Abstract
Introduction: Human papilloma virus (HPV) vaccination is a key strategy for preventing HPV-related cancers, yet vaccine hesitancy remains a challenge due to persistent myths and misconceptions. This study aimed to identify the most frequently encountered HPV vaccine-related myths in clinical practice from the perspective of family doctors and to assess differences in their prevalence between urban and rural populations. Methods: A cross-sectional study was conducted among family doctors in Romania who reported common myths encountered when discussing HPV vaccination with parents and women eligible for catch-up vaccination. The analysis focused on identifying the most prevalent perceived myths and assessing differences between urban and rural settings, age groups and genders, using Kruskal-Wallis test, followed by post-hoc Dunn’s tests with Holm correction to account for multiple comparisons, as well as Chi-square tests. Results: The most frequently reported myths overall were “The HPV vaccine is only for girls” (mean score ± SD, 2.91 ± 1.27), “The HPV vaccine has severe and long-term side effects” (mean score ± SD, 2.83 ± 1.27), and “There are too many new vaccines” (mean score ± SD, 2.77 ± 1.3). Rural respondents reported significantly higher belief in concerns related to vaccine safety, effectiveness, increasing number of vaccines, necessity in monogamous individuals, fear of injections, and concerns about promiscuity, particularly in their perception of parents of adolescent girls. Conclusions: Family doctors consider that persistent myths continue to fuel vaccine hesitancy, especially in rural areas. Strengthening family doctors' communication skills through motivational interviewing and evidence-based counseling is essential. Public health efforts should focus on targeted educational interventions and social prescription tools to improve vaccine acceptance and reduce the burden of HPV-related diseases.
Introduction
According to official estimates, Romania has the highest incidence and mortality rates for cervical cancer in the European Union (EU). Each year, approximately 3,380 new cases and 1,805 deaths are recorded [1,2,3], highlighting the critical need to strengthen prevention efforts through expanded human papillomavirus (HPV) vaccination coverage and more effective cervical cancer screening programs.
The role of HPV infection in the development of precancerous lesions and, ultimately, cervical cancer has been unequivocally established. In response, the World Health Organization (WHO) has called on member countries to work towards the elimination of cervical cancer by 2030, setting ambitious public health targets: 90% HPV vaccination coverage among girls by age 15, ensuring that 70% of women undergo high-performance screening by ages 35 and 45, and providing treatment for 90% of women diagnosed with cervical lesions [4,5]. HPV infection can be prevented through primary prevention (vaccination, health education) and secondary prevention (screening). Although a national screening program is in place in Romania, its results remain below expectations and coverage targets [3,6,7].
HPV vaccination was first introduced in Romania in 2008, targeting girls aged 9-10 years. Despite a cohort of approximately 110,000 eligible girls, only 2,600 received the vaccine between 2008 and 2009, representing just 2% coverage [8,9,10,11]. This early rollout coincided with the emergence of Romania’s anti-vaccine movement and was hindered by widespread misinformation and fake news. Public resistance led many parents to refuse vaccination, prompting the Ministry of Health to suspend HPV vaccine procurement until 2020 [8,12,13,14].
This initial failure was part of a broader vaccine hesitancy trend that extended beyond HPV to routine childhood immunizations under the National Vaccination Program (PNV). As a result, Romania experienced a decline in coverage for essential childhood and at-risk group vaccines, including influenza and, eventually, COVID-19 vaccines [11,15,16,17,18,19].
HPV vaccine hesitancy was not unique to Romania. Similar resistance was observed in other Eastern European countries, where it had a substantial impact on national immunization programs. A recent meta-analysis identified key factors contributing to parental reluctance, such as older parental age (>40 years), immigrant status, unemployment, religious beliefs, previous vaccine refusals, safety concerns, and fears of increased sexual activity post-vaccination. Conversely, a history of abnormal Pap smears and belief in the vaccine’s effectiveness were linked to greater acceptance [20].These insights are crucial for shaping targeted public health strategies.
HPV vaccination was reintroduced in January 2020, following parental requests submitted to family doctors since 2017. Despite the rollout overlapping with the COVID-19 pandemic, uptake steadily increased, reaching 128,314 individuals vaccinated by December 1, 2023, according to the National Electronic Vaccination Registry (RENV). Initially, the program offered free HPV vaccination only to girls aged 11-14, with vaccine doses procured centrally by the Ministry of Health. In September 2021, eligibility expanded to include adolescents aged 15-18, improving accessibility. Vaccines continued to be administered through family doctors' offices, despite procedural and administrative challenges [2,6,11].
As of December 1, 2023, a reimbursement mechanism was introduced, shifting from centralized procurement to pharmacy-based access via electronic prescriptions issued by any physician contracted with the National Health Insurance House (CNAS). Under this new system, girls and boys aged 11-18 receive 100% reimbursement, and women aged 19-45 benefit from 50% compensation as part of a catch-up program. While family doctors remain the primary vaccinators, HPV vaccines are now also available in specialized outpatient clinics, further expanding access [21,22].
According to the National Institute of Public Health, between December 1, 2023, and December 31, 2024, a total of 94,497 individuals initiated HPV vaccination – representing 43% of all individuals vaccinated since January 2020 (222,811 in total) [2]. These data suggest a substantial increase in vaccine uptake following the implementation of the reimbursement mechanism. Nevertheless, Romania still falls short of the cervical cancer elimination goals set by the WHO and the targets outlined in the National Vaccination Strategy 2023-2030 [23].
Family doctors are central to Romania’s vaccination infrastructure. They administer the majority of vaccines included in the National Vaccination Calendar, with the exception of BCG and the first dose of the hepatitis B vaccine, which are delivered in maternity hospitals. Their long-term relationships with patients and the high level of public trust they enjoy position them as key players in combating vaccine hesitancy and improving immunization coverage [19,24].
This study aimed to assess family doctors’ perceptions of persistent HPV vaccine-related myths in Romania. Given their central role in vaccination, understanding the types and prevalence of myths they encounter is critical. We further analyzed these misconceptions by gender and age group to uncover specific patterns of hesitancy. This segmentation will inform the development of tailored communication strategies across primary care, specialty clinics, and hospital settings, ultimately supporting higher HPV vaccine acceptance and coverage.
Methods
Study design
We conducted a cross-sectional survey among family physicians in Romania between February 20-28, 2025, following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. We developed an online questionnaire consisting of 17 items in Google Forms, targeting family physicians nationwide. The questionnaire included both open-ended and closed-ended questions aimed at capturing the most frequently encountered HPV-related myths, as perceived by family doctors, during their discussions with different categories of patients and parents.
