
Mental Health in Childhood and Adolescence: The Role of Polyunsaturated Fatty Acids



Abstract
1. Introduction
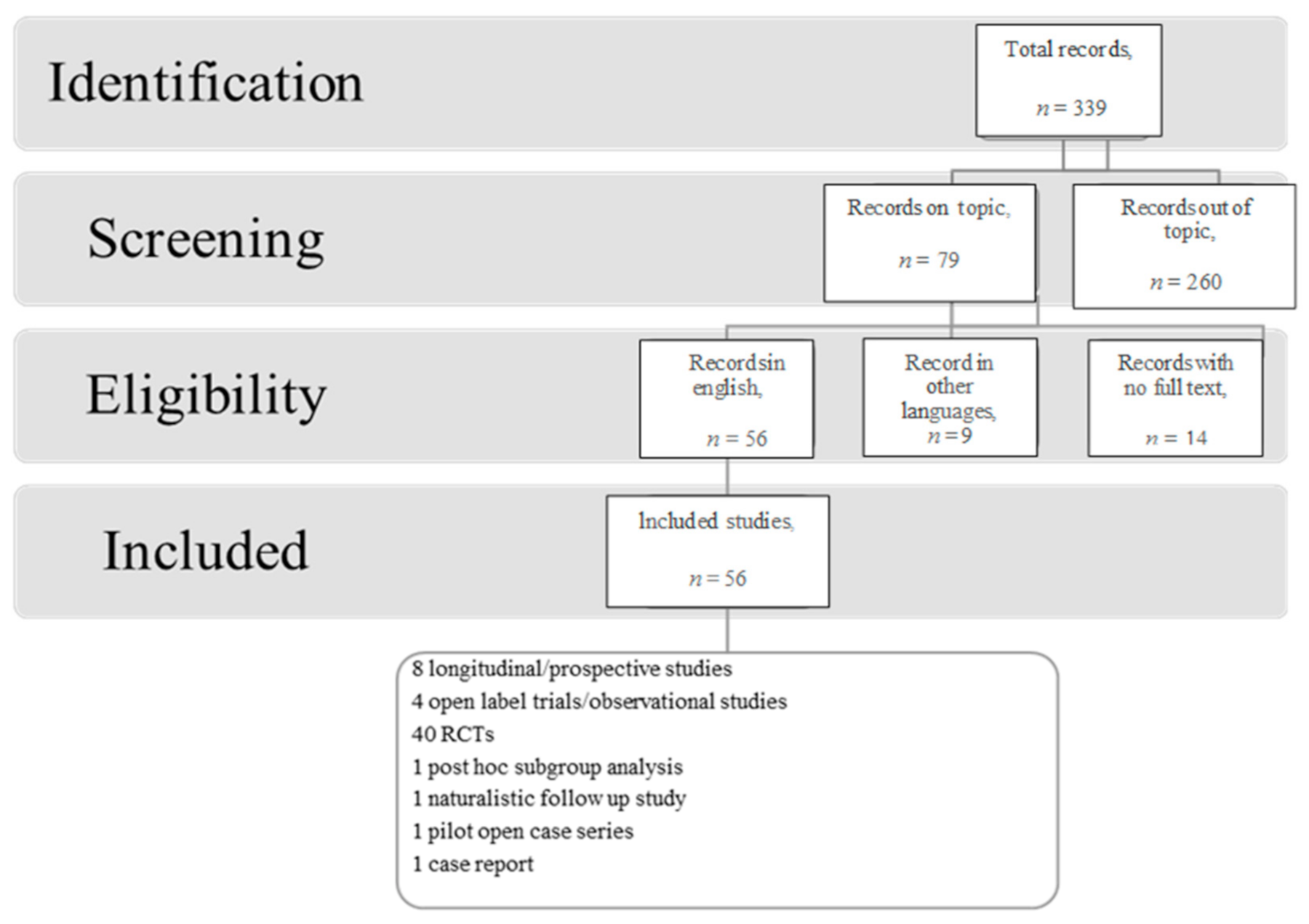
2. Methods
3. Results
4. Discussion
4.1. Schizophrenia
4.2. Bipolar Disorder
4.3. Major Depression
4.4. Anxiety Disorders
4.5. Obsessive Compulsive Disorder
4.6. Attention Deficit Hyperactivity Disorder
4.7. Autism Spectrum Disorders
4.8. Eating Disorders
4.9. Borderline Personality Disorder
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ABC | Aberrant Behaviour Checklist |
| AM | Active monitoring |
| AN | Anorexia nervosa |
| AA | Arachidonic Acid |
| ADHD | Attention deficit hyperactivity disorder |
| ADOS | Autism Diagnostic Observation Schedule |
| ASD | Autism Spectrum Disorder |
| BAIT | Beck Anxiety Inventory-Trait |
| BASC | Behaviour Assessment Scale for Children |
| BRIEF | Behaviour Rating Inventory of Executive Functioning |
| BRI | Behaviour Regulation |
| BP-NOS | Bipolar disorder not otherwise specified |
| BPD | Borderline Personality Disorder |
| BITSEA | Brief Infant Toddler Social and Emotional Assessment |
| BPRS | Brief Psychosis Rating Scale |
| CDSS | Calgary Depression Scale for Schizophrenia |
| CES-D | Centre for Epidemiologic Studies Depression Scale |
| CBCL | Child Behaviour Checklist |
| CBCL-PR | Child Behaviour Checklist—Parent Report |
| CDI | Child Development Inventory |
| CDRS | Children’s Depression Rating Scale |
| CGI-S | Clinical Global Impressions scale was used to measure symptom severity |
| CHR | Clinical High Risk |
| CBCM | Cognitive behavioural case management |
| CPRS-L | Conners’ Parent Rating Scale |
| CYC | Cyclothymic disorder |
| DHA | Docosahexaenoic acid |
| EAT-26 | Eating Attitudes Test |
| EA | Eating Disorder |
| EPA | Eicosapentaenoic acid |
| EFAs | Essential Fatty Acids |
| ECBI | Eyberg Child Behaviour Inventory |
| GAF | Global Assessment of functioning |
| C-GAS | Global Assessment Scale for Children |
| GEC | Global Executive Composite |
| HAM-D | Hamilton Depression Rating Scale |
| IF-PEP | Individual family |
| IVA/CPT | Intermediate Visual and Auditory/Continuous Performance Test |
| K-SADS | Kiddie Schedule for Affective Disorders Rating Scales |
| KRDS | Depression |
| KMRS | Mania |
| LA | Linolenic acid |
| MDD | Major depressive disorder |
| MADRS | Montgomery-Åsberg Depression Rating Scale |
| n-3 PUFAs | Omega 3 Polyunsaturated Fatty Acids |
| n-6 PUFAs | Omega 3 Polyunsaturated Fatty Acids |
| PDD NOS | Pervasive Developmental Disorder, Not Otherwise Specified |
| PDDST-II | Pervasive Developmental Disorders Screening Test II |
| PANSS | Positive and Negative Syndrome Scale |
| PEP | psychoeducational psychotherapy |
| SANS | Schedule for Assessment of Negative Symptoms |
| SDQ | Strengths and Difficulties Questionnaire |
| SNAP-IV | Swanson, Nolan, and Pelham-IV |
| SAFTEE-SI | Systematic Assessment for Treatment Emergent Events Specific Inquiry |
| TRS | Teacher’s Report Form |
| TOVA | Test of Variables of Attention |
| SRS-P | The Social Responsiveness Scale–Parent |
| UHR | Ultra-High-Risk |
| YMRS | Young Mania Rating Scale |
| GLA | γ-linolenic acid |
References
- Curtis, L.T.; Patel, K. Nutritional and Environmental Approaches to Preventing and Treating Autism and Attention Deficit Hyperactivity Disorder (ADHD): A Review. J. Altern. Complement. Med. 2008, 14, 79–85. [Google Scholar] [CrossRef]
- Transler, C.; Eilander, A.; Mitchell, S.; Van De Meer, N. The Impact of Polyunsaturated Fatty Acids in Reducing Child Attention Deficit and Hyperactivity Disorders. J. Atten. Disord. 2010, 14, 232–246. [Google Scholar] [CrossRef] [PubMed]
- Sinn, N.; Milte, C.; Howe, P.R.C. Oiling the Brain: A Review of Randomized Controlled Trials of Omega-3 Fatty Acids in Psychopathology across the Lifespan. Nutrients 2010, 2, 128–170. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Bosco, N.; Bourdet-Sicard, R.; Capuron, L.; Delzenne, N.; Doré, J.; Franceschi, C.; Lehtinen, M.J.; Recker, T.; Salvioli, S.; et al. Health Relevance of the Modification of Low Grade Inflammation in Ageing (Inflammageing) and the Role of Nu-Trition. Ageing Res. Rev. 2017, 40, 95–119. [Google Scholar] [CrossRef]
- Lee, S.; Gura, K.M.; Kim, S.; Arsenault, D.A.; Bistrian, B.R.; Puder, M. Current Clinical Applications of Ω-6 and Ω-3 Fatty Acids. Nutr. Clin. Pract. 2006, 21, 323. [Google Scholar] [CrossRef] [PubMed]
- Zou, R.; El Marroun, H.; Voortman, T.; Hillegers, M.; White, T.; Tiemeier, H. Maternal Polyunsaturated Fatty Acids During Pregnancy and Offspring Brain Development in Childhood. Am. J. Clin. Nutr. 2021, 114, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Pusceddu, M.M.; Nolan, Y.M.; Green, H.F.; Robertson, R.C.; Stanton, C.; Kelly, P.; Cryan, J.F.; Dinan, T.G. The Omega-3 Polyunsaturated Fatty Acid Docosahexaenoic Acid (DHA) Reverses Corticosterone-Induced Changes in Cortical Neurons. Int. J. Neuropsychopharmacol. 2016, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Leon, A.M.; Lapuente, M.; Estruch, R.; Casas, R. Clinical Advances in Immunonutrition and Atherosclerosis: A Review. Front. Immunol. 2019, 10, 837. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Cook, N.R.; Lee, I.-M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Albert, C.M.; Gordon, D.; Copeland, T.; et al. Marine n−3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer. N. Engl. J. Med. 2019, 380, 23–32. [Google Scholar] [CrossRef]
- Erdman, J.W.; MacDonald, I.A.; Zeisel, S.H. Present Knowledge in Nutrition, 10th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2012. [Google Scholar]
- Chang, C.-Y.; Kuan, Y.-H.; Li, J.-R.; Chen, W.-Y.; Ou, Y.-C.; Pan, H.-C.; Liao, S.-L.; Raung, S.-L.; Chang, C.-J.; Chen, C.-J. Docosahexaenoic Acid Reduces Cellular Inflammatory Response Following Permanent Focal Cerebral Ischemia in Rats. J. Nutr. Biochem. 2013, 24, 2127. [Google Scholar] [CrossRef]
- Zúñiga, J.; Cancino, M.; Medina, F.; Varela, P.; Vargas, R.; Tapia, G.; Videla, L.A.; Fernández, V. N-3 PUFA Supplementation Triggers PPAR-α Activation and PPAR-α/NF-ΚB Interaction: Anti-Inflammatory Implications in Liver Ischemia-Reperfusion Injury. PLoS ONE 2011, 6. [Google Scholar] [CrossRef]
- Healy-Stoffel, M.; Levant, B. N-3 (Omega-3) Fatty Acids: Effects on Brain Dopamine Systems and Potential Role in the Etiology and Treatment of Neuropsychiatric Disorders. CNS Neurol. Disord. Drug Targets 2018, 17, 216. [Google Scholar] [CrossRef]
