Abstract
Introduction: Bloodstream infection is a common condition at the Emergency Department (ED). Appropriate antibiotic therapy is also crucial for patients with bloodstream infection particularly at the ED. This study therefore aimed to find clinical factors predictive of types of bacterial pathogens in bloodstream infection patients presenting at the ED focused on Gram-negative bacterial infections. Methods: This was a retrospective study. The inclusion criteria were adult patients who were suspected for bloodstream infection defined by blood culture collection presenting at the ED and intravenous antibiotics were initiated during the ED visits. The study period was between 1 January 2016 and 31 December 2018. Clinical data of the eligible patients were retrieved from the ED database. Factors associated with Gram-negative infection were calculated by logistic regression analysis. Results: There were 727 patients at the ED who had positive blood culture for bacteria. Of those, 504 patients (69.33%) had positive blood culture for Gram-negative bacteria. There were three independent factors for Gram-negative infection including sex, solid organ malignancy, and body temperature. The highest adjusted odds ratio (95% confidence interval) was 2.004 (1.330, 3.020) for solid organ malignancy. Conclusions: Gram-negative bacterial infection was more prominent than Gram-positive bacterial infection in patients presenting at the ED (69.33%). Solid organ malignancy, being female, and a high body temperature were independent factors of Gram-negative bacterial infection.
Introduction
Bloodstream infections are common conditions in emergency departments (ED). A study conducted in a national surveillance system revealed that the incidence of such infections was 220 per 100,000 people and had significantly increased by 14% in a 6-year period. [1] Meanwhile, the mortality rate of bloodstream infections was 13.5-23.4% in developed countries and 12.83–28.00% in South Africa, China, and Vietnam. [2,3,4,5,6,7] The mortality rate of bloodstream infections has increased in specific units within hospitals, including neonatal intensive care units, particularly those with central lines, where the mortality rate can be as high as 50%. [8,9,10,11]
Blood cultures are common tools for diagnosing bloodstream infections and related to mortality with adjusted odds ratio (OR) of 1.130 (95% confidence interval [CI]: 1.130, 1.961). [12] The positive blood culture rate among patients with septic shock was 34.2%, 75% of whom had bacteria as a causative pathogen categorized as Gram-negative (56.7%) or Gram-positive (17.8%). [4]
Several predictors for mortality in bloodstream infections have been identified, including age, comorbid disease or neutropenia, and serum procalcitonin. [6,13,14] Studies have also shown that patients with bloodstream infection have had significantly higher levels of serum procalcitonin than ones with negative blood cultures (4.19 vs 1.06 ng/mL; p=0.0116). [14] Causative pathogens are another independent factor of mortality. Enterobacteriaceae infection increased the risk of death by 1.722-fold in patients with bloodstream infections. [6] Different pathogens also have different mortality rates; while the mortality rate of Enterococcus faecalis bacteremia was 21.4%, that of Staphylococcus aureus bacteremia can be up to 30%. [15,16]
Treatment with appropriate antibiotics is crucial for patients with bloodstream infections, particularly in EDs. Therefore, in our study we aimed to identify clinical factors able to predict types of bacterial pathogens in patients with bloodstream infections who presented at an ED, with special focus on Gram-negative bacterial infection due to a higher prevalence of Gram- positive bacteria.
Methods
As part of a project on treating infections in EDs, our retrospective study was conducted in the ED at Khon Kaen University Hospital in Thailand. The study’s protocol was approved by the Ethics Committee in Human Research at Khon Kaen University (No. HE631115). Participants’ informed consent was waived because the study was conducted retrospectively and collected data from medical charts.
To be included in the study, from January 1st, 2016, to December 31st, 2018, patients had to be adults (≥18 years old) suspected of having bloodstream infections following blood culture collection in the ED. All patients had received intravenous antibiotics during their ED visits. Patients were excluded from the study if they had cardiac arrest or trauma, were referred from other hospitals, had previously received antibiotics, had missing clinical data, or had non-bacterial infection.