The selection of relevant myths was conducted through an online focus group with the 14 members of the Immunization Working Group (IWG) of the Romanian National Society of Family Medicine (SNMF). The questionnaire was developed based on the insights from this discussion. Prior to its launch, it was pilot-tested with 10 family physicians on February 20, 2025, in Bucharest, to assess clarity and refine wording. The final version was then distributed online.
We used Cochran’s formula to calculate the sample size when the population is finite for our study, adjusting it using a correction:

where:
Z = Z-score for the confidence level (1.96 for 95% confidence)
p = estimated proportion (0.5)
e = margin of error (0.05)
n = initial sample size from Cochran’s formula
N = 10,480
Our required sample size, based on Cochran’s formula and adjusted for a finite population, is 372 family doctors.
We computed Cronbach’s alpha to measure the internal consistency of items used in our questionnaire. The overall Cronbach’s alpha value for all items combined was 0.915, further indicating very high reliability of the survey, meaning the 10 Likert-scale items are strongly related and consistently measure the same construct (barriers to HPV vaccination).
The questionnaire investigated prevalent myths encountered by family doctors regarding HPV vaccination, categorizing them into three major themes: vaccine safety, vaccine effectiveness and necessity, and behavioral consequences. They were measured on a 5-point Likert scale (1 = "Strongly Disagree”, 2 = "Disagree”, 3 = "Neutral”, 4 = "Agree”, 5 = "Strongly Agree”) – Supplementary Table S1.
The questionnaire’s introduction provided information about the study objectives, the intended use of the data, and included a clear statement of informed consent. Participation was voluntary and continuation of the questionnaire implied consent to take part in the study.
Inclusion criteria were: agreement to participate, being a family physician (regardless of professional rank), and completion of all mandatory sections of the questionnaire.Exclusion criteria included: physicians from other specialties and incomplete responses.
The questionnaire was distributed online via the official communication platforms of the SNMF, including the national and county mailing list, Facebook groups, and WhatsApp groups. A total of 531 doctors from all counties in Romania responded to the questionnaire (Supplementary Figure S1).
After applying the exclusion criteria, 466 responses were retained for analysis, representing 4.44% of the 10,480 family physicians currently practicing nationwide under contract with the CNAS. Among the respondents, 63.91% were from urban areas and 36.08% from rural areas [25].
Statistical analysis
We used the Kruskal-Wallis test to determine if there are statistically significant differences between the five groups of the ordinal dependent variable (Likert score for the ten myths), followed by post-hoc Dunn’s tests with Holm correction to account for multiple comparisons. Chi-square tests (χ²) were applied to evaluate categorical differences in myth prevalence among groups. Significance levels were set at p<0.05. Statistical analyses were conducted using R (ggplot2 and ggstatsplot packages), and statistical significance was set to 0.05.
Ethics considerations
The study was approved by the Ethics Committee of the University of Medicine and Pharmacy of Craiova, Romania (no. 118/10.02.2025), adhering to the Helsinki Declaration and other established ethical principles.
Results
Participants
A number of 466 family doctors participated in this study, of which 68.5% were based in offices, a proportion closely aligned with the national average. The respondents’ ages ranged from under 30 years (1.5%) to over 70 years (5.2%). Their years of professional experience also varied, from early-career physicians (8.4%) to those with over 40 years of practice (13.5%). The largest proportion of participants (15.9%) had 21-25 years of experience. All experience groups were well represented, reflecting a broad range of expertise levels among the respondents (Table 1).

Table 1.
Characteristics of participating family doctors.
Analyzing overall trends, the main reported myth was "The HPV vaccine is only for girls” (2.91±1.27), followed by "The HPV vaccine has severe and long-term side effects (cancer, autoimmune diseases, others not yet discovered) because it contains harmful substances” (2.83±1.27) and "There are too many new vaccines” (2.77±1.3) – Table 2.
Table 2.
Applying Mann-Whitney U test to compare the myths across groups.
In analyzing the most frequently encountered myths by family doctors, we identified key misconceptions reported across different parental groups. Among parents of girls aged 11-14 (F14), the most common myth reported by the respondents was M2 – "The HPV vaccine is only for girls” (3.06±1.20), followed by M4 – "The HPV vaccine has severe and long-term side effects” (2.99±1.26) and M7 – "There are too many new vaccines” (2.92±1.27). Similarly, for parents of girls aged 15-18 (F18), the leading misconception reported was M4 – "The HPV vaccine has severe and long-term side effects” (2.93±1.24), followed by M2 – "The HPV vaccine is only for girls” (2.85±1.23) and the perception that there are too many new vaccines – M7 – "There are too many new vaccines” (2.82±1.29). For women over 19 years old (F19), the most frequently encountered myth was M4 – "The HPV vaccine has severe and long-term side effects” (2.69±1.26). The second most reported myth was M7 – "There are too many new vaccines” (2.58±1.31), followed by M2 – "The HPV vaccine is only for girls” (2.57±1.23).
For parents of boys aged 11-14 (B14), the top myths included M2 – "The HPV vaccine is only for girls” (3.09±1.31), concerns about severe and long-term side effects – M4 (2.81±1.30), and general skepticism about the increasing number of vaccines - M7 (2.81±1.31), as perceived by the family doctors. Similarly, in parents of boys aged 15-18 (B18), the dominant reported misconception was again M2 – "The HPV vaccine is only for girls” (2.96±1.28), followed by concerns over severe side effects (2.76±1.27) and the belief that there are too many new vaccines – M7 (2.72±1.32).
Statistical analysis revealed no significant differences between urban and rural areas in the F14 group regarding the myths encountered by family doctors. However, in the F18 group (parents of girls aged 15-18), significant differences were observed in multiple myths. The belief that the HPV vaccine has severe and long-term side effects (M4) was more frequently encountered in rural areas (3.16±1.24) compared to urban areas (2.83±1.22, p=0.009). Similarly, the perception that the HPV vaccine does not work and that Pap smears are sufficient (M5) was significantly more reported in rural settings (2.51±1.2) compared to urban areas (2.14±1.09, p=0.003). Additionally, skepticism regarding the increasing number of vaccines (M7) was higher in rural areas (3.1±1.35) than in urban ones (2.69±1.25, p=0.002), as perceived by family doctors. Other myths that showed significant differences included concerns about vaccine necessity in monogamous individuals (M8, rural: 2.77±1.3, urban: 2.45±1.26, p=0.017), fear of injections (M9, rural: 2.56±2.72, urban: 2.14±1.12, p=0.001), and concerns about HPV vaccination leading to promiscuity (M10, rural: 2.35±1.23, urban: 2.07±1.17, p=0.016).