- Zirpoli, H.; Chang, C.L.; Carpentier, Y.A.; Michael-Titus, A.T.; Ten, V.S.; Deckelbaum, R.J. Novel Approaches for Omega-3 Fatty Acid Therapeutics: Chronic Versus Acute Administration to Protect Heart, Brain, and Spinal Cord. Annu. Rev. Nutr. 2020, 40, 161–187. [Google Scholar] [CrossRef]
- Bazan, N.G. Docosanoids and Elovanoids from Omega-3 Fatty Acids Are Pro-Homeostatic Modulators of Inflammatory Responses, Cell Damage and Neuroprotection. Mol. Asp. Med. 2018, 64, 18–33. [Google Scholar] [CrossRef]
- Yang, L.; Song, Z.; Cao, W.; Wang, Y.; Lu, H.; Guo, F.; Yang, H.; Chen, J.; Wang, S.; Sun, G. Effects of Diets with Different N-6/N-3 Fatty Acids on Cardiovascular Risk Factors in Mice Fed High-Fat diets. J. Hyg. Res. 2016, 45, 436–441. [Google Scholar]
- Dyall, S.C. Long-Chain Omega-3 Fatty Acids and the Brain: A Review of the Independent and Shared Effects of EPA, DPA and DHA. Front. Aging Neurosci. 2015, 7, 52. [Google Scholar] [CrossRef]
- Birch, E.E.; Garfield, S.; Hoffman, D.R.; Uauy, R.; Birch, D.G. A Randomized Controlled Trial of Early Dietary Supply of Long-Chain Polyunsaturated Fatty Acids and Mental Development in Term Infants. Dev. Med. Child Neurol. 2000, 42, 174. [Google Scholar] [CrossRef]
- Wainwright, P.E.; Ward, G.R.; Winfield, D.; Huang, Y.-S.; Mills, D.E.; Ward, R.P.; McCutcheon, D. Effects of Prenatal Ethanol and Long-Chain N-3 Fatty Acid Supplementation on Development in Mice. 1. Body and Brain Growth, Sensorimotor De-Velopment, and Water T-Maze Reversal Learning. Alcohol. Clin. Exp. Res. 1990, 14, 405. [Google Scholar]
- Crawford, M.A.; Sinclair, A.J. Nutritional Influences in the Evolution of Mammalian Brain. In Novartis Foundation Symposia; Wiley: Hoboken, NJ, USA, 2008; pp. 267–292. [Google Scholar] [CrossRef]
- Georgieff, M.K.; Innis, S.M. Controversial Nutrients That Potentially Affect Preterm Neurodevelopment: Essential Fatty Acids and Iron. Pediatr. Res. 2005, 57 Pt 2, 99R–103R. [Google Scholar] [CrossRef]
- Wang, L.; Albrecht, M.A.; Wurtman, R.J. Dietary Supplementation with Uridine-5′-Monophosphate (UMP), a Membrane Phosphatide Precursor, Increases Acetylcholine Level and Release in Striatum of Aged Rat. Brain Res. 2007, 1133, 42–48. [Google Scholar] [CrossRef][Green Version]
- Wang, L.; Pooler, A.M.; Albrecht, M.A.; Wurtman, R.J. Dietary Uridine-5’-Monophosphate Supplementation Increases Potassium-Evoked Dopamine Release and Promotes Neurite Outgrowth in Aged Rats. J. Mol. Neurosci. 2005, 27, 137–146. [Google Scholar] [CrossRef]
- Zhou, M.-M.; Che, H.-X.; Huang, J.-Q.; Zhang, T.-T.; Xu, J.; Xue, C.-H.; Wang, Y.-M. Comparative Study of Different Polar Groups of EPA-Enriched Phospholipids on Ameliorating Memory Loss and Cognitive Deficiency in Aged SAMP8 Mice. Mol. Nutr. Food Res. 2018, 62, e1700637. [Google Scholar] [CrossRef] [PubMed]
- Heras-Sandoval, D.; Pedraza-Chaverri, J.; Pérez-Rojas, J.M. Role of Docosahexaenoic Acid in the Modulation of Glial Cells in Alzheimer’s Disease. J. Neuroinflammation 2016, 13, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Belkouch, M.; Hachem, M.; Elgot, A.; Van, A.L.; Picq, M.; Guichardant, M.; Lagarde, M.; Bernoud-Hubac, N. The Pleiotropic Effects of Omega-3 Docosahexaenoic Acid on the Hallmarks of Alzheimer’s Disease. J. Nutr. Biochem. 2016, 38, 1–11. [Google Scholar] [CrossRef]
- Bozzatello, P.; Rocca, P.; Mantelli, E.; Bellino, S. Polyunsaturated Fatty Acids: What Is Their Role in Treatment of Psychiatric Disorders? Int. J. Mol. Sci. 2019, 20, 5257. [Google Scholar] [CrossRef]
- Bozzatello, P.; Brignolo, E.; De Grandi, E.; Bellino, S. Supplementation with Omega-3 Fatty Acids in Psychiatric Disorders: A Review of Literature Data. J. Clin. Med. 2016, 5, 67. [Google Scholar] [CrossRef]
- Mischoulon, D.; Freeman, M.P. Omega-3 Fatty Acids in Psychiatry. Psychiatr. Clin. N. Am. 2013, 36, 15–23. [Google Scholar] [CrossRef]
- Hallahan, B.; Garland, M.R. Essential Fatty Acids and Mental Health. Br. J. Psychiatry 2005, 186, 275–277. [Google Scholar] [CrossRef]
- Gören, J.L.; Tewksbury, A.T. The Use of Omega-3 Fatty Acids in Mental Illness. J. Pharm. Pr. 2011, 24, 452–471. [Google Scholar] [CrossRef]
- Bozzatello, P.; De Rosa, M.; Rocca, P.; Bellino, S. Effects of Omega 3 Fatty Acids on Main Dimensions of Psychopathology. Int. J. Mol. Sci. 2020, 21, 6042. [Google Scholar] [CrossRef]
- Agostoni, C.; Nobile, M.; Ciappolino, V.; Delvecchio, G.; Tesei, A.; Turolo, S.; Crippa, A.; Mazzocchi, A.; Altamura, C.A.; Brambilla, P. The Role of Omega-3 Fatty Acids in Developmental Psychopathology: A Systematic Review on Early Psychosis, Autism, and ADHD. Int. J. Mol. Sci. 2017, 18, 2608. [Google Scholar] [CrossRef]
- Kraguljac, N.; Montori, V.M.; Pavuluri, M.; Chai, H.S.; Wilson, B.S.; Unal, S.S. Efficacy of Omega-3 Fatty Acids in Mood Disorders—A Systematic Review and Metaanalysis. Psychopharmacol. Bull. 2009, 42, 39–54. [Google Scholar]
- Fenton, W.S.; Hibbeln, J.; Knable, M. Essential Fatty Acids, Lipid Membrane Abnormalities, and the Diagnosis and Treatment of Schizophrenia. Biol. Psychiatry 2000, 47, 8–21. [Google Scholar] [CrossRef]
- Wolkin, A.; Segarnick, D.; Sierkierski, J.; Manku, M.; Horrobin, D.; Rotrosen, J. Essential Fatty Acid Supplementation During Early Alcohol Abstinence. Alcohol. Clin. Exp. Res. 1987, 11, 87–92. [Google Scholar] [CrossRef]
- Assies, J.; Lieverse, R.; Vreken, P.; Wanders, R.J.A.; Dingemans, P.M.J.A.; Linszen, D.H. Significantly Reduced Docosahex-Aenoic and Docosapentaenoic Acid Concentrations in Erythrocyte Membranes from Schizophrenic Patients Compared with a Carefully Matched Control Group. Biol. Psychiatry 2001, 49, 510. [Google Scholar] [CrossRef]
- Berger, M.; Nelson, B.; Markulev, C.; Yuen, H.P.; Schäfer, M.R.; Mossaheb, N.; Schlögelhofer, M.; Smesny, S.; Hickie, I.B.; Berger, G.E.; et al. Relationship Between Polyunsaturated Fatty Acids and Psychopathology in the NEURAPRO Clinical Trial. Front. Psychiatry 2019, 10, 14. [Google Scholar] [CrossRef]
- Horrobin, D.F.; Glen, A.M.; Vaddadi, K. The Membrane Hypothesis of Schizophrenia. Schizophr. Res. 1994, 13, 195–207. [Google Scholar] [CrossRef]
- Tessier, C.; Sweers, K.; Frajerman, A.; Bergaoui, H.; Ferreri, F.; Delva, C.; Lapidus, N.; Lamaziere, A.; Roiser, J.; De Hert, M.; et al. Membrane Lipidomics in Schizophrenia Patients: A Correlational Study with Clinical and Cognitive Manifestations. Transl. Psychiatry 2016, 6, e906. [Google Scholar] [CrossRef]
- Yao, J.; Vankammen, D. Red Blood Cell Membrane Dynamics in Schizophrenia I. Membrane Fluidity. Schizophr. Res. 1994, 11, 209–216. [Google Scholar] [CrossRef]
