
Understanding the Impacts of Healing Agents on the Properties of Fresh and Hardened Self-Healing Concrete: A Review



Abstract
1. Introduction
2. Novel Self-Healing Agents
- (1)
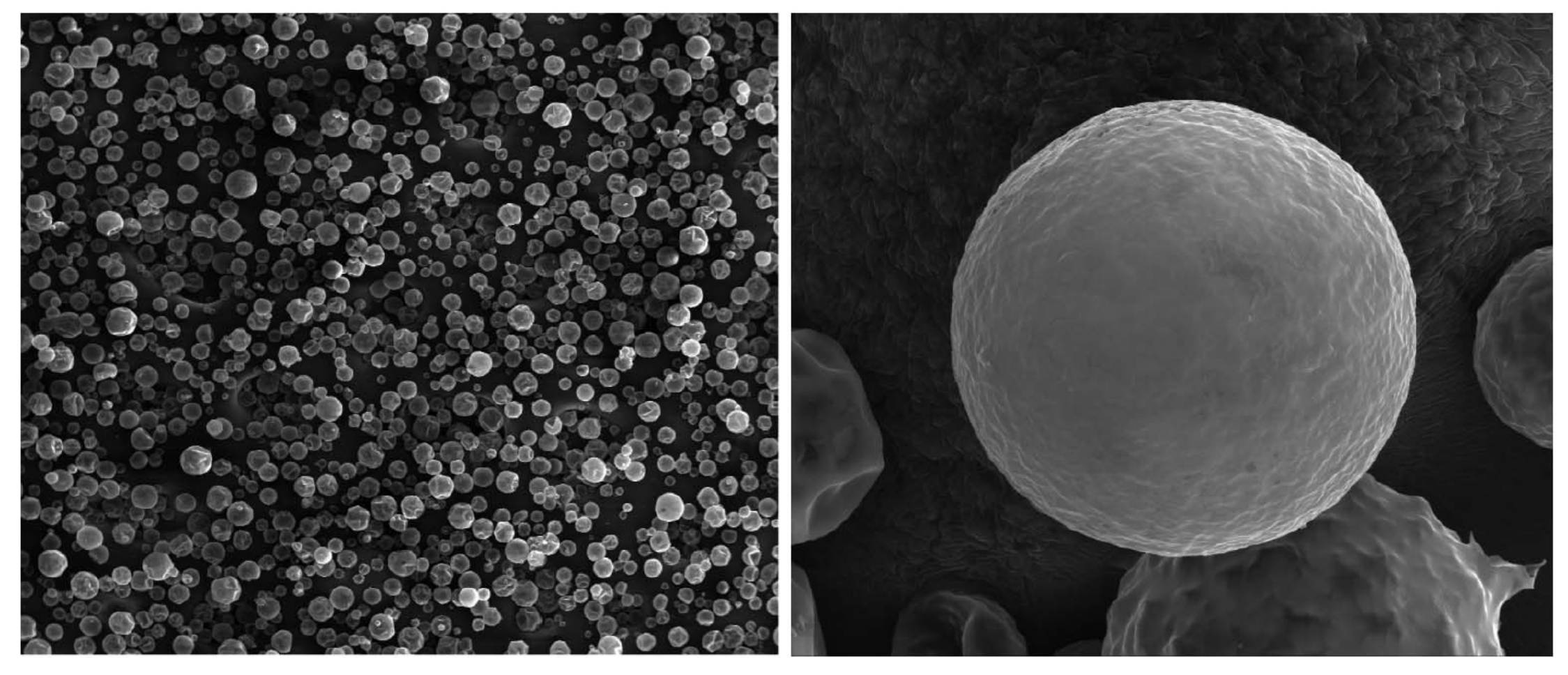
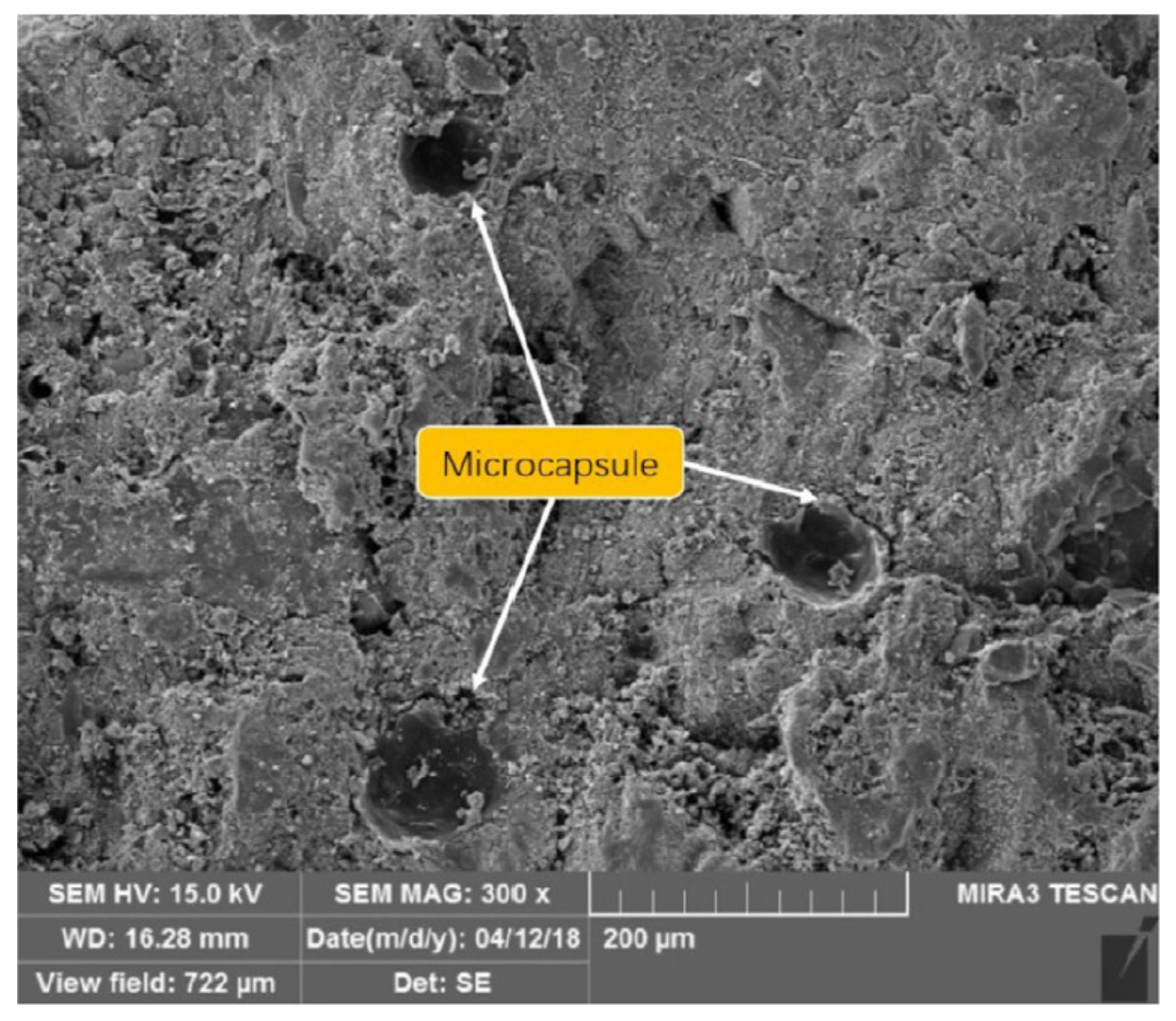
- Microcapsules have a nominal size of no more than 1 mm and are produced with a variety of production methods (i.e., interfacial polymerization, in situ polymerization, spray drying, ionic gelatin and complex coacervation–as discussed by Kanellopoulos et al. [18]). Table 1 shows the different types of microcapsules which have been successfully applied in concrete. Morphologically, microcapsules have mostly a spherical shape, as shown in Figure 4. The production of microcapsules has to be carefully performed because many parameters may change the physical properties of the final product. Three important design parameters of interest are capsule size/diameter, shell thickness and surface texture [41]. Other parameters such as type of formation, materials and volume will certainly affect the size distribution. The size of microcapsules significantly affects self-healing efficacy. Comparing the same amount of healing agent in smaller or larger capsules, smaller microcapsules open the possibility to heal more scattered cracks due to their high distribution inside the matrix, while larger microcapsules carry more healing agents that may cover a larger healed area, which are effective to seal wider cracks and can simultaneously heal smaller cracks in a nearby region. Hence, it is still unclear what would be the best size of the microcapsules in order to achieve optimal self-healing performance. In general, thin-walled microcapsules would fail during the production process and concrete mixing, while thick-walled microcapsules are reluctant to break as the propagated crack will hardly penetrate [17]. The morphology, size and shape of prepared microcapsules are dependent on numerous factors including temperature, pH and agitation rate [17,18,42,43]. The microcapsules are typically stored in the preserving solution to prevent shrinkage and the premature hardening of microcapsules as may occur in the dry condition. To incorporate the microcapsules in the concrete, direct addition during the mixing stage is done in numerous studies.
