
Association between Blood Pressure, Blood Pressure Variability, and Post-Stroke Cognitive Impairment


Abstract
1. Introduction
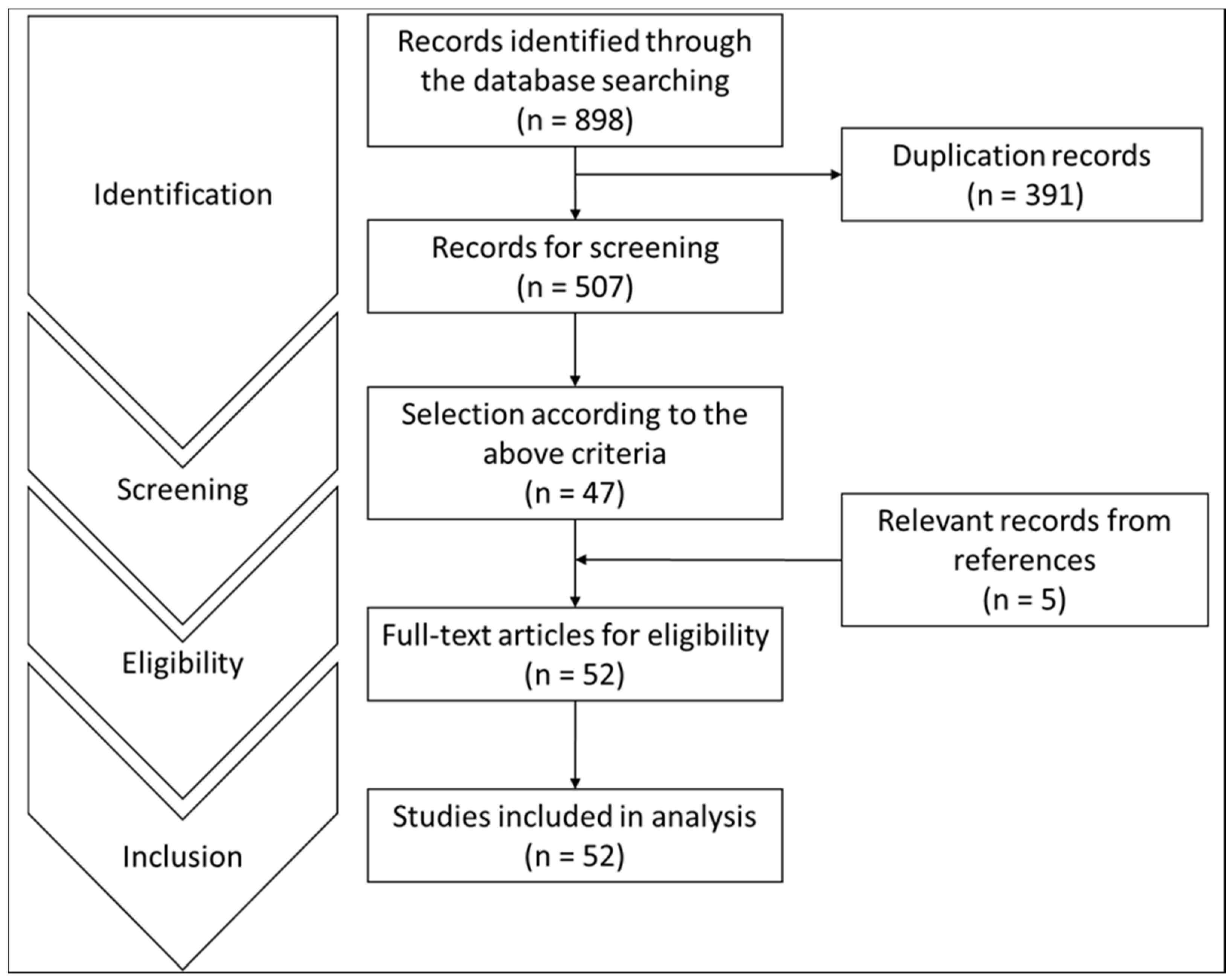
2. Method and Data Source
- (Post-stroke cognitive impairment) AND (Blood pressure)
- (Poststroke cognitive impairment) AND (Blood pressure)
- (Post-stroke cognitive impairment) AND (Blood pressure variability)
- (Poststroke cognitive impairment) AND (Blood pressure variability)
- (Post-stroke dementia) AND (Blood pressure)
- (Poststroke dementia) AND (Blood pressure)
- (Post-stroke dementia) AND (Blood pressure variability)
- (Poststroke dementia) AND (Blood pressure variability)
- (Cognitive impairment after stroke) AND (Blood pressure variability)
- (Dementia) AND (Blood pressure variability)
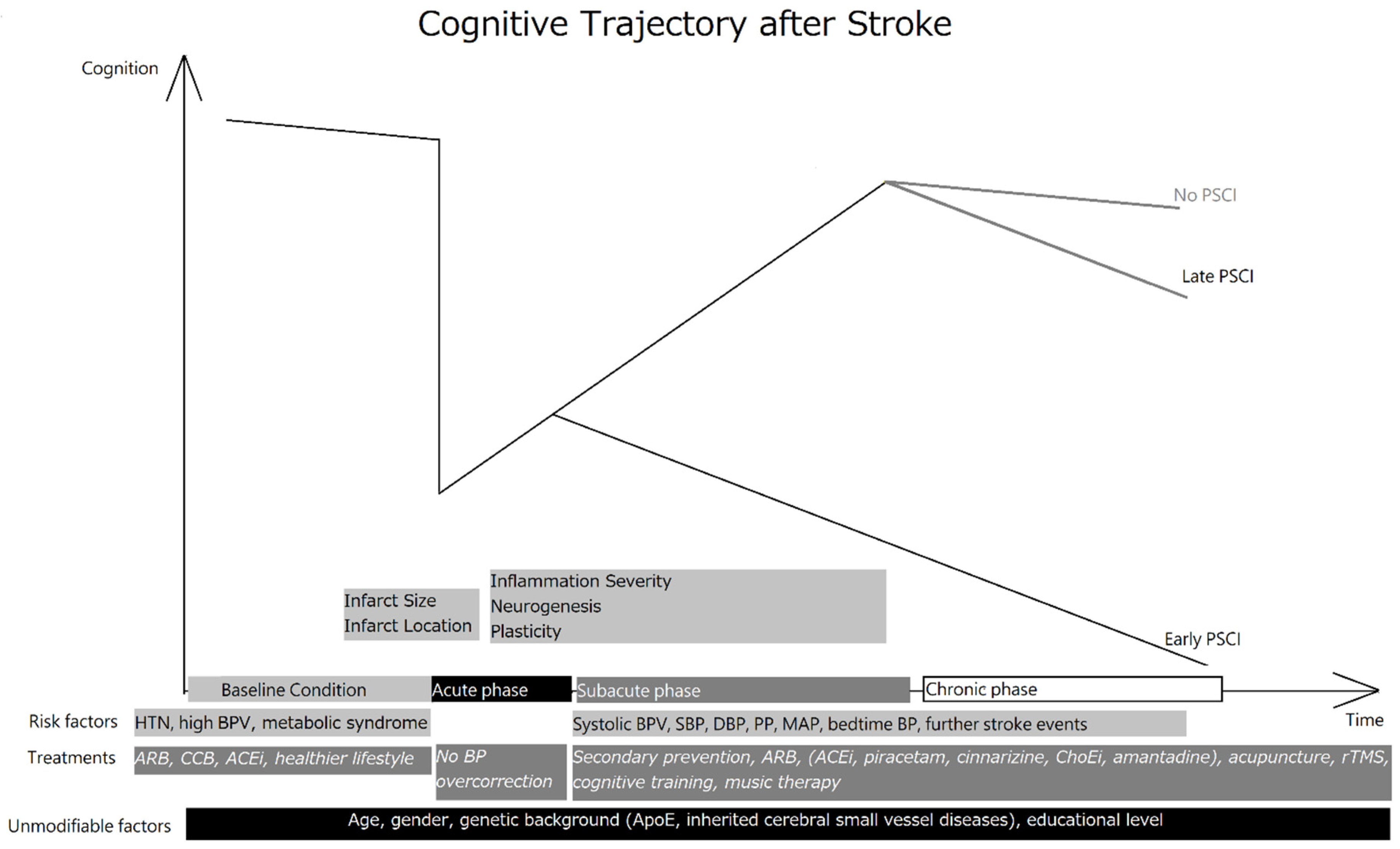
3. Anatomical, Biochemical and Pathological Changes after Stroke and Their Relationship with PSCI/PSD
4. Biomarkers for PSCI/PSD
4.1. Serological Biomarkers
4.2. Imaging Biomarkers
5. The Relationship between BP, BPV, and PSCI/PSD
5.1. The Association between BP and Cognition
5.2. The Association between BPV and Cognition
5.3. Influence of BP/BPV in PSCI and PSD
6. Management to Modify or Prevent PSCI
6.1. General Picture of BP Control in Stroke
6.2. Evidence Regarding Modifying the Potential Effect of BP/BPV on PSCI
6.3. Other Pharmacological and Nonpharmacological Approach to Modify or Prevent PSCI
7. Limitation
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Donnan, G.A.; Khatri, P. Stroke. Lancet 2008, 371, 1612–1623. [Google Scholar] [CrossRef]
- Hu, H.H.; Sheng, W.Y.; Chu, F.L.; Lan, C.F.; Chiang, B.N. Incidence of stroke in Taiwan. Stroke 1992, 23, 1237–1241. [Google Scholar] [CrossRef]
- Hu, H.H.; Chu, F.L.; Chiang, B.N.; Lan, C.F.; Sheng, W.Y.; Lo, Y.K.; Wong, W.J.; Luk, Y.O. Prevalence of stroke in Taiwan. Stroke 1989, 20, 858–863. [Google Scholar] [CrossRef]