- Bentsen, H.; Solberg, D.K.; Refsum, H.; Gran, J.M.; Bøhmer, T.; Torjesen, P.A.; Halvorsen, O.; Lingjærde, O. Bimodal Distribution of Polyunsaturated Fatty Acids in Schizophrenia Suggests Two Endophenotypes of the Disorder. Biol. Psychiatry 2011, 70, 97–105. [Google Scholar] [CrossRef]
- Marshall, M.; Rathbone, J. Early Intervention for Psychosis. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2006. [Google Scholar]
- Power, L.; Polari, A.R.; Yung, A.; McGorry, P.D.; Nelson, B. Distress in Relation to Attenuated Psychotic Symptoms in the Ultra-High-Risk Population Is Not Associated With Increased Risk of Psychotic Disorder. Early Interv. Psychiatry 2015, 10, 258–262. [Google Scholar] [CrossRef]
- Rapado-Castro, M.; Calvo, A.; McGorry, P.; Yung, A.; Nelson, B. Poster #T191 Sources of Clinical Distress in Young People at Ultra High Risk of Psychosis. Schizophr. Res. 2014, 153, S356–S357. [Google Scholar] [CrossRef]
- Ziermans, T.B.; Schothorst, P.F.; Sprong, M.; van Engeland, H. Transition and Remission in Adolescents at Ultra-High Risk for Psychosis. Schizophr. Res. 2011, 126, 58–64. [Google Scholar] [CrossRef]
- Cadenhead, K.S.; Minichino, A.; Kelsven, S.; Addington, J.; Bearden, C.; Cannon, T.D.; Cornblatt, B.A.; Mathalon, D.; McGlashan, T.H.; Perkins, D.O.; et al. Metabolic Abnormalities and Low Dietary Omega 3 Are Associated with Symptom Severity and Worse Functioning Prior to the Onset of Psychosis: Findings from the North American Prodrome Longitudinal Studies Consortium. Schizophr. Res. 2019, 204, 96–103. [Google Scholar] [CrossRef]
- McGlashan, T.H.; Zipursky, R.B.; Perkins, D.; Addington, J.; Miller, T.; Woods, S.W.; Hawkins, K.A.; Hoffman, R.E.; Preda, A.; Epstein, I.; et al. Randomized, Double-Blind. Trial of Olanzapine Versus Placebo in Patients Prodromally Symptomatic for Psychosis. Am. J. Psychiatry 2006, 163, 790. [Google Scholar] [CrossRef]
- Morrison, A.P.; French, P.; Walford, L.; Lewis, S.; Kilcommons, A.; Green, J.; Parker, S.; Bentall, R.P. Cognitive Therapy for the Prevention of Psychosis in People at Ultra-High Risk. Br. J. Psychiatry 2004, 185, 291–297. [Google Scholar] [CrossRef]
- Amminger, G.P.; Schäfer, M.R.; Papageorgiou, K.; Klier, C.M.; Cotton, S.M.; Harrigan, S.M.; Mackinnon, A.; McGorry, P.D.; Berger, G.E. Long-Chain ω-3 Fatty Acids for Indicated Prevention of Psychotic Disorders: A Randomized, Placebo-Controlled Trial. Arch. Gen. Psychiatry 2010, 67, 146. [Google Scholar] [CrossRef] [PubMed]
- Pawełczyk, T.; Grancow-Grabka, M.; Kotlicka-Antczak, M.; Trafalska, E.; Pawełczyk, A. A Randomized Controlled Study of the Efficacy of Six-Month Supplementation with Concentrated Fish Oil Rich in Omega-3 Polyunsaturated Fatty Acids in First Episode Schizophrenia. J. Psychiatr. Res. 2016, 73, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Mcgorry, P.D.; Nelson, B.; Markulev, C.; Yuen, H.P.; Schäfer, M.R.; Mossaheb, N.; Schlögelhofer, M.; Smesny, S.; Hickie, I.B.; Berger, G.E.; et al. Effect of ω-3 Polyunsaturated Fatty Acids in Young People at Ultrahigh Risk for Psychotic Disorders: The NEURAPRO. Randomized Clin. Trial. JAMA Psychiatry 2017, 74, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Amminger, G.P.; Mechelli, A.; Rice, S.; Kim, S.W.; Klier, C.M.; McNamara, R.K.; Berk, M.; McGorry, P.D.; Schäfer, M.R. Pre-Dictors of Treatment Response in Young People at Ultra-High. Risk for Psychosis Who Received Long-Chain Omega-3 Fatty Acids. Transl. Psychiatry 2015, 5, e495. [Google Scholar] [CrossRef]
- Sethom, M.; Fares, S.; Bouaziz, N.; Melki, W.; Jemaa, R.; Feki, M.; Hechmi, Z.; Kaabachi, N. Polyunsaturated Fatty Acids Deficits Are Associated with Psychotic State and Negative Symptoms in Patients With Schizophrenia. Prostaglandins Leukot. Essent. Fat. Acids 2010, 83, 131–136. [Google Scholar] [CrossRef]
- Anderson, G.; Maes, M. Schizophrenia: Linking Prenatal Infection to Cytokines, the Tryptophan Catabolite (TRYCAT) Pathway, NMDA Receptor Hypofunction, Neurodevelopment and Neuroprogression. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2013, 42, 5–19. [Google Scholar] [CrossRef]
- Galderisi, S.; Rucci, P.; Mucci, A.; Rossi, A.; Rocca, P.; Bertolino, A.; Aguglia, E.; Amore, M.; Bellomo, A.; Bozzatello, P.; et al. The Interplay Among Psychopathology, Personal Resources, Context-Related Factors and Real-Life Functioning in Schizophrenia: Stability in Relationships After 4 Years and Differences in Network Structure Between Recovered and Non-Recovered Patients. World Psychiatry 2020, 19, 81. [Google Scholar] [CrossRef]
- Scheffer, R.E.; Kowatch, R.A.; Carmody, T.; Rush, A. Randomized, Placebo-Controlled Trial of Mixed Amphetamine Salts for Symptoms of Comorbid ADHD in Pediatric Bipolar Disorder After Mood Stabilization with Divalproex Sodium. Am. J. Psychiatry 2005, 162, 58–64. [Google Scholar] [CrossRef]
- Mcnamara, R.K.; Jandacek, R.; Tso, P.; Blom, T.J.; Welge, J.A.; Strawn, J.R.; Adler, C.M.; Strakowski, S.M.; Delbello, M.P. Ad-Olescents With or at Ultra-High Risk for Bipolar Disorder Exhibit Erythrocyte Docosahexaenoic Acid and Eicosapentaenoic Acid Deficits: A Candidate Prodromal Risk Biomarker. Early Interv. Psychiatry 2016, 10, 203. [Google Scholar] [CrossRef]
- Wozniak, J.; Biederman, J.; Mick, E.; Waxmonsky, J.; Hantsoo, L.; Best, C.; Cluette-Brown, J.E.; Laposata, M. Omega-3 Fatty Acid Monotherapy for Pediatric Bipolar Disorder: A Prospective Open-Label Trial. Eur. Neuropsychopharmacol. 2007, 17, 440–447. [Google Scholar] [CrossRef]
- Wozniak, J.; Faraone, S.V.; Chan, J.; Tarko, L.; Hernandez, M.; Davis, J.; Woodworth, K.Y.; Biederman, J. A Randomized Clinical Trial of High Eicosapentaenoic Acid Omega-3 Fatty Acids and Inositol As Monotherapy and in Combination in the Treatment of Pediatric Bipolar Spectrum Disorders: A Pilot Study. J. Clin. Psychiatry 2015, 76, 1548. [Google Scholar] [CrossRef]
- Clayton, E.H.; Hanstock, T.L.; Hirneth, S.J.; Kable, C.J.; Garg, M.L.; Hazell, P.L. Reduced Mania and Depression in Juvenile Bipolar Disorder Associated with Long-Chain ω-3 Polyunsaturated Fatty Acid Supplementation. Eur. J. Clin. Nutr. 2009, 63, 1037–1040. [Google Scholar] [CrossRef]
- Cao, J.; Schwichtenberg, K.A.; Hanson, N.Q.; Tsai, M. Incorporation and Clearance of Omega-3 Fatty Acids in Erythrocyte Membranes and Plasma Phospholipids. Clin. Chem. 2006, 52, 2265–2272. [Google Scholar] [CrossRef]
- Vidgren, H.M.; Ågren, J.J.; Schwab, U.; Rissanen, T.; Hänninen, O.; Uusitupa, M.I.J. Incorporation of N-3 Fatty Acids into Plasma Lipid Fractions, and Erythrocyte Membranes and Platelets During Dietary Supplementation with Fish, Fish Oil, and Docosahexaenoic Acid-Rich Oil Among Healthy Young Men. Lipids 1997, 32, 697–705. [Google Scholar] [CrossRef]