- (2)
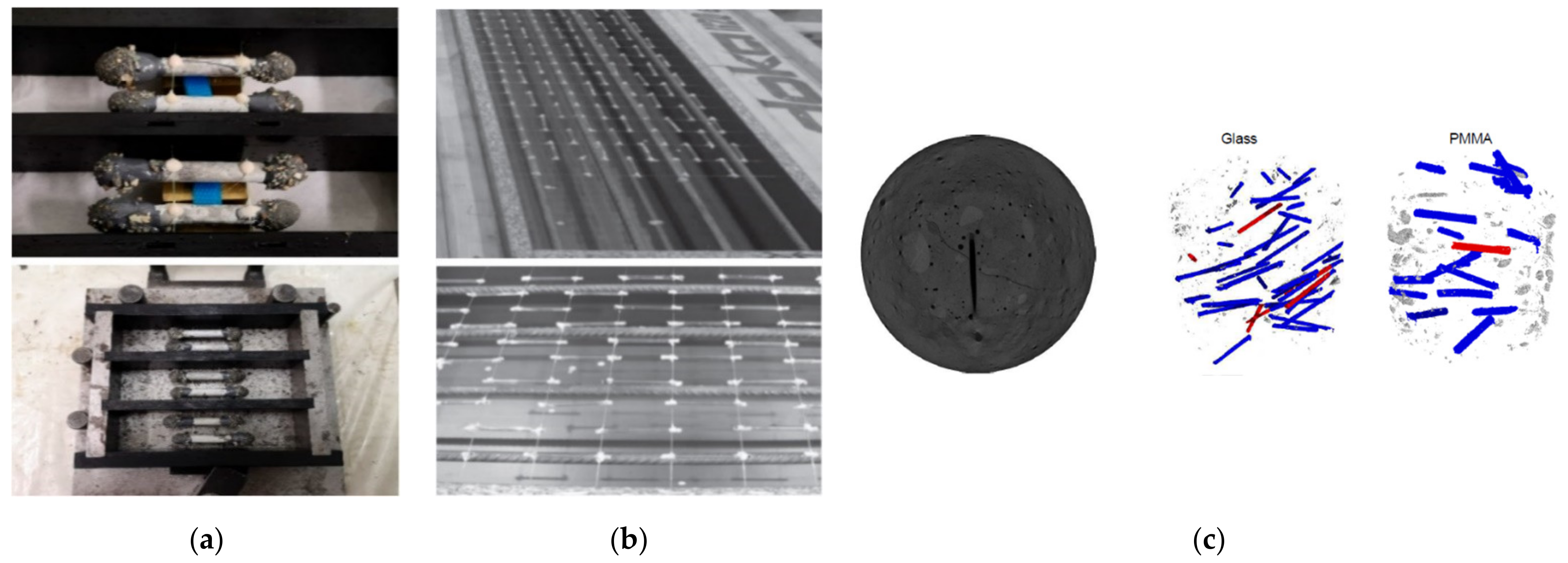
- Macrocapsules are literally bigger in size (>1 mm) and can store a larger amount of healing agents than microcapsules. Macrocapsules are commercially available, such as borosilicate glass or ceramic capsules which are cut from a long tube, or the capsules can be manufactured by means of an extruder through an extrusion process [22,23,44]. Table 2 presents the various types of capsules used in the application of self-healing concrete. The physical appearance of some cylindrical capsules is shown in Figure 5. Glass capsules could affect negatively the concrete durability due to the undesired alkali-silica reaction (ASR) [45,46], while polymeric capsules could cause premature curing of an entrapped agent such as PU [44]. To avoid these drawbacks, ceramic capsules [47] and cementitious capsules [22,23,24,25] were successfully experimented. To incorporate the capsules into the concrete, other aspects such as capsule dimensions (i.e., diameter, thickness and length) also play an important role in the self-healing scenario because the capsule should be able to break when a crack propagates. Thin-walled capsules are effective for capsule breakage during cracking of the concrete as they are relatively fragile; however, they would fail when the capsules are added during the mixing. Conversely, thick-walled capsules are highly resistant to withstand mixing forces, but they are reluctant to break as the propagated crack will hardly penetrate through the planar surface of the capsules and this might lead to a lower self-healing efficiency. The same problem occurs with the length of capsules. Short capsules may cause a slip when a crack appears, while long capsules will be more difficult to be incorporated into the concrete because of the interaction with aggregates which will disturb the packing system. Thus, the optimal design of macrocapsules remains an interesting topic of research. To authors’ knowledge, there are two methodologies to incorporate macrocapsules in concrete mixes, namely manual placement and direct addition. In the first method, the most practical application is manually placing the capsules in the cover zone of mortar/concrete (as shown in Figure 5a,b), while in the second method, a previous work [46] attempted to incorporate the capsules directly into the fresh mixture during the mixing stage. The random distribution of mixed-in capsules was observed in the hardened concrete core, as shown in Figure 5c.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. | Production Method | Microcapsule Shell | Cargo | Capsule Diameter (μm) | Shell Thickness (μm) | Remarks |
|---|---|---|---|---|---|---|
| [42] | In situ polymerization | Polyurethane/urea-formaldehyde | Sodium silicate | Not specified | Not specified | Spherical double-walled microcapsules with rough surface |
| [41] | Interfacial polymerization | Polyurethane | Sodium silicate | Not specified | Not specified | Self-synthesized microcapsules with rough surface |
| [18,50] | Complex coacervation | Gelatin/gum Arabic shell | Sodium silicate | 290 | 5–20 | Microcapsules with the shape of “rugby-ball” which have switchable mechanical properties |
| [19] | In situ polymerization | Urea-formaldehyde | Epoxy resin | 45–185 | 5.46 | Spherical-shaped organic microcapsules that can produce ductility for the cementitious composites |
| [51] | In situ polymerization | Urea-formaldehyde | Epoxy resin | 110–190 | Not specified | Round-shaped microcapsules with non-smooth surface which has a good thermal stability |
| [52] | In situ polymerization | Urea-formaldehyde | Calcium nitrate | 22–59 | Not specified | Smooth surface and non-porous texture |
| [48] | In situ polymerization | Urea-formaldehyde | Calcium nitrate | 22–109 | Not specified | Smooth exterior surface coated with Span60 emulsifier |
| [43] | In situ polymerization | Urea-formaldehyde | Calcium nitrate | 41–107 | 0.60–1.31 | Spherical-shaped microcapsules with smooth exterior surface and rough interior surface |
| [53] | In situ polymerization | Urea-formaldehyde | Dicyclopentadiene | 80–600 | 0.20–0.25 | Rough permeable outer layer and smooth interior shell free of cavities; more uniform |
| Ref. | Type of Composite | Specimen Size (mm) | Macrocapsules | Cargo | Dosage of Capsules | Placement Method | Remarks | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Shell | OD (mm) | ID (mm) | Length (mm) | Coat | |||||||
| [49] | SR-SCC | 150 × 250 × 3000 | Glass | 3.35 | 3 | 50 | - | PU | 350 capsules/beam | Manual | Capsules started to break when the crack width amounted to 50 μm. |
