

Comparison between Magneto-Dynamic, Piezoelectric, and Conventional Surgery for Dental Extractions: A Pilot Study

 ,
, 
 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
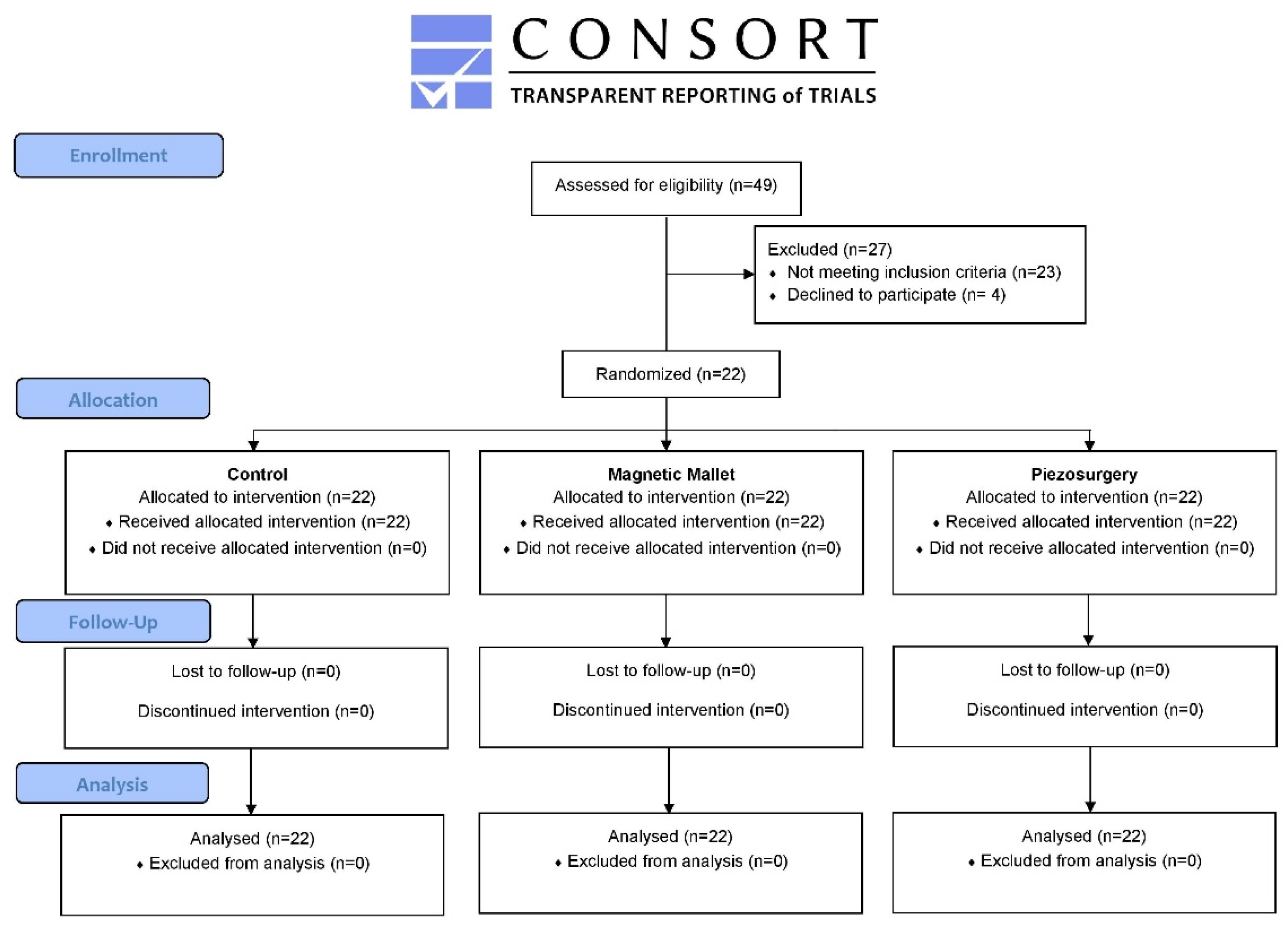
2.1. Study Design
2.2. Study Sample
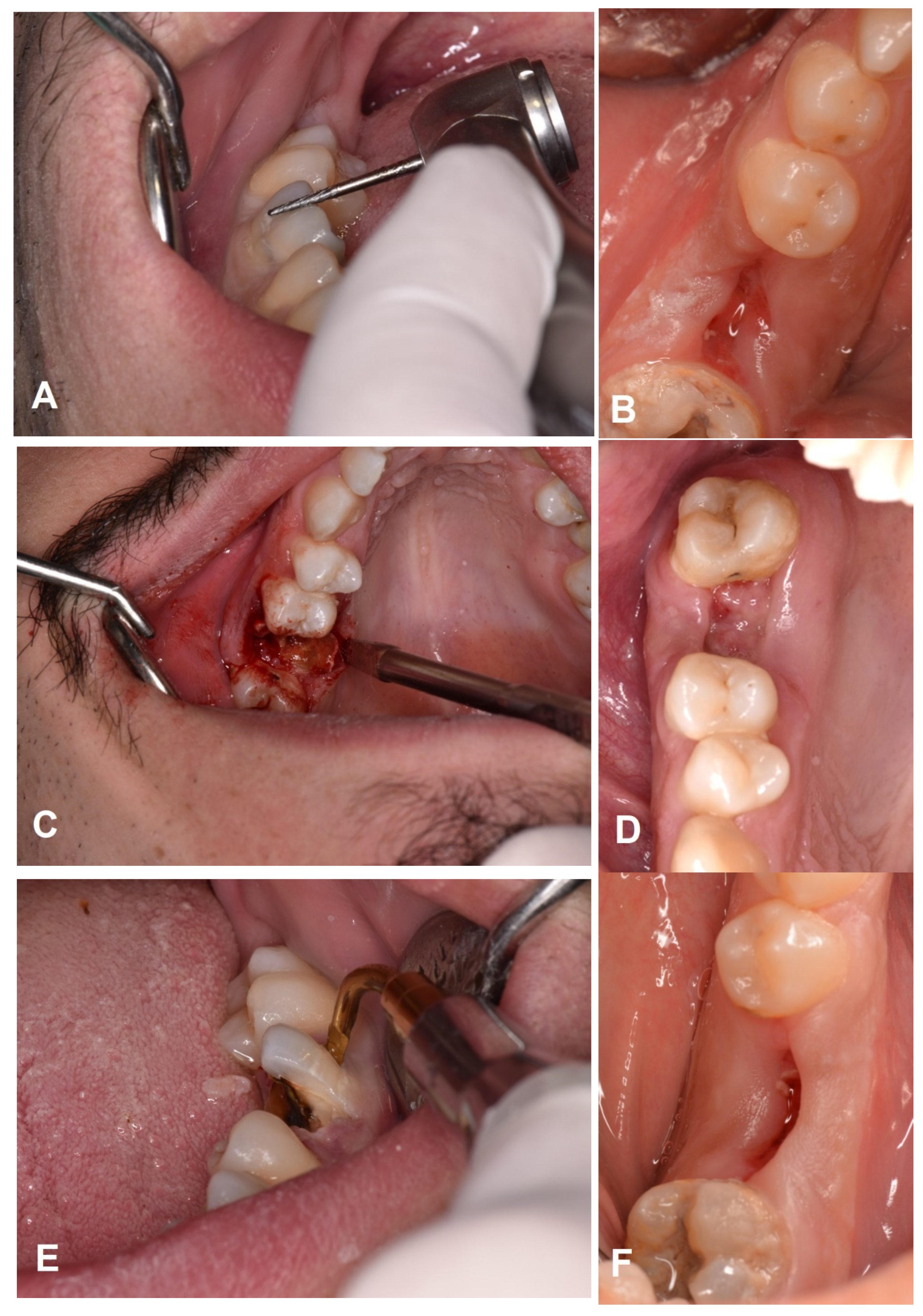
2.3. Procedure
2.4. Outcome Assessment
- Pain assessment
- Healing assessment
- Complete wound closure without the presence of fibrin;
- Complete wound closure with the presence of fibrin;
- Incomplete wound closure (dehiscence);
- Incomplete wound closure (necrosis).