- Fristad, M.A.; Young, A.S.; Vesco, A.T.; Nader, E.S.; Healy, K.Z.; Gardner, W.; Wolfson, H.L.; Arnold, L.E. A Randomized Controlled Trial of Individual Family Psychoeducational Psychotherapy and Omega-3 Fatty Acids in Youth with Subsyn-Dromal Bipolar Disorder. J. Child Adolesc. Psychopharmacol. 2015, 25, 764. [Google Scholar] [CrossRef] [PubMed]
- Sinn, N.; Bryan, J. Effect of Supplementation With Polyunsaturated Fatty Acids and Micronutrients on Learning and Be-Havior Problems Associated with Child ADHD. J. Dev. Behav. Pediatrics 2007, 28, 82. [Google Scholar] [CrossRef] [PubMed]
- Sorgi, P.J.; Hallowell, E.M.; Hutchins, H.L.; Sears, B. Effects of an Open-Label Pilot Study with High-Dose EPA/DHA Concentrates on Plasma Phospholipids and Behavior in Children With Attention Deficit Hyperactivity Disorder. Nutr. J. 2007, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Fristad, M.A.; Roley-Roberts, M.E.; Black, S.R.; Arnold, L.E. Moody Kids Years Later: Long-Term Outcomes of Youth from the Omega-3 and Therapy (OATS) Studies. J. Affect. Disord. 2021, 281, 24–32. [Google Scholar] [CrossRef]
- Vesco, A.T.; Young, A.S.; Arnold, L.E.; Fristad, M.A. Omega-3 Supplementation Associated with Improved Parent-Rated Executive Function in Youth with Mood Disorders: Secondary Analyses of the Omega 3 and Therapy (OATS) Trials. J. Child Psychol. Psychiatry 2017, 59, 628–636. [Google Scholar] [CrossRef]
- Twenge, J.M.; Gentile, B.; DeWall, C.N.; Ma, D.; Lacefield, K.; Schurtz, D.R. Birth Cohort Increases in Psychopathology Among Young Americans, 1938–2007: A Cross-Temporal Meta-Analysis of the MMPI. Clin. Psychol. Rev. 2010, 30, 145–154. [Google Scholar] [CrossRef]
- Logan, A.C.; Jacka, F.N. Nutritional Psychiatry Research: An Emerging Discipline and Its Intersection with Global Ur-Banization, Environmental Challenges and the Evolutionary Mismatch. J. Physiol. Anthropol. 2014, 33. [Google Scholar] [CrossRef]
- Hibbeln, J.R.; Salem, N. Dietary Polyunsaturated Fatty Acids and Depression: When Cholesterol Does Not Satisfy. Am. J. Clin. Nutr. 1995, 62, 1–9. [Google Scholar] [CrossRef]
- Lin, P.-Y.; Huang, S.-Y.; Su, K.-P. A Meta-Analytic Review of Polyunsaturated Fatty Acid Compositions in Patients with Depression. Biol. Psychiatry 2010, 68, 140–147. [Google Scholar] [CrossRef]
- McNamara, R.K.; Nandagopal, J.J.; Strakowski, S.M.; DelBello, M.P. Preventative Strategies for Early-Onset Bipolar Dis-Order: Towards a Clinical Staging Mode. CNS Drugs 2010, 24, 983–996. [Google Scholar] [CrossRef]
- McNamara, R.K.; Hahn, C.-G.; Jandacek, R.; Rider, T.; Tso, P.; Stanford, K.E.; Richtand, N.M. Selective Deficits in the Omega-3 Fatty Acid Docosahexaenoic Acid in the Postmortem Orbitofrontal Cortex of Patients with Major Depressive Disorder. Biol. Psychiatry 2007, 62, 17–24. [Google Scholar] [CrossRef]
- Pottala, J.; Talley, J.; Churchill, S.; Lynch, D.; von Schacky, C.; Harris, W. Red Blood Cell Fatty Acids Are Associated with Depression in a Case-Control Study of Adolescents. Prostaglandins Leukot. Essent. Fat. Acids 2012, 86, 161–165. [Google Scholar] [CrossRef]
- Nemets, H.; Nemets, B.; Apter, A.; Bracha, Z.; Belmaker, R.H. Omega-3 Treatment of Childhood Depression: A Controlled, Dou-Ble-Blind. Pilot Study. Am. J. Psychiatry 2006, 163, 1098. [Google Scholar] [CrossRef]
- Trebatická, J.; Hradečná, Z.; Surovcová, A.; Katrenčíková, B.; Gushina, I.; Waczulíková, I.; Sušienková, K.; Garaiova, I.; Šuba, J.; Ďuračková, Z. Omega-3 Fatty-Acids Modulate Symptoms of Depressive Disorder, Serum Levels of Omega-3 Fatty Acids and Ome-Ga-6/Omega-3 Ratio in Children. A Randomized, Double-Blind. And Controlled Trial. Psychiatry Res. 2020, 287, 112911. [Google Scholar]
- Young, A.S.; Arnold, L.E.; Wolfson, H.L.; Fristad, M.A. Psychoeducational Psychotherapy and Omega-3 Supplementation Improve Co-Occurring Behavioral Problems in Youth with Depression: Results from a Pilot RCT. J. Abnorm. Child Psychol. 2016, 45, 1025–1037. [Google Scholar] [CrossRef]
- Kessler, R.C.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Wittchen, H.-U. Twelve-Month and Lifetime Prevalence and Lifetime Morbid Risk of Anxiety and Mood Disorders in the United States. Int. J. Methods Psychiatr. Res. 2012, 21, 169–184. [Google Scholar] [CrossRef]
- Merikangas, K.R.; He, J.-P.; Burstein, M.; Swanson, S.A.; Avenevoli, S.; Cui, L.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime Prevalence of Mental Disorders in U.S. Adolescents: Results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef]
- Pine, D.S.; Cohen, P.; Gurley, D.; Brook, J.; Ma, Y. The Risk for Early-Adulthood Anxiety and Depressive Disorders in Ad-Olescents With Anxiety and Depressive Disorders. Arch. Gen. Psychiatry 1998, 55, 56. [Google Scholar] [CrossRef]
- Wehry, A.M.; Beesdo-Baum, K.; Hennelly, M.M.; Connolly, S.D.; Strawn, J.R. Assessment and Treatment of Anxiety Disorders in Children and Adolescents. Curr. Psychiatry Rep. 2015, 17, 1–11. [Google Scholar] [CrossRef]
- Hamazaki, K.; Itomura, M.; Huan, M.; Nishizawa, H.; Sawazaki, S.; Tanouchi, M.; Watanabe, S.; Hamazaki, T.; Terasawa, K.; Yazawa, K. Effect of ω-3 Fatty Acid-Containing Phospholipids on Blood Catecholamine Concentrations in Healthy Volunteers: A Randomized, Placebo-Controlled, Double-Blind Trial. Nutrition 2005, 21, 705. [Google Scholar] [CrossRef]
- Kiecolt-Glaser, J.K.; Belury, M.A.; Andridge, R.; Malarkey, W.B.; Glaser, R. Omega-3 Supplementation Lowers Inflammation and Anxiety in Medical Students: A Randomized Controlled Trial. Brain Behav. Immun. 2011, 25, 1725. [Google Scholar] [CrossRef]
- Manos, B.E.; Bravender, T.D.; Harrison, T.M.; Lange, H.L.H.; Cottrill, C.B.; Abdel-Rasoul, M.; Bonny, A.E. A Pilot Randomized Controlled Trial of Omega-3 Fatty Acid Supplementation for the Treatment of Anxiety in Adolescents with Anorexia Nervosa. Int. J. Eat. Disord. 2018, 51, 1367–1372. [Google Scholar] [CrossRef]
- Robinson, D.G.; Gallego, J.A.; John, M.; Hanna, L.A.; Zhang, J.-P.; Birnbaum, M.L.; Greenberg, J.; Naraine, M.; Peters, B.D.; McNamara; et al. A Potential Role for Adjunctive Omega-3 Polyunsaturated Fatty Acids for Depression and Anxiety Symptoms in Recent Onset Psychosis: Results from a 16 Week Randomized Placebo-Controlled Trial for Participants Concurrently Treated with Risperidone. Schizophr. Res. 2019, 204, 295–303. [Google Scholar] [CrossRef]
