
Plaque-Like Dermatofibroma: Case Report of a Rare Entity


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
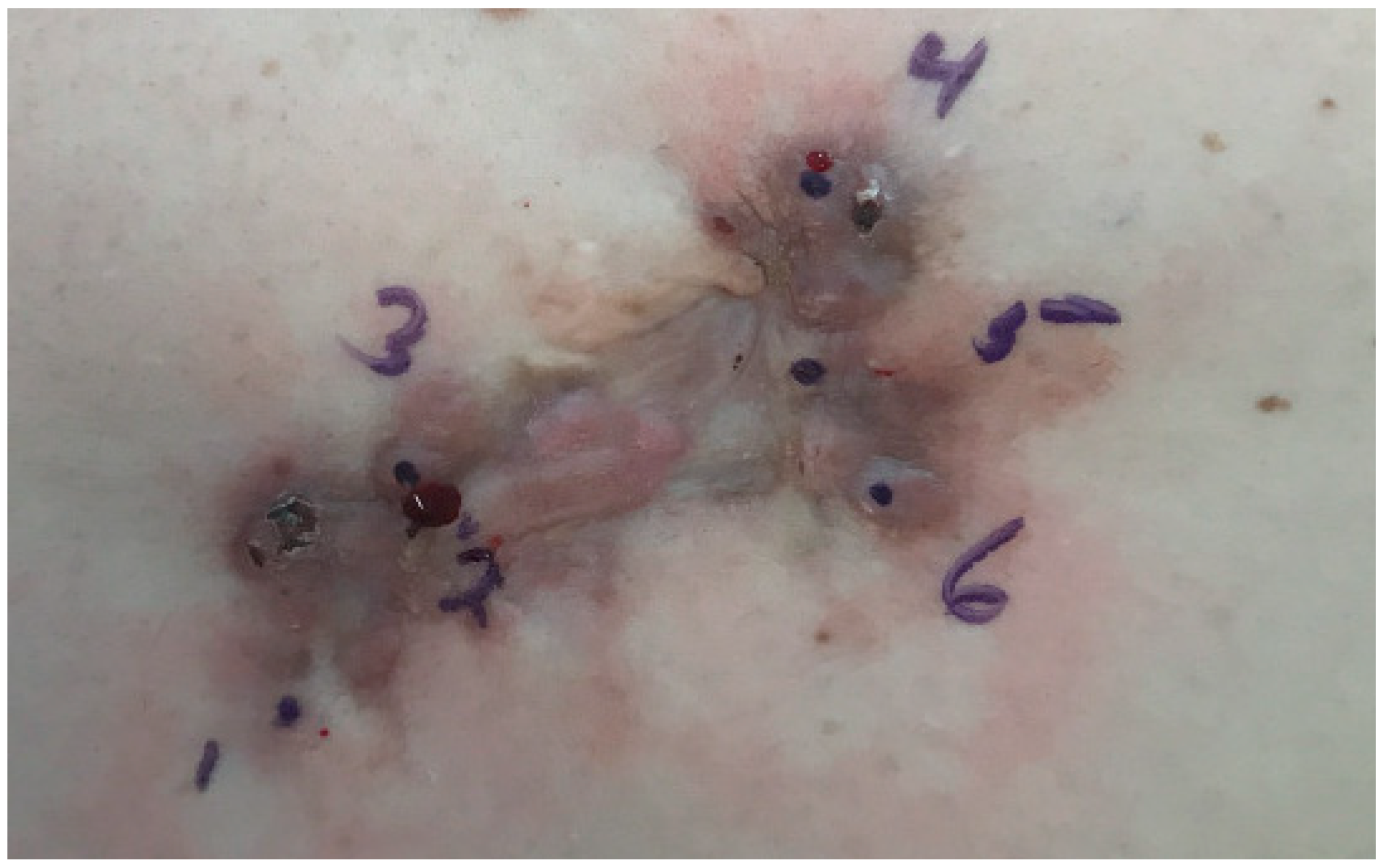
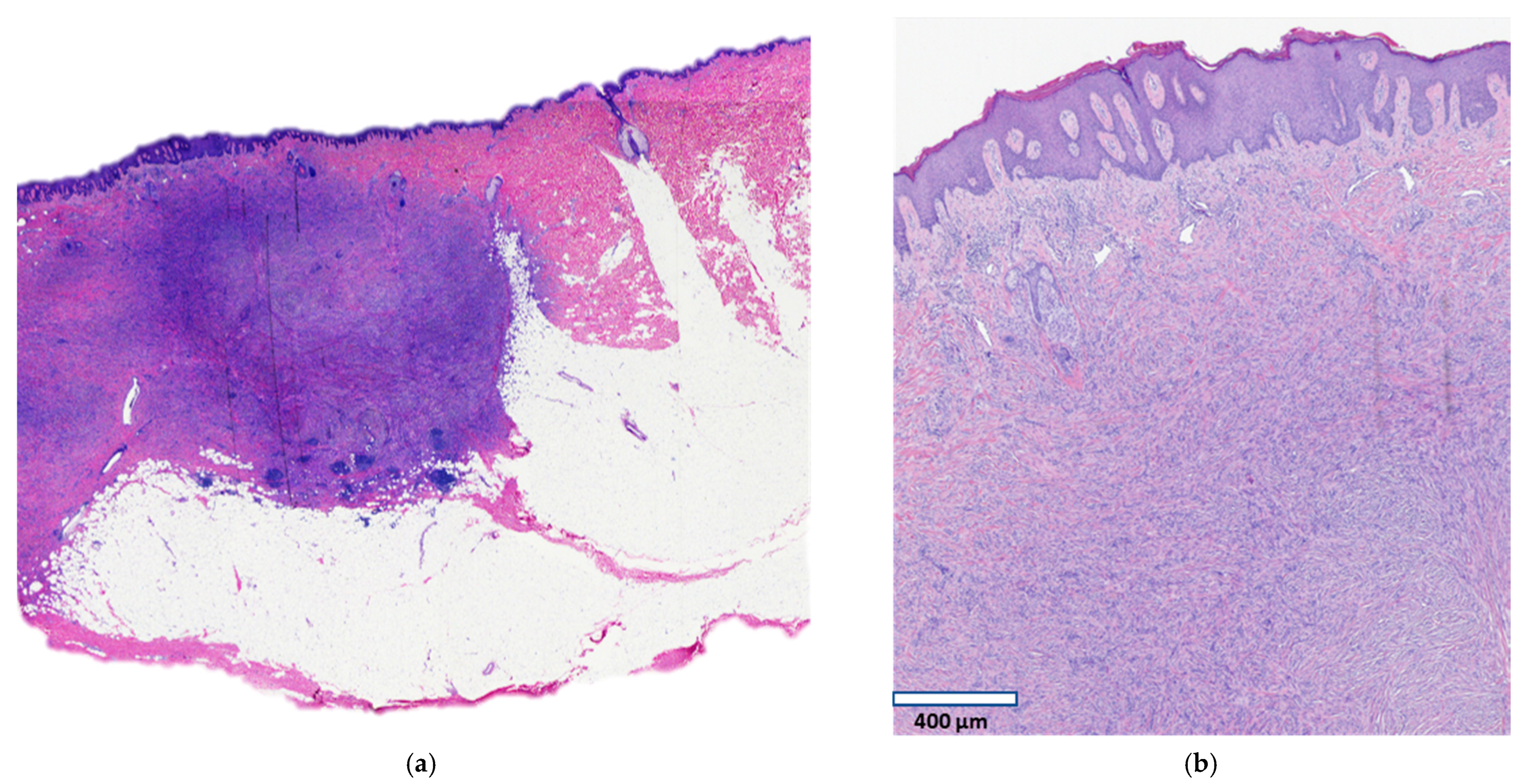
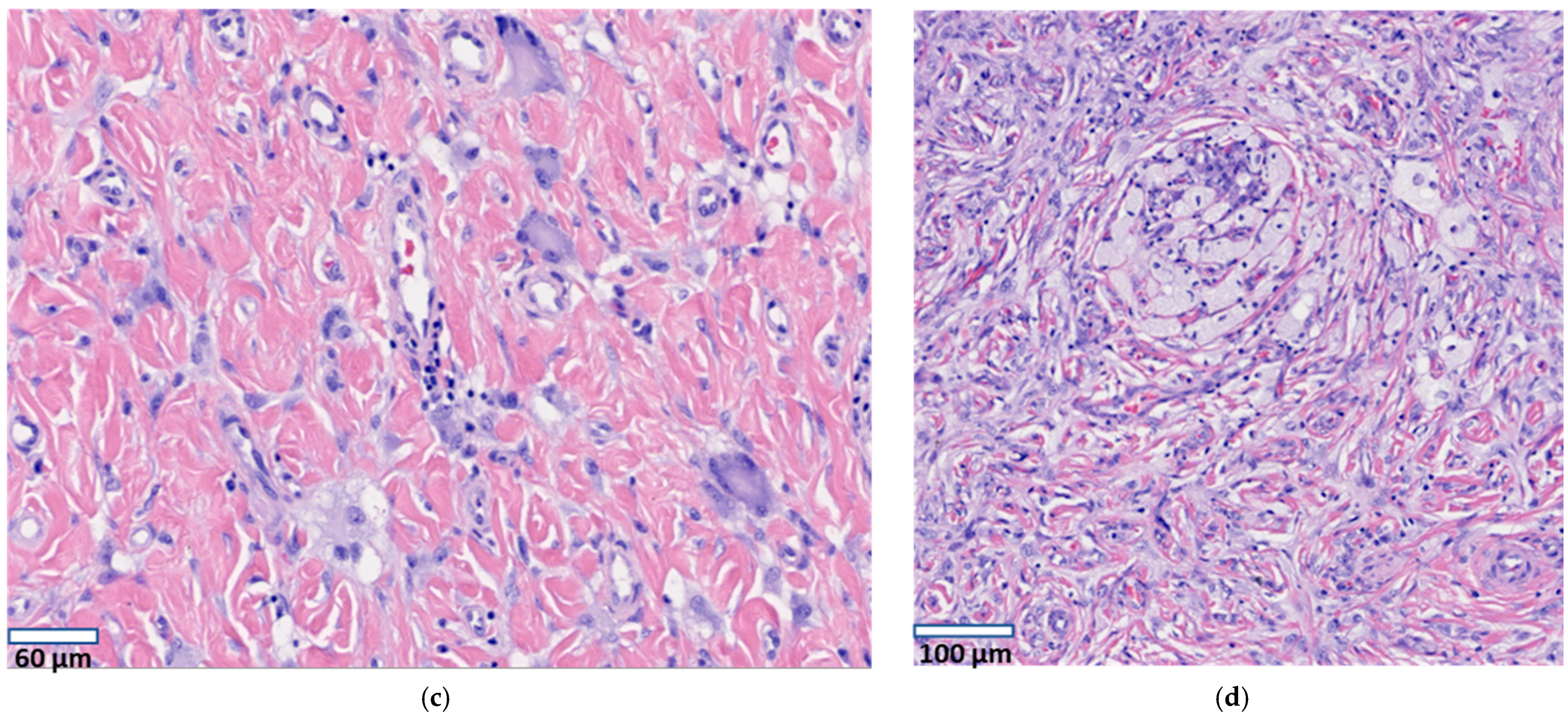
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Requena, L.; Fariña, M.C.; Fuente, C.; Piqué, E.; Olivares, M.; Martín, L.; Yus, E.S. Giant dermatofibroma. A little-known clinical variant of dermatofibroma. J. Am. Acad. Dermatol. 1994, 30, 714–718. [Google Scholar] [CrossRef]
- Panicker, V.V.; Dharmaratnam, A.D.; Seethalekshmy, N.V. Plaque-like giant dermatofibroma: A case report. J. Cutan. Aesthet. Surg. 2017, 10, 51–53. [Google Scholar] [CrossRef] [PubMed]
- Micantonio, T.; Fargnoli, M.C.; Peris, K. Giant Dermatofibroma Appearing During Pregnancy. Acta Derm. Venereol. 2005, 86, 86–87. [Google Scholar] [CrossRef] [PubMed]
- Leow, L.J.; Sinclair, P.A.; Horton, J.J. Plaque-like dermatofibroma: A distinct and rare benign neoplasm? Australas. J. Dermatol. 2008, 49, 106–108. [Google Scholar] [CrossRef]
- Lozano Masdemont, B.; Campos Domínguez, M.; Gómez-Recuero Muñoz, L.; Bergón Sendín, M.; Parra Blanco, V.; Suárez Fer-nández, R. Multiple clustered dermatofibroma: A rare variant of plaque-like dermatofibroma. G Ital. Dermatol. Venereol. 2016, 151, 718–720. [Google Scholar]
- Findeis, S.; Lynch, M.C.; Sceppa, J.; Helm, K.F. Plaque-like dermatofibroma with satellitosis. Dermatol. Surg. 2017, 43, 139–142. [Google Scholar] [CrossRef]
