
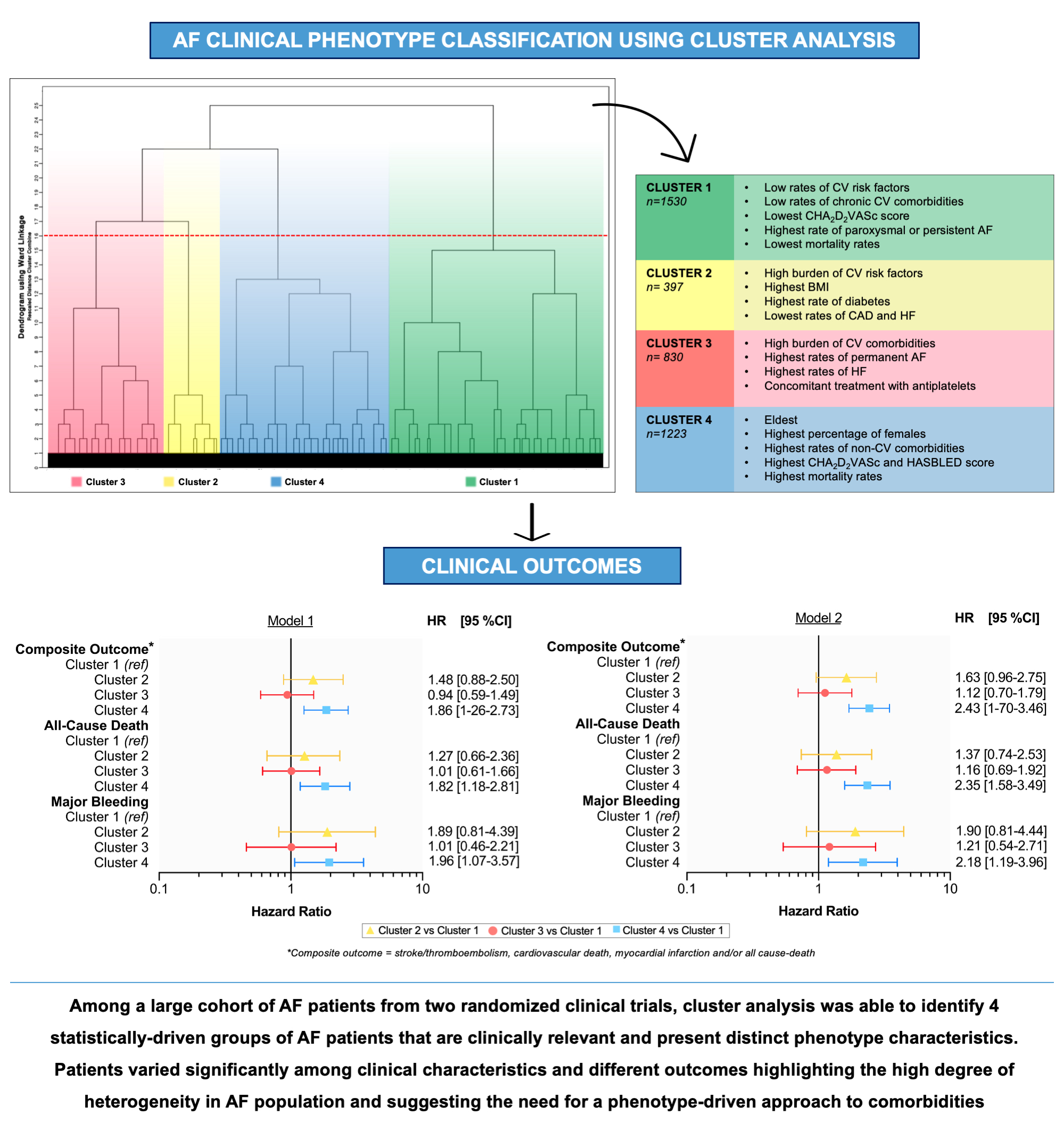
Clinical Phenotype Classification of Atrial Fibrillation Patients Using Cluster Analysis and Associations with Trial-Adjudicated Outcomes


 ,
,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Cohort
2.2. Study Outcomes
2.3. Statistical Analysis
3. Results
3.1. Clusters
3.1.1. Cluster 1 (n = 1530)
3.1.2. Cluster 2 (n = 397)
3.1.3. Cluster 3 (n = 830)
3.1.4. Cluster 4 (n = 1221)
3.2. Associations with Clinical Outcomes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Supplemental Methods
References
- Vitolo, M.; Proietti, M.; Harrison, S.; Lane, D.A.; Potpara, T.S.; Boriani, G.; Lip, G.Y.H. The Euro Heart Survey and EURObservational Research Programme (EORP) in atrial fibrillation registries: Contribution to epidemiology, clinical management and therapy of atrial fibrillation patients over the last 20 years. Intern. Emerg. Med. 2020, 15, 1183–1192. [Google Scholar] [CrossRef] [PubMed]
- Proietti, M.; Lip, G.Y.H.; Laroche, C.; Fauchier, L.; Marin, F.; Nabauer, M.; Potpara, T.; Dan, G.A.; Kalarus, Z.; Tavazzi, L.; et al. Relation of outcomes to ABC (Atrial Fibrillation Better Care) pathway adherent care in European patients with atrial fibrillation: An analysis from the ESC-EHRA EORP Atrial Fibrillation General Long-Term (AFGen LT) Registry. EP Europace 2021, 23, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Proietti, M.; Laroche, C.; Nieuwlaat, R.; Crijns, H.J.; Maggioni, A.P.; Lane, D.A.; Boriani, G.; Lip, G.Y. Increased burden of comorbidities and risk of cardiovascular death in atrial fibrillation patients in Europe over ten years: A comparison between EORP-AF pilot and EHS-AF registries. Eur. J. Intern. Med. 2018, 55, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Boriani, G.; Ruff, C.T.; Kuder, J.F.; Shi, M.; Lanz, H.J.; Antman, E.M.; Braunwald, E.; Giugliano, R.P. Edoxaban versus Warfarin in Patients with Atrial Fibrillation at the Extremes of Body Weight: An Analysis from the ENGAGE AF-TIMI 48 Trial. Thromb. Haemost. 2021, 121, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.R.; Choi, E.K.; Jung, J.H.; Park, S.H.; Han, K.D.; Oh, S.; Lip, G.Y. Body Mass Index and Clinical Outcomes in Asian Patients with Atrial Fibrillation Receiving Oral Anticoagulation. Stroke 2021, 52, 521–530. [Google Scholar] [CrossRef]
- Vitolo, M.; Lip, G.Y.H.; Shantsila, A. Why Is Atrial Fibrillation So Frequent in Hypertensive Patients? Am. J. Hypertens. 2020, 33, 1067–1070. [Google Scholar] [CrossRef]
- Boriani, G.; Vitolo, M.; Diemberger, I.; Proietti, M.; Valenti, A.C.; Malavasi, V.L.; Lip, G.Y. Optimizing indices of AF susceptibility and burden to evaluate AF severity, risk and outcomes. Cardiovasc. Res. 2021. [Google Scholar] [CrossRef]