- Zijlmans, J.; Marhe, R.; van der Ende, J.; Verhulst, F.C.; Popma, A.; Tiemeier, H.; van den Heuvel, O.A. Children with Obses-Sive-Compulsive Symptomology in the General Population: Different Subtypes? J. Dev. Behav. Pediatrics 2017, 38, 476. [Google Scholar] [CrossRef]
- Valleni-Basile, L.A.; Garrison, C.Z.; Waller, J.L.; Addy, C.L.; McKeown, R.E.; Jackson, K.L.; Cuffe, S.P. Incidence of Obses-Sive-Compulsive Disorder in a Community Sample of Young Adolescents. J. Am. Acad. Child Adolesc. Psychiatry 1996, 35, 898. [Google Scholar] [CrossRef] [PubMed]
- Zohar, A.H.; Zohar, A.H. The Epidemiology of Obsessive-Compulsive Disorder in Children and Adolescents. Child Adolesc. Psychiatr. Clin. N. Am. 1999, 8, 445–460. [Google Scholar] [CrossRef]
- Fux, M.; Benjamin, J.; Nemets, B. A Placebo-Controlled Cross-over Trial of Adjunctive EPA in OCD. J. Psychiatr. Res. 2004, 38, 323–325. [Google Scholar] [CrossRef]
- Polanczyk, G.; De Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The Worldwide Prevalence of ADHD: A Systematic Review and Metaregression Analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.R.; Stevens, L.; Zhang, W.; Peck, L. Long-Chain Polyunsaturated Fatty Acids in Children With Attention-Deficit Hyperactivity Disorder. Am. J. Clin. Nutr. 2000, 71, 327S–330S. [Google Scholar] [CrossRef]
- Mitchell, E.; Aman, M.G.; Turbott, S.H.; Manku, M. Clinical Characteristics and Serum Essential Fatty Acid Levels in Hyperactive Children. Clin. Pediatr. 1987, 26, 406–411. [Google Scholar] [CrossRef]
- Stevens, L.J.; Zentall, S.S.; Deck, J.L.; Abate, M.L.; Watkins, B.; Lipp, S.R.; Burgess, J.R. Essential Fatty Acid Metabolism in Boys with Attention-Deficit Hyperactivity Disorder. Am. J. Clin. Nutr. 1995, 62, 761–768. [Google Scholar] [CrossRef]
- Yonezawa, K.; Nonaka, S.; Iwakura, Y.; Kusano, Y.; Funamoto, Y.; Kanchi, N.; Yamaguchi, N.; Kusumoto, Y.; Imamura, A.; Ozawa, H. Investigation into the Plasma Concentration of Ω3 Polyunsaturated Fatty Acids in Japanese Attention-Deficit Hy-Peractivity Disorder Patients. J. Neural Transm. 2018, 125, 1395. [Google Scholar] [CrossRef]
- Ross, B.M.; McKenzie, I.; Glen, I.; Bennett, C.P.W. Increased Levels of Ethane, A Non-Invasive Marker of N-3 Fatty Acid Oxidation, in Breath of Children with Attention Deficit Hyperactivity Disorder. Nutr. Neurosci. 2003, 6, 277–281. [Google Scholar] [CrossRef]
- Sumich, A.; Matsudaira, T.; Gow, R.V.; Ibrahimovic, A.; Ghebremeskel, K.; Crawford, M.; Taylor, E. Resting State Electroencephalographic Correlates With Red Cell Long-Chain Fatty Acids, Memory Performance and Age in Adolescent Boys with Attention Deficit Hyperactivity Disorder. Neuropharmacology 2009, 57, 708–714. [Google Scholar] [CrossRef]
- Voigt, R.G.; Llorente, A.M.; Jensen, C.L.; Fraley, J.K.; Berretta, M.C.; Heird, W.C. A Randomized, Double-Blind, Place-Bo-Controlled Trial of Docosahexaenoic Acid Supplementation in Children with Attention-Deficit/Hyperactivity Disorder. J. Pediatrics 2001, 139, 189. [Google Scholar] [CrossRef]
- Richardson, A.J.; Puri, B. A Randomized Double-Blind, Placebo-Controlled Study of the Effects of Supplementation with Highly Unsaturated Fatty Acids on ADHD-Related Symptoms in Children with Specific Learning Difficulties. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2002, 26, 233–239. [Google Scholar] [CrossRef]
- Stevens, L.; Zhang, W.; Peck, L.; Kuczek, T.; Grevstad, N.; Mahon, A.; Zentall, S.S.; Arnold, L.E.; Burgess, J.R. EFA Supplementation in Children With Inattention, Hyperactivity, and Other Disruptive Behaviors. Lipids 2003, 38, 1007. [Google Scholar] [CrossRef]
- Widenhorn-Müller, K.; Schwanda, S.; Scholz, E.; Spitzer, M.; Bode, H. Effect of Supplementation with Long-Chain ω-3 Polyunsaturated Fatty Acids on Behavior and Cognition in Children With Attention deficit/Hyperactivity Disorder (ADHD): A Randomized Placebo-Controlled Intervention Trial. Prostaglandins Leukot. Essent. Fat. Acids 2014, 91, 49–60. [Google Scholar] [CrossRef]
- Harding, L.K.; Judah, D.R.; Gant, C.E. Outcome-Based Comparison of Ritalin Versus Food-Supplement Treated Children With AD/HD. Altern. Med. Rev. A J. Clin. Ther. 2003, 8, 319. [Google Scholar]
- Huss, M.; Völp, A.; Stauss-Grabo, M. Supplementation of Polyunsaturated Fatty Acids, Magnesium and Zinc in Children Seeking Medical Advice for Attention-Deficit/Hyperactivity Problems—An Observational Cohort Study. Lipids Health Dis. 2010, 9, 1–12. [Google Scholar] [CrossRef]
- Wu, Q.; Zhou, T.; Ma, L.; Yuan, D.; Peng, Y. Protective Effects of Dietary Supplementation with Natural ω-3 Polyunsaturated Fatty Acids on the Visual Acuity of School-Age Children With Lower IQ or Attention-Deficit Hyperactivity Disorder. Nutr. 2015, 31, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, S.; Hamazaki, T.; Terasawa, K. Effect of Docosahexaenoic Acid-Containing Food Administration on Symptoms of Attention-Deficit/Hyperactivity Disorder—A Placebo-Controlled Double-Blind Study. Eur. J. Clin. Nutr. 2004, 58, 467. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.; MacKinlay, E.; Dick, J.; MacDonald, D.; Boyle, R.; Glen, A. Essential Fatty Acids and Phospholipase A2 in Autistic Spectrum Disorders. Prostaglandins Leukot. Essent. Fat. Acids 2004, 71, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Bu, B.; Ashwood, P.; Harvey, D.; King, I.; de Water, J.; Jin, L.-W. Fatty Acid Compositions of Red Blood Cell Phospholipids in Children with Autism. Prostaglandins Leukot. Essent. Fat. Acids 2006, 74, 215–221. [Google Scholar] [CrossRef]
- Wiest, M.; German, J.; Harvey, D.; Watkins, S.; Hertz-Picciotto, I. Plasma Fatty Acid Profiles in Autism: A Case-Control Study. Prostaglandins Leukot. Essent. Fat. Acids 2009, 80, 221–227. [Google Scholar] [CrossRef]
- Yui, K.; Imataka, G.; Kawasak, Y.; Yamada, H. Increased ω-3 Polyunsaturated Fatty acid/Arachidonic Acid Ratios and Upregulation of Signaling Mediator in Individuals with Autism Spectrum Disorders. Life Sci. 2016, 145, 205–212. [Google Scholar] [CrossRef]
- Amminger, G.P.; Berger, G.E.; Schäfer, M.R.; Klier, C.; Friedrich, M.H.; Feucht, M. Omega-3 Fatty Acids Supplementation in Children with Autism: A Double-Blind Randomized, Placebo-Controlled Pilot Study. Biol. Psychiatry 2007, 61, 551–553. [Google Scholar] [CrossRef]
- Yui, K.; Koshiba, M.; Nakamura, S.; Kobayashi, Y. Effects of Large Doses of Arachidonic Acid Added to Docosahexaenoic Acid on Social Impairment in Individuals with Autism Spectrum Disorders: A Double-Blind, Placebo-Controlled, Randomized Trial. J. Clin. Psychopharmacol. 2012, 32, 200. [Google Scholar] [CrossRef]
