
A Case of Adult-Onset Eccrine Angiomatous Hamartoma—The Comparison with Epithelioid Hemangioma

 ,
,
Abstract
:1. Introduction
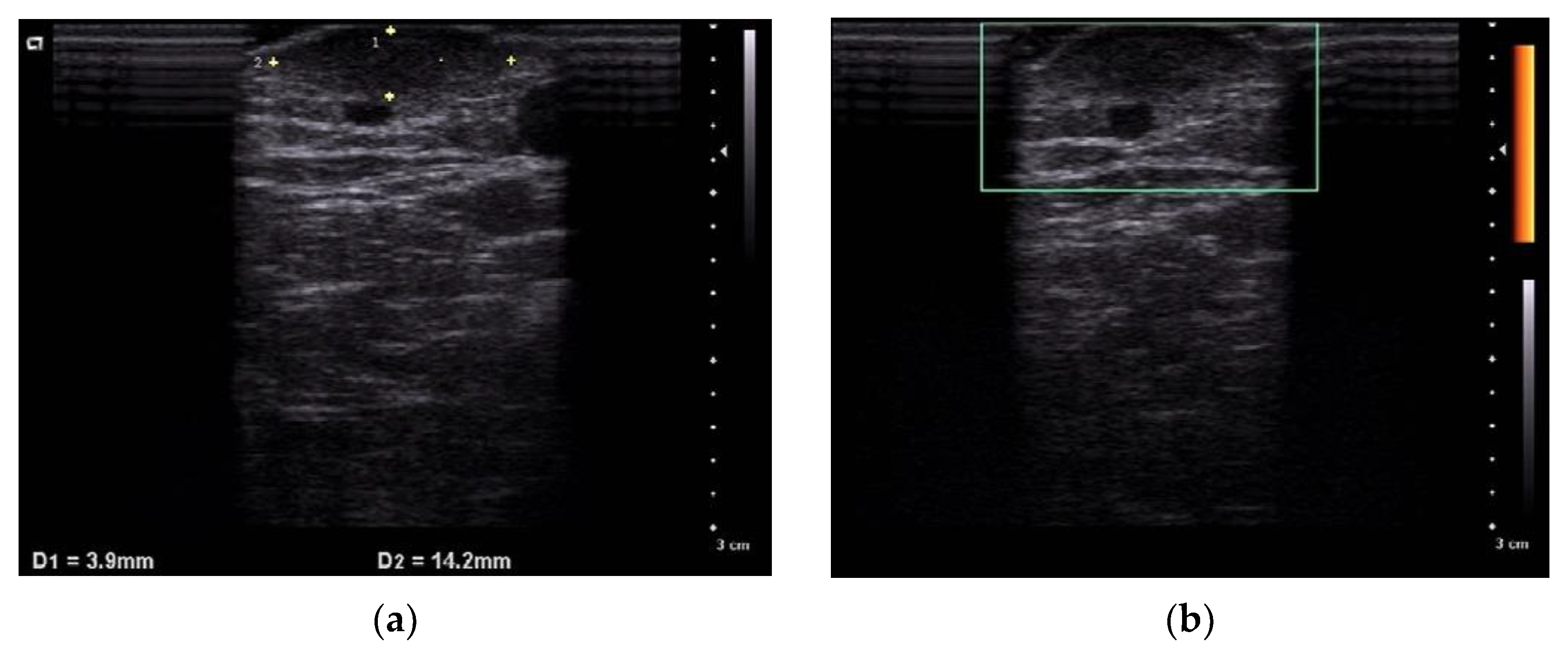
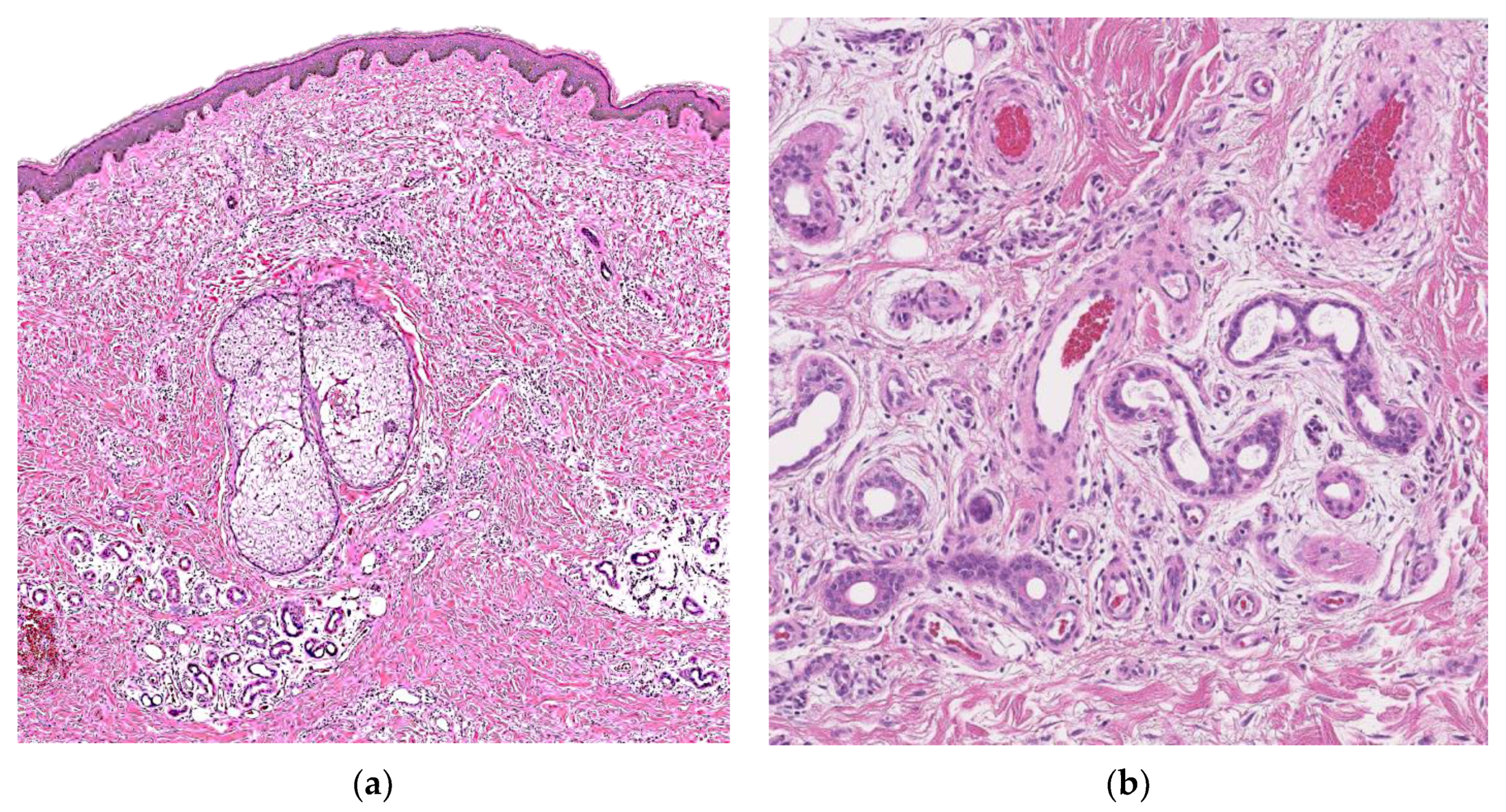
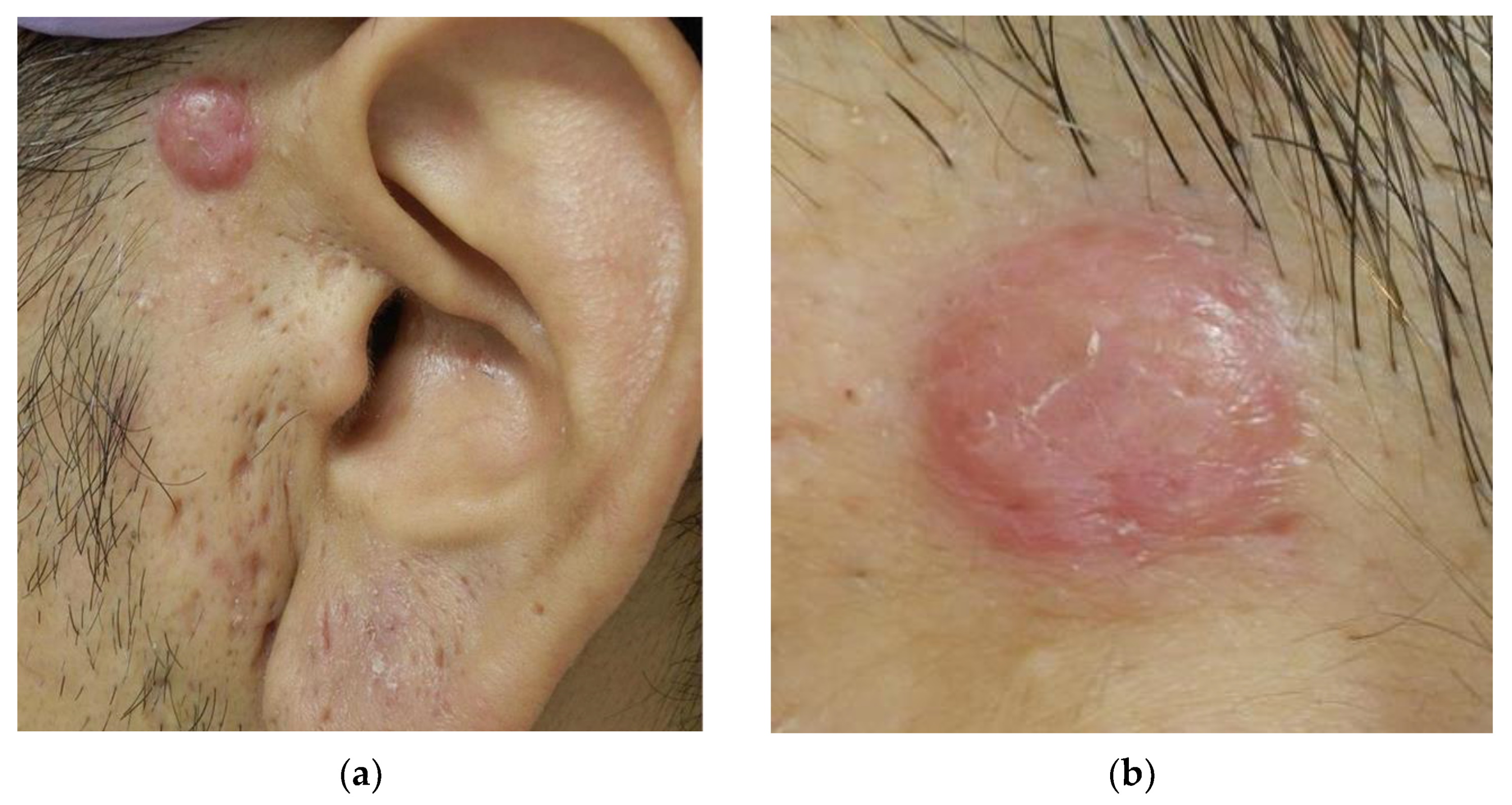
2. Case Report
2.1. Case 1
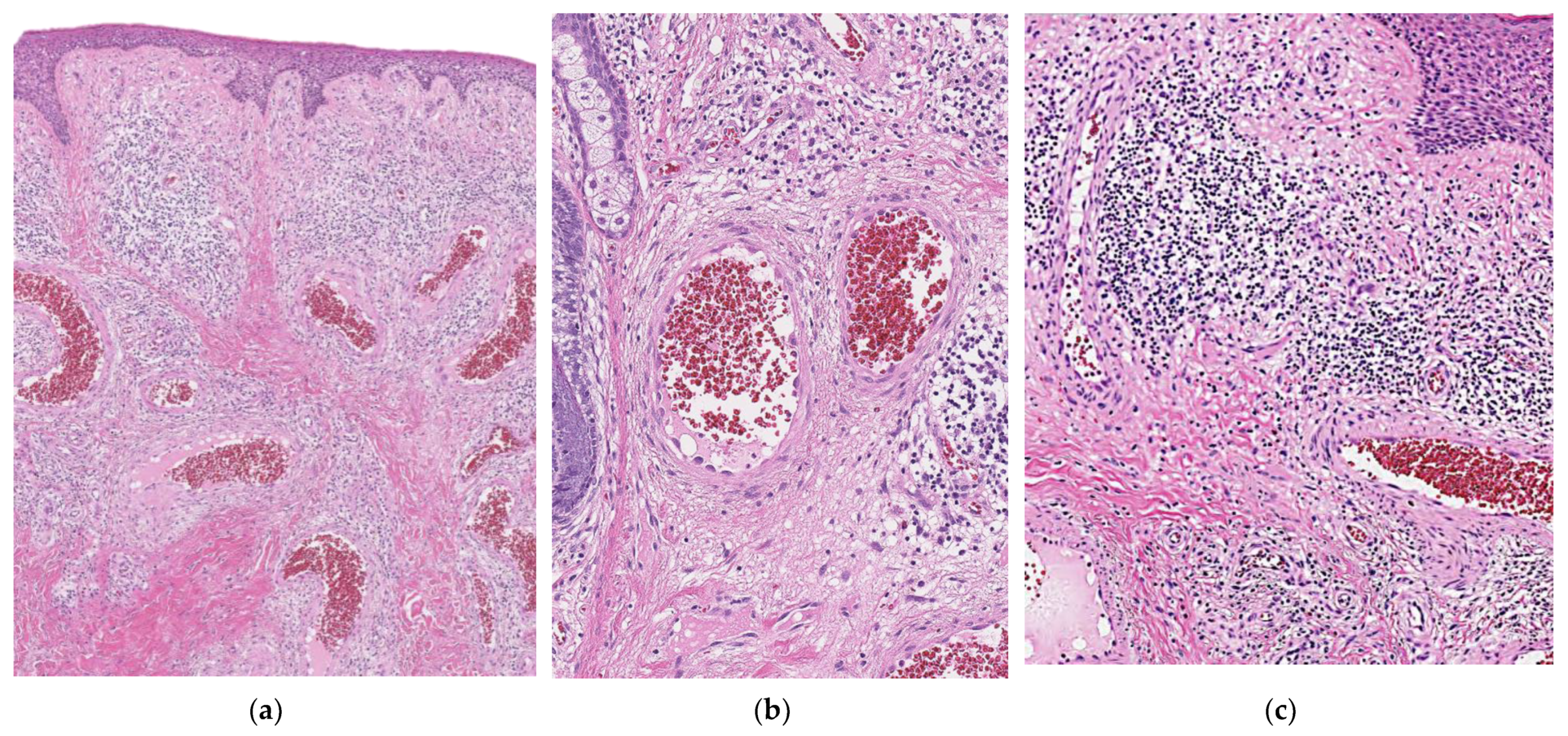
2.2. Case 2
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lotzbeck, C. A case of sweat gland tumor on cheek. Virchows Arch. 1859, 16, 160. [Google Scholar] [CrossRef] [Green Version]
- Hyman, A.B.; Harris, H.; Brownstein, M.H. Eccrine angiomatous hamartoma. N. Y. State J. Med. 1968, 68, 2803–2806. [Google Scholar] [PubMed]
- Yoshida, M.N.T.; Kawata, A. A case of eccrine angiomatous hamartoma. JJCD 2013, 67, 689–692. [Google Scholar]
