
Sharing the Same Perspective. Mental Disorders and Central Serous Chorioretinopathy: A Systematic Review of Evidence from 2010 to 2020

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Processes
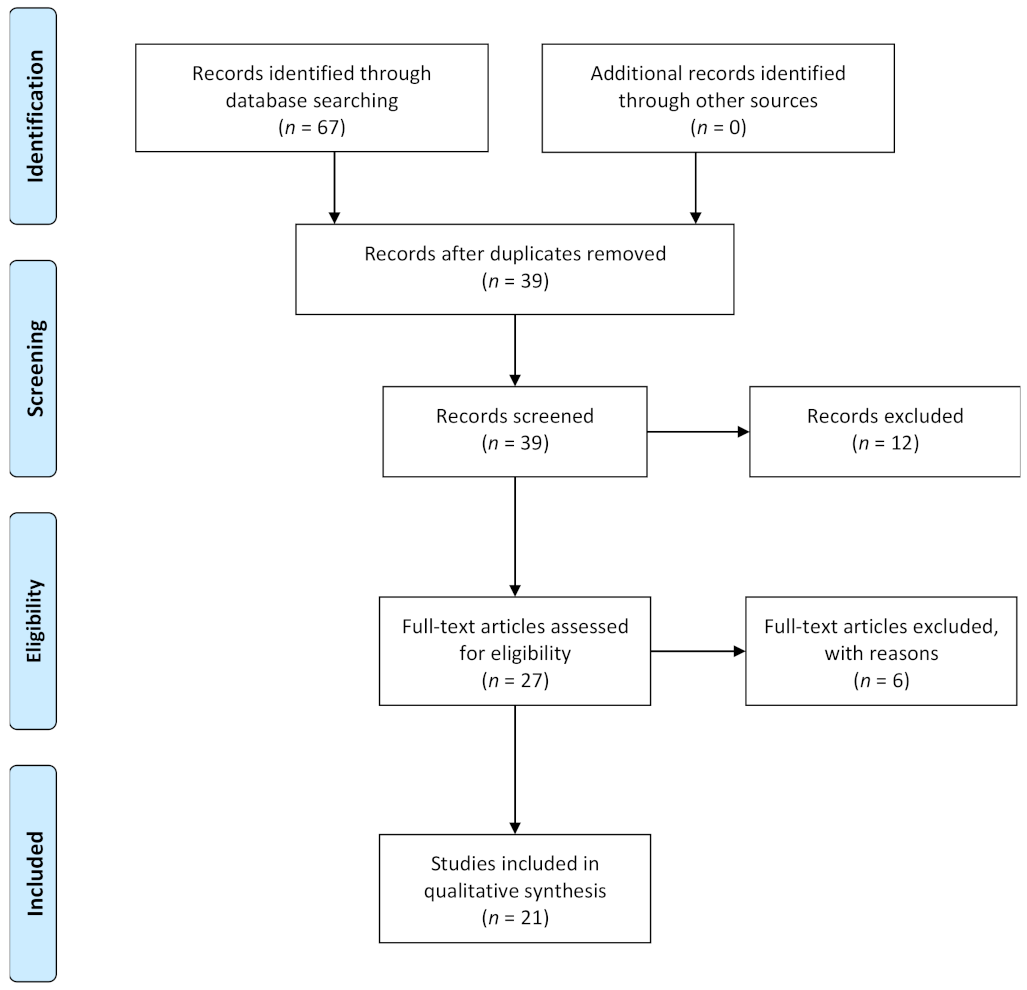
2.2. Study Selection
2.3. Data Extraction
3. Results
3.1. Acute CSC
3.2. Chronic CSC
3.3. Recurrent CSC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Greenberg, P.E.; Fournier, A.A.; Sisitsky, T.; Pike, C.T.; Kessler, R.C. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J. Clin. Psychiatry 2015, 76, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Eppelmann, L.; Parzer, P.; Salize, H.J.; Voss, E.; Resch, F.; Kaess, M. Stress, mental and physical health and the costs of health care in German high school students. Eur. Child Adolesc. Psychiatry 2020, 29, 1277–1287. [Google Scholar] [CrossRef] [PubMed]
- De Hert, M.; Detraux, J.; Vancampfort, D. The intriguing relationship between coronary heart disease and mental disorders. Dialogues Clin. Neurosci. 2018, 20, 31–40. [Google Scholar] [CrossRef]
- Novellino, F.; Saccà, V.; Donato, A.; Zaffino, P.; Spadea, M.F.; Vismara, M.; Arcidiacono, B.; Malara, N.; Presta, I.; Donato, G. Innate Immunity: A Common Denominator between Neurodegenerative and Neuropsychiatric Diseases. Int. J. Mol. Sci. 2020, 21, 1115. [Google Scholar] [CrossRef]
- Prince, M.; Patel, V.; Saxena, S.; Maj, M.; Maselko, J.; Phillips, M.R.; Rahman, A. No health without mental health. Lancet 2007, 370, 859–877. [Google Scholar] [CrossRef] [PubMed]
- Borooah, S.; Sim, P.Y.; Phatak, S.; Moraes, G.; Wu, C.Y.; Cheung, C.M.G.; Pal, B.; Bujarborua, D. Pachychoroid spectrum disease. Acta Ophthalmol. 2020. Epub ahead of print. [Google Scholar] [CrossRef]
- Liew, G.; Quin, G.; Gillies, M.; Fraser-Bell, S. Central serous chorioretinopathy: A review of epidemiology and pathophysiology. Clin. Exp. Ophthalmol. 2013, 41, 201–214. [Google Scholar] [CrossRef] [PubMed]
- Gülkaş, S.; Şahin, Ö. Current Therapeutic Approaches to Chronic Central Serous Chorioretinopathy. Turk. J. Ophthalmol. 2019, 49, 30–39. [Google Scholar] [CrossRef]
- Scarinci, F.; Ghiciuc, C.M.; Patacchioli, F.R.; Palmery, M.; Parravano, M. Investigating the Hypothesis of Stress System Dysregulation as a Risk Factor for Central Serous Chorioretinopathy: A Literature Mini-Review. Curr. Eye Res. 2019, 44, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Bazzazi, N.; Ahmadpanah, M.; Akbarzadeh, S.; Seif Rabiei, M.A.; Holsboer-Trachsler, E.; Brand, S. In patients suffering from idiopathic central serous chorioretinopathy, anxiety scores are higher than in healthy controls, but do not vary according to sex or repeated central serous chorioretinopathy. Neuropsychiatr. Dis. Treat. 2015, 11, 1131–1136. [Google Scholar] [CrossRef][Green Version]
- Chen, Y.Y.; Huang, L.Y.; Liao, W.L.; Chou, P. Association between Central Serous Chorioretinopathy and Risk of Depression: A Population-Based Cohort Study. J. Ophthalmol. 2019, 2019, 2749296. [Google Scholar] [CrossRef]