- Ooi, Y.P.; Weng, S.-J.; Jang, L.Y.; Low, L.; Seah, J.; Teo, S.; Ang, R.; Lim, C.G.; Liew, A.; Fung, D.S.; et al. Omega-3 Fatty Acids in the Management of Autism Spectrum Disorders: Findings from an Open-Label Pilot Study in Singapore. Eur. J. Clin. Nutr. 2015, 69, 969–971. [Google Scholar] [CrossRef]
- Keim, S.A.; Gracious, B.; Boone, K.M.; A Klebanoff, M.; Rogers, L.K.; Rausch, J.; Coury, D.L.; Sheppard, K.W.; Husk, J.; Rhoda, D. ω-3 and ω-6 Fatty Acid Supplementation May Reduce Autism Symptoms Based on Parent Report in Preterm Toddlers. J. Nutr. 2018, 148, 227–235. [Google Scholar] [CrossRef]
- Johnson, C.R.; Handen, B.L.; Zimmer, M.; Sacco, K. Polyunsaturated Fatty Acid Supplementation in Young Children with Autism. J. Dev. Phys. Disabil. 2009, 22, 1–10. [Google Scholar] [CrossRef]
- Bent, S.; Bertoglio, K.; Ashwood, P.; Bostrom, A.; Hendren, R.L. A Pilot Randomized Controlled Trial of Omega-3 Fatty Acids for Autism Spectrum Disorder. J. Autism Dev. Disord. 2010, 41, 545–554. [Google Scholar] [CrossRef]
- Voigt, R.G.; Mellon, M.W.; Katusic, S.K.; Weaver, A.L.; Matern, D.; Mellon, B.; Jensen, C.L.; Barbaresi, W.J. Dietary Do-Cosahexaenoic Acid Supplementation in Children with Autism. J. Pediatric Gastroenterol. Nutr. 2014, 58, 715. [Google Scholar] [CrossRef]
- Parellada, M.; Llorente, C.; Calvo-Escalona, R.; Gutierrez, S.; Lázaro, L.; Graell, M.; Guisasola, M.; Dorado, M.L.; Boada, L.; Romo, J.; et al. Randomized Trial of Omega-3 for Autism Spectrum Disorders: Effect on Cell Membrane Composition and Behavior. Eur. Neuropsychopharmacol. 2017, 27, 1319–1330. [Google Scholar] [CrossRef]
- James, S.; Montgomery, P.; Williams, K. Omega-3 Fatty Acids Supplementation for Autism Spectrum Disorders (ASD). Cochrane Database Syst. Rev. 2011, CD007992. [Google Scholar] [CrossRef]
- Yeo, M.; Hughes, E. Eating Disorders—Early Identification in General Practice. Aust. Fam. Physician 2011, 40, 108. [Google Scholar]
- LeDoux, S.; Choquet, M.; Flament, M. Eating Disorders Among Adolescents in an Unselected French Population. Int. J. Eat. Disord. 1991, 10, 81–89. [Google Scholar] [CrossRef]
- Leichner, P.; Arnett, J.; Rallo, J.S.; Srikameswaran, S.; Vulcano, B. An Epidemiologic Study of Maladaptive Eating Attitudes in a Canadian School Age Population. Int. J. Eat. Disord. 1986, 5, 969–982. [Google Scholar] [CrossRef]
- Pastore, D.R.; Fisher, M.; Friedman, S.B. Abnormalities in Weight Status, Eating Attitudes, and Eating Behaviors Among Urban High School students: Correlations with Self-Esteem and Anxiety. J. Adolesc. Health 1996, 18, 312–319. [Google Scholar] [CrossRef]
- Tomori, M.; Rus-Makovec, M. Eating Behavior, Depression, and Self-Esteem in High School Students. J. Adolesc. Health 2000, 26, 361–367. [Google Scholar] [CrossRef]
- Holman, R.T.; E Adams, C.; A Nelson, R.; Grater, S.J.; A Jaskiewicz, J.; Johnson, S.B.; Erdman, J.W. Patients with Anorexia Nervosa Demonstrate Deficiencies of Selected Essential Fatty Acids, Compensatory Changes in Nonessential Fatty Acids and Decreased Fluidity of Plasma Lipids. J. Nutr. 1995, 125, 901. [Google Scholar]
- Langan, S.M.; Farrell, P.M. Vitamin E, Vitamin A and Essential Fatty Acid Status of Patients Hospitalized for Anorexia Nervosa. Am. J. Clin. Nutr. 1985, 41, 1054–1060. [Google Scholar] [CrossRef]
- Žák, A.; Vecka, M.; Tvrzická, E.; Hrubý, M.; Novák, F.; Papežová, H.; Lubanda, H.; Veselá, L.; Staňková, B. Composition of Plasma Fatty Acids and Non-Cholesterol Sterols in Anorexia Nervosa. Physiol. Res. 2005, 54, 443. [Google Scholar]
- Swenne, I.; Rosling, A. Omega-3 Essential Fatty Acid Status Is Improved During Nutritional Rehabilitation of Adolescent Girls with Eating Disorders and Weight Loss. Acta Paediatr. 2012, 101, 858–861. [Google Scholar] [CrossRef]
- Swenne, I.; Rosling, A.; Tengblad, S.; Vessby, B. Essential Fatty Acid Status in Teenage Girls with Eating Disorders and Weight Loss. Acta Paediatr. 2011, 100, 762–767. [Google Scholar] [CrossRef]
- Swenne, I.; Rosling, A.; Tengblad, S.; Vessby, B. Omega-3 Polyunsaturated Essential Fatty Acids Are Associated with Depression in Adolescents with Eating Disorders and Weight Loss. Acta Paediatr. Int. J. Paediatr. 2011, 100, 1610. [Google Scholar] [CrossRef]
- Ayton, A.K.; Azaz, A.; Horrobin, D.F. Rapid Improvement of Severe Anorexia Nervosa During Treatment with Ethyl-Eicosapentaenoate and Micronutrients. Eur. Psychiatry 2004, 19, 317–319. [Google Scholar] [CrossRef]
- Ayton, A.K.; Azaz, A.; Horrobin, D.F. A Pilot Open Case Series of Ethyl-EPA Supplementation in the Treatment of Anorexia nervosa. Prostaglandins, Leukot. Essent. Fat. Acids 2004, 71, 205–209. [Google Scholar] [CrossRef]
- Amminger, G.P.; Chanen, A.; Ohmann, S.; Klier, C.; Mossaheb, N.; Bechdolf, A.; Nelson, B.; Thompson, A.; McGorry, P.D.; Yung, A.; et al. Omega-3 Fatty Acid Supplementation in Adolescents with Borderline Personality Disorder and Ultra-High Risk Criteria for Psychosis: A Post Hoc Subgroup Analysis of a Double—Blind, Randomized Controlled Trial. Can. J. Psychiatry 2013, 58, 402–408. [Google Scholar] [CrossRef]
- Zanarini, M.C.; Stanley, B.; Black, D.W.; Markowitz, J.C.; Goodman, M.; Pilkonis, P.; Lynch, T.R.; Levy, K.; Fonagy, P.; Bohus, M.; et al. Methodological Considerations for Treatment Trials for Persons with Borderline Personality Disorder. Ann. Clin. Psychiatry 2010, 22, 75. [Google Scholar]
- Fristad, M.A. Evidence-Based Psychotherapies and Nutritional Interventions for Children with Bipolar Spectrum Disorders and Their Families. J. Clin. Psychiatry 2016, 77 (Suppl. E1), e04. [Google Scholar] [CrossRef] [PubMed]
- Pawełczyk, T.; Grancow, M.; Kotlicka-Antczak, M.; Trafalska, E.; Gębski, P.; Szemraj, J.; Żurner, N.; Pawełczyk, A. Omega-3 Fatty Acids in First-Episode Schizophrenia—A Randomized Controlled Study of Efficacy and Relapse Prevention (OFFER): Rationale, Design, and Methods. BMC Psychiatry 2015, 15, 1–13. [Google Scholar] [CrossRef] [PubMed]
- MDíaz-Marsá; Bardanca, S.G.; Tajima, K.; García-Albea, J.; Navas, M.; Carrasco, J.L. Psychopharmacological Treatment in Borderline Personality Disorder. Actas Espanolas De Psiquiatria 2008, 36, 39–49. [Google Scholar]
- Karaszewska, D.M.; Ingenhoven, T.; Mocking, R.J.T. Marine Omega-3 Fatty Acid Supplementation for Borderline Personality Disorder. J. Clin. Psychiatry 2021, 82. [Google Scholar] [CrossRef] [PubMed]
- Stoffers, J.M.; Lieb, K. Pharmacotherapy for Borderline Personality Disorder—Current Evidence and Recent Trends. Curr. Psychiatry Rep. 2015, 17, 534. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study Design | Country | No. | Age Group | Disease | Daily Dosage (g/d) | Duration | Rating Scale | Outcome | |