| [46] | SR-SCC | 200 × 400 × 2500 | PMMA | 6.5 | 5.1 | 50 | - | WRA | 22 capsules/L of concrete | Direct addition | Survival probability of the PMMA capsules increased as the wall thickness of the capsules increased. Capsules were able to rupture at crack width of 116 μm. |
| SR-SCC | 200 × 400 × 2500 | Glass | 5 | 3.4 | 50 | - | WRA | 22 capsules/L of concrete | Direct addition | Good survivability with the thicker capsule and more uniform distribution using glass capsules. Capsules were able to rupture at a crack width of 30 μm. | |
| [47] | FRC | 100 × 100 × 650 | Glass, ceramic | Not specified | 3 | 60, 400 | Mortar layer, cement paste bar | PU | Not specified | Manual, direct addition | Capsules broke during the mixing stage, while they remained intact when the capsules were placed manually using wire. |
| [44] | TC | 120 × 120 × 500 | Glass | 2.3 | 1.7 | 25, 50 | Ethyl cellulose | PU | 2% v/v | Direct addition | The dip-coated capsules showed a higher survivability than uncoated capsules. Capsules were able to rupture at a crack width of 400 μm. |
| Mortar | 40 × 40 × 160 | Ethyl cellulose | 5 | 3 | 50 | - | PU | 2 capsules/prism | Manual | Some capsules were not broken after complete cracking and polymeric capsules showed an incompatibility issue that the stored healing agent is prematurely cured inside the capsule. | |
| [55] | Mortar | 50 × 50 × 220 | Glass | 7.05 | 6.15 | 50 | Thin PVC film | TEOS, SS, CS, C | 2 capsules/prism | Manual | Capsules and its corresponding cargo could survive in a high pH solution (pH = 12) similar to cement, except cyanoacrylate which started to harden within 4 days after encapsulation. |
| [20] | Mortar | 40 × 40 × 160 | Polymers–PLA, PS, P(MMA/n-BMA | 5 | 3 | 50, 100 | - | Water | 2–4 capsules/prism | Manual, direct addition | Moderate resistance during mixing stage. P(MMA/n-BMA) capsules showed a high brittleness and they ruptured when subjected to relatively small deformation. |
| [23] | Mortar | 40 × 40 × 160 | Cementitious | 10 | 7.5 | 50 | Epoxy | WRA, PU, bacteria | 1–2 capsules/prism | Manual | Cementitious capsules were able to sequester and release the healing agents. They showed a good protection between agents and harsh environment of the matrix. |
3. Comparative Study on the Inclusion of Self-Healing Agents into the Concrete Mix
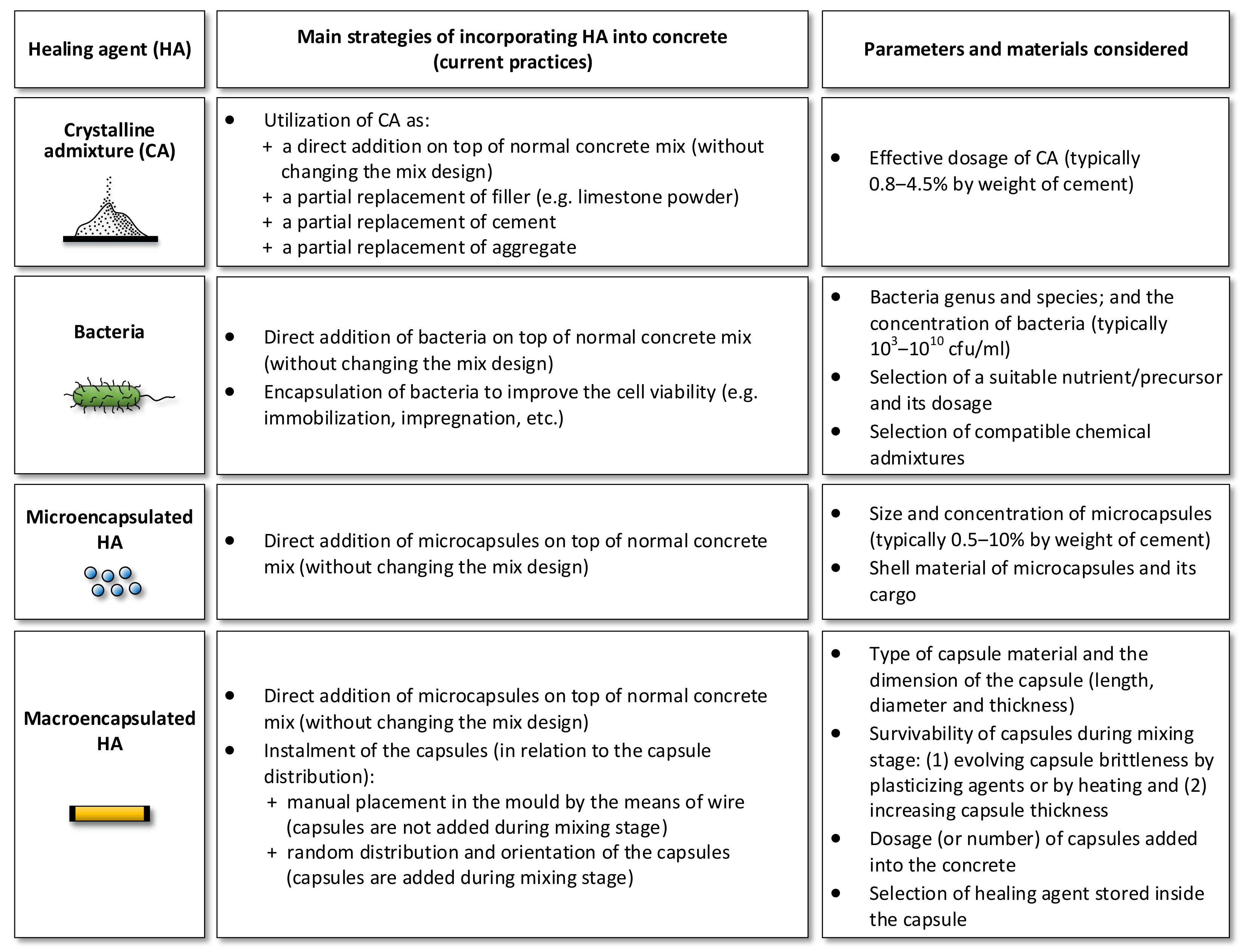
- The main strategies of incorporating healing agent with or without capsules into the self-healing concrete mixes, as described in Figure 6;
- Effect of addition of healing agents on the properties of fresh and hardened concrete before healing (especially for micro- and macro-encapsulated agents, these properties will be evaluated based on the physical presence of capsules in the concrete matrix);
- Brief evaluation of self-healing phenomenon in the cracked concrete after healing (Note: the term of healing efficiency/ratio refers to the crack width reduction or crack closure by microscopic investigation, while the sealing efficiency/ratio is determined by permeability test). Testing methods to evaluate self-healing/sealing capacity of the concrete will not be addressed in this review, but can be found in [56].
3.1. Effects of CA on Concrete Properties
3.1.1. Properties of the Fresh Concrete Mixture
3.1.2. Properties of the Hardened Concrete
3.1.3. Self-Healing Properties
3.2. Effects of Bacteria on Concrete Properties
3.2.1. Properties of the Fresh Concrete Mixture
3.2.2. Properties of the Hardened Concrete
3.2.3. Self-Healing Properties
3.3. Effects of Micro-Encapsulated Agent on Concrete Properties
3.3.1. Properties of the Fresh Concrete Mixture
3.3.2. Properties of the Hardened Concrete
3.3.3. Self-Healing Properties
3.4. Effects of Macro-Encapsulated Agent on Concrete Properties
3.4.1. Properties of the Fresh Concrete Mixture
3.4.2. Properties of the Hardened Concrete
3.4.3. Self-Healing Properties
4. Conclusions
- (1)
- There is still no clear explanation regarding the workability of concrete due to the addition of healing agents. Some studies claimed that the addition of CA, bacteria or capsules did not show negative effects on the workability, while other studies argued that they contributed to a longer setting time, loss of plasticity, higher air content and a decrease in slump value. Consequently, there is a need to further investigate the consistency and workability of self-healing concrete and understand the underlying mechanisms leading to the changes and formulate mitigation plans.