- Bousquet, E.; Dhundass, M.; Lehmann, M.; Rothschild, P.R.; Bayon, V.; Leger, D.; Bergin, C.; Dirani, A.; Beydoun, T.; Behar-Cohen, F. Shift Work: A Risk Factor for Central Serous Chorioretinopathy. Am. J. Ophthalmol. 2016, 165, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Deng, T.; Zhang, J. Risk factors for central serous chorioretinopathy: A Systematic Review and Meta-Analysis. Retina 2016, 36, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Penas, S.; Castro, P.; Pereira, G.; Oliveira, A.M.; Carneiro, Â.M.; Rocha-Sousa, A.; Azevedo, E.; Falcão-Reis, F.M. Cerebral Neurovascular Coupling Impairment in Central Serous Chorioretinopathy. Ophthalmic Res. 2020. Epub ahead of print. [Google Scholar] [CrossRef]
- Tien, P.T.; Lai, C.Y.; Lin, C.J.; Chen, W.L.; Lin, P.K.; Muo, C.H.; Tsai, Y.Y.; Wan, L.; Ho, W.C.; Lin, H.J. Increased Risk of Central Serous Chorioretinopathy among Patients with Nonorganic Sleep Disturbance. J. Ophthalmol. 2020, 2020, 1712503. [Google Scholar] [CrossRef]
- Scarinci, F.; Patacchioli, F.R.; Ghiciuc, C.M.; Pasquali, V.; Bercea, R.M.; Cozma, S.; Parravano, M. Psychological Profile and Distinct Salivary Cortisol Awake Response (CAR) in Two Different Study Populations with Obstructive Sleep Apnea (OSA) and Central Serous Chorioretinopathy (CSC). J. Clin. Med. 2020, 9, 2490. [Google Scholar] [CrossRef] [PubMed]
- Scarinci, F.; Patacchioli, F.R.; Palmery, M.; Pasquali, V.; Costanzo, E.; Ghiciuc, C.M.; Parravano, M. Diurnal trajectories of salivary cortisol and α-amylase and psychological profiles in patients with central serous chorioretinopathy. Chronobiol. Int. 2020, 37, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Xu, G.; Chang, Q.; Ye, X.; Li, L.; Jiang, C.; Zhao, Q. Risk Factors for Persistent or Recurrent Central Serous Chorioretinopathy. J. Ophthalmol. 2019, 2019, 5970659. [Google Scholar] [CrossRef]
- Jain, M. Quetiapine associated Central Serous Chorioretinopathy: Implicit role of serotonin and dopamine pathways. Indian J. Ophthalmol. 2019, 67, 292–294. [Google Scholar] [CrossRef]
- Kim, Y.K.; Woo, S.J.; Park, K.H.; Chi, Y.K.; Han, J.W.; Kim, K.W. Association of Central Serous Chorioretinopathy with Psychosocial Factors is Dependent on Its Phase and Subtype. Korean J. Ophthalmol. 2018, 32, 281–289. [Google Scholar] [CrossRef]
- Nicholson, B.P.; Ali Idris, A.M.; Bakri, S.J. Central Serous Chorioretinopathy: Clinical Characteristics Associated with Visual Outcomes. Semin. Ophthalmol. 2018, 33, 804–807. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.; Li, M.; Zhang, X.; Peng, Y.; Wen, F. Poor Sleep Quality Is the Risk Factor for Central Serous Chorioretinopathy. J. Ophthalmol. 2018, 2018, 9450297. [Google Scholar] [CrossRef]
- Matet, A.; Daruich, A.; Zola, M.; Behar-Cohen, F. Risk factors for recurrences of central serous chorioretinopathy. Retina 2018, 38, 1403–1414. [Google Scholar] [CrossRef] [PubMed]
- Balkarli, A.; Erol, M.K.; Yalcinkaya, S.; Erol, R.S. Frequency of Erectile Dysfunction in Males with Central Serous Chorioretinopathy. Semin. Ophthalmol. 2018, 33, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Balkarli, A.; Erol, M.K.; Yucel, O.; Akar, Y. Frequency of fibromyalgia syndrome in patients with central serous chorioretinopathy. Arq. Bras. Oftalmol. 2017, 80, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Setrouk, E.; Hubault, B.; Vankemmel, F.; Zambrowski, O.; Nazeyrollas, P.; Delemer, B.; Durlach, V.; Ducasse, A.; Arndt, C. Circadian disturbance and idiopathic central serous chorioretinopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2016, 254, 2175–2181. [Google Scholar] [CrossRef] [PubMed]