- Viticchi, G.; Falsetti, L.; Burattini, M.; Zaccone, V.; Buratti, L.; Bartolini, M.; Moroncini, G.; Silvestrini, M. Atrial Fibrillation on Patients with Vascular Dementia: A Fundamental Target for Correct Management. Brain Sci. 2020, 10, 420. [Google Scholar] [CrossRef]
- Falsetti, L.; Viticchi, G.; Buratti, L.; Grigioni, F.; Capucci, A.; Silvestrini, M. Interactions between Atrial Fibrillation, Cardiovascular Risk Factors, and ApoE Genotype in Promoting Cognitive Decline in Patients with Alzheimer’s Disease: A Prospective Cohort Study. J. Alzheimers Dis. 2018, 62, 713–725. [Google Scholar] [CrossRef]
- Inohara, T.; Shrader, P.; Pieper, K.; Blanco, R.G.; Thomas, L.; Singer, D.E.; Freeman, J.V.; Allen, L.A.; Fonarow, G.C.; Gersh, B.; et al. Association of of Atrial Fibrillation Clinical Phenotypes with Treatment Patterns and Outcomes: A Multicenter Registry Study. JAMA Cardiol. 2018, 3, 54–63. [Google Scholar] [CrossRef]
- Inohara, T.; Piccini, J.P.; Mahaffey, K.W.; Kimura, T.; Katsumata, Y.; Tanimoto, K.; Inagawa, K.; Ikemura, N.; Ueda, I.; Fukuda, K.; et al. A Cluster Analysis of the Japanese Multicenter Outpatient Registry of Patients with Atrial Fibrillation. Am. J. Cardiol. 2019, 124, 871–878. [Google Scholar] [CrossRef]
- Ahmad, T.; Pencina, M.J.; Schulte, P.J.; O’Brien, E.; Whellan, D.J.; Piña, I.L.; Kitzman, D.W.; Lee, K.L.; O’Connor, C.M.; Felker, G.M. Clinical implications of chronic heart failure phenotypes defined by cluster analysis. J. Am. Coll. Cardiol. 2014, 64, 1765–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwak, S.; Lee, Y.; Ko, T.; Yang, S.; Hwang, I.-C.; Park, J.-B.; Yoon, Y.E.; Kim, H.-L.; Kim, H.-K.; Kim, Y.-J.; et al. Unsupervised Cluster Analysis of Patients with Aortic Stenosis Reveals Distinct Population with Different Phenotypes and Outcomes. Circ. Cardiovasc. Imaging 2020, 13, e009707. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, Y.; Tanimoto, S.; Latif, M.; Urayama, K.Y.; Aoki, J.; Yahagi, K.; Okuno, T.; Sato, Y.; Tanaka, T.; Koseki, K.; et al. Identifying novel phenotypes of acute heart failure using cluster analysis of clinical variables. Int. J. Cardiol. 2018, 262, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Parikh, K.S.; Rao, Y.; Ahmad, T.; Shen, K.; Felker, G.M.; Rajagopal, S. Novel approach to classifying patients with pulmonary arterial hypertension using cluster analysis. Pulm. Circ. 2017, 7, 486–493. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, T.; Desai, N.; Wilson, F.; Schulte, P.; Dunning, A.; Jacoby, D.; Allen, L.; Fiuzat, M.; Rogers, J.; Felker, G.M.; et al. Clinical Implications of Cluster Analysis-Based Classification of Acute Decompensated Heart Failure and Correlation with Bedside Hemodynamic Profiles. PLoS ONE 2016, 11, e0145881. [Google Scholar] [CrossRef]