- (2)
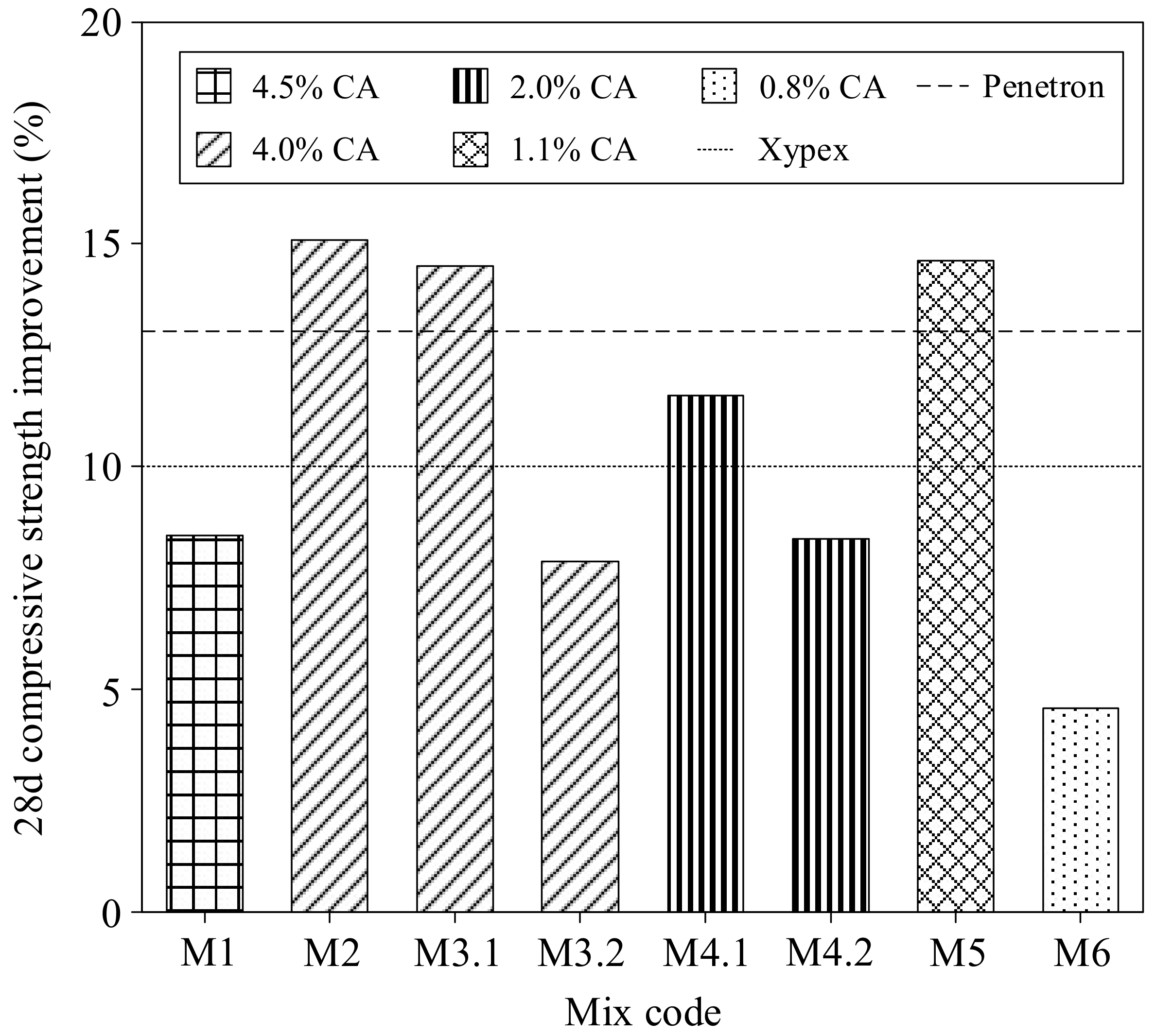
- The addition of CA and bacteria with suitable nutrients generally enhances the compressive strength of concrete composites. This may be attributed to: (1) the filling and water-barrier effects of CA as well as the role of CA as hydration activator to promote the further densification of the concrete microstructure and (2) pores clogging phenomenon by microbial calcite precipitation leading to a denser microstructure and the notable effect of suitable nutritional admixtures to react and help producing more CaCO3-based materials.
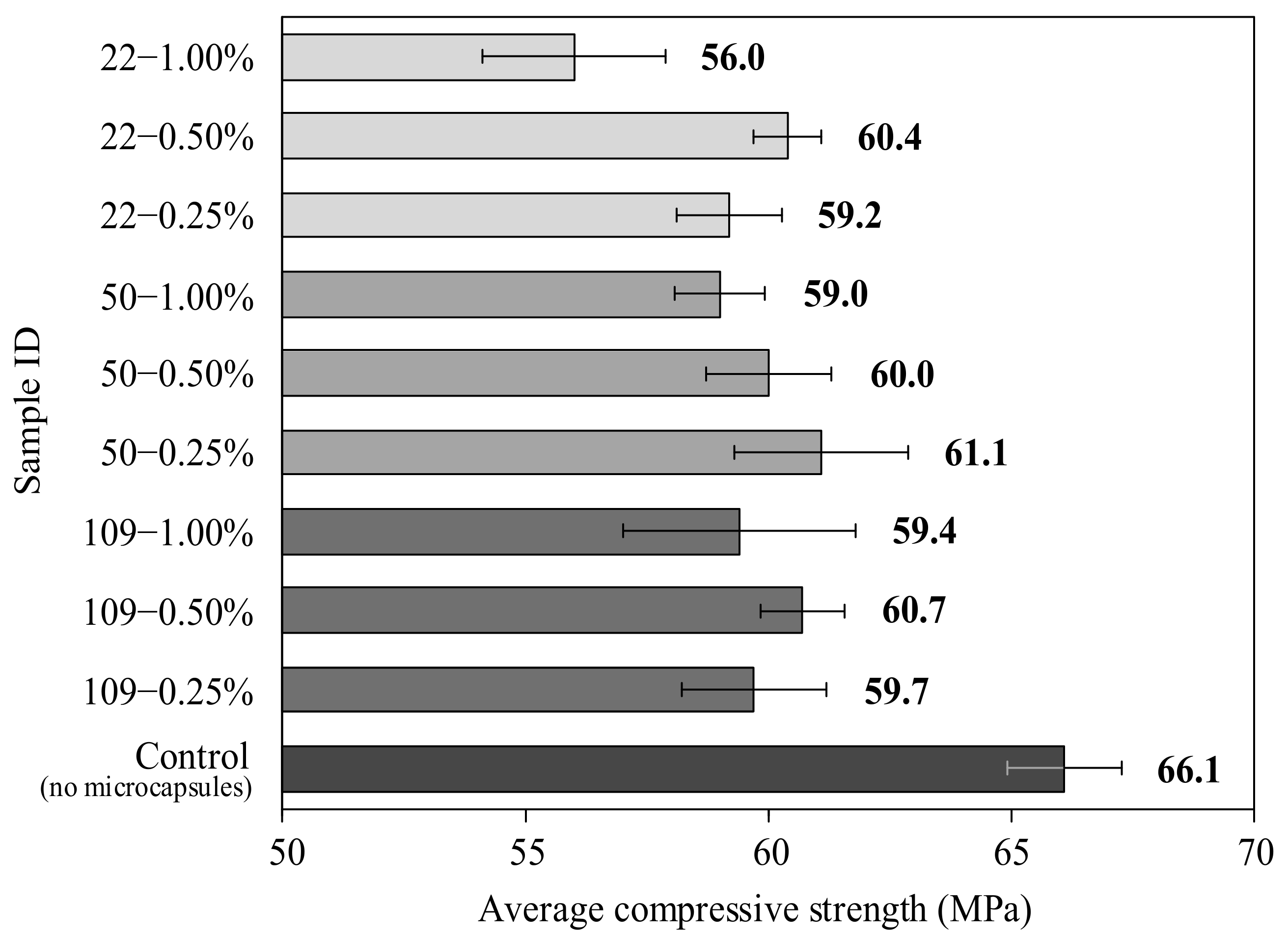
- (3)
- The incorporation of microcapsules caused a steep decrease of the strength value due to the high pore volume as a result of capsules presence inside the concrete matrix. The properties of the hardened concrete with macrocapsules are still not well understood, while, in fact, the presence of macrocapsules may disturb the packing of aggregates.