- Uhumwangho, O.M.; Momoh, R.O. Central serous chorioretinopathy in Benin City, Nigeria. Ann. Afr. Med. 2015, 14, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.S.; Weng, S.F.; Chang, C.; Wang, J.J.; Wang, J.Y.; Jan, R.L. Associations Between Topical Ophthalmic Corticosteroids and Central Serous Chorioretinopathy: A Taiwanese Population-Based Study. Investig. Ophthalmol. Vis. Sci. 2015, 56, 4083–4089. [Google Scholar] [CrossRef] [PubMed]
- Sahin, A.; Bez, Y.; Kaya, M.C.; Türkcü, F.M.; Sahin, M.; Yüksel, H. Psychological distress and poor quality of life in patients with central serous chorioretinopathy. Semin. Ophthalmol. 2014, 29, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Tsai, D.C.; Chen, S.J.; Huang, C.C.; Chou, P.; Chung, C.M.; Huang, P.H.; Lin, S.J.; Chen, J.W.; Chen, T.J.; Leu, H.B.; et al. Epidemiology of idiopathic central serous chorioretinopathy in Taiwan, 2001–2006: A population-based study. PLoS ONE 2013, 8, e66858. [Google Scholar] [CrossRef] [PubMed]
- Fok, A.C.; Chan, P.P.; Lam, D.S.; Lai, T.Y. Risk factors for recurrence of serous macular detachment in untreated patients with central serous chorioretinopathy. Ophthalmic. Res. 2011, 46, 160–163. [Google Scholar] [CrossRef] [PubMed]
- DeSoto, M.C.; Salinas, M. Neuroticism and cortisol: The importance of checking for sex differences. Psychoneuroendocrinology 2015, 62, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Bujarborua, D.; Borooah, S.; Dhillon, B. Getting serious with retinopathy: Approaching an integrated hypothesis for central serous chorioretinopathy. Med. Hypotheses. 2013, 81, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Karska-Basta, I.; Pociej-Marciak, W.; Chrząszcz, M.; Kubicka-Trząska, A.; Romanowska-Dixon, B.; Sanak, M. Altered plasma cytokine levels in acute and chronic central serous chorioretinopathy. Acta Ophthalmol. 2021, 99, e222–e231. [Google Scholar] [CrossRef] [PubMed]
- Ayyildiz, D.; Ayyildiz, T. Central choroidal thickness in children and adolescents with anxiety disorders: Enhanced depth imaging optical coherence tomography findings. Int. J. Ophthalmol. 2020, 13, 1580–1585. [Google Scholar] [CrossRef]
- Sahbaz, C.; Elbay, A.; Ozcelik, M.; Ozdemir, H. Insomnia Might Influence the Thickness of Choroid, Retinal Nerve Fiber and Inner Plexiform Layer. Brain Sci. 2020, 10, 178. [Google Scholar] [CrossRef]
- Keskinruzgar, A.; Kalenderoglu, A.; Yapici Yavuz, G.; Koparal, M.; Simsek, A.; Karadag, A.S.; Utkun, M. Investigation of neurodegenerative and inflammatory processes in sleep bruxism. CRANIO 2020, 38, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Polat, S.; Gediz, B.S.; Ercan, A.C.; Kaim, M.; Hocaoglu, C. The Place of Optical Coherence Tomography in Patients with Obsessive Compulsive Disorder. Eurasian J. Med. 2019, 51, 237–241. [Google Scholar] [CrossRef]
- Read, S.A.; Pieterse, E.C.; Alonso-Caneiro, D.; Bormann, R.; Hong, S.; Lo, C.H.; Richer, R.; Syed, A.; Tran, L. Daily morning light therapy is associated with an increase in choroidal thickness in healthy young adults. Sci. Rep. 2018, 8, 8200. [Google Scholar] [CrossRef]
- Kalenderoglu, A.; Çelik, M.; Sevgi-Karadag, A.; Egilmez, O.B. Optic coherence tomography shows inflammation and degeneration in major depressive disorder patients correlated with disease severity. J. Affect. Disord. 2016, 204, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Nelson, E.E.; Guyer, A.E. The development of the ventral prefrontal cortex and social flexibility. Dev. Cogn. Neurosci. 2011, 1, 233–245. [Google Scholar] [CrossRef]