In the F19 group (women over 19 years old), significant differences were observed between urban and rural respondents regarding myths related to vaccine necessity and safety. The belief that HPV vaccination is only for girls (M2) was more frequently encountered in rural areas (p=0.006). Similarly, concerns about the HPV vaccine causing severe and long-term side effects (M4) were significantly more reported in rural settings (2.91±1.30) compared to urban areas (2.59±1.23, p=0.012). The perception that the HPV vaccine does not work and that Pap smears are sufficient for cervical cancer prevention (M5) was also higher in rural respondents (2.45±1.22) compared to urban respondents (2.14±1.05, p=0.016). Additionally, concerns about the appropriate timing of HPV vaccination (M6) were significantly higher in rural areas (2.49±1.18) compared to urban areas (2.22±1.13, p=0.022). Skepticism regarding the necessity of the HPV vaccine in monogamous individuals (M8) was more prevalent in rural areas (2.60±1.25) than in urban areas (2.08±1.16, p<0.001). Likewise, fear of injections (M9) was significantly higher in rural settings (2.44±1.26) compared to urban ones (1.87±1.06, p<0.001). Finally, concerns that HPV vaccination leads to promiscuity (M10) were also more frequently reported in rural areas (2.20±1.19) compared to urban respondents (1.90±1.07, p=0.010).
According to family doctors, among parents of boys aged 11-14 (B14), several myths were more frequently encountered in rural settings. Concerns about vaccine safety (M4) were more commonly reported in rural areas (2.99±1.35) reporting higher than urban ones (2.72±1.26, p=0.043). Similarly, the belief that HPV vaccination is unnecessary for monogamous individuals (M8) was more prevalent in rural areas (2.56±1.33) compared to urban ones (2.22±1.23, p=0.011). Additionally, fear of injections (M9) was more frequently noted in rural respondents (2.69±1.31) versus urban ones (2.17±1.20, p<0.001). Finally, the misconception that HPV vaccination may encourage promiscuity (M10) was more often encountered by family doctors in rural contexts (2.35±1.27) compared to urban ones (2.02±1.14, p=0.007).
Similarly, for the B18 group (parents of boys aged 15-18), significant differences were observed between the identified myths of respondents across urban and rural areas. The belief that HPV vaccination is unnecessary if the child is not sexually active (M3) was more frequently reported by rural respondents (2.84±1.25) compared to urban ones (2.55±1.24, p=0.026). Concerns about vaccine safety (M4) were perceived as more common in rural settings (3.02±1.29) compared to urban ones (2.63±1.25, p=0.003). Similarly, skepticism about HPV vaccine effectiveness (M5) was more often reported by rural respondents (2.52±1.24) compared to urban respondents (2.17±1.13, p=0.005). Regarding the appropriate timing of HPV vaccination (M6), family doctors indicated that rural parents expressed higher belief in delaying vaccination (2.54±1.25) compared to urban respondents (2.25±1.11, p=0.024). Vaccine skepticism (M7) was also significantly more frequently perceived in rural settings (3.07 ± 1.35) compared to urban ones (2.55±1.28, p<0.001).
Family doctors reported that, in rural areas, the myth that HPV vaccination is unnecessary for individuals in monogamous relationships (M8) was encountered more frequently (rural: 2.61±1.34, urban: 2.23±1.22, p=0.004). Fear of injections (M9) was significantly more reported among rural respondents (2.59±1.32) than urban ones (2.15±1.21, p=0.001). Lastly, concerns about HPV vaccination leading to promiscuity (M10) were higher in rural settings (2.22±1.22) compared to urban ones (1.98±1.13, p=0.039).
There are statistically significant differences between the groups (χ2(4)=17.14, p<0.001, ɛ2=7.36e-03, 95%CI: [3.83e-03, 1.00]). Further, the post-hoc test results indicated a significant difference between specific groups: according to family doctors responses myth M1 was more frequently encountered in parents of girls under 14 than parents of the boys under 14 (p=0.04). The magnitude and direction of the differences between parents of girls 14-18 years old and women over 19 (p=0.03) or boys under 14 (p<0.001) are visually represented in Figure 1A. We observed no differences between the perception of the myths in regard to parents of girls under 14, girls under 18 and women over 19 related to the infertility that HPV vaccine would hypothetically cause.
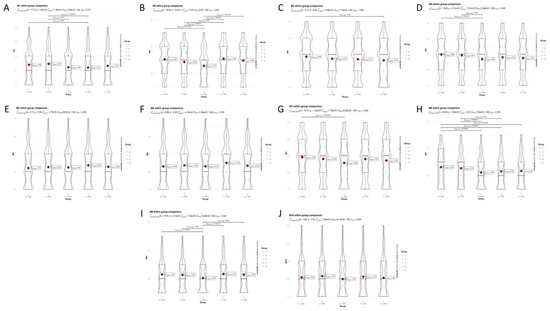
Figure 1.
Comparison across the perception over the five groups. (1 = parents of girls under 14 years, 2 = parents of girls between 15-18 years, 3 = women over 19 years, 4 = parents of boys under 14 years, 5 = parents of boys between 15-18 years) for (A) M1 myth (The HPV vaccine causes infertility); (B) M2 myth (The HPV vaccine is only for girls); (C) M3 myth (The HPV vaccine is not necessary if the child is not sexually active); (D) M4 myth (The HPV vaccine has severe and long-term side effects – cancer, autoimmune diseases, others not yet discovered, because it contains harmful substances); (E) M5 myth (The HPV vaccine does not work. Pap smears are sufficient to prevent cervical cancer); (F) M6 myth (The HPV vaccine should only be given in adolescence/after menarche); (G) M7 myth (There are too many new vaccines); (H) M8 myth (The HPV vaccine is not necessary because my daughter will be good, have monogamous relationships); (I) M9 myth (They don't want to administer for fear of the injection); (J) M10 myth (Promiscuity (girls/boys will be tempted to have multiple sexual relationships)).
Significant differences were found between the five groups (χ2(4)=53.06, p<0.001, ɛ2=0.02, 95%CI: [0.02, 1.00]) regarding the myth M2: The HPV vaccine is only for girls, as shown in Figure 1B. The central tendency of the groups varies, with perception that parents of girls under 14 and boys under 14 having the highest beliefs in this myth.