- Time to complete each individual procedure (excluding suturing; measured in second);
- Any additional complication (oroantral communication, root fracture, bleeding, dry socket or alveolitis, abscess, fistula, nerve injury).
2.5. Data Collection, Processing, and Statistical Analysis
3. Results
3.1. Study Sample
3.2. Outcomes
3.3. Data Analysis
3.3.1. Pain Assessment
3.3.2. Healing Assessment
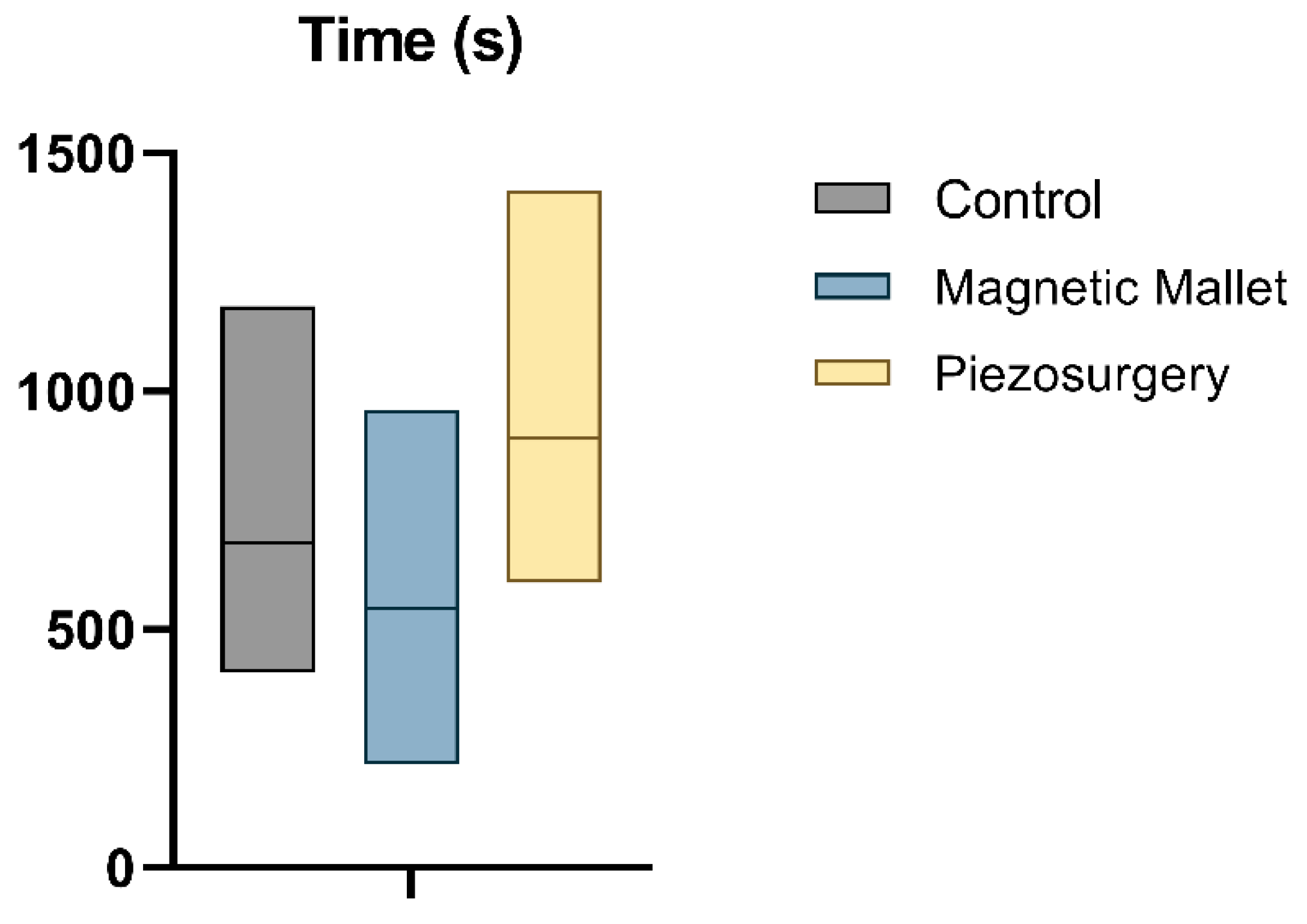
3.3.3. Time to Complete Each Individual Procedure
3.3.4. Any Additional Complication
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hong, B.; Bulsara, Y.; Gorecki, P.; Dietrich, T. Minimally invasive vertical versus conventional tooth extraction: An interrupted time series study. J. Am. Dent. Assoc. 2018, 149, 688–695. [Google Scholar] [CrossRef]
- Atieh, M.A.; Alsabeeha, N.H.M.; Tawse-Smith, A.; Duncan, W.J. Piezoelectric versus conventional implant site preparation: A systematic review and meta-analysis. Clin. Implant. Dent. Relat. Res. 2018, 20, 261–270. [Google Scholar] [CrossRef]
- Saund, D.; Dietrich, T. Minimally-invasive tooth extraction: Doorknobs and strings revisited! Dent. Update 2013, 40, 325–330. [Google Scholar] [CrossRef]