- Genovese, G.; Meduri, A.; Muscatello, M.; Gangemi, S.; Cedro, C.; Bruno, A.; Aragona, P.; Pandolfo, G. Central Serous Chorioretinopathy and Personality Characteristics: A Systematic Review of Scientific Evidence over the Last 10 Years (2010 to 2020). Medicina 2021, 57, 628. [Google Scholar] [CrossRef]


{kind=link}
| Number | Search Term |
|---|---|
| 1 | “Central serous chorioretinopathy” |
| 2 | “Mental disorder” |
| 3 | “anxiety” |
| 4 | “sleep disorder” |
| 5 | “insomnia” |
| 6 | “depression” |
| 7 | “panic” |
| 8 | “psychiatry” |
| 9 | 1 AND 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10 |
| 10 | English OR Italian [language] |
| 11 | up to 31 December 2020 [publication date] |
| Reference | Study Design | Aim | Subjects | Assessment | Main Findings |
|---|---|---|---|---|---|
| [15] | Case-control study | To investigate cerebrovascular regulation and anxiety in Central Serous Chorioretinopathy (CSC). | 20 CSC patients (acute, chronic, inactive) and 14 healthy controls (HC) | State-Trait Anxiety Inventory (STAI) | Neurovascular Coupling was negatively associated with STAI scores, especially anxiety-state scores (r = −0.602, p = 0.002). |
| [16] | Retrospective cohort study | to investigate nonorganic sleep disturbance (NOSD) and CSC. | 53.743 NOSD patients without CSC, 214.972 random controls. | / | NOSD patients have a higher incidence of CSC than controls (HR, 1.65; 95% CI, 1.34–2.02). In the NOSD groups, subjects using sleeping pills had an even higher CSC risk (1.72-fold, 95% CI, 1.35–2.20). |
| [17] | Case-control study | To investigate obstructive sleep apnea (OSA) and CSC. | 14 OSA patients and 14 matched HC; 14 acute CSC patients and 14 matched HC. | Hamilton Rating Scale for Depression (HAM-D); The Hamilton Anxiety Rating Scale (HAM-A), and the Daily Hassles Scale (DHS) | CSC subjects showed a medium level of perceived stress (scores between 76 and 115 on the DHS scale), HDS and HAM-D scores were significantly higher than controls (p < 0.001; p < 0.05); no anxiety was reported. |
| [18] | Cross-sectional observational study | To investigate stress, psychological profile, and CSC. | 17 initial acute CSC patients and 17 HC. | The Positive and Negative Affect Schedule (PANAS); STAI; The Beck Depression Inventory-II (BDI-II); DHS. | CSC group scores were higher than control on the negative subscale of the PANAS (p = 0.023), the DHS (p < 0.001), and the BDI-II (p = 0.036). No significant differences in the STAI scores were found. |
| [19] | Cross sectional | To investigate risk factors for chronic CSC. | 20 First episode CSC, 118 chronic CSC (46 persistent CSC; 72 recurrent CSC). | Insomnia Severity Index (ISI) | Higher Insomnia Severity Index score is associated with persistent or recurrent CSC (p = 0.015). |
| [11] | Retrospective cohort study | To investigate the risk for depression in CSC patients. | 25,939 CSC patients (first onset and recurrent) and 103,756 controls. | / | CSC group had a significantly higher risk for depression (p < 0.0001; HR = 1.29); treatment of CSC did not significantly reduce the risk for depression (HR = 0.85). |