The results for the M3 myth ("The HPV vaccine is not necessary if the child is not sexually active”) comparation across the four groups indicate statistically significant differences (χ2(3)=8.12, p=0.04, ɛ2=4.36e-03, 95%CI: [1.75e-03, 1.00]), as shown in Figure 1C.Highest mean score (2.86), indicating the highest level of agreement with the myth, was considered for parents of girls under 14. Lowest mean score (2.65), suggesting the least agreement with the myth, was reported by family doctors in parents of boys between 15 and 18 years.
The significant differences in perceptions about the myth regarding severe and long-term side effects of the HPV vaccine were observed (χ2(4)=16.8, p<0.001, ɛ2=7.21e-03, 95%CI: [3.46e-03, 1.00]). Responders state that the myth is encountered more in parents of younger children: groups 1 and 4 (the mean score is higher: 2.99 for girls and 2.81 for boys), as shown in Figure 1D. It is least encountered in women over 19, which have the lowest mean score (2.69), suggesting less concern or belief in the myth (p=0.04 compared with group 2 and p<0.0001 compared with group 1).
The results for the M5 myth ("The HPV vaccine does not work. Pap smears are sufficient to prevent cervical cancer”) comparisons across the five groups indicate that there are no statistically significant differences between the groups (χ2(4)=4.13, p=0.389, ɛ2=1.77e-03, 95%CI: [9.87e-04, 1.00]), as shown in Figure 1E. We observed uniform awareness or misinformation about the HPV vaccine and Pap smears across groups.
There are marginal differences in the perception of the M6 myth across the five groups (χ2(4)=9.66, p=0.05, ɛ2=4.15e-03, 95%CI: [1.68e-03, 1.00]), which is the threshold of statistical differences. The effect size (4.15e-03) is relatively small, indicating that the differences between groups are not very large. This could imply that the belief in the M6 myth is relatively consistent across the groups, with only minor variations. Group 4 has the highest mean score (mean score = 2.50), suggesting that this perception of parents of boys under 14 is more strongly associated with the myth that the HPV vaccine should only be given in adolescence, as shown in Figure 1F.
A statistically significant difference between the groups forM7 myth (χ2(4)=18.15, p<0.001, ɛ2=7.79e-03, 95%CI: [3.25e-03, 1.00]), as shown in Figure 1G. The mean perception scores regarding the groups is relatively close, ranging from 2.72 to 2.88. This suggests that while there are statistically significant differences, the practical differences in perceptions might be small. The Holm-adjusted p-value is 5.81e-04 (group 1 vs group 3), which further confirms the significance of the results after adjusting for multiple comparisons. Parents of younger children (groups 1 and 4) might be more concerned about the number of vaccines due to the higher frequency of vaccinations in early childhood. Parents of teenagers (groups 2 and 5) might have different concerns based on the specific vaccines recommended for older children and adolescents. Group 3 might have different perspectives based on their own experiences and knowledge about vaccines, which could be less influenced by immediate parental concerns.
A statistically significant difference between groups was found regarding myth M8 (χ2(4)=29.09, p<0.001, ɛ2=0.01, 95%CI: [7.60e-03, 1.00]), as shown in Figure 1H. Multiple Holm-adjusted p-values are provided, ranging from 9.23e-05 to 0.03, indicating significant results after adjusting for multiple comparisons. We observed that statistically differences were based on developmental stages (group 1 vs group 3, p < 0.001) or gender (group 1 vs group 4, p < 0.001).
The Kruskal-Wallis test shows that there are statistically significant differences in the perception of the M9 myth across the five groups (χ2(4)=16.81, p<0.001, ɛ2=7.22e-03, 95%CI: [4.28e-03, 1.00]), as shown in Figure 1I. This means that fear of the injection as a reason for not administering the HPV vaccine varies significantly depending on the group. The small but meaningful effect size (7.22e−03) suggests that while the differences between groups are not large, they are still notable and statistically significant. Group 3 has the lowest mean score (mean = 2.05), suggesting that this group is less likely to agree with the myth that fear of the injection is a reason for not administering the HPV vaccine. The other groups (1, 2, 4, and 5) have higher mean scores, ranging from 2.27 to 2.33, indicating stronger agreement with the myth compared to Group 3.
The results (χ2(4)=4.65, p=0.32, ɛ2=2.00e-03, 95%CI: [9.10e-04, 1.00]) indicate that there are no significant differences in the perception of the M10 myth across the five groups. The effect size (2.00e-03), which is very small, further supports the lack of significant differences between groups, as shown in Figure 1J. All groups have similar levels of agreement or disagreement with the myth that the HPV vaccine might lead to promiscuity.
Discussion
Over time, various myths about HPV vaccination have been documented. Bednarczyk outlined several recurring concerns, such as: "HPV vaccine has not been shown to prevent cervical cancer”, "Pap smears are sufficient”, "vaccines are unsafe”, or "11-12 years is too young” for vaccination [26]. Other studies have noted myths around infertility, vaccine ineffectiveness, and sexual disinhibition [27].
This study explored how frequently Romanian family doctors encounter these myths in clinical practice, based on their interactions with parents of boys and girls aged 11-18 years and women over 19 years old. Their responses reflect real-world challenges in vaccine communication and provide insights into demographic patterns of vaccine hesitancy.
Vaccine safety
Myth M1 ("HPV vaccines are associated with infertility”) was encountered at low to moderate levels by doctors across all groups, with no significant urban–rural variation. Despite public concern, studies show the vaccine is protective – reducing infertility risk through the prevention of HPV-related lesions and infections [28,29,30,31,32,33].
Myth M4 ("The HPV vaccine has severe and long-term adverse reactions – cancer, autoimmune diseases, others not yet discovered, because it contains harmful substances”) was reported more frequently in rural settings and by doctors interacting with parents of younger children. Although long-term evaluations show no association with such conditions [34,35,36,37,38,39], this remains a widely encountered myth.
This practical concern regarding M9 ("They don't want to administer it for fear of the injection”) was commonly perceived by doctors during discussions with parents – especially of younger children – but less so with adult women. It remains a persistent barrier to vaccine uptake. Numerous studies have identified it as a significant barrier to vaccination programs, potentially reducing vaccine acceptance not only for the HPV vaccine but also for the influenza vaccine and other immunizations [16,40,41].
Doctors cited the M7 myth ("There are too many new vaccines”) more often among rural parents, reflecting broader vaccine skepticism. However, research confirms that current vaccine schedules are safe and immunologically manageable [42]. Our findings show that perception on parents of younger children, both boys and girls, showed higher concern, likely due to early childhood vaccination schedules, while women over 19 years old had the lowest concern, possibly reflecting personal vaccine experience rather than parental hesitancy.