- Ergina, P.L.; Cook, J.; Blazeby, J.; Boutron, I.; Clavien, P.-A.; Reeves, B.C.; Seiler, C.M. Challenges in evaluating surgical innovation. Lancet 2009, 374, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- Bennardo, F.; Barone, S.; Vocaturo, C.; Nucci, L.; Antonelli, A.; Giudice, A. Usefulness of Magnetic Mallet in Oral Surgery and Implantology: A Systematic Review. J. Pers. Med. 2022, 12, 108. [Google Scholar] [CrossRef]
- Cai, Y.; Sun, R.; Zhao, J.H. Flapless boning to increase space by piezosurgery: A novel mini-invasive strategy for teeth extraction. A retrospective study. Medicine 2018, 97, e11398. [Google Scholar] [CrossRef] [PubMed]
- Vercellotti, T.; De Paoli, S.; Nevins, M. The piezoelectric bony window osteotomy and sinus membrane elevation: Introduction of a new technique for simplification of the sinus augmentation procedure. Int. J. Periodontics Restor. Dent. 2001, 21, 561–567. [Google Scholar]
- Vercellotti, T. Technological characteristics and clinical indications of piezoelectric bone surgery. Minerva Stomatol. 2004, 53, 207–214. [Google Scholar] [PubMed]
- Pandis, N.; Chung, B.; Scherer, R.W.; Elbourne, D.; Altman, D.G. CONSORT 2010 statement: Extension checklist for reporting within person randomised trials. BMJ 2017, 357, j2835. [Google Scholar] [CrossRef]
- SIDCO. Position statement su “appropriatezza in chirurgia estrattiva”: Criteri decisionali endodontici, restaurativi, parodontali. Available online: https://www.sidcoinforma.it/download/position.pdf (accessed on 15 September 2022).