| [20] | Case report | To describe Quetiapine administration and possible related CSC. | A 30-year-old male with insomnia | / | After the withdrawal of medication, he showed a marked reduction in both signs and symptoms of CSC. He showed recurrence of disease when resumed quetiapine 10 months later. |
| [21] | Case-control study | To investigate psychological dimensions and CSC phases and subtypes | 9 chronic CSC and 10 acute CSC (active CSC phase), 18 inactive CSC phase, and 37 HC | STAI; BDI; Social Readjustment Rating Scale; the Coping Inventory for Stressful Situations; Medical Outcomes Study Social Support Survey. | Inactive CSC groups results did not differ in all psychological dimensions compared with HC. Acute CSC patients reported higher scores in depression (p = 0.029), the severity of depression showed linear correlation with the choroidal pathology (R2 = 0.622; p = 0.007). Chronic active CSC was associated with stress level (p = 0.024). |
| [22] | Retrospective cohort study | To investigate clinical characteristics and visual outcomes in CSC. | 258 CSC patients | / | Use of psychiatric medication at presentation was protective for vision loss (p = 0.0066). There was a trend toward a protective effect with the use of beta-blockers, known for the anxiolytic effect (p = 0.060). |
| [23] | Case-control study | To investigate sleep quality and CSC. | 134 treatment-naive CSC patients and 134 HC | Depression Anxiety Stress Scales 21-item version (DASS-21); The Epworth Sleepiness Scale (ESS); The Pittsburgh Sleep Quality Index (PSQI) | Poor sleep quality (PSQI > 5) and stress (p < 15) was significantly more frequent in CSC groups than in HC (p < 0.0001; p = 0.002). CSC patients showed more frequent relevant depression (p > 10) and anxiety (p > 8) symptoms than controls (p = 0.001; p = 0.008). |
| [24] | Retrospective Case series | To investigate risk factors for recurrent CSC. | 46 patients with acute CSC | / | History of depression, psychological stress, and sleep disorder was not associated with recurrences of CSC. |
| [25] | Case-control Study | To investigate CSC and erectile dysfunction (ED). | 58 patients with CSC (12 acute, 46 chronic), 99 HC. | BDI; BAI; The 15-question Index of Erectile Function-15 (IIEF-15). | CSC patients showed higher incidence of erectile dysfunction than controls (p < 0.001). Sexual desire score at IIEF-15 was negatively associated with CSC duration (p = 0.025). Sexual satisfaction was higher in acute CSC than chronic CSC group (p = 0.016). |
| [26] | Case-control Study | To investigate fibromyalgia (Fm) among CSC patients. | 83 patients with CSC (23 acute, 58 chronic), and 201 HC. | BAI; BDI. | In the CSC group, patients with Fm showed higher scores in BDI and BAI scales than patients without Fm (p < 0.001). |
| [27] | Case-control study | To investigate circadian rhythm and CSC. | 29 chronic CSC; 29 patients non-CSC. | The PSQI; The Epworth questionnaire; The Hospital Anxiety and Depression scale | There were no significant differences between the two groups in sleeping, depressive and anxiety disorders, or psychopharmacologic medication use. |
| [12] | Case-control study | To investigate sleep disturbances and CSC. | 40 active CSC (26 acute; 14 chronic) and 40 HC | ISI. | CSC patients had significantly more sleep disturbance than HC (p < 0.001), especially in chronic than in the acute subtype (p < 0.05). There was no significant difference between the two groups about depression. |