Vaccine effectiveness
The M2 myth ("The HPV vaccines are only for girls”) was frequently reported by doctors during discussions with parents of boys. Directly, vaccination protects against cutaneous HPV-related diseases, penile cancer, and throat cancer. Indirectly, in countries with low HPV vaccination coverage among girls, vaccinating boys enhances herd immunity, contributing to broader community protection [43,44,45,46,47,48,49,50,51,52]. Although vaccination benefits both genders, this misconception persists, indicating the need for clearer messaging around the role of boys in HPV transmission and prevention.
Family doctors encountered the M3 myth ("The HPV vaccine is not necessary if the child is not sexually active”) most often among parents of girls under 14 years. HPV vaccination is most effective before sexual debut [53,54,55], and Romanian data shows early initiation of sexual activity and adolescent pregnancies [56,57].
This myth (M5 "The HPV vaccine does not work. Pap smears are sufficient to prevent cervical cancer”) was more common in rural areas, as reported by doctors. While screening is essential, in Romania women undergo Pap tests more often when they experience symptoms rather than as a preventive measure, and it cannot replace the benefits of primary prevention through vaccination [3,4,58,59].
Doctors noted the belief in M6 ("The HPV vaccine should only be given in adolescence, after the onset of menarche”) especially in discussions with parents of boys under 14 years. The timing misconception conflicts with guidelines that recommend vaccination as early as possible [53,54].
The belief – often cited by rural parents – overlooks unpredictable sexual behaviors and non-sexual transmission of M8 (The HPV vaccine is not necessary because my daughter will be well-behaved, she will have monogamous relationships). Doctors reported it most often in parents of younger girls, while adult women were less likely to hold this view [60,61,62,63,64].
Behavior consequences
Although relatively consistent across groups, the M10 myth ("Promiscuity - girls will be tempted to have multiple sexual relationships. HPV vaccine will cause sexual disinhibition: risk compensation”) was more commonly encountered by doctors in rural consultations. Numerous studies refute any link between vaccination and increased sexual activity [65,66,67,68].
Although no single myth exhibited significant differences between rural and urban areas across all groups, four myths - M4 (concerns about severe and long-term vaccine side effects), M8 (vaccine necessity in monogamous individuals), M9 (fear of injections), and M10 (concerns about increased promiscuity post-vaccination) – consistently showed statistically significant differences between urban and rural respondents in four groups (F18, F19, B14, and B18). These results indicate that vaccine hesitancy varies across demographic groups and underscore key misconceptions that should be addressed through targeted public health interventions.
Communication
Our findings highlight the crucial role of frontline healthcare workers (HCWs) in effectively engaging with patients and addressing vaccine hesitancy. Persuasive communication strategies are essential, including motivational interviewing and empathetic refutational interviews, which have been shown to increase vaccination intent among counseled individuals. Addressing HPV vaccine hesitancy requires a multi-stakeholder approach that improves public communication, evidence-based policymaking, provider education, and media responsibility to rebuild trust and vaccine confidence, ultimately reducing preventable diseases and complications [69]. Additionally, community-based social events can serve as valuable platforms for disseminating accurate information [70]. Furthermore, the implementation of social prescription tools, where qualified professionals deliver evidence-based messages in an accessible and culturally appropriate manner, may offer an effective strategy for debunking myths and improving adherence to preventive measures [71,72,73].
Limitations
This study has several limitations that should be considered when interpreting the results. First, the study relies on self-reported data, which may be subject to recall bias or social desirability bias. Participants may have underreported or overreported certain myths or attitudes due to perceived professional expectations. Second, the sample may not be entirely representative of all HCWs, as participation was voluntary, potentially leading to selection bias. Third, while the study explores significant differences between urban and rural settings, it does not account for other potential confounding factors such as socioeconomic status, educational background, or prior exposure to vaccine-related misinformation. Lastly, while the study provides valuable insights into the myths encountered in clinical practice, it does not measure the direct impact of interventions or educational programs on vaccine acceptance, requiring further research to evaluate the effectiveness of tailored communication strategies.
Generalizability
The findings of this study are relevant and applicable to healthcare settings where family doctors play a primary role in vaccination counseling and administration. The results can be generalized to similar healthcare systems, particularly in countries where vaccine hesitancy remains a challenge. However, cultural, educational, and systemic differences across countries and regions may limit full generalizability. The study's focus on myths encountered in routine clinical practice makes it valuable for designing targeted interventions applicable in primary care, public health campaigns, and vaccination programs. Nevertheless, variability in national vaccination policies, healthcare infrastructure, and public attitudes toward HPV vaccination may influence how the findings translate to other settings. Further multinational and longitudinal studies are needed to assess whether similar patterns persist in different healthcare and social contexts.
Conclusions
This study highlights family doctors’ perceptions of persistent myths encountered in their practice, surrounding HPV vaccination, particularly those related to safety, gender specificity, and necessity. These misconceptions are perceived as more common among rural populations. The findings underscore the need for targeted educational efforts and improved communication tools to support family doctors in addressing vaccine hesitancy and promoting informed decision-making.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.18683/germs.2025.1453/s1, Figure S1: Regional distribution of respondents by county; Table S1: Questionnaire on HPV vaccine myths encountered in clinical practice.
Author Contributions
Conceptualization, GGD, ATS and RS; methodology, GGD, RS; investigations, ATS, ȘOP; software, ATS; validation, ATS, GGD, AL, ȘOP; formal analysis, ATS; resources, GGD; data curation, SAA, DS, CB, MC, CVB, AD, AG, ML, IB, MV, AL, CAD, FP, DS, MAI; writing—original draft preparation, GGD, ATS, RS; writing – review and editing, AL, ȘOP, CAD; supervision, ATS, ȘOP; project administration GGD; All authors read and approved the final version of the manuscript.
Funding
None to declare.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee from the University of Medicine and Pharmacy of Craiova, Romania (no. 118/10.02.2025).
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.
Acknowledgments
The authors would like to extend their sincere appreciation to their colleague respondents for their participation in this study.
Conflicts of Interest
All authors – none to declare.
References
- ICO/IARC Information Centre on HPV and Cancer. Romania Human Papillomavirus and Related Cancers, Fact Sheet 2023. Available online: https://hpvcentre.net/statistics/reports/ROU_FS.pdf (accessed on 22 February 2025).
- Institutul Național de Sănătate Publică. Raport privind evolutia vaccinarii impotriva HPV 2024. Available online: https://insp.gov.ro/centrul-national-de-supraveghere-si-control-al-bolilor-transmisibile-cnscbt/analiza-date-supraveghere/ (accessed on 22 February 2025).