- Avila, C.; Lause, M.; McIntyre, M., 2nd; Rzepka, P.V.; Chung, C.; Trinidad, J. Plaque-like dermatofibroma with satellitosis in a young woman. Int. J. Dermatol. 2019, 58, 1199–1201. [Google Scholar] [CrossRef]
- Shaheen, B.; Saldanha, G.; Calonje, E.; Johnston, G.A. Multiple clustered dermatofibromas (fibrous histiocytomas): An atypical clinical variant of dermatofibroma. Clin. Exp. Dermatol. 2013, 39, 88–90. [Google Scholar] [CrossRef]
- Higaki-Mori, H.; Yoshida, Y.; Hisaoka, M.; Nishigori, C.; Shindo, M.; Yamamoto, O. Unusual Congenital Multiple Clustered Dermatofibroma: First Reported Case on the Face. Acta Derm. Venereol. 2019, 99, 341–342. [Google Scholar] [CrossRef]
- Finch, J.; Berke, A.; McCusker, M.; Chang, M.W. Congenital multiple clustered dermatofibroma in a 12-year-old girl. Pediatr. Dermatol. 2014, 31, 105–117. [Google Scholar] [CrossRef]
- Gershtenson, P.C.; Krunic, A.L.; Chen, H.M. Multiple clustered dermatofibroma: Case report and review of the literature. J. Cutan. Pathol. 2009, 37, e42–e45. [Google Scholar] [CrossRef]
- Soon, S.L.; Howard, A.K.; Washington, C.V. Multiple, clustered dermatofibroma: A rare clinical variant of dermatofibroma. J. Cutan. Med. Surg. 2003, 7, 455–457. [Google Scholar] [CrossRef]
- Berbis, P.; Benderitter, T.; Perier, C.; Frey, J.; Privat, Y. Multiple Clustered Dermatofibromas. Dermatology 1988, 177, 185–188. [Google Scholar] [CrossRef]
- De Unamono, P.; Carames, Y.; Fernandez-Lopez, E.; Hernández-Martín, A.; Peña, C. Congenital multiple clustered dermatofibroma. Br. J. Dermatol. 2000, 142, 1040–1043. [Google Scholar] [CrossRef]