- Naik, V.; Arsenovic, N.; Reed, M. Eccrine angiomatous hamartoma: A rare multifocal variant with features suggesting trauma. Dermatol. Online J. 2009, 15, 6. [Google Scholar] [CrossRef]
- Hawryluk, E.B.; Schmidt, B.; Maguiness, S. Enlargement of eccrine angiomatous hamartoma following trauma. Pediatr. Dermatol. 2015, 32, e92–e94. [Google Scholar] [CrossRef]
- Gadroy, A.; Belhadjali, H.; Bayle, P.; Albes, B.; Lamant, L.; Bazex, J. Eccrine angiomatous hamartoma: An atypical case. Ann. Dermatol. Venereol. 2003, 130, 337–339. [Google Scholar] [PubMed]
- Pelle, M.T.; Pride, H.B.; Tyler, W.B. Eccrine angiomatous hamartoma. J. Am. Acad. Dermatol. 2002, 47, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Cebreiro, C.; Sanchez-Aguilar, D.; Gomez Centeno, P.; Fernandez-Redondo, V.; Toribio, J. Eccrine angiomatous hamartoma: Report of seven cases. Clin. Exp. Dermatol. 1998, 23, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Arpa, M.; Rodriguez-Vazquez, M.; Cortina-de la Calle, P.; Romero-Aguilera, G.; Lopez-Perez, R. Multiple and familial eccrine angiomatous hamartoma. Acta Derm. Venereol. 2005, 85, 355–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fetsch, J.F.; Weiss, S.W. Observations concerning the pathogenesis of epithelioid hemangioma (angiolymphoid hyperplasia). Mod. Pathol. 1991, 4, 449–455. [Google Scholar]
- Sun, Z.J.; Zhang, L.; Zhang, W.F.; Alsharif, M.J.; Chen, X.M.; Zhao, Y.F. Epithelioid hemangioma in the oral mucosa: A clinicopathological study of seven cases and review of the literature. Oral. Oncol. 2006, 42, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Apte, A.; Nema, P.; Bandi, A. Eccrine angiokeratomatous hamartoma: Case report of a 1.5-year girl. J. Surg. Case Rep. 2017, 2017, rjx133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chien, J.A.; Asgari, M.; Argenyi, B.Z. Eccrine angiomatous hamartoma with elements of an arteriovenous malformation: A newly recognized variant. J. Cutan. Pathol. 2006, 33, 433–436. [Google Scholar] [CrossRef] [PubMed]
- Tjarks, J.S.C.S. Tufted Tumors. Available online: https://www.pathologyoutlines.com/topic/skintumornonmelanocyticacquiredangioma.html (accessed on 10 March 2021).