|---|---|---|---|---|---|---|---|---|---|
| Amminger et al., 2010 [50] | Randomised, double-blind, placebo controlled trial | Austria | 81 | 13–25 years | - Individuals at ultra-high risk of psychotic disorder. | 1.2g/d n-3 PUFAs or placebo | 12 weeks | - PANSS - MADRS - GAF - SCID-I/P | The cumulative conversion rates to psychotic disorder were 4.9% (2 of 41) in the n-3 group and 27.5% (11 of 40) in the placebo group. |
| Amminger et al., 2015 [53] | Post hoc subgroup analysis | Austria | 81 | 13–25 years | - Individuals at ultra-high risk of psychotic disorder. - BPD | 1.2g/d n-3 PUFAs or placebo | 12 weeks | - PANSS - MADRS - GAF | N-3 PUFAs provided improvements in functioning and symptoms. |
| Mcgorry et al., 2017 | Randomised, double-blind, placebo controlled trial | Australia | 304 | 13–40 years | - Individuals at ultra-high risk of psychotic disorder. | 1.4 g/d n-3 PUFAs together with CBCM or placebo with CBCM or placebo | 24 weeks | - YMRS - BPRS - CDRS | No significant difference between ω-3 PUFAs and placebo in transition rate. |
| Pawełczyk et al., 2016 [51] | Randomised, double-blind, placebo controlled trial | Poland | 71 | 16–35 years | -Individuals at first-episode schizophrenia | 2.2 g/d n-3 PUFAs or placebo | 26 weeks | - PANSS - CDSS - GAF - CGI-S | 50% improvement in total PANSS score was achieved significantly more frequently in the n-3 PUFAS group than in the placebo group. |
| Study Design | Country | No. | Age Group | Disease | Daily Dosage (g/d) | Duration | Rating Scale | End Point | |
|---|---|---|---|---|---|---|---|---|---|
| Wozniak et al., 2007 [59] | Open label trial | USA | 20 | 6–17 years | - Bipolar spectrum disorder | 1290 mg–4300 mg/d n-3 PUFAs | 8 weeks | - YMRS - BPRS - SANS - MADRS | 8.9 ± 2.9 point reduction in the YMRS scores (p < 0.001). |
| Clayton et al., 2009 [61] | Open label trial | Australia | 18 | mean age = 16.1 ± 0.81 years | - Bipolar spectrum disorder | 360 mg/day EPA and 1560 mg/day DHA | 6 weeks | - YMRS - HAM-D - C-GAS) - CBCL-PR, | Clinician ratings of YMRS and HAM-D were significantly lower (p = 0.004 and p = 0.002) and C-GAS significantly higher (p < 0.001) following supplementation. |
| Fristad et al., 2015 [64] | Randomised controlled trial | USA | 23 | 7–14 years | - BP-NOS - CYC | 2000 mg/day of n-3 PUFAs versus placebo and IF-PEP versus AM using a 2 · 2 design (O3 + PEP: n = 5; O3 + AM: n = 5; placebo + PEP: n = 7; placebo + AM: n = 6) | 12 weeks | - K-SADS - KDRS - KMRS - CDRS-R - YMRS | Manic symptoms improved over time without significant treatment effects. Effect of IF-PEP on child depression compared with AM was medium (d = 0.63, CDRS-R) to large (d = 1.24, KDRS). Effect of n-3 PUFAs on depression was medium (d = 0.48, KDRS). |
| Vesco et al., 2018 [68] | Randomised controlled trial | USA | 95 | 7–14 years | - BP-NOS or CYC (n = 23) - MDD (n= 72) | - 1.87 g/d n3-PUFAs in monotherapy - PEP monotherapy - PEP + n3-PUFAs | 12 week | - BRIEF - GEC - BRI - YMRS | PUFAs supplementation were associated with significant improvements in executive functions and in dysphoric mood, irritability, and self-esteem. |
| Fristad et al., 2021 [67] | Naturalistic follow-up study | USA | 38 | 11–19 years | - BP-NOS or CYC (n = 13) - MDD (n = 25) | 2–5 years after participation in randomised clinical trials (RCTs) Fristad et al., 2015 | - Mental Health Services and Medication Grids - CDRS - YMRS - BRIEF - CGAS - The OATS Family Experience Assessment—Child and Parent Report (FEA) | Compared to baseline depressive symptoms, participants had significantly lower CDRS-R scores at follow-up, with a small effect size and were functioning better (CGAS scores) with a medium effect size. Manic symptom severity, executive functioning, and global functioning remained comparable to end of RCT. The majority of parents and youth reported improved youth emotion regulation skills and family communication. |
| Study Design | Country | No. | Age Group | Disease | Daily Dosage (g/d) | Duration | Rating Scale | End Point | |
|---|---|---|---|---|---|---|---|---|---|
| Nemets et al., 2006 [76] | Randomised controlled trial | Israel | 28 | 6–12 years | - MDD | 400 mg/d EPA and 200 mg/d DHA or placebo | 4 weeks | - CDRS - CDI - CGI | Highly significant effects of omega-3 on symptoms using the CDRS (p = 0.003), CDI (p < 0.005), and CGI (p = 0.002). |
| Young et al., 2017 [78] | Randomised controlled trial | USA | 72 | 7–14 years | - MDD (n = 37) - dysthymic disorder (n = 5) -depressive disorder not otherwise specified (n = 30) | - 2 g/d n3-PUFAs in monotherapy - PEP in monotherapy- PEP + n3-PUFA - placebo | 12 weeks | - SNAP-IV - ECBI | N-3 PUFAs yielded more favourable trajectories than placebo on the SNAP-IV Hyperactivity/Impulsivity subscale (p = 0.034, d = 0.44) and marginally more favourable on Total (p = 0.080, d = 0.42), and Inattention scores (p = 0.059, d = 0.49). |
| Vesco et al., 2018 [68] | Randomised controlled trial | USA | 95 | 7–14 years | - BP-NOS or CYC (n = 23) - Depressive disorder (n = 72) | - 1.87 g/d n3-PUFAs in monotherapy - PEP monotherapy - PEP + n3-PUFAs | 12 weeks | - BRIEF - GEC - BRI - YMRS | PUFAs supplementation were associated with significant improvement in executive functions and in dysphoric mood, irritability, and self-esteem. |
| Trebatická et al., 2020 [77] | Randomised, double-blind, placebo controlled trial | Slovakia | 60 | 7–18 years | -MDD (n = 31) -Mixed anxiety and depressive disorder (n = 29) | 2400 mg of total omega-3 PUFAs/day or placebo | 12 weeks | - CDI | PUFAs supplementation were associated with reductions in Children’s Depression Inventory (CDI) scores. |
| Study Design | Country | No. | Age Group | Disease | Daily Dosage (g/d) | Duration | Rating Scale | End Point | |
|---|---|---|---|---|---|---|---|---|---|
| Hamazaki et al., 2005 [83] | Randomised, double-blind, placebo controlled trial | Japan | 22 | 18–24 years | Healthy subjects | - EPA 400 mg/d + DHA 300 mg/d Or placebo | 8 weeks | EP, NE, dopamine, cortisol and corticotropin concentration | PUFAs supplementation were associated with a decreased activation of the hypothalamic–pituitary–adrenal (HPA) axis. |
| Kiecolt-Glaser et al., 2011 [84] | Randomised, double-blind, placebo controlled trial | USA | 68 | 21–29 years | Healthy subjects | EPA 2085 mg/d + DHA 348 mg/d or placebo | 12 weeks | -Beck Anxiety Inventory | PUFAs supplementation were associated with 20% reduction in anxiety symptoms, without significant change in depressive symptoms. |