- Giudice, A.; Esposito, M.; Bennardo, F.; Brancaccio, Y.; Buti, J.; Fortunato, L. Dental extractions for patients on oral antiplatelet: A within-person randomised controlled trial comparing haemostatic plugs, advanced-platelet-rich fibrin (A-PRF+) plugs, leukocyte- and platelet-rich fibrin (L-PRF) plugs and suturing alone. Int. J. Oral Implantol. 2019, 12, 77–87. [Google Scholar]
- Barone, S.; Antonelli, A.; Averta, F.; Diodati, F.; Muraca, D.; Bennardo, F.; Giudice, A. Does Mandibular Gonial Angle Influence the Eruption Pattern of the Lower Third Molar? A Three-Dimensional Study. J. Clin. Med. 2021, 10, 4057. [Google Scholar] [CrossRef]
- Sortino, F.; Pedullà, E.; Masoli, V. The piezoelectric and rotatory osteotomy technique in impacted third molar surgery: Comparison of postoperative recovery. J. Oral Maxillofac. Surg. 2008, 66, 2444–2448. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.J.; Chen, Y.L.; Chang, H.H.; Shyu, Y.C.; Lin, C.P. Effect of piezoelectric instruments on healing propensity of alveolar sockets following mandibular third molar extraction. J. Dent. Sci. 2012, 7, 296–300. [Google Scholar] [CrossRef]
- Vercellotti, T. Piezoelectric surgery in implantology: A case report—A new piezoelectric ridge expansion technique. Int. J. Periodontics Restor. Dent. 2000, 20, 358–365. [Google Scholar]
- Stacchi, C.; Berton, F.; Turco, G.; Franco, M.; Navarra, C.O.; Andolsek, F.; Maglione, M.; Di Lenarda, R. Micromorphometric analysis of bone blocks harvested with eight different ultrasonic and sonic devices for osseous surgery. J. Craniomaxillofac. Surg. 2016, 44, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, C.; Zhou, S.; Jiang, W.; Liu, Z.; Xu, L. A comparison review on orthopedic surgery using piezosurgery and conventional tools. Procedia Cirp. 2017, 65, 99–104. [Google Scholar] [CrossRef]
- Massimi, L.; Rapisarda, A.; Bianchi, F.; Frassanito, P.; Tamburrini, G.; Pelo, S.; Caldarelli, M. Piezosurgery in pediatric neurosurgery. World Neurosurg. 2019, 126, e625–e633. [Google Scholar] [CrossRef]
- Crosetti, E.; Battiston, B.; Succo, G. Piezosurgery in head and neck oncological and reconstructive surgery: Personal experience on 127 cases. Acta Otorhinolaryngol. Ital. 2009, 29, 1. [Google Scholar]
- Cicciù, M.; Stacchi, C.; Fiorillo, L.; Cervino, G.; Troiano, G.; Vercellotti, T.; Herford, A.S.; Galindo-Moreno, P.; Di Lenarda, R. Piezoelectric bone surgery for impacted lower third molar extraction compared with conventional rotary instruments: A systematic review, meta-analysis, and trial sequential analysis. Int. J. Oral Maxillofac. Surg. 2021, 50, 121–131. [Google Scholar] [CrossRef]
- Magesty, R.A.; Galvão, E.L.; de Castro Martins, C.; Dos Santos, C.R.R.; Falci, S.G.M. Rotary instrument or piezoelectric for the removal of third molars: A meta-analysis. J. Maxillofac. Oral Surg. 2017, 16, 13–21. [Google Scholar] [CrossRef]
- Ribeiro, F.V.; Hirata, D.Y.; Reis, A.F.; Santos, V.R.; Miranda, T.S.; Faveri, M.; Duarte, P.M. Open-flap versus flapless esthetic crown lengthening: 12-month clinical outcomes of a randomized controlled clinical trial. J. Periodontol. 2014, 85, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.; Patil, S.; Mitra, D.; Shah, R. Magnetic Mallet-Feel the Future. JIDA J. Indian Dent. Assoc. 2020, 14, 26–30. [Google Scholar] [CrossRef]