- Shah, S.J.; Katz, D.; Selvaraj, S.; Burke, M.A.; Yancy, C.W.; Gheorghiade, M.; Bonow, R.O.; Huang, C.-C.; Deo, R.C. Phenomapping for Novel Classification of Heart Failure with Preserved Ejection Fraction. Circulation 2015, 131, 269–279. [Google Scholar] [CrossRef] [Green Version]
- Ernande, L.; Audureau, E.; Jellis, C.L.; Bergerot, C.; Henegar, C.; Sawaki, D.; Czibik, G.; Volpi, C.; Canoui-Poitrine, F.; Thibault, H.; et al. Clinical Implications of Echocardiographic Phenotypes of Patients with Diabetes Mellitus. J. Am. Coll. Cardiol. 2017, 70, 1704–1716. [Google Scholar] [CrossRef]
- Sevakula, R.K.; Au-Yeung, W.M.; Singh, J.P.; Heist, E.K.; Isselbacher, E.M.; Armoundas, A.A. State-of-the-Art Machine Learning Techniques Aiming to Improve Patient Outcomes Pertaining to the Cardiovascular System. J. Am. Heart Assoc. 2020, 9, e013924. [Google Scholar] [CrossRef]
- Bousser, M.G.; Bouthier, J.; Büller, H.R.; Cohen, A.T.; Crijns, H.; Davidson, B.L.; Halperin, J.; Hankey, G.; Levy, S.; Pengo, V.; et al. Comparison of idraparinux with vitamin K antagonists for prevention of thromboembolism in patients with atrial fibrillation: A randomised, open-label, non-inferiority trial. Lancet 2008, 371, 315–321. [Google Scholar]
- Buller, H.R.; Halperin, J.; Hankey, G.J.; Pillion, G.; Prins, M.H.; Raskob, G.E. Comparison of idrabiotaparinux with vitamin K antagonists for prevention of thromboembolism in patients with atrial fibrillation: The Borealis-Atrial Fibrillation Study. J. Thromb. Haemost. JTH 2014, 12, 824–830. [Google Scholar] [CrossRef] [Green Version]
- Malavasi, V.L.; Fantecchi, E.; Tordoni, V.; Melara, L.; Barbieri, A.; Vitolo, M.; Lip, G.Y.H.; Boriani, G. Atrial fibrillation pattern and factors affecting the progression to permanent atrial fibrillation. Intern. Emerg. Med. 2020, 1–10. [Google Scholar] [CrossRef]
- Vitolo, M.; Lip, G.Y.H. Understanding the global burden of atrial fibrillation and regional variations: We need improvement. Cardiovasc. Res. 2021, 117, 1420–1422. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Lip, G.Y.; Banerjee, A.; Boriani, G.; Chiang, C.E.; Fargo, R.; Freedman, B.; Lane, D.A.; Ruff, C.T.; Turakhia, M.; Werring, D.; et al. Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report. Chest 2018, 154, 1121–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boriani, G.; Vitolo, M.; Lane, D.A.; Potpara, T.S.; Lip, G.Y. Beyond the 2020 guidelines on atrial fibrillation of the European society of cardiology. Eur. J. Intern. Med. 2021, 86, 1–11. [Google Scholar] [CrossRef]