Blood cultures at the ED were obtained with two bottles of aerobic cultures, and the clinical data of eligible patients were retrieved from the ED’s database. The studied variables were baseline characteristics, comorbid disease, physical signs, sepsis scores (SIRS, qSOFA, and NEWS), and the results of laboratory tests including blood culture. Patient disposition, use of mechanical ventilators and vasopressors, and mortality rate were also studied. The results of blood cultures were categorized as showing either Gram-positive or Gram-negative infection. Pathogens were identified if at least one positive blood culture was of clinical relevance, as previously reported. [6,13,15,16,17]
For statistical analyses, eligible patients were categorized into two groups: Gram-negative and Gram-positive according to the results of blood cultures. Descriptive statistics were used to compare differences in the studied variables between the groups. Numerical data in each group were tested for normal distribution by Shapiro-Wilk test. If data were not normally distributed, Wilcoxon rank sum test was used to evaluate differences between groups. For categorical data, Chi square test was used to compute differences between groups. Z scores by Wilcoxon rank sum test and Chi square values by Chi square test were reported.
Factors associated with Gram-negative infection were calculated in logistic regression analysis, while univariate and multivariate logistic regressions were used to calculate unadjusted and adjusted ORs (95% CI) for each factor. Factors with p values less than 0.20 in univariate logistic regression analysis were submitted to the subsequent stepwise multivariate logistic regression analysis. The final model for predicting Gram-negative infection was tested for goodness of fit by the Hosmer–Lemeshow method. All statistical analyses were performed in Stata version 10.1 (USA).
Results
Of the 731 patients suspected of having bloodstream infections, four were excluded due to lacking bacterial infection (Figure 1). Of the 727 remaining patients at the ED with positive blood cultures for bacteria, 504 (69.33%) had blood cultures positive for Gram-negative bacteria. Four factors between the groups with Gram-positive versus Gram-negative infections were significant (Table 1). The Gram-negative group had a significantly higher proportion of male patients (63.68% vs 52.58%), and moderate to severe chronic kidney disease (16.14% vs 9.92%) than the Gram-negative infection group. The Gram-negative infection group had significantly higher proportion of solid organ malignancy (35.12% vs 23.32%) than the Gram- positive infection group. However, no significant differences arose in the results of laboratory tests, patient disposition, use of mechanical ventilators or vasopressors, or death.
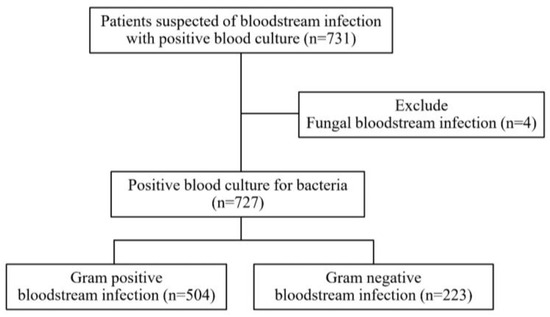
Figure 1.
Study flow chart of patients with bloodstream infection who presented at the emergency department.

Table 1.
Baseline characteristics of patients with bloodstream infection who presented at the emergency department categorized by type of bacterial infection.
The most common Gram-positive and—negative organisms were Staphylococcus aureus (55 patients) and Escherichia coli (272 patients), as shown in Table 2. Five factors remained in the model to predict Gram-negative infection: age, sex, solid organ malignancy, moderate to severe chronic kidney disease, and body temperature (Table 3). Serum lactate was removed from the final model due to stepwise method, three independent factors for Gram-negative infection remained: sex, solid organ malignancy, and body temperature. The highest adjusted OR was 2.004 (95% CI: 1.330, 3.020) for solid organ malignancy. The Hosmer–Lemeshow Chi-square value of the final model was 8.34 (p=0.400).
Table 2.
Top three causative pathogens among patients with bloodstream infection who presented at the emergency department categorized by type of bacterial infection.
Table 3.
Factors remaining in the final predictive model of Gram-negative bacterial infection in patients with bloodstream infection who presented at the emergency department.
