalheiros-Lobo, Maria João, Mafalda Calheiros-Lobo, and Teresa Pinho. 2023. "Esthetic Perception of Different Clinical Situations of Maxillary Lateral Incisor Agenesis According to Populations with Dental and Non-Dental Backgrounds: A Systematic Review and Meta-Analysis" Dentistry Journal 11, no. 4: 105. https://doi.org/10.3390/dj11040105
APA StyleCalheiros-Lobo, M. J., Calheiros-Lobo, M., & Pinho, T. (2023). Esthetic Perception of Different Clinical Situations of Maxillary Lateral Incisor Agenesis According to Populations with Dental and Non-Dental Backgrounds: A Systematic Review and Meta-Analysis. Dentistry Journal, 11(4), 105. https://doi.org/10.3390/dj11040105