- Proietti, M.; Romiti, G.F.; Olshansky, B.; Lane, D.A.; Lip, G.Y.H. Comprehensive Management with the ABC (Atrial Fibrillation Better Care) Pathway in Clinically Complex Patients with Atrial Fibrillation: A Post Hoc Ancillary Analysis From the AFFIRM Trial. J. Am. Heart Assoc. 2020, 9, e014932. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Lane, D.A.; Wang, L.; Zhang, H.; Wang, H.; Zhang, W.; Wen, J.; Xing, Y.; Wu, F.; Xia, Y.; et al. Mobile Health Technology to Improve Care for Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2020, 75, 1523–1534. [Google Scholar] [CrossRef]
- Proietti, M.; Vitolo, M.; Lip, G.Y.H. Integrated care and outcomes in patients with atrial fibrillation and comorbidities. Eur. J. Clin. Investig. 2021, 51, e13498. [Google Scholar] [CrossRef]
- Malavasi, V.L.; Zoccali, C.; Brandi, M.C.; Micali, G.; Vitolo, M.; Imberti, J.F.; Mussi, C.; Schnabel, R.B.; Freedman, B.; Boriani, G. Cognitive impairment in patients with atrial fibrillation: Implications for outcome in a cohort study. Int. J. Cardiol. 2021, 323, 83–89. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Cluster 1 N = 1530 | Cluster 2 N = 397 | Cluster 3 N = 830 | Cluster 4 N = 1223 | p Value | |
|---|---|---|---|---|---|
| Age, years, median (IQR) | 71 (64–76) | 68 (61–73) | 65 (59–70) | 76 (70–79) | <0.001 |
| Age, years, mean (SD) | 69.4 (9.4) | 67.5 (8.0) | 64.4 (7.9) | 74.4 (8.0) | <0.001 |
| Females, n (%) | 516 (33.7) | 160 (40.3) | 279 (33.6) | 505 (41.3) | <0.001 |
| BMI, median (IQR) | 27 (24–30) | 31 (27–35) | 30 (27–35) | 28 (25–31) | <0.001 |
| BMI Classes, n (%) | <0.001 | ||||
| Normal Weight | 474 (31.0) | 42 (10.6) | 22 (2.7) | 292 (23.9) | |
| Overweight | 636 (41.6) | 123 (31.0) | 324 (39.0) | 527 (43.1) | |
| Obese | 420 (27.4) | 232 (58.4) | 484 (58.3) | 404 (33.0) | |
| Permanent AF, n (%) | 779 (50.9) | 242 (61.0) | 521 (62.8) | 664 (54.3) | <0.001 |
| CHA2DS2-VASc, median (IQR) | 3 (2–4) | 4 (3–5) | 4 (3–5) | 5 (4–6) | <0.001 |
| HAS-BLED, median (IQR) | 2 (1–2) | 2 (1–2) | 2 (1–2) | 2 (2–3) | <0.001 |
| Previous TE, n (%) | 466 (30.5) | 51 (12.8) | 116 (14.0) | 439 (35.9) | <0.001 |
| Hypertension, n (%) | 1041 (68.0) | 366 (92.2) | 806 (97.1) | 1144 (93.5) | <0.001 |
| Heart Failure, n (%) | 273 (17.8) | 59 (14.9) | 645 (77.7) | 572 (46.8) | <0.001 |
| Diabetes Mellitus, n (%) | 62 (4.1) | 387 (97.5) | 275 (33.1) | 307 (25.1) | <0.001 |
| CAD, n (%) | 362 (23.7) | 77 (19.4) | 401 (48.3) | 628 (51.3) | <0.001 |
| CKD, n (%) | 61 (4.0) | 37 (9.3) | 24 (2.9) | 435 (35.6) | <0.001 |
| Anaemia, n (%) | 43 (2.8) | 31 (7.8) | 0 (0) | 413 (33.8) | <0.001 |
| Any Antiplatelet Drugs, n (%) | 121 (7.9) | 5 (1.3) | 442 (53.3) | 404 (33.0) | <0.001 |
| TTR, median (IQR) | 60 (46—71) | 57 (43–73) | 58 (40–73) | 59 (43–73) | 0.10 |
| Cluster 1 N = 1530 | Cluster 2 N = 397 | Cluster 3 N = 830 | Cluster 4 N = 1223 | p Value | |
|---|---|---|---|---|---|
| Composite outcome, n (%) | 47 (3.1) | 20 (5.0) | 31 (3.7) | 102 (8.3) | <0.001 |
| All-cause death, n (%) | 38 (2.5) | 14 (3.5) | 27 (3.3) | 81 (6.6) | <0.001 |