Discussion
As previously reported, Gram-negative bacterial infection is more common than Gram- positive bacterial infection. [3] Escherichia coli (69.32%) and Staphylococcus aureus (7.56%) have been reported as the most common Gram- negative and Gram-positive pathogens, respectively. [1,15] In terms of clinical outcomes, patients in our study with Gram-negative versus Gram-positive bacterial infection showed similar results (Table 1). Three factors predicted Gram- negative bacterial infection: sex, solid organ malignancy, and body temperature.
E.coli is the most common pathogen related with urinary tract infection. [13,16] Likewise, we found that female patients were more at risk of Gram-negative bloodstream infection than men by 1.520-fold (Table 3). Of 312,896 patients with urinary tract infection in a study in England, 78.8. were female. [13] Gram-negative bacterial infection has also been more common than Gram-positive bacterial infection in cases of solid organ malignancy. [17]. [18] The proportion of Gram- negative to Gram-positive bacterial infection in our study was 1.85.1 (65%:35%). The primary risk factor of Gram-negative bacterial infection was neutropenia from chemotherapy. [18,19] Solid organ malignancy is also a risk factor for Gram- negative bacterial infection from Achromobacter spp. [20]
Lipopolysaccharide (LPS), produced by Gram-negative bacteria, is a primary factor in inducing immune system and acute inflammatory responses that result in high-grade fever. [21,22] A study in rats revealed that LPS induced fever centrally via a neutrophil chemoattractant that increases prostaglandin E2 in the cerebrospinal fluid and interleukin.6 (IL.6), [23,24] which along with IL.8 mediates fever. [24] Compared with Gram- positive bacteria, Gram-negative bacteria cause more than twice the levels of IL.6 and IL.8 (p<0.001.. [23] Those trends may explain the higher body temperature in cases of Gram-negative than Gram-positive bacterial infection in our study (Table 1). An increase in body temperature by 1 °C increases the risk of Gram-negative bacterial infection by 20%. However, sepsis scores (qSOFA, and NEWS) and lactate level did not significantly impact the differentiation of causative bacterial infection (Table 1). Serum lactate was thus removed from our model as a result of stepwise logistic regression analysis, which indicated that it was not significant compared with other factors remaining in the model.
Predictors of Gram-negative bloodstream infection in our study might have been slightly different from previous studies. Similar to our findings, a study in Taiwan revealed that patients with Gram-negative bacteremia were mostly older adults (62.1% vs 56.9%; p=0.03) and that fewer had chronic kidney disease (15.55% vs 24.9%; p< 0.001) than those with Gram-positive bacteremia. [25] In our study, we had a higher proportion of patients more than 55 years old (74.01% vs 71.30%; p=0.468) and a lower proportion of patients with moderate to severe chronic kidney disease (9.92% vs 16.14%; p=0.024) in the Gram-negative than in the Gram- positive group. However, those two factors were not significant after being adjusted for other factors (Table 3). In previous research, those two factors were not adjusted, which may mean that their results are less reliable than ours. Another study conducted among patients who inject drugs revealed that being more than 50 years old had an adjusted OR of 2.9 (95% CI: 1.2, 7.2), whereas we did not find any significant result for older age (adjusted OR=1.008; 95% CI: 0.996, 1.021). [26] The higher risk of Gram-negative bacteria infection among older patients who inject drugs may be due to injection techniques that risk Gram-negative bloodstream infection. [26] Therefore, the different results for age as a predictor for Gram-negative infection between the studies may be due to differences in the study populations. None of the patients in our study reported using or receiving drugs intravenously (Table 1).
Our findings have some limitations. First, our study was conducted in a tertiary referral university hospital, meaning that the results should be generalized to other clinical situations with caution. Second, we exclusively enrolled patients with bloodstream bacterial infections. Last, due to the study’s retrospective design, some information may have been missing or not examined (e.g., lactate level and albuminuria in chronic kidney disease). [27,28]
Conclusions
Gram-negative bacterial infection was more prominent than Gram-positive bacterial infection among patients who presented at the ED (69.33%). Solid organ malignancy, being female, and high body temperature were independent factors for Gram-negative bacterial infection.