| [28] | Descriptive case series | To investigate clinical presentation in CSC. | 5 CSC | / | All patients had a positive history of underlying anxiety/stressful conditions. |
| [29] | Case-control study | To investigate corticosteroid use and CSC. | 2.921 acute CSC; 17.526 controls | / | Patients with CSC had a significantly higher prevalence of psychiatric disease (p < 0.001). |
| [10] | Case control study | To investigate anxiety associated with the occurrence of CSC. | 17 CSC at first episode (8 female, 9 male), 13 CSC at second episode (5 female, 8 male); 30 HC. | HAM-A | Anxiety scores were significantly higher in CSC patients compared with HC (p-value not reported), independently from sex and number of episodes. No statistically significant correlations were observed between the anxiety scores and choroidal alteration and duration of the CSC episode |
| [30] | Case-control study | To investigate Quality of Life in CSC patients | 30 acute CSC patients, 30 HC. | the Symptom Checklist 90-R (SCL-90R), Short Form-36 (SF-36) | CSC group showed higher scores than controls in all symptomatic dimensions at SCL-90-R (global severity index p = 0.001) and lower score at all subscale SF-36 except bodily pain. They found a negative correlation between depression subscale scores and visual acuity (r = −0.425, p = 0.04) |
| [31] | Retrospective cohort study | To investigate risk factors for CSC unrelated to corticosteroid use. | 786 CSC patients (500 males), 3606 controls (2294 male). | / | Exposure to anti-anxiety drugs within a one-year period before enrolment was independently associated with idiopathic CSC among males only (OR, 1.63). |
| [32] | Retrospective longitudinal study | To investigate risk factors for recurrence in CSC | 73 CSC patients | / | Patients with a history of psychiatric illness were associated with an increased risk of CSC recurrence (p = 0.007). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pandolfo, G.; Genovese, G.; Bruno, A.; Palumbo, D.; Poli, U.; Gangemi, S.; Aragona, P.; Meduri, A. Sharing the Same Perspective. Mental Disorders and Central Serous Chorioretinopathy: A Systematic Review of Evidence from 2010 to 2020. Biomedicines 2021, 9, 1067. https://doi.org/10.3390/biomedicines9081067
Pandolfo G, Genovese G, Bruno A, Palumbo D, Poli U, Gangemi S, Aragona P, Meduri A. Sharing the Same Perspective. Mental Disorders and Central Serous Chorioretinopathy: A Systematic Review of Evidence from 2010 to 2020. Biomedicines. 2021; 9(8):1067. https://doi.org/10.3390/biomedicines9081067
Chicago/Turabian StylePandolfo, Gianluca, Giovanni Genovese, Antonio Bruno, Diletta Palumbo, Umberto Poli, Sebastiano Gangemi, Pasquale Aragona, and Alessandro Meduri. 2021. "Sharing the Same Perspective. Mental Disorders and Central Serous Chorioretinopathy: A Systematic Review of Evidence from 2010 to 2020" Biomedicines 9, no. 8: 1067. https://doi.org/10.3390/biomedicines9081067
APA StylePandolfo, G., Genovese, G., Bruno, A., Palumbo, D., Poli, U., Gangemi, S., Aragona, P., & Meduri, A. (2021). Sharing the Same Perspective. Mental Disorders and Central Serous Chorioretinopathy: A Systematic Review of Evidence from 2010 to 2020. Biomedicines, 9(8), 1067. https://doi.org/10.3390/biomedicines9081067