- Furtunescu, F.; Bohiltea, R.E.; Neacsu, A.; et al. Cervical cancer mortality in Romania: trends, regional and rural-urban inequalities, and policy implications. Medicina (Kaunas) 2021, 58, 18. [Google Scholar] [CrossRef]
- Brisson, M.; Drolet, M. Global elimination of cervical cancer as a public health problem. Lancet Oncol. 2019, 20, 319–321. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem. Available online: https://www.who.int/publications/i/item/9789240014107 (accessed on day month year).
- Simion, L.; Rotaru, V.; Cirimbei, C.; et al. Inequities in screening and HPV vaccination programs and their impact on cervical cancer statistics in Romania. Diagnostics (Basel). 2023, 13, 2776. [Google Scholar] [CrossRef]
- Todor, R.D.; Bratucu, G.; Moga, M.A.; Candrea, A.N.; Marceanu, L.G.; Anastasiu, C.V. Challenges in the prevention of cervical cancer in Romania. Int J Environ Res Public Health. 2021, 18, 1721. [Google Scholar] [CrossRef]
- Voidăzan, S.; Tarcea, M.; Morariu, S.H.; Grigore, A.; Dobreanu, M. Human papillomavirus vaccine - knowledge and attitudes among parents of children aged 10-14 years: a cross-sectional study, Tîrgu Mureş, Romania. Cent Eur J Public Health. 2016, 24, 29–38. [Google Scholar] [CrossRef]
- Ministry of Health. Comunicat de presă Ministerul Sănătăţii demarează campania de informare pentru prevenirea prin vaccinare a cancerului de col uterin. Available online: https://old.ms.ro/index.php?pag=62&id=6683&pg=1 (accessed on 22 February 2025).
- Stefanopol, I.A.; Baroiu, L.; Chirila, S.; et al. The influence of living in rural areas on the evolution and management of pediatric ovarian cystic lesions: a retrospective study on a cohort from South Eastern Romania. Int J Gen Med. 2022, 15, 5273–5284. [Google Scholar] [CrossRef]
- Manolescu, L.S.C.; Zugravu, C.; Zaharia, C.N.; et al. Barriers and facilitators of Romanian HPV (human papillomavirus) vaccination. Vaccines (Basel). 2022, 10, 1722. [Google Scholar] [CrossRef]
- Voidăzan, T.S.; Budianu, M.A.; Rozsnyai, F.F.; Kovacs, Z.; Uzun, C.C.; Neagu, N. Assessing the level of knowledge, beliefs and acceptance of HPV vaccine: a cross-sectional study in Romania. Int J Environ Res Public Health. 2022, 19, 6939. [Google Scholar] [CrossRef]
- Penţa, M.A.; Băban, A. Dangerous agent or saviour? HPV vaccine representations on online discussion forums in Romania. Int J Behav Med. 2014, 21, 20–28. [Google Scholar] [CrossRef]
- Penţa, M.A.; Băban, A. Mass media coverage of HPV vaccination in Romania: a content analysis. Health Educ Res. 2014, 29, 977–992. [Google Scholar] [CrossRef] [PubMed]
- Turcu-Stiolica, A.; Boicea, A.R.; Nechita, F.; et al. Development and validation of a questionnaire to measure COVID-19 vaccine hesitancy within the Romanian industrial laborers. Front Public Health. 2025, 13, 1482778. [Google Scholar] [CrossRef]
- Dumitra, G.G.; Alexiu, S.A.; Sănduțu, D.; et al. Segmenting attitudes toward vaccination –behavioral insights into influenza vaccination refusal in Romania. Germs. 2024, 14, 362–374. [Google Scholar] [CrossRef]
- Dascalu, S.; Geambasu, O.; Covaciu, O.; et al. Prospects of COVID-19 vaccination in Romania: challenges and potential solutions. Front Public Health. 2021, 9, 644538. [Google Scholar] [CrossRef]
- Dube, E.; Pistol, A.; Stanescu, A.; et al. Vaccination barriers and drivers in Romania: a focused ethnographic study. Eur J Public Health. 2023, 33, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Societatea Națională de Medicina Familiei. Comunicat de presă - Atitudinea populației față de vaccinuri și vaccinare - Sondaj privind vaccinarea. Available online: https://snmf.ro/2019/03/10/atitudinea-populatiei-fata-de-vaccinuri-si-vaccinare-sondaj-de-opinie-inscop-research/ (accessed on 15 September 2024).
- Achimaș-Cadariu, T.; Pașca, A.; Jiboc, N.M.; Puia, A.; Dumitrașcu, D.L. Vaccine hesitancy among European parents-psychological and social factors influencing the decision to vaccinate against HPV: a systematic review and meta-analysis. Vaccines (Basel). 2024, 12, 127. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Ordin nr. 3120 din 12 septembrie 2023 pentru aprobarea segmentelor populaționale care beneficiază de prescrierea, eliberarea și decontarea în regim de compensare a medicamentelor imunologice folosite pentru producerea imunității active sau folosite pentru prevenirea unor boli transmisibile. Available online: https://legislatie.just.ro/public/DetaliiDocument/274488 (accessed on 2 February 2025).
- Ministerul Sănătății România. Ordin nr. 3278/804/2023 privind completarea anexei nr. 1 la ordinul ministrului sănătății și al președintelui Casei Naționale de Asigurări de Sănătate nr. 564/499/2021 pentru aprobarea protocoalelor terapeutice. Monitorul Oficial. Available online: https://legislatie.just.ro/Public/DetaliiDocument/274834 (accessed on 17 July 2024).
- Guvernul României. Hotărâre privind aprobarea strategiei nationale de vaccinare 2023-2030. Available online: https://sgglegis.gov.ro/legislativ/docs/2023/08/g63hp1tcrwfb8s02dv5m.pdf (accessed on 30 August 2024).
- Institutul Român pentru Evaluare și Strategie. Percepții, atitudini și comportamente cu privire la vaccinarea COVID-19 - sondaj de opinie septembrie 2021. Available online: https://ires.ro/uploads/articole/ires_pac_vaccinare-covid-19_sondaj-national_sept-2021_romania-curata_prezentare.pdf (accessed on 23 February 2025).
- Casa Națională de Asigurări de Sănătate, Raport de activitate ianuarie-decembrie 2023. Available online: https://cnas.ro/wp-content/uploads/2024/10/Raport-de-activitate-al-CNAS-pentru-anul-2023.pdf (accessed on 1 March 2025).