Author Contributions
Conceptualization: PP and KS. Methodology: PP, KA. Validation: PP, KI and WB. Formal analysis: PP and KS. Investigation: PP. Resources: PP, NL and SS. Data curation: PP. Writing—original draft preparation: PP. Writing—review and editing: KS. Supervision: KS. All authors have read and approved the final version of the manuscript.
Funding
None to declare.
Conflicts of interest
All authors—none to declare.
References
- Buetti N, Atkinson A, Marschall J, Kronenberg A, Swiss Centre for Antibiotic Resistance (ANRESIS). Incidence of bloodstream infections: A nationwide surveillance of acute care hospitals in Switzerland 2008-2014. BMJ Open 2017, 7, e013665. [Google Scholar] [CrossRef]
- Hattori, H.; Maeda, M.; Nagatomo, Y.; et al. Epidemiology and risk factors for mortality in bloodstream infections: A single-center retrospective study in Japan. Am J Infect Control 2018, 46, e75–e79. [Google Scholar] [CrossRef]
- Goto, M.; Al-Hasan, M.N. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin Microbiol Infect 2013, 19, 501–509. [Google Scholar] [CrossRef]
- Corcione, S.; Angilletta, R.; Raviolo, S.; et al. Epidemiology and risk factors for mortality in bloodstream infection by CP-Kp, ESBL-E, Candida and CDI: A single center retrospective study. Eur J Intern Med 2018, 48, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.; Zhao, C.; Li, H.; Wang, R.; Wang, Q.; Wang, H. Clinical profile, prognostic factors, and outcome prediction in hospitalized patients with bloodstream infection: Results from a 10-year prospective multicenter study. Front Med (Lausanne) 2021, 8, 629671. [Google Scholar] [CrossRef] [PubMed]
- Dat, V.Q.; Long, N.T.; Hieu, V.N.; et al. Clinical characteristics, organ failure, inflammatory markers and prediction of mortality in patients with community acquired bloodstream infection. BMC Infect Dis 2018, 18, 535. [Google Scholar] [CrossRef] [PubMed]
- Reddy, K.; Bekker, A.; Whitelaw, A.C.; Esterhuizen, T.M.; Dramowski, A. A retrospective analysis of pathogen profile, antimicrobial resistance and mortality in neonatal hospital-acquired bloodstream infections from 2009-2018 at Tygerberg Hospital, South Africa. PLoS ONE 2021, 16, e0245089. [Google Scholar] [CrossRef]
- Russotto, V.; Cortegiani, A.; Graziano, G.; et al. Bloodstream infections in intensive care unit patients: Distribution and antibiotic resistance of bacteria. Infect Drug Resist 2015, 8, 287–296. [Google Scholar] [CrossRef]
- Singhal, T.; Shah, S.; Thakkar, P.; Naik, R. The incidence, aetiology and antimicrobial susceptibility of central line- associated bloodstream infections in intensive care unit patients at a private tertiary care hospital in Mumbai, India. Indian J Med Microbiol 2019, 37, 521–526. [Google Scholar] [CrossRef]
- Mishra, S.B.; Misra, R.; Azim, A.; et al. Incidence, risk factors and associated mortality of central line-associated bloodstream infections at an intensive care unit in northern India. Int J Qual Health Care 2017, 29, 63–67. [Google Scholar] [CrossRef]
- Johnson, J.; Robinson, M.L.; Rajput, U.C.; et al. High burden of bloodstream infections associated with antimicrobial resistance and mortality in the neonatal intensive care unit in Pune, India. Clin Infect Dis 2021, 73, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.J.; Li, D.; Zhao, Q.; et al. Incidence, risk factors and impact on outcomes of secondary infection in patients with septic shock: An 8-year retrospective study. Sci Rep 2016, 6, 38361. [Google Scholar] [CrossRef] [PubMed]