- Pinto-Almeida, T.; Caetano, M.; Alves, R.; Selores, M. Congenital multiple clustered dermatofibroma and multiple eruptive dermatofibromas—Unusual presentations of a common entity*. Anais Brasileiros de Dermatologia 2013, 88, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Espiñeira-Carmona, M.J.; Salazar-Nievas, M.; Girón-Prieto, M.S.; Aneiros-Fernández, J.; Buendía-Eisman, A.; Arias-Santiago, S.A. Multiple clustered dermatofibromas. Eur. J. Dermatol. 2013, 23, 270–272. [Google Scholar] [CrossRef]
- Sanli, H.; Akay, B.N.; Heper, A.O. Congenital multiple clustered dermatofibroma: Dermatoscopic findings. Eur. J. Dermatol. 2009, 19, 653. [Google Scholar] [CrossRef] [PubMed]
- Mitri, F.; Haenssle, H.; Enk, A.; Toberer, F. Congenital multiple clustered dermatofibroma on the abdomen. Br. J. Dermatol. 2020, 183, e64. [Google Scholar] [CrossRef]
- Reynolds, H.; Perry, A.; Satter, E.K. Multiple clustered and focally atrophic dermatofibromas (DF). Dermatol. Online J. 2014, 20. [Google Scholar] [CrossRef]
- Veraldi, S.; Bocor, M.; Gianotti, R.; Gasparini, G. Multiple Eruptive Dermatofibromas Localized Exclusively to the Buttock. Int. J. Dermatol. 1991, 30, 507–508. [Google Scholar] [CrossRef]
- Komforti, M.; Jewell, J.; Pavlis, M. Multiple Clustered Dermatofibromas Associated with Pulmonary Arterial Hypertension. Am. J. Dermatopathol. 2016, 38, e30–e32. [Google Scholar] [CrossRef]
- Rognstad, Ø.B.; Haas, N.; Sterry, W.; Astner, S. Multiple clustered dermatofibroma with overlying sebaceous hyperplasia. J. Dtsch. Dermatol. Ges. 2009, 7, 962–964. [Google Scholar] [CrossRef]