- (4)
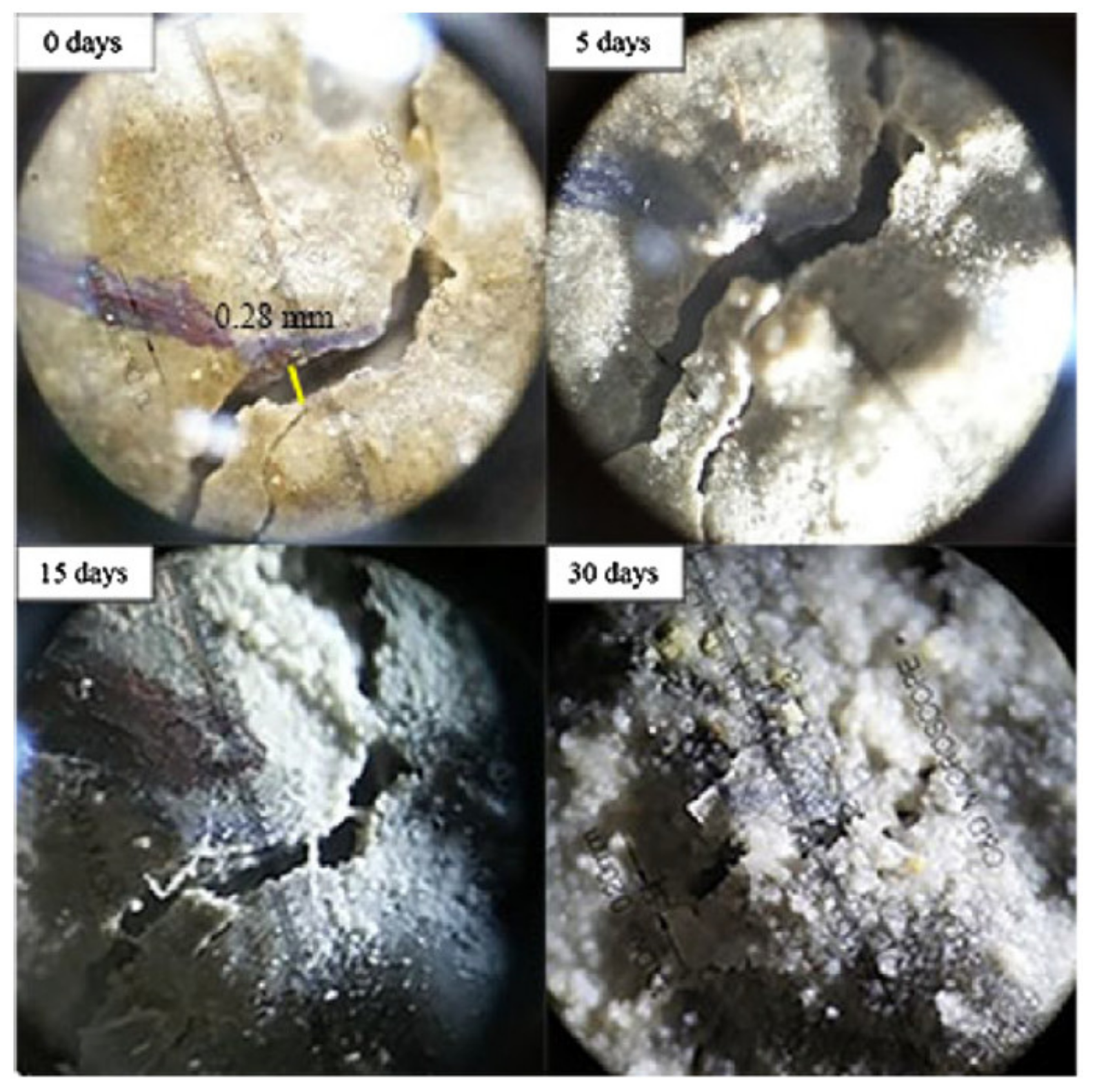
- The inclusion of healing agents demonstrates adequate healing capabilities to a great extent and the durability performance of self-healing concrete is remarkably improved upon healing activation.
Author Contributions
Funding

Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ACI Committee 212. Report on Chemical Admixtures for Concrete; American Concrete Institute: Farmington Hills, MI, USA, 2010; Volume 1, pp. 1–6. [Google Scholar]
- Sisomphon, K.; Copuroglu, O.; Koenders, E.A.B. Self-healing of surface cracks in mortars with expansive additive and crystalline additive. Cem. Concr. Compos. 2012, 34, 566–574. [Google Scholar] [CrossRef]
- Li, D.; Chen, B.; Chen, X.; Fu, B.; Wei, H.; Xiang, X. Synergetic effect of superabsorbent polymer (SAP) and crystalline admixture (CA) on mortar macro-crack healing. Constr. Build. Mater. 2020, 247, 118521. [Google Scholar] [CrossRef]
- García-Vera, V.E.; Tenza-Abril, A.J.; Saval, J.M.; Lanzón, M. Influence of crystalline admixtures on the short-term behaviour of mortars exposed to sulphuric acid. Materials 2018, 12, 82. [Google Scholar] [CrossRef]
- Ferrara, L.; Krelani, V.; Moretti, F. On the use of crystalline admixtures in cement based construction materials: From porosity reducers to promoters of self healing. Smart Mater. Struct. 2016, 25, 1–17. [Google Scholar] [CrossRef]
- Jonkers, H.M.; Thijssen, A.; Muyzer, G.; Copuroglu, O.; Schlangen, E. Application of bacteria as self-healing agent for the development of sustainable concrete. Ecol. Eng. 2010, 36, 230–235. [Google Scholar] [CrossRef]
- Palin, D.; Wiktor, V.; Jonkers, H.M. A bacteria-based bead for possible self-healing marine concrete applications. Smart Mater. Struct. 2016, 25, 084008. [Google Scholar] [CrossRef]
- Palin, D.; Wiktor, V.; Jonkers, H.M. A bacteria-based self-healing cementitious composite for application in low-temperature marine environments. Biomimetics 2017, 2, 13. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Mignon, A.; Trenson, G.; Van Vlierberghe, S.; Boon, N.; De Belie, N. A chitosan based pH-responsive hydrogel for encapsulation of bacteria for self-sealing concrete. Cem. Concr. Compos. 2018, 93, 309–322. [Google Scholar] [CrossRef]
- Seifan, M.; Sarmah, A.K.; Samani, A.K.; Ebrahiminezhad, A.; Ghasemi, Y.; Berenjian, A. Mechanical properties of bio self-healing concrete containing immobilized bacteria with iron oxide nanoparticles. Appl. Microbiol. Biotechnol. 2018, 102, 4489–4498. [Google Scholar] [CrossRef] [PubMed]
- Alazhari, M.; Sharma, T.; Heath, A.; Cooper, R.; Paine, K. Application of expanded perlite encapsulated bacteria and growth media for self-healing concrete. Constr. Build. Mater. 2018, 160, 610–619. [Google Scholar] [CrossRef]
- Wu, M.; Hu, X.; Zhang, Q.; Cheng, W.; Xue, D.; Zhao, Y. Application of bacterial spores coated by a green inorganic cementitious material for the self-healing of concrete cracks. Cem. Concr. Compos. 2020, 113, 103718. [Google Scholar] [CrossRef]
- Mondal, S.; Ghosh, A.D. Investigation into the optimal bacterial concentration for compressive strength enhancement of microbial concrete. Constr. Build. Mater. 2018, 183, 202–214. [Google Scholar] [CrossRef]
- Pei, R.; Liu, J.; Wang, S.; Yang, M. Use of bacterial cell walls to improve the mechanical performance of concrete. Cem. Concr. Compos. 2013, 39, 122–130. [Google Scholar] [CrossRef]
- Schreiberová, H.; Bílý, P.; Fládr, J.; Šeps, K.; Chylík, R.; Trtík, T. Impact of the self-healing agent composition on material characteristics of bio-based self-healing concrete. Case Stud. Constr. Mater. 2019, 11, e00250. [Google Scholar] [CrossRef]
- White, S.R.; Sottos, N.R.; Geubelle, P.H.; Moore, J.S.; Kessler, M.R.; Sriram, S.R.; Brown, E.N.; Viswanathan, S. Autonomic healing of polymer composites. Nature 2001, 409, 794–817. [Google Scholar] [CrossRef] [PubMed]
- Giannaros, P.; Kanellopoulos, A.; Al-Tabbaa, A. Sealing of cracks in cement using microencapsulated sodium silicate. Smart Mater. Struct. 2016, 25, 1–12. [Google Scholar] [CrossRef]
- Kanellopoulos, A.; Giannaros, P.; Palmer, D.; Kerr, A.; Al-Tabbaa, A. Polymeric microcapsules with switchable mechanical properties for self-healing concrete: Synthesis, characterisation and proof of concept. Smart Mater. Struct. 2017, 26, 045025. [Google Scholar] [CrossRef]
- Wang, X.; Sun, P.; Han, N.; Xing, F. Experimental study on mechanical properties and porosity of organic microcapsules based self-healing cementitious composite. Materials 2017, 10, 20. [Google Scholar] [CrossRef] [PubMed]
- Hilloulin, B.; Van Tittelboom, K.; Gruyaert, E.; De Belie, N.; Loukili, A. Design of polymeric capsules for self-healing concrete. Cem. Concr. Compos. 2015, 55, 298–307. [Google Scholar] [CrossRef]
- Van Tittelboom, K.; De Belie, N.; Van Loo, D.; Jacobs, P. Self-healing efficiency of cementitious materials containing tubular capsules filled with healing agent. Cem. Concr. Compos. 2011, 33, 497–505. [Google Scholar] [CrossRef]
- Anglani, G.; Tulliani, J.M.; Antonaci, P. Behaviour of pre-cracked self-healing cementitious materials under static and cyclic loading. Materials 2020, 13, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Anglani, G.; Van Mullem, T.; Zhu, X.; Wang, J.; Antonaci, P.; De Belie, N.; Tulliani, J.-M.; Van Tittelboom, K. Sealing efficiency of cement-based materials containing extruded cementitious capsules. Constr. Build. Mater. 2020, 251, 119039. [Google Scholar] [CrossRef]
- Formia, A.; Terranova, S.; Antonaci, P.; Pugno, N.M.; Tulliani, J.M. Setup of extruded cementitious hollow tubes as containing/releasing devices in self-healing systems. Materials 2015, 8, 1897–1923. [Google Scholar] [CrossRef] [PubMed]