- Bednarczyk, R.A. Addressing HPV vaccine myths: practical information for healthcare providers. Hum Vaccin Immunother. 2019, 15, 1628–1638. [Google Scholar] [CrossRef]
- Zimet, G.D.; Rosberger, Z.; Fisher, W.A.; Perez, S.; Stupiansky, N.W. Beliefs, behaviors and HPV vaccine: correcting the myths and the misinformation. Prev Med. 2013, 57, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Schuler, C.L.; Hanley, C.J.; Coyne-Beasley, T. Misconception: human papillomavirus vaccine and infertility. Clin Pediatr (Phila). 2014, 53, 158–165. [Google Scholar] [CrossRef]
- Levy, M.S.; Hunt, K.N.; Rinehart, S.; et al. COVID-19 vaccine information and infertility posts on X: insights on a misinformation pandemic. Perm J. 2024, 28, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, H.E.; Vann, J.C.J. Strategies to address COVID-19 vaccine and pregnancy myths. MCN Am J Matern Child Nurs. 2023, 48, 215–223. [Google Scholar] [CrossRef]
- Schmuhl, N.B.; Mooney, K.E.; Zhang, X.; Cooney, L.G.; Conway, J.H.; LoConte, N.K. No association between HPV vaccination and infertility in U.S. females 18-33 years old. Vaccine. 2020, 38, 4038–4043. [Google Scholar] [CrossRef]
- Dempsey, A.F.; Butchart, A.; Singer, D.; Clark, S.; Davis, M. Factors associated with parental intentions for male human papillomavirus vaccination: results of a national survey. Sex Transm Dis. 2011, 38, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Muscianisi, F.; Foresta, C.; Garolla, A. Role of HPV vaccination for prevention of male infertility. Minerva Endocrinol (Torino). 2022, 47, 70–76. [Google Scholar] [CrossRef]
- Angelo, M.G.; David, M.P.; Zima, J.; et al. Pooled analysis of large and long-term safety data from the human papillomavirus-16/18-AS04-adjuvanted vaccine clinical trial programme. Pharmacoepidemiol Drug Saf. 2014, 23, 466–479. [Google Scholar] [CrossRef]
- Lu, B.; Kumar, A.; Castellsagué, X.; Giuliano, A.R. Efficacy and safety of prophylactic vaccines against cervical HPV infection and diseases among women: a systematic review & meta-analysis. BMC Infect Dis. 2011, 11, 13. [Google Scholar] [CrossRef]
- Joshi, J.; Das, M.K.; Polpakara, D.; Aneja, S.; Agarwal, M.; Arora, N.K. Vaccine Safety and Surveillance for Adverse Events Following Immunization (AEFI) in India. Indian J Pediatr. 2018, 85, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Dey, A.; Wang, H.; Quinn, H.; et al. Surveillance of adverse events following immunisation in Australia: annual report, 2018. Commun Dis Intell. 2020, 44, 1–28. [Google Scholar] [CrossRef]
- Guo, B.; Page, A.; Wang, H.; Taylor, R.; McIntyre, P. Systematic review of reporting rates of adverse events following immunization: an international comparison of post-marketing surveillance programs with reference to China. Vaccine. 2013, 31, 603–617. [Google Scholar] [CrossRef]
- Dey, A.; Wang, H.; Quinn, H.; et al. Surveillance of adverse events following immunisation in Australia annual report, 2017. Commun Dis Intell. 2019, 43, 1–28. [Google Scholar] [CrossRef]
- Bonanni, P.; Zanella, B.; Santomauro, F.; Lorini, C.; Bechini, A.; Boccalini, S. Safety and perception: what are the greatest enemies of HPV vaccination programmes? Vaccine. 2018, 36, 5424–5429. [Google Scholar] [CrossRef]
- Turki, Y.M.; Alqurashi, J. Knowledge, attitudes, and perceptions towards human papillomavirus (HPV) vaccination among adult women in primary health care centers in Makkah, Saudi Arabia. Cureus. 2023, 15, e44157. [Google Scholar] [CrossRef]
- Offit, P.A.; Quarles, J.; Gerber, M.A.; et al. Addressing parents' concerns: do multiple vaccines overwhelm or weaken the infant's immune system? Pediatrics. 2002, 109, 124–129. [Google Scholar] [CrossRef]
- Chan, J.Y.K.; Cheung, M.K.; Lan, L.; et al. Characterization of oral microbiota in HPV and non-HPV head and neck squamous cell carcinoma and its association with patient outcomes. Oral Oncol. 2022, 135, 106245. [Google Scholar] [CrossRef]
- 44. Constantin, M.; Chifiriuc, M.C.; Mihaescu, G.; et al. Implications of oral dysbiosis and HPV infection in head and neck cancer: from molecular and cellular mechanisms to early diagnosis and therapy. Front Oncol. 2023, 13, 1273516. [Google Scholar] [CrossRef]
- Alemany, L.; Cubilla, A.; Halec, G.; et al. Role of human papillomavirus in penile carcinomas worldwide. Eur Urol. 2016, 69, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Iorga, L.; Marcu, D.R.; Diaconu, C.C.; et al. Penile carcinoma and HPV infection (Review). Exp Ther Med. 2020, 20, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Miralles-Guri, C.; Bruni, L.; Cubilla, A.L.; Castellsagué, X.; Bosch, F.X.; de Sanjosé, S. Human papillomavirus prevalence and type distribution in penile carcinoma. J Clin Pathol. 2009, 62, 870–878. [Google Scholar] [CrossRef]
- Șandru, F.; Radu, A.M.; Petca, A.; Dumitrașcu, M.C.; Petca, R.C.; Roman, AM. Unveiling the therapeutic horizon: HPV vaccines and their impact on cutaneous diseases-a comprehensive review. Vaccines (Basel). 2024, 12, 228. [Google Scholar] [CrossRef] [PubMed]
- Pham, C.T.; Juhasz, M.; Sung, C.T.; Mesinkovska, N.A. The human papillomavirus vaccine as a treatment for human papillomavirus-related dysplastic and neoplastic conditions: a literature review. J Am Acad Dermatol. 2020, 82, 202–212. [Google Scholar] [CrossRef]
- Ng, S.S.; Hutubessy, R.; Chaiyakunapruk, N. Systematic review of cost-effectiveness studies of human papillomavirus (HPV) vaccination: 9-valent vaccine, gender-neutral and multiple age cohort vaccination. Vaccine. 2018, 36, 2529–2544. [Google Scholar] [CrossRef]
- Colzani, E.; Johansen, K.; Johnson, H.; Pastore Celentano, L. Human papillomavirus vaccination in the European Union/European Economic Area and globally: a moral dilemma. Euro Surveill. 2021, 26, 2001659. [Google Scholar] [CrossRef]
- Jentschke, M.; Kampers, J.; Becker, J.; Sibbertsen, P.; Hillemanns, P. Prophylactic HPV vaccination after conization: a systematic review and meta-analysis. Vaccine. 2020, 38, 6402–6409. [Google Scholar] [CrossRef]
- Baisley, K.; Kemp, T.J.; Mugo, N.R.; et al. Comparing one dose of HPV vaccine in girls aged 9-14 years in Tanzania (DoRIS) with one dose in young women aged 15-20 years in Kenya (KEN SHE): an immunobridging analysis of randomised controlled trials. Lancet Glob Health. 2024, 12, e491–e499. [Google Scholar] [CrossRef]
- Seyferth, E.R.; Bratic, J.S.; Bocchini, J.A., Jr. Human papillomavirus epidemiology and vaccine recommendations: selected review of the recent literature. Curr Opin Pediatr. 2016, 28, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Valentino, K.; Poronsky, C.B. Human papillomavirus infection and vaccination. J Pediatr Nurs. 2016, 31, e155–e166. [Google Scholar] [CrossRef] [PubMed]
- Pagina de Psihologie. În România, 22,5% dintre adolescenți au primul contact sexual înainte de 15 ani, iar 11,8% prima naștere. Interviu cu Gabriel Brumariu (2022). Available online: https://www.paginadepsihologie.ro/in-romania-225-dintre-adolescenti-au-primul-contact-sexual-inainte-de-15-ani-iar-118-prima-nastere-interviu-cu-gabriel-brumariu/?srsltid=AfmBOorUq3LWVaT6AsciaqGbWaBLpmUAXc7wUIe3UZ_hJDhVCwBoSraV (accessed on 1 March 2025).