- Clarke, J.T.; Clarke, L.E.; Miller, C.; Helm, K.F.; Zaenglein, A.L. Plaque-like myofibroblastic tumor of infancy. Pediatr. Dermatol. 2007, 24, e83–e87. [Google Scholar] [CrossRef] [PubMed]
- Moulonguet, I.; Biaggi, A.; Eschard, C.; Durlach, A.; Stock, N.; Delanoé, P.; Coussirat-Voreaux, M.-F.; Fraitag, S. Plaque-Like Myofibroblastic Tumor: Report of 4 Cases. Am. J. Dermatopathol. 2017, 39, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Marqueling, A.L.; Dasher, D.; Friedlander, S.F.; McCalmont, T.H.; Frieden, I.J. Plaque-Like Myofibroblastic Tumor: Report of Three Cases. Pediatr. Dermatol. 2013, 30, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Berklite, L.; Ranganathan, S.; John, I.; Picarsic, J.; Santoro, L.; Alaggio, R. Fibrous histiocytoma/dermatofibroma in children: The same as adults? Hum. Pathol. 2020, 99, 107–115. [Google Scholar] [CrossRef]
- Caldarola, G.; Bisceglia, M.; Pellicano, R. Multiple eruptive plaque-like dermatofibromas during anti-TNFα treatment. Int. J. Dermatol. 2012, 52, 638–641. [Google Scholar] [CrossRef]
- Viseux, V.; Chaby, G.; Agbalika, F.; Luong, M.; Chatelain, D.; Westeel, P.-F.; Denoeux, J.; Lok, C. Multiple Clustered Dermatofibromas on a Superficial Venous Thrombosis in a Kidney-Transplanted Patient. Dermatology 2004, 209, 156–157. [Google Scholar] [CrossRef]
- Ruiz-Villaverde, R.; Diaz-Martinez, M.A.; Sancez-Cano, D. Multiple clustered dermatofibromas following Ustekimumab treatment for psoriasis vulgaris. Sultan Qaboos Univ. Med. J. 2017, 17, e375–e377. [Google Scholar] [CrossRef]