- Formia, A.; Irico, S.; Bertola, F.; Canonico, F.; Antonaci, P.; Pugno, N.M.; Tulliani, J.-M. Experimental analysis of self-healing cement-based materials incorporating extruded cementitious hollow tubes. J. Intell. Mater. Syst. Struct. 2016, 27, 2633–2652. [Google Scholar] [CrossRef]
- Park, B.; Choi, Y.C. Self-healing capability of cementitious materials with crystalline admixtures and super absorbent polymers (SAPs). Constr. Build. Mater. 2018, 189, 1054–1066. [Google Scholar] [CrossRef]
- Xue, C.; Li, W.; Qu, F.; Sun, Z.; Shah, S.P. Self-healing efficiency and crack closure of smart cementitious composite with crystalline admixture and structural polyurethane. Constr. Build. Mater. 2020, 260, 119955. [Google Scholar] [CrossRef]
- Pazderka, J.; Hájková, E. Crystalline admixtures and their effect on selected properties of concrete. Acta. Polytech. 2016, 56, 306–311. [Google Scholar] [CrossRef]
- Jafarnia, M.S.; Khodadad Saryazdi, M.; Moshtaghioun, S.M. Use of bacteria for repairing cracks and improving properties of concrete containing limestone powder and natural zeolite. Constr. Build. Mater. 2020, 242, 118059. [Google Scholar] [CrossRef]
- Andalib, R.; Abd Majid, M.Z.; Hussin, M.W.; Ponraj, M.; Keyvanfar, A.; Mirza, J.; Lee, H.-S. Optimum concentration of Bacillus megaterium for strengthening structural concrete. Constr. Build. Mater. 2016, 118, 180–193. [Google Scholar] [CrossRef]
- Madhu Sudana Reddy, B.; Revathi, D. An experimental study on effect of Bacillus sphaericus bacteria in crack filling and strength enhancement of concrete. Mater. Today Proc. 2019, 19, 803–809. [Google Scholar] [CrossRef]
- Vijay, K.; Murmu, M. Self-repairing of concrete cracks by using bacteria and basalt fiber. SN Appl. Sci. 2019, 1, 1–10. [Google Scholar] [CrossRef]
- Khaliq, W.; Ehsan, M.B. Crack healing in concrete using various bio influenced self-healing techniques. Constr. Build. Mater. 2016, 102, 349–357. [Google Scholar] [CrossRef]
- Nguyen, T.H.; Ghorbel, E.; Fares, H.; Cousture, A. Bacterial self-healing of concrete and durability assessment. Cem. Concr. Compos. 2019, 104, 103340. [Google Scholar] [CrossRef]
- Siddique, R.; Jameel, A.; Singh, M.; Barnat-Hunek, D.; Aït-Mokhtar, A.; Belarbi, R.; Rajor, A. Effect of bacteria on strength, permeation characteristics and micro-structure of silica fume concrete. Constr. Build. Mater. 2017, 142, 92–100. [Google Scholar] [CrossRef]
- Chahal, N.; Siddique, R.; Rajor, A. Influence of bacteria on the compressive strength, water absorption and rapid chloride permeability of fly ash concrete. Constr. Build. Mater. 2012, 28, 351–356. [Google Scholar] [CrossRef]
- Chahal, N.; Siddique, R.; Rajor, A. Influence of bacteria on the compressive strength, water absorption and rapid chloride permeability of concrete incorporating silica fume. Constr. Build. Mater. 2012, 37, 645–651. [Google Scholar] [CrossRef]
- Ameri, F.; Shoaei, P.; Bahrami, N.; Vaezi, M.; Ozbakkaloglu, T. Optimum rice husk ash content and bacterial concentration in self-compacting concrete. Constr. Build. Mater. 2019, 222, 796–813. [Google Scholar] [CrossRef]
- Mohammed, H.; Ortoneda-Pedrola, M.; Nakouti, I.; Bras, A. Experimental characterisation of non-encapsulated bio-based concrete with self-healing capacity. Constr. Build. Mater. 2020, 256, 119411. [Google Scholar] [CrossRef]
- Van Mullem, T.; Gruyaert, E.; Caspeele, R.; De Belie, N. First large scale application with self-healing concrete in belgium: Analysis of the laboratory control tests. Materials 2020, 13, 997. [Google Scholar] [CrossRef]
- Sidiq, A.; Gravina, R.J.; Setunge, S.; Giustozzi, F. Microstructural analysis of healing efficiency in highly durable concrete. Constr. Build. Mater. 2019, 215, 969–983. [Google Scholar] [CrossRef]
- Mostavi, E.; Asadi, S.; Hassan, M.M.; Alansari, M. Evaluation of Self-Healing Mechanisms in Concrete with Double-Walled Sodium Silicate Microcapsules. J. Mater. Civ. Eng. 2015, 27, 04015035. [Google Scholar] [CrossRef]
- Hassan, M.M.; Milla, J.; Rupnow, T.; Al-Ansari, M.; Daly, W.H. Microencapsulation of calcium nitrate for concrete applications. Transp. Res. Rec. 2016, 2577, 8–16. [Google Scholar] [CrossRef]
- Gruyaert, E.; Van Tittelboom, K.; Sucaet, J.; Anrijs, J.; Van Vlierberghe, S.; Dubruel, P.; De Geest, B.G.; Remon, J.P.; De Belie, N. Capsules with evolving brittleness to resist the preparation of self-healing concrete. Mater. Constr. 2016, 66, e092. [Google Scholar] [CrossRef]
- De Belie, N.; Gruyaert, E.; Al-Tabbaa, A.; Antonaci, P.; Baera, C.; Bajare, D.; Darquennes, A.; Davies, R.; Ferrara, L.; Jefferson, T.; et al. A Review of Self-Healing Concrete for Damage Management of Structures. Adv. Mater. Interfaces. 2018, 5, 1–28. [Google Scholar] [CrossRef]
- Araújo, M.; Chatrabhuti, S.; Gurdebeke, S.; Alderete, N.; Van Tittelboom, K.; Raquez, J.M.; Cnudde, V.; Van Vlierberghe, S.; De Belie, N.; Gruyaert, E. Poly(methyl methacrylate) capsules as an alternative to the proof-of-concept’’ glass capsules used in self-healing concrete. Cem. Concr. Compos. 2018, 89, 260–271. [Google Scholar] [CrossRef]
- Van Tittelboom, K.; Tsangouri, E.; Van Hemelrijck, D.; De Belie, N. The efficiency of self-healing concrete using alternative manufacturing procedures and more realistic crack patterns. Cem. Concr. Compos. 2015, 57, 142–152. [Google Scholar] [CrossRef]
- Milla, J.; Hassan, M.M.; Rupnow, T. Evaluation of Self-Healing Concrete with Microencapsulated Calcium Nitrate. J. Mater. Civ. Eng. 2017, 29, 04017235. [Google Scholar] [CrossRef]
- Van Tittelboom, K.; Wang, J.; Araújo, M.; Snoeck, D.; Gruyaert, E.; Debbaut, B.; Derluyn, H.; Cnudde, V.; Tsangouri, E.; Van Hemelrijck, D.; et al. Comparison of different approaches for self-healing concrete in a large-scale lab test. Constr. Build. Mater. 2016, 107, 125–137. [Google Scholar] [CrossRef]