- Crespi, R.; Bruschi, G.B.; Gastaldi, G.; Capparé, P.; Gherlone, E.F. Immediate Loaded Implants in Split-Crest Procedure. Clin. Implant. Dent. Relat. Res. 2015, 17 (Suppl. S2), e692–e698. [Google Scholar] [CrossRef] [PubMed]
- Crespi, R.; Capparé, P.; Crespi, G.; Gastaldi, G.; Gherlone, E.F. Dimensional Changes of Fresh Sockets with Reactive Soft Tissue Preservation: A Cone Beam CT Study. Implant. Dent. 2017, 26, 417–422. [Google Scholar] [CrossRef]
- Menchini-Fabris, G.B.; Toti, P.; Crespi, G.; Covani, U.; Crespi, R. Distal Displacement of Maxillary Sinus Anterior Wall versus Conventional Sinus Lift with Lateral Access: A 3-Year Retrospective Computerized Tomography Study. Int. J. Environ. Res. Public Health 2020, 17, 7199. [Google Scholar] [CrossRef]
- Crespi, R.; Bruschi, G.B.; Capparé, P.; Gherlone, E. The utility of the electric mallet. J. Craniofac. Surg. 2014, 25, 793–795. [Google Scholar] [CrossRef]
- Crespi, R.; Capparé, P.; Crespi, G.; Gastaldi, G.; Gherlone, E. Bone-Level Changes around Delayed Dental Implants in Previous Large Bone Defects Filled with Reactive Soft Tissue After Extraction: A Cone Beam Computed Tomography Study. Int. J. Oral Maxillofac. Implant. 2016, 31, 1429–1434. [Google Scholar] [CrossRef]
- Bakkar, M.; Liu, Y.; Fang, D.; Stegen, C.; Su, X.; Ramamoorthi, M.; Lin, L.-C.; Kawasaki, T.; Makhoul, N.; Pham, H.; et al. A Simplified and Systematic Method to Isolate, Culture, and Characterize Multiple Types of Human Dental Stem Cells from a Single Tooth. Methods Mol. Biol. 2017, 1553, 191–207. [Google Scholar]
- Di Vito, A.; Giudice, A.; Chiarella, E.; Malara, N.; Bennardo, F.; Fortunato, L. In Vitro Long-Term Expansion and High Osteogenic Potential of Periodontal Ligament Stem Cells: More Than a Mirage. Cell Transpl. 2019, 28, 129–139. [Google Scholar] [CrossRef]
- Schierano, G.; Baldi, D.; Peirone, B.; Mauthe von Degerfeld, M.; Navone, R.; Bragoni, A.; Colombo, J.; Autelli, R.; Muzio, G. Biomolecular, Histological, Clinical, and Radiological Analyses of Dental Implant Bone Sites Prepared Using Magnetic Mallet Technology: A Pilot Study in Animals. Materials 2021, 14, 6945. [Google Scholar] [CrossRef]
- Feher, B.; Frommlet, F.; Gruber, R.; Hirtler, L.; Ulm, C.; Kuchler, U. Resonance frequency analysis of implants placed in condensed bone. Clin. Oral Implant. Res. 2021, 32, 1200–1208. [Google Scholar] [CrossRef] [PubMed]
- Giudice, A.; Bennardo, F.; Antonelli, A.; Barone, S.; Fortunato, L. COVID-19 is a New Challenge for Dental Practitioners: Advice on Patients’ Management from Prevention of Cross Infections to Telemedicine. Open Dent. J. 2020, 14, 298–304. [Google Scholar] [CrossRef]
- Giudice, A.; Antonelli, A.; Bennardo, F. To test or not to test? An opportunity to restart dentistry sustainably in the ‘COVID-19 era’. Int. Endod. J. 2020, 53, 1020–1021. [Google Scholar] [CrossRef] [PubMed]
- Bennardo, F.; Antonelli, A.; Barone, S.; Figliuzzi, M.M.; Fortunato, L.; Giudice, A. Change of Outpatient Oral Surgery during the COVID-19 Pandemic: Experience of an Italian Center. Int. J. Dent. 2020, 2020, 8893423. [Google Scholar] [CrossRef] [PubMed]