- Raboudi, A.L.N. Congenital Smooth Muscle Hamartoma. Available online: https://www.ncbi.nlm.nih.gov/books/NBK545188/ (accessed on 24 March 2021).
- Ladha, A.M.; Remington, T. Acquired smooth muscle hamartoma: A case report on the lower extremity hidrosis. SAGE Open Med. Case Rep. 2019, 7, 2050313X19893834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baigrie, D.R.S.A. Blue Bubber Bleb Nevus Syndrome. Available online: https://www.ncbi.nlm.nih.gov/books/NBK541085/ (accessed on 10 March 2021).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Number of Cases Reported in English | Histopathological Finding | Reference |
|---|---|---|---|
| EAH | <100 | the lesion affects mainly mid and deep dermis and is composed of lobules of proliferating capillaries intricately admixed with sweat glands and ducts, fat and myxoid tissue. | [12] |
| Eccrine nevus | 20 | It is characterized by groupings of normal to enlarged eccrine structures. (The absence of angiomatous hyperplasia) | [13] |
| Tufted angioma | 200 | multiple, scattered lobules of small capillary type vessels with small oval to spindle shaped cells throughout the dermis and subcutaneous tissue imparting a “cannonball” or glomerular appearance. | [14] |
| Smooth muscle hamartoma | <20 (Only acquired type) | It shows disseminated proliferation of mature smooth muscle cells of a central cigar-shaped nucleus and fibrillary and eosinophilic cytoplasm. | [15,16] |
| Blue rubber bleb nevus syndrome | 200 | cutaneous lesions are non-specific and have features of venous malformations. Large, tortuous, dilated vessels with a single endothelial lining are noted, and smooth muscle may be present in the vessel walls. | [17] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishimura, M.; Matsushima, Y.; Nakai, Y.; Habe, K.; Hayashi, A.; Yamanaka, K. A Case of Adult-Onset Eccrine Angiomatous Hamartoma—The Comparison with Epithelioid Hemangioma. Dermatopathology 2022, 9, 94-99. https://doi.org/10.3390/dermatopathology9020012
Nishimura M, Matsushima Y, Nakai Y, Habe K, Hayashi A, Yamanaka K. A Case of Adult-Onset Eccrine Angiomatous Hamartoma—The Comparison with Epithelioid Hemangioma. Dermatopathology. 2022; 9(2):94-99. https://doi.org/10.3390/dermatopathology9020012
Chicago/Turabian StyleNishimura, Mai, Yoshiaki Matsushima, Yasuo Nakai, Koji Habe, Akinobu Hayashi, and Keiichi Yamanaka. 2022. "A Case of Adult-Onset Eccrine Angiomatous Hamartoma—The Comparison with Epithelioid Hemangioma" Dermatopathology 9, no. 2: 94-99. https://doi.org/10.3390/dermatopathology9020012
APA StyleNishimura, M., Matsushima, Y., Nakai, Y., Habe, K., Hayashi, A., & Yamanaka, K. (2022). A Case of Adult-Onset Eccrine Angiomatous Hamartoma—The Comparison with Epithelioid Hemangioma. Dermatopathology, 9(2), 94-99. https://doi.org/10.3390/dermatopathology9020012