- Al-Tabbaa, A.; Litina, C.; Giannaros, P.; Kanellopoulos, A.; Souza, L. First UK field application and performance of microcapsule-based self-healing concrete. Constr. Build. Mater. 2019, 208, 669–685. [Google Scholar] [CrossRef]
- Wang, X.; Huang, Y.; Huang, Y.; Zhang, J.; Fang, C.; Yu, K.; Chen, Q.; Li, T.; Han, R.; Yang, Z.; et al. Laboratory and field study on the performance of microcapsule-based self-healing concrete in tunnel engineering. Constr. Build. Mater. 2019, 220, 90–101. [Google Scholar] [CrossRef]
- Milla, J.; Hassan, M.M.; Rupnow, T.; Daly, W.H. Measuring the crack-repair efficiency of steel fiber reinforced concrete beams with microencapsulated calcium nitrate. Constr. Build. Mater. 2019, 201, 526–538. [Google Scholar] [CrossRef]
- Gilford, J.; Hassan, M.M.; Rupnow, T.; Barbato, M.; Okeil, A.; Asadi, S. Dicyclopentadiene and Sodium Silicate Microencapsulation for Self-Healing of Concrete. J. Mater. Civ. Eng. 2014, 26, 886–896. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, M.; Xing, F.; Han, N. Effect of a healing agent on the curing reaction kinetics and its mechanism in a self-healing system. Appl. Sci. 2018, 8, 2241. [Google Scholar] [CrossRef]
- Kanellopoulos, A.; Qureshi, T.S.; Al-Tabbaa, A. Glass encapsulated minerals for self-healing in cement based composites. Constr. Build. Mater. 2015, 98, 780–791. [Google Scholar] [CrossRef]
- Ferrara, L.; Van Mullem, T.; Alonso, M.C.; Antonaci, P.; Borg, R.P.; Cuenca, E.; Jefferson, A.; Ng, P.-L.; Peled, A.; Roig-Flores, M.; et al. Experimental characterization of the self-healing capacity of cement based materials and its effects on the material performance: A state of the art report by COST Action SARCOS WG2. Constr. Build. Mater. 2018, 167, 115–142. [Google Scholar] [CrossRef]
- Roig-Flores, M.; Pirritano, F.; Serna, P.; Ferrara, L. Effect of crystalline admixtures on the self-healing capability of early-age concrete studied by means of permeability and crack closing tests. Constr. Build. Mater. 2016, 114, 447–457. [Google Scholar] [CrossRef]
- Roig-Flores, M.; Moscato, S.; Serna, P.; Ferrara, L. Self-healing capability of concrete with crystalline admixtures in different environments. Constr. Build. Mater. 2015, 86, 1–11. [Google Scholar] [CrossRef]
- Escoffres, P.; Desmettre, C.; Charron, J.P. Effect of a crystalline admixture on the self-healing capability of high-performance fiber reinforced concretes in service conditions. Constr. Build. Mater. 2018, 173, 763–774. [Google Scholar] [CrossRef]
- Azarsa, P.; Gupta, R.; Biparva, A. Assessment of self-healing and durability parameters of concretes incorporating crystalline admixtures and Portland Limestone Cement. Cem. Concr. Compos. 2019, 99, 17–31. [Google Scholar] [CrossRef]
- Xypex Concrete Waterproofing by CrystallizationTM. Available online: https://www.xypex.com/docs/default-source/default-document-library/english/xypex-catalogue.pdf?sfvrsn=e9df0169_66 (accessed on 24 March 2021).
- Durable Concrete Starts with Penetron Admix. Available online: https://www.penetron.com/uploads/Penetron_Admix_Brochure.pdf (accessed on 12 February 2021).
- Wang, X.F.; Yang, Z.H.; Fang, C.; Wang, W.; Liu, J.; Xing, F. Effect of carbonate-containing self-healing system on properties of a cementitious composite: Fresh, mechanical, and durability properties. Constr. Build. Mater. 2020, 235, 117442. [Google Scholar] [CrossRef]
- Chandraiah, M.; Reddy, T.C.S. Study on Strength Characteristics of Self-Healing Concrete with Crystalline Admixture. Int. J. Innov. Res. Sci. Eng. Technol. 2020, 6, 1312–1319. [Google Scholar] [CrossRef]
- Sideris, K.K.; Chatzopoulos, A.; Tassos, C.; Manita, P. Durability of concretes prepared with crystalline admixtures. MATEC Web Conf. 2019, 289, 09003. [Google Scholar] [CrossRef]
- Nasim, M.; Dewangan, U.K.; Deo, S.V. Effect of crystalline admixture, fly ash, and PVA fiber on self-healing capacity of concrete. Mater. Today Proc. 2020, 32, 844–849. [Google Scholar] [CrossRef]
- Wang, X.; Fang, C.; Li, D.; Han, N.; Xing, F. A self-healing cementitious composite with mineral admixtures and built-in carbonate. Cem. Concr. Compos. 2018, 92, 216–229. [Google Scholar] [CrossRef]
- Scrivener, K.L.; Crumbie, A.K.; Laugesen, P. The interfacial transition zone (ITZ) between cement paste and aggregate in concrete. Interface Sci. 2004, 12, 411–421. [Google Scholar] [CrossRef]
- Chuo, S.C.; Mohamed, S.F.; Setapar, S.H.M.; Ahmad, A.; Jawaid, M.; Wani, W.A.; Yaqoob, A.A.; Ibrahim, M.N.M. Insights into the current trends in the utilization of bacteria for microbially induced calcium carbonate precipitation. Materials 2020, 13, 4993. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Yuan, J.; Alazhari, M. Effect of Microbiological Growth Components for Bacteria-Based Self-Healing on the Properties of Cement Mortar. Materials 2019, 12, 1303. [Google Scholar] [CrossRef]
- Norambuena-Contreras, J.; Liu, Q.; Zhang, L.; Wu, S.; Yalcin, E.; Garcia, A. Influence of encapsulated sunflower oil on the mechanical and self-healing properties of dense-graded asphalt mixtures. Mater. Struct. Constr. 2019, 52, 1–13. [Google Scholar] [CrossRef]
- Al-Ansari, M.; Abu Taqa, A.G.; Senouci, A.; Hassan, M.M.; Shaat, A. Effect of calcium nitrate healing microcapsules on concrete strength and air permeability. Mag. Concr. Res. 2019, 71, 195–206. [Google Scholar] [CrossRef]
- Van Mullem, T.; Anglani, G.; Dudek, M.; Vanoutrive, H.; Bumanis, G.; Litina, C.; Kwiecień, A.; Al-Tabbaa, A.; Bajare, D.; Stryszewska, T.; et al. Addressing the need for standardization of test methods for self-healing concrete: An inter-laboratory study on concrete with macrocapsules. Sci. Technol. Adv. Mater. 2020, 21, 661–682. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.X.; Hu, X.M.; Cheng, W.M.; Zhao, Y.Y.; Wu, M.Y. Performance optimization of one-component polyurethane healing agent for self-healing concrete. Constr. Build. Mater. 2018, 179, 151–159. [Google Scholar] [CrossRef]