- Luengo-Fernandez, R.; Violato, M.; Candio, P.; Leal, J. Economic burden of stroke across Europe: A population-based cost analysis. Eur. Stroke J. 2020, 5, 17–25. [Google Scholar] [CrossRef]
- Rajsic, S.; Gothe, H.; Borba, H.H.; Sroczynski, G.; Vujicic, J.; Toell, T.; Siebert, U. Economic burden of stroke: A systematic review on post-stroke care. Eur. J. Health Econ. 2019, 20, 107–134. [Google Scholar] [CrossRef] [PubMed]
- Madureira, S.; Guerreiro, M.; Ferro, J.M. Dementia and cognitive impairment three months after stroke. Eur. J. Neurol. 2001, 8, 621–627. [Google Scholar] [CrossRef]
- Pendlebury, S.T.; Rothwell, P.M. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: A systematic review and meta-analysis. Lancet Neurol. 2009, 8, 1006–1018. [Google Scholar] [CrossRef]
- Lin, J.-H.; Lin, R.-T.; Tai, C.-T.; Hsieh, C.-L.; Hsiao, S.-F.; Liu, C.-K. Prediction of poststroke dementia. Neurology 2003, 61, 343–348. [Google Scholar] [CrossRef]
- Jacova, C.; Pearce, L.; Costello, R.; McClure, L.A.; Holliday, S.L.; Hart, R.G.; Benavente, O.R.; Ms, L.A.P. Cognitive impairment in lacunar strokes: The SPS3 trial. Ann. Neurol. 2012, 72, 351–362. [Google Scholar] [CrossRef]
- Makin, S.D.J.; Turpin, S.; Dennis, M.S.; Wardlaw, J. Cognitive impairment after lacunar stroke: Systematic review and meta-analysis of incidence, prevalence and comparison with other stroke subtypes. J. Neurol. Neurosurg. Psychiatry 2013, 84, 893–900. [Google Scholar] [CrossRef]
- Qu, Y.; Zhuo, L.; Li, N.; Hu, Y.; Chen, W.; Zhou, Y.; Wang, J.; Tao, Q.; Hu, J.; Nie, X.; et al. Prevalence of Post-Stroke Cognitive Impairment in China: A Community-Based, Cross-Sectional Study. PLoS ONE 2015, 10, e0122864. [Google Scholar] [CrossRef]
- Gao, C.-Y.; Lian, Y.; Zhang, M.; Zhang, L.-L.; Fang, C.-Q.; Deng, J.; Li, J.; Xu, Z.-Q.; Zhou, H.-D.; Wang, Y.-J. Association of dementia with death after ischemic stroke: A two-year prospective study. Exp. Ther. Med. 2016, 12, 1765–1769. [Google Scholar] [CrossRef]