- Libertatea. Studiu: La ce vârstă își încep copiii români viața sexuală. Available online: https://www.libertatea.ro/stiri/studiu-la-ce-varsta-isi-incep-copiii-romani-viata-sexuala-1166420 (accessed on 1 March 2025).
- Simion, L.; Rotaru, V.; Cirimbei, C.; et al. Inequities in screening and HPV vaccination programs and their impact on cervical cancer statistics in Romania. Diagnostics (Basel). 2023, 13, 2776. [Google Scholar] [CrossRef]
- Ministry of Health. Planul Național de Combatere și Control al Cancerului. Comisia Multidisciplinară de Oncologie (2023). Available online: https://www.ms.ro/media/documents/Planul_Național_de_Combatere_și_Control_al_Cancerului_RIQiTXG.pdf (accessed on 28 February 2025).
- Gavillon, N.; Vervaet, H.; Derniaux, E.; Terrosi, P.; Graesslin, O.; Quereux, C. Papillomavirus humain (HPV): comment ai-je attrapé ça? [How did I contract human papillomavirus (HPV)?]. Gynecol Obstet Fertil. 2010, 38, 199–204. [Google Scholar] [CrossRef]
- Brouwer, A.F.; Meza, R.; Eisenberg, M.C. Transmission heterogeneity and autoinoculation in a multisite infection model of HPV. Math Biosci. 2015, 270 Pt A, 115–125. [Google Scholar] [CrossRef]
- Kero, K.; Rautava, J. HPV infections in heterosexual couples: mechanisms and covariates of virus transmission. Acta Cytol. 2019, 63, 143–147. [Google Scholar] [CrossRef]
- Sethi, S.; Ju, X.; Antonsson, A.; et al. Oral HPV infection among Indigenous Australians; incidence, persistence, and clearance at 12-month follow-up. Cancer Epidemiol Biomarkers Prev. 2022, 31, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Wei, F.; Gaisa, M.M.; D'Souza, G.; et al. Epidemiology of anal human papillomavirus infection and high-grade squamous intraepithelial lesions in 29 900 men according to HIV status, sexuality, and age: a collaborative pooled analysis of 64 studies. Lancet HIV. 2021, 8, e531–e543. [Google Scholar] [CrossRef]
- Donken, R.; Ogilvie, G.S.; Bettinger, J.A.; Sadarangani, M.; Goldman, R.D. Effect of human papillomavirus vaccination on sexual behaviour among young females. Can Fam Physician. 2018, 64, 509–513. [Google Scholar]
- Rysavy, M.B.; Kresowik, J.D.; Liu, D.; Mains, L.; Lessard, M.; Ryan, G.L. Human papillomavirus vaccination and sexual behavior in young women. J Pediatr Adolesc Gynecol. 2014, 27, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Otero, C.; Thompson, E.L.; Daley, E.M.; Griner, S.B.; Logan, R.; Vamos, C.A. Dispelling the myth: exploring associations between the HPV vaccine and inconsistent condom use among college students. Prev Med. 2016, 93, 147–150. [Google Scholar] [CrossRef]
- Stupiansky, N.W.; Zimet, G.D. Chapter 11 - STD vaccine acceptability in sexually transmitted diseases. In Sexually Transmitted Diseases, 2nd ed.; Stanberry, L.R., Rosenthal, S.L., Eds.; Academic Press, 2013; pp. 251–269. [Google Scholar] [CrossRef]
- Kunitoki, K.; Funato, M.; Mitsunami, M.; Kinoshita, T.; Reich, M.R. Access to HPV vaccination in Japan: increasing social trust to regain vaccine confidence. Vaccine. 2021, 39, 6104–6110. [Google Scholar] [CrossRef]
- Mundagowa, P.T.; Vora, S.; Seck, F.; Dhankhode, N.; Sakyi, K.S.; Kanyangarara, M. Exploring the views of barbers and stylists on the acceptability of delivering community-based interventions to promote COVID-19 testing and vaccination in South Carolina. Vaccines (Basel). 2024, 12, 1011. [Google Scholar] [CrossRef]
- Surugiu, R.; Iancu, M.A.; Lăcătus, A.M.; et al. Unveiling the presence of social prescribing in Romania in the context of sustainable healthcare—a scoping review. Sustainability. 2023, 15, 11652. [Google Scholar] [CrossRef]
- Gagneur, A. Motivational interviewing: a powerful tool to address vaccine hesitancy. Can Commun Dis Rep. 2020, 46, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Gagneur, A.; Lemaître, T.; Gosselin, V.; et al. A postpartum vaccination promotion intervention using motivational interviewing techniques improves short-term vaccine coverage: PromoVac study. BMC Public Health. 2018, 18, 811. [Google Scholar] [CrossRef] [PubMed]




© GERMS 2025.