- Gharbi, M.; Drysdale, J.H.; Lishman, H.; et al. Antibiotic management of urinary tract infection in elderly patients in primary care and its association with bloodstream infections and all cause mortality: Population based cohort study. BMJ 2019, 364, 364–1525. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.L.; Kramer, N.; Stead, T.G.; et al. Serum procalcitonin level is associated with positive blood cultures, in-hospital mortality, and septic shock in emergency department sepsis patients. Cureus 2020, 12, e7812. [Google Scholar] [CrossRef]
- Cheung, Y.; Ko, S.; Wong, O.F.; Lam, H.S.B.; Ma, H.M.; Lit, C.H.A. Clinical experience in management of bloodstream infection in emergency medical ward: A preliminary report. Hong Kong J Emerg Med 2021, 28, 215–226. [Google Scholar] [CrossRef]
- Linhares, S.G.; Pereira, J.C.; Fernades, P.M.; de Campos, J.R. Functional exercise capacity and lung function in patients undergoing an early rehabilitation program after the Nuss procedure: A randomized controlled trial. Pediatr Surg Int 2017, 33, 69–74. [Google Scholar] [CrossRef]
- Samonis, G.; Vardakas, K.Z.; Maraki, S.; et al. A prospective study of characteristics and outcomes of bacteremia in patients with solid organ or hematologic malignancies. Support Care Cancer 2013, 21, 2521–2526. [Google Scholar] [CrossRef]
- Osmani, A.H.; Jabbar, A.A.; Gangwani, M.K.; Hassan, B. Outcomes of high risk patients with febrile neutropenia at a tertiary care center. Asian Pac J Cancer Prev 2017, 18, 2741–2745. [Google Scholar]
- Al-Otaibi, F.E.; Bukhari, E.E.; Badr, M.; Alrabiaa, A.A. Prevalence and risk factors of Gram-negative bacilli causing blood stream infection in patients with malignancy. Saudi Med J 2016, 37, 979–984. [Google Scholar] [CrossRef]
- Swenson, C.E.; Sadikot, R.T. Achromobacter respiratory infections. Ann Am Thorac Soc 2015, 12, 252–258. [Google Scholar] [CrossRef]
- Snell, E.S. Gram-negative bacterial endotoxin and the pathogenesis of fever. Prog Drug Res 1975, 19, 402–411. [Google Scholar] [CrossRef]
- Matsuguchi, T. Mast cells as critical effectors of host immune defense against Gram-negative bacteria. Curr Med Chem 2012, 19, 1432–1442. [Google Scholar] [CrossRef]
- Yamashiro, L.H.; de Souza, G.E.P.; de Melo Soares, D. Role of CINC-1 and CXCR2 receptors on LPS-induced fever in rats. Pflugers Arch 2019, 471, 301–311. [Google Scholar] [CrossRef]
- Engel, A.; Kern, W.V.; Mürdter, G.; Kern, P. Kinetics and correlation with body temperature of circulating interleukin-6, interleukin-8, tumor necrosis factor alpha and interleukin-1 beta in patients with fever and neutropenia. Infection 1994, 22, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Lee, C.H.; Hsieh, C.C.; Hong, M.Y.; Chen, M.J.; Lee, C.C. Differential effects of inappropriate empirical antibiotic therapy in adults with community-onset gram- positive and gram-negative aerobe bacteremia. J Infect Chemother 2020, 26, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.C.; Yeager, S.D.; Shorman, M.A.; Wright, L.R.; Veve, M.P. Incidence and predictors of gram-negative bacilli in hospitalized people who inject drugs with injection drug use-attributable infections. Antimicrob Agents Chemother 2021, 65, e0092521. [Google Scholar] [CrossRef] [PubMed]
- Charoentanyarak, S.; Sawunyavisuth, B.; Deepai, S.; Sawanyawisuth, K. A point-of-care serum lactate level and mortality in adult sepsis patients: A community hospital setting. J Prim Care Community Health 2021, 12, 21501327211000230. [Google Scholar] [CrossRef]
- Jeerasuwannakul, B.; Sawunyavisuth, B.; Khamsai, S.; Sawanyawisuth, K. Prevalence and risk factors of proteinuria in patients with type 2 diabetes mellitus. Asia Pac J Sci Technol 2021, 26, APST–26. [Google Scholar]


© GERMS 2022.