- Lugtmeijer, S.; Lammers, N.A.; de Haan, E.H.F.; de Leeuw, F.-E.; Kessels, R.P.C. Post-Stroke Working Memory Dysfunction: A Meta-Analysis and Systematic Review. Neuropsychol. Rev. 2021, 31, 202–219. [Google Scholar] [CrossRef]
- Guo, J.; Wang, J.; Sun, W.; Liu, X. The advances of post-stroke depression: 2021 update. J. Neurol. 2021. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhao, S.; Fan, Z.; Li, Z.; He, F.; Lin, C.; Topatana, W.; Yan, Y.; Liu, Z.; Chen, Y.; et al. Evaluation of the Mini-Mental State Examination and the Montreal Cognitive Assessment for Predicting Post-stroke Cognitive Impairment During the Acute Phase in Chinese Minor Stroke Patients. Front. Aging Neurosci. 2020, 12, 236. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.; Park, J.; Seo, W. A 2-year prospective follow-up study of temporal changes associated with post-stroke cognitive impairment. Int. J. Nurs. Pract. 2018, 24, e12618. [Google Scholar] [CrossRef] [PubMed]
- Mok, V.C.T.; Lam, B.Y.K.; Wong, A.; Ko, H.; Markus, H.S.; Wong, L.K.S. Early-onset and delayed-onset poststroke dementia—revisiting the mechanisms. Nat. Rev. Neurol. 2017, 13, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Mijajlović, M.D.; Pavlović, A.; Brainin, M.; Heiss, W.-D.; Quinn, T.J.; Ihle-Hansen, H.B.; Hermann, D.M.; Ben Assayag, E.; Richard, E.; Thiel, A.; et al. Post-stroke dementia–A comprehensive review. BMC Med. 2017, 15, 11. [Google Scholar] [CrossRef] [PubMed]
- Morsund, Å.H.; Ellekjaer, H.; Gramstad, A.; Reiestad, M.T.; Midgard, R.; Sando, S.B.; Jonsbu, E.; Naess, H.; Ellekjær, H.; Næss, H. The development of cognitive and emotional impairment after a minor stroke: A longitudinal study. Acta Neurol. Scand. 2019, 140, 281–289. [Google Scholar] [CrossRef]