- Bhabha, F.K.; Magee, J.; Ng, S.Y.; Grills, C.E.; Su, J.; Orchard, D. Multiple clustered dermatofibroma presenting in a segmental distribution. Australas. J. Dermatol. 2014, 57, e20–e22. [Google Scholar] [CrossRef]
- Katsuoka, K.; Happle, R.; Hoffmann, R.; Niiyama, S. Multiple eruptive dermatofibromas: A review of the literature. Acta Derm. Venereol. 2002, 82, 241–244. [Google Scholar] [CrossRef]
- Beatrous, S.V.; Riahi, R.R.; Grisoli, S.B.; Cohen, P.R. Associated conditions in patients with multiple dermatofibromas: Case reports and literature review. Dermatol. Online J. 2017, 23. [Google Scholar] [CrossRef]
- Płaszczyca, A.; Nilsson, J.; Magnusson, L.; Brosjö, O.; Larsson, O.; von Steyern, F.V.; Domanski, H.; Lilljebjörn, H.; Fioretos, T.; Tayebwa, J.; et al. Fusions involving protein kinase C and membrane-associated proteins in benign fibrous histiocytoma. Int. J. Biochem. Cell Biol. 2014, 53, 475–481. [Google Scholar] [CrossRef]
- Walther, C.; Hofvander, J.; Nilsson, J.; Magnusson, L.; Domanski, H.A.; Gisselsson, D.; Tayebwa, J.; Doyle, L.A.; Fletcher, C.D.M.; Mertens, F. Gene fusion detection in formalin-fixed paraffin-embedded benign fibrous histiocytomas using fluorescence in situ hybridization and RNA sequencing. Lab. Investig. 2015, 95, 1071–1076. [Google Scholar] [CrossRef]
- Ishigami, T.; Hida, Y.; Matsudate, Y.; Murao, K.; Kubo, Y. The involvement of fibroblast growth factor receptor signaling pathways in dermatofibroma and dermatofibrosarcoma protuberans. J. Med. Investig. 2013, 60, 106–113. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hafner, C.; Hartmann, A.; Van Oers, J.M.M.; Stoehr, R.; Zwarthoff, E.C.; Hofstaedter, F.; Landthaler, M.; Vogt, T. FGFR3 mutations in seborrheic keratoses are already present in flat lesions and associated with age and localization. Mod. Pathol. 2007, 20, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, D.; Gao, J.; Phillips, S.M.; Kundra, R.; Zhang, H.; Wang, J.; Rudolph, J.E.; Yaeger, R.; Soumerai, T.; Nissan, M.H.; et al. OncoKB: A Precision Oncology Knowledge Base. JCO Precis. Oncol. 2017, 1, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.-Y.; Zheng, H.; Du, X.-L.; Yang, J.-L. Characterization of FGFR signaling pathway as therapeutic targets for sarcoma patients. Cancer Biol. Med. 2016, 13, 260–268. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moradi, S.; Mnayer, L.; Earle, J.; Cech, A.C.; Ehrig, T. Plaque-Like Dermatofibroma: Case Report of a Rare Entity. Dermatopathology 2021, 8, 337-341. https://doi.org/10.3390/dermatopathology8030038
Moradi S, Mnayer L, Earle J, Cech AC, Ehrig T. Plaque-Like Dermatofibroma: Case Report of a Rare Entity. Dermatopathology. 2021; 8(3):337-341. https://doi.org/10.3390/dermatopathology8030038
Chicago/Turabian StyleMoradi, Sara, Laila Mnayer, Jonathan Earle, Alex C. Cech, and Torsten Ehrig. 2021. "Plaque-Like Dermatofibroma: Case Report of a Rare Entity" Dermatopathology 8, no. 3: 337-341. https://doi.org/10.3390/dermatopathology8030038
APA StyleMoradi, S., Mnayer, L., Earle, J., Cech, A. C., & Ehrig, T. (2021). Plaque-Like Dermatofibroma: Case Report of a Rare Entity. Dermatopathology, 8(3), 337-341. https://doi.org/10.3390/dermatopathology8030038