| Ref. | Mix Code | Concrete Type | Cement Type | w/c | CA Dosage (% Wt. Cement) | Role of CA | Age of Cracking | Healing Time | Crack Width | Healing Ratio (Scale 0–1) | Exposure |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [63] | M1 | LWC | Not specified | 0.45 | 4.50% | Cement replacement | 7 days | 28 days | 0.15 mm | - | Water immersion |
| [58] | M2 | FRC | II 42.5R | 0.45 | 4.00% | Limestone powder replacement | 2 days | 42 days | ≤0.3 mm | 0.90–1.00 | Water immersion |
| [57] | M3.1 | Precast FRC | II 42.5R | 0.45 | 4.00% | Limestone powder replacement | 2 days | 42 days | 0.1–0.4 mm | 0.80–1.00 | Water immersion |
| M3.2 | FRC | II 42.5R | 0.60 | 4.00% | Limestone powder replacement | 2 days | 42 days | 0.1–0.4 mm | 0.80–1.00 | Water immersion | |
| [60] | M4.1 | NSC | I 42.5R | 0.53 | 2.00% | Direct addition (on top of concrete mix) | 28 days | 4–5 days | 0.1–0.4 mm | 0.98–1.00 | Water immersion |
| M4.2 | NSC | GUL | 0.53 | 2.00% | Direct addition (on top of concrete mix) | 28 days | 4–5 days | 0.1–0.4 mm | 0.97–0.99 | Water immersion | |
| [64] | M5 | FRC | OPC 53 | 0.45 | 1.10% | Cement replacement | 2 days | 42 days | ≤0.4 mm | - | Water immersion |
| [65] | M6 | NSC | II 32.5R | 0.64 | 0.80% | Direct addition (on top of concrete mix) | - | - | - | - | Curing chamber (T = 20 °C,RH > 98%) |
| [66] | M7 | NSC | OPC 43 | 0.40 | 2.00% | Direct addition (on top of concrete mix) | 3 days | 42 days | ≤0.4 mm | - | Water immersion |
| [5] | M8 | HPFRCC | II 42.5R | 0.63 | 1.00% | Direct addition (on top of concrete mix) | 42 days | 365 days | 0.2 mm | 0.60 | Open air |
| Ref. | Bacteria | Bacteria Concentration | Nutrient | SCM | Changes at 28 Days | Water Absorption | |||
|---|---|---|---|---|---|---|---|---|---|
| Compressive Strength | Flexural Strength | Split Tensile Strength | Control Concrete | Bacterial Concrete | |||||
| [10] | Bacillus sphaericus | 250 μg/mL | YE, UR, CaCl | - | ↑ 15% | - | - | - | - |
| Bacillus sphaericus | 103 cells/mL | YE, UR | - | ↑ 10% | ↑ 2% | ↑ 16% | - | - | |
| [31] | 105 cells/mL | YE, UR | - | ↑ 20% | ↑ 35% | ↑ 25% | - | - | |
| 107 cells/mL | YE, UR | - | ↑ 17% | ↑ 22% | ↑ 19% | - | - | ||
| [32] | Bacillus subtilis | 105 cells/mL | LAC | - | ↑ 21% | ↑ 17% | - | - | - |
| [33] | Bacillus subtilis | 3 × 108 cells/mL | LAC | - | ↑ 12% | - | - | - | - |
| [34] | Bacillus subtilis | 108 cells/mL | YE, Peptone | - | - | - | - | 6.3% | 5.3% |
| [35] | Bacillus aerius | 105 cells/mL | Not specified | - | ↑ 11% | - | - | 2.3% | 1.2% |
| 105 cells/mL | Not specified | 10% SF | ↑ 31% | - | - | 0.8% | |||
| Bacillus megaterium | 103 cells/mL | LAC, UR | - | ↑ 3% | - | - | - | - | |
| [30] | 105 cells/mL | LAC, UR | - | ↑ 5% | - | - | - | - | |
| 107 cells/mL | LAC, UR | - | ↓ 5% | - | - | - | - | ||
| [29] | Sporoscarcina pasteurii | 107 cells/mL | Not specified | - | ↑ 5% | - | ↑ 11% | - | - |
| 107 cells/mL | Not specified | 10% NZ | ↑ 20% | - | ↑ 20% | - | - | ||
| [36] | Sporoscarcina pasteurii | 103 cells/mL | Not specified | - | ↑ 4% | - | - | 17.7% | 14.0% |
| 105 cells/mL | Not specified | - | ↑ 17% | - | - | 13.0% | |||
| 107 cells/mL | Not specified | - | ↑ 8% | - | - | 13.7% | |||
| 103 cells/mL | Not specified | 10% FA | No changes | - | - | 17.7% | 4.0% | ||
| 105 cells/mL | Not specified | 10% FA | ↑ 15% | - | - | 3.3% | |||
| 107 cells/mL | Not specified | 10% FA | ↑ 4% | - | - | 3.7% | |||
| [37] | Sporoscarcina pasteurii | 103 cells/mL | Not specified | 10% SF | ↑ 52% | - | - | 17.5% | 0.1% |
| 105 cells/mL | Not specified | 10% SF | ↑ 66% | - | - | 0.1% | |||
| 107 cells/mL | Not specified | 10% SF | ↑ 45% | - | - | 0.8% | |||
| [38] | Sporoscarcina pasteurii | 103 cells/mL | LAC | 15% RHA | ↑ 13% | ↑ 23% | ↑ 21% | 4.8% | 3.2% |
| 105 cells/mL | LAC | 15% RHA | ↑ 20% | ↑ 29% | ↑ 29% | 1.4% | |||
| 107 cells/mL | LAC | 15% RHA | ↑ 17% | ↑ 26% | ↑ 25% | 1.1% | |||
| [39] | Shewanella oneidensis | 2.3 × 108 cells/mL | TSB | - | ↑ 3% | - | - | - | - |
| Bacillus sphaericus | 2.3 × 108 cells/mL | TSB | 60% GGBS | ↓ 10% | - | - | - | - | |
| Nutrient | Dosage (% Weight of Cement) | Mean Values of Compressive Strength | |||||
|---|---|---|---|---|---|---|---|
| 3 Days | 7 Days | 28 Days | |||||
| (MPa) | (%) | (MPa) | (%) | (MPa) | (%) | ||
| Control | - | 22.88 | 100 | 28.93 | 100 | 45.31 | 100 |
| Calcium lactate | 3.00 | 27.70 | 121 | 36.02 | 125 | 58.76 | 130 |
| Calcium nitrate | 3.00 | 26.44 | 116 | 33.47 | 116 | 41.13 | 91 |
| Calcium formate | 3.00 | 37.96 | 166 | 44.23 | 153 | 57.63 | 127 |
| Yeast extract | 0.85 | 10.65 | 47 | 19.61 | 68 | 35.12 | 77 |
| Urea | 2.50 | 30.80 | 135 | 34.77 | 120 | 44.39 | 98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hermawan, H.; Minne, P.; Serna, P.; Gruyaert, E. Understanding the Impacts of Healing Agents on the Properties of Fresh and Hardened Self-Healing Concrete: A Review. Processes 2021, 9, 2206. https://doi.org/10.3390/pr9122206
Hermawan H, Minne P, Serna P, Gruyaert E. Understanding the Impacts of Healing Agents on the Properties of Fresh and Hardened Self-Healing Concrete: A Review. Processes. 2021; 9(12):2206. https://doi.org/10.3390/pr9122206
Chicago/Turabian StyleHermawan, Harry, Peter Minne, Pedro Serna, and Elke Gruyaert. 2021. "Understanding the Impacts of Healing Agents on the Properties of Fresh and Hardened Self-Healing Concrete: A Review" Processes 9, no. 12: 2206. https://doi.org/10.3390/pr9122206
APA StyleHermawan, H., Minne, P., Serna, P., & Gruyaert, E. (2021). Understanding the Impacts of Healing Agents on the Properties of Fresh and Hardened Self-Healing Concrete: A Review. Processes, 9(12), 2206. https://doi.org/10.3390/pr9122206