- Alexandrova, M.L.; Danovska, M.P. Cognitive impairment one year after ischemic stroke: Predictorsand dynamics of significant determinants. Turk. J. Med. Sci. 2016, 46, 1366–1373. [Google Scholar] [CrossRef]
- Wolf, T.J.; Barbee, A.R.; White, D. Executive Dysfunction Immediately after Mild Stroke. OTJR: Occup. Particip. Health 2011, 31, S23–S29. [Google Scholar] [CrossRef]
- Aam, S.; Einstad, M.S.; Munthe-Kaas, R.; Lydersen, S.; Ihle-Hansen, H.; Knapskog, A.-B.; Ellekjær, H.; Seljeseth, Y.; Saltvedt, I. Post-stroke Cognitive Impairment—Impact of Follow-Up Time and Stroke Subtype on Severity and Cognitive Profile: The Nor-COAST Study. Front. Neurol. 2020, 11, 699. [Google Scholar] [CrossRef] [PubMed]
- Elgh, E.; Hu, X. Dynamic Trajectory of Long-Term Cognitive Improvement Up to 10 Years in Young Community-Dwelling Stroke Survivors: A Cohort Study. Front. Neurol. 2019, 10, 97. [Google Scholar] [CrossRef]
- Sachdev, P.S.; Chen, X.; Brodaty, H.; Thompson, C.; Altendorf, A.; Wen, W. The determinants and longitudinal course of post-stroke mild cognitive impairment. J. Int. Neuropsychol. Soc. 2009, 15, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Mărgăritescu, O.; Mogoanta, L.; Pirici, I.; Pirici, D.; Cernea, D.; Mărgăritescu, C. Histopathological changes in acute ischemic stroke. Rom. J. Morphol. Embryol. 2009, 50, 327–339. [Google Scholar]
- Kalaria, R.N.; Akinyemi, R.; Ihara, M. Stroke injury, cognitive impairment and vascular dementia. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2016, 1862, 915–925. [Google Scholar] [CrossRef]
- Lambertsen, K.L.; Biber, K.; Finsen, B. Inflammatory Cytokines in Experimental and Human Stroke. Br. J. Pharmacol. 2012, 32, 1677–1698. [Google Scholar] [CrossRef]
- Swardfager, W.; Winer, D.A.; Herrmann, N.; Winer, S.; Lanctôt, K.L. Interleukin-17 in post-stroke neurodegeneration. Neurosci. Biobehav. Rev. 2013, 37, 436–447. [Google Scholar] [CrossRef] [PubMed]