- Chien, A.T.; Stehle, N.E.; Karian, B.K. The Use of Chisels in the Extraction of Mandibular Third Molars: A Technique That May Prevent the Aerosolization of Severe Acute Respiratory Syndrome Coronavirus 2. J. Oral Maxillofac. Surg. 2021, 79, 1199–1206. [Google Scholar] [CrossRef]
- Franchignoni, F.; Salaffi, F.; Tesio, L. How should we use the visual analogue scale (VAS) in rehabilitation outcomes? I: How much of what? The seductive VAS numbers are not true measures. J. Rehabil. Med. 2012, 44, 798–799. [Google Scholar] [CrossRef]
- Devlin, H.; Horner, K.; Ledgerton, D. A comparison of maxillary and mandibular bone mineral densities. J. Prosthet. Dent. 1998, 79, 323–327. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Arm | Treatment |
|---|---|
| Control (C) | Periotomes to remove PDL fibers Contra-angle handpiece/turbine with surgical burs to remove periradicular bone Elevators and extraction forceps for luxation |
| Magnetic Mallet (M) | Magnetic Mallet® handpiece with dedicated tips (EXTR 1, EXTR 2, EXTR 3, EXTR 4, EXTR 5; Osseotouch, Gallarate, VA, Italy) for removing PDL fibers, periradicular bone, and luxation |
| Piezosurgery (P) | Piezosurgery® handpiece with dedicated ultrasonic tips (EX 1, EX 2, EX 3; Mectron, Carasco, GE, Italy) to remove periodontal ligament fibers and periradicular bone Elevators and extraction forceps for luxation |
| Subgroups | Extracted Teeth | Control (n = 22) | Magnetic Mallet (n = 22) | Piezosurgery (n = 22) |
|---|---|---|---|---|
| Single-rooted (5 patients) | Incisors | 3 Mandible 1, Maxilla 2 | 3 Mandible 2, Maxilla 1 | 4 Mandible 2, Maxilla 2 |
| Canines | 2 Mandible 1, Maxilla 1 | 2 Mandible 1, Maxilla 1 | 1 Mandible -, Maxilla 1 | |
| Multi-rooted (17 patients) | Premolars | 9 Mandible 4, Maxilla 5 | 8 Mandible 3, Maxilla 5 | 7 Mandible 4, Maxilla 3 |
| Molars | 8 Mandible 4, Maxilla 4 | 9 Mandible 3, Maxilla 5 | 10 Mandible 6, Maxilla 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bennardo, F.; Barone, S.; Vocaturo, C.; Gheorghe, D.N.; Cosentini, G.; Antonelli, A.; Giudice, A. Comparison between Magneto-Dynamic, Piezoelectric, and Conventional Surgery for Dental Extractions: A Pilot Study. Dent. J. 2023, 11, 60. https://doi.org/10.3390/dj11030060
Bennardo F, Barone S, Vocaturo C, Gheorghe DN, Cosentini G, Antonelli A, Giudice A. Comparison between Magneto-Dynamic, Piezoelectric, and Conventional Surgery for Dental Extractions: A Pilot Study. Dentistry Journal. 2023; 11(3):60. https://doi.org/10.3390/dj11030060
Chicago/Turabian StyleBennardo, Francesco, Selene Barone, Camillo Vocaturo, Dorin Nicolae Gheorghe, Giorgio Cosentini, Alessandro Antonelli, and Amerigo Giudice. 2023. "Comparison between Magneto-Dynamic, Piezoelectric, and Conventional Surgery for Dental Extractions: A Pilot Study" Dentistry Journal 11, no. 3: 60. https://doi.org/10.3390/dj11030060
APA StyleBennardo, F., Barone, S., Vocaturo, C., Gheorghe, D. N., Cosentini, G., Antonelli, A., & Giudice, A. (2023). Comparison between Magneto-Dynamic, Piezoelectric, and Conventional Surgery for Dental Extractions: A Pilot Study. Dentistry Journal, 11(3), 60. https://doi.org/10.3390/dj11030060