| Stroke/TE, n (%) | 15 (1.0) | 8 (2.0) | 10 (1.2) | 30 (2.5) | 0.013 |
| Cardiovascular death, n (%) | 17 (1.1) | 5 (1.3) | 13 (1.6) | 41 (3.4) | <0.001 |
| Myocardial infarction, n (%) | 2 (0.1) | 2 (0.5) | 3 (0.4) | 10 (0.8) | 0.05 |
| Major bleeding, n (%) | 17 (1.1) | 8 (2.0) | 10 (1.2) | 34 (2.8) | 0.005 |
| Unadjusted Analysis | Multivariate Analysis [Model 1] | Multivariate Analysis [Model 2] | |||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | |
| Composite outcome * | |||||||||
| Cluster 1 (ref) | - | - | - | - | - | - | - | - | - |
| Cluster 2 | 1.62 | 0.96–2.73 | 0.07 | 1.48 | 0.88–2.50 | 0.14 | 1.63 | 0.96–2.75 | 0.07 |
| Cluster 3 | 1.07 | 0.68–1.69 | 0.77 | 0.94 | 0.59–1.49 | 0.81 | 1.12 | 0.70–1.79 | 0.63 |
| Cluster 4 | 2.59 | 1.83–3.66 | <0.001 | 1.86 | 1.26–2.73 | 0.002 | 2.43 | 1.70–3.46 | <0.001 |
| All cause-death * | |||||||||
| Cluster 1 (ref) | - | - | - | - | - | - | - | - | - |
| Cluster 2 | 1.38 | 0.75–2.55 | 0.30 | 1.27 | 0.66–2.36 | 0.44 | 1.37 | 0.74–2.53 | 0.31 |
| Cluster 3 | 1.12 | 0.68–1.85 | 0.64 | 1.01 | 0.61–1.66 | 0.98 | 1.16 | 0.69–1.92 | 0.58 |
| Cluster 4 | 2.47 | 1.68–3.63 | <0.001 | 1.82 | 1.18–2.81 | 0.006 | 2.35 | 1.58–3.49 | <0.001 |
| Major Bleeding § | |||||||||
| Cluster 1 (ref) | - | - | - | - | - | - | - | - | - |
| Cluster 2 | 1.76 | 0.76–4.09 | 0.18 | 1.89 | 0.81–4.39 | 0.13 | 1.90 | 0.81–4.44 | 0.13 |
| Cluster 3 | 1.01 | 0.46–2.20 | 0.98 | 1.01 | 0.46–2.21 | 0.97 | 1.21 | 0.54–2.71 | 0.63 |
| Cluster 4 | 2.42 | 1.35–4.34 | 0.003 | 1.96 | 1.07–3.57 | 0.02 | 2.18 | 1.19–3.96 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitolo, M.; Proietti, M.; Shantsila, A.; Boriani, G.; Lip, G.Y.H. Clinical Phenotype Classification of Atrial Fibrillation Patients Using Cluster Analysis and Associations with Trial-Adjudicated Outcomes. Biomedicines 2021, 9, 843. https://doi.org/10.3390/biomedicines9070843
Vitolo M, Proietti M, Shantsila A, Boriani G, Lip GYH. Clinical Phenotype Classification of Atrial Fibrillation Patients Using Cluster Analysis and Associations with Trial-Adjudicated Outcomes. Biomedicines. 2021; 9(7):843. https://doi.org/10.3390/biomedicines9070843
Chicago/Turabian StyleVitolo, Marco, Marco Proietti, Alena Shantsila, Giuseppe Boriani, and Gregory Y. H. Lip. 2021. "Clinical Phenotype Classification of Atrial Fibrillation Patients Using Cluster Analysis and Associations with Trial-Adjudicated Outcomes" Biomedicines 9, no. 7: 843. https://doi.org/10.3390/biomedicines9070843
APA StyleVitolo, M., Proietti, M., Shantsila, A., Boriani, G., & Lip, G. Y. H. (2021). Clinical Phenotype Classification of Atrial Fibrillation Patients Using Cluster Analysis and Associations with Trial-Adjudicated Outcomes. Biomedicines, 9(7), 843. https://doi.org/10.3390/biomedicines9070843