- Rothenburg, L.S.; Herrmann, N.; Swardfager, W.; Black, S.; Tennen, G.; Kiss, A.; Gladstone, D.; Ween, J.; Snaiderman, A.; Lanctot, K.L. The Relationship Between Inflammatory Markers and Post Stroke Cognitive Impairment. J. Geriatr. Psychiatry Neurol. 2010, 23, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Gulyaeva, N.V. Biochemical Mechanisms and Translational Relevance of Hippocampal Vulnerability to Distant Focal Brain Injury: The Price of Stress Response. Biochemostry 2019, 84, 1306–1328. [Google Scholar] [CrossRef] [PubMed]
- Delattre, C.; Bournonville, C.; Auger, F.; Lopes, R.; Delmaire, C.; Henon, H.; Mendyk, A.M.; Bombois, S.; Devedjian, J.C.; Leys, D.; et al. Hippocampal Deformations and Entorhinal Cortex Atrophy as an Anatomical Signature of Long-Term Cognitive Impairment: From the MCAO Rat Model to the Stroke Patient. Transl. Stroke Res. 2018, 9, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Grysiewicz, R.; Gorelick, P.B. Key Neuroanatomical Structures for Post-Stroke Cognitive Impairment. Curr. Neurol. Neurosci. Rep. 2012, 12, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Thiel, A.; Cechetto, D.F.; Heiss, W.-D.; Hachinski, V.; Whitehead, S.N. Amyloid Burden, Neuroinflammation, and Links to Cognitive Decline After Ischemic Stroke. Stroke 2014, 45, 2825–2829. [Google Scholar] [CrossRef]
- Cuartero, M.I.; García-Culebras, A.; Torres-López, C.; Medina, V.; Fraga, E.; Vázquez-Reyes, S.; Jareño-Flores, T.; García-Segura, J.M.; Lizasoain, I.; Moro, M.Á. Post-stroke Neurogenesis: Friend or Foe? Frontiers in cell and developmental biology. Front. Cell Dev. Biol. 2021, 9, 657846–657846. [Google Scholar] [CrossRef] [PubMed]
- Kempermann, G.; Song, H.; Gage, F.H. Neurogenesis in the Adult Hippocampus. Cold Spring Harb. Perspect. Biol. 2015, 7, a018812. [Google Scholar] [CrossRef]
- Lindvall, O.; Kokaia, Z. Neurogenesis following Stroke