| Manos et al., 2018 [85] | Randomised, double-blind, placebo controlled trial | USA | 24 | 12–21 years | - anxiety disorder and AN | - EPA 2120 mg/d + DHA 600 mg/d or placebo | 12 weeks | - BAIT - CES-D - EAT-26 | No evidence that omega-3 PUFA benefited anxiety. |
| Robinson et al., 2019 [86] | Randomised, double-blind, placebo controlled trial | USA | 50 | 15–40 years | - early psychosis and anxiety | - EPA 740 mg/d and DHA 400 mg/d or placebo | 16 weeks | - BPRS - SANS - CGI - SAFTEE-SI | Implementation with n-3 PUFAs was found mainly useful on depression-anxiety domain measured with the Brief Psychiatric Rating Scale (BPRS). |
| Study Design | Country | No. | Age Group | Disease | Daily Dosage (g/d) | Duration | Rating Scale | End Point | |
|---|---|---|---|---|---|---|---|---|---|
| Voigt et al., 2001 [98] | Randomized, double-blind, placebo controlled trial | USA | 63 | 6–12 years | ADHD | - DHA 345 mg/d or placebo | 16 weeks | -TOVA - Children’s Colour Trails test - CBCL - CRS | Supplementation does not decrease symptoms of ADHD. |
| Richardson & Puri, 2002 [99] | Randomized, double-blind, placebo controlled trial | UK | 41 | 8–12 years | Learning disabilities | EPA186 mg/d + DHA 480 mg/d + GLA 96 mg/d + vitamin E 60 IU/d + AA 42 mg/d + LA (864 mg/d +thyme oil 8 mg/d or placebo | 12 weeks | CPRS-L | Significant benefit in alleviating many ADHD-related symptoms in children with specific learning difficulties. |
| Harding et al., 2003 [102] | double-blind, placebo controlled trial | USA | 20 | 7–12 years | ADHD | EPA 180 mg/d + DHA 120 mg/d + GLA 45 mg/d OR methilphenidate | 4 weeks | - IVA/CPT | Supplementation resulted in equivalent improvements in attention and self-control as methylphenidate. |
| Hirayama et al., 2004 [105] | Randomized, double-blind, placebo controlled trial | Japan | 40 | 6–12 years | ADHD | DHA 515 mg/d + EPA 100 mg/d or placebo | 8 weeks | - AD/HD-related symptoms - Aggression assessment- Development Test of Visual Perception - Visual and auditory short-term memory; - Developmental test of visual–motor integration – Continuous performance test - Impatience test. | No improvement of ADHD. |
| Widenhorn-Müller et al., 2014 [101] | Randomized, double-blind, placebo controlled trial | Germany | 95 | 6–12 years | ADHD | EPA 600 mg/d +DHA 120 mg/d or placebo | 16 weeks | - CBCL - TRS | No effect on cognitive measures and parent- and teacher-rated behaviour. |
| Wu et al., 2015 [104] | Randomized, double-blind, placebo controlled trial | China | 179 | 7–12 years | ADHD (n = 91) Lower IQs (n = 88) | eggs rich in n-3 PUFAs or normal eggs | 12 weeks | - Mann–Whitney test - Wilcoxon Signed Ranks test | Improvements both in visual acuity and in the RBC fatty acid profile. |
| Study Design | Country | No. | Age Group | Disease | Daily Dosage (g/d) | Duration | Rating Scale | Outcome | |
|---|---|---|---|---|---|---|---|---|---|
| Amminger et al., 2007 [110] | Randomised, double-blind, placebo controlled trial | Austria | 13 | 5–17 years | ASD | EPA 840 mg/d + DHA 700 mg/d Or placebo | 6 weeks | - ABC | Advantage of n-3 PUFAs compared with placebo for hyperactive behaviours and stereotypy. |
| Johnson et al., 2010 [114] | Prospective, open label trial | USA | 23 | 44.7 m (s.d. = 7.63) years | ASD (n = 17)PDD, NOS (n = 6) | DHA 400 mg/d | 12 weeks | - CBCL - ADOS | No clinical improvements were observed. |
| Bent et al., 2011 [115] | Pilot randomised placebo controlled trial | USA | 27 | 3–8 years | ASD | EPA 350 mg/d + DHA 230 mg/d or placebo | 12 weeks | - SRS - CGI - BASC - ABC | Not statistically significant improvements in the treatment group vs. the placebo. |
| Yui et al., 2012 [111] | Randomised, double-blind, placebo controlled trial | Japan | 13 | 6–28 years | ASD | DHA 240 mg/d + ARA 240 mg/dor placebo | 16 weeks | - SRS - ABC | Improvement of social deficit in individuals with ASD. |
| Voigt et al., 2014 [116] | Randomised, double-blind, placebo controlled trial | USA | 48 | 3–10 years | ASD | DHA 200 mg/d or placebo | 24 weeks | - CGI-I - ABC - CDI - BASC | No improvement in core symptoms of autism. |
| Ooi et al., 2015 [112] | Open label trial | Singapore | 41 | 7–18 years | ASD | DHA 840 mg/d + EPA 192 mg/d | 12 weeks | - SRS-P - CBCL | Significant improvements on all subscales of the Social Responsiveness Scale (p < 0.01) and the Social and Attention Problems syndrome scales of the Child Behaviour Checklist (p < 0.05). |
| Parellada et al., 2017 [117] | Randomized, crossover, placebo controlled trial | SPAIN | 68 | 5–17 years | ASD | PUFAs 962 mg/d for children and 1155 mg/d for adolescents or placebo | 8 weeks | - SRS | No treatment effect. |
| Keim et al., 2018 [113] | Randomized, double-blind, placebo controlled trial | USA | 31 | 18–38 years | ASD | EPA 338 mg/d + DHA 225 mg/d + GLA 83 mg/d or placebo | 12 weeks | - BITSEA - PDDST-II - Ages and Stages Questionnaire-Social Emotional | Significant improvements in ASD symptoms measured by the BITSEA, but no significant effects were observed on other outcome measures. |
| Study Design | Country | No. | Age Group | Disease | Daily Dosage (g/d) | Duration | Rating Scale | Outcome | |
|---|---|---|---|---|---|---|---|---|---|
| Ayton et al., 2004 [130] | Case report | UK | 1 | 15 y | AN | EPA 1 g/day | 12 weeks | BMI | Improvements in both weight and food intake. |
| Ayton et al., 2004 [131] | Pilot open case series | UK | 10 | 13–22 y | AN | EPA 1 g/day | 6–8 weeks | BMI | Improvement of general functioning and mood. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bozzatello, P.; Blua, C.; Rocca, P.; Bellino, S. Mental Health in Childhood and Adolescence: The Role of Polyunsaturated Fatty Acids. Biomedicines 2021, 9, 850. https://doi.org/10.3390/biomedicines9080850
Bozzatello P, Blua C, Rocca P, Bellino S. Mental Health in Childhood and Adolescence: The Role of Polyunsaturated Fatty Acids. Biomedicines. 2021; 9(8):850. https://doi.org/10.3390/biomedicines9080850
Chicago/Turabian StyleBozzatello, Paola, Cecilia Blua, Paola Rocca, and Silvio Bellino. 2021. "Mental Health in Childhood and Adolescence: The Role of Polyunsaturated Fatty Acids" Biomedicines 9, no. 8: 850. https://doi.org/10.3390/biomedicines9080850
APA StyleBozzatello, P., Blua, C., Rocca, P., & Bellino, S. (2021). Mental Health in Childhood and Adolescence: The Role of Polyunsaturated Fatty Acids. Biomedicines, 9(8), 850. https://doi.org/10.3390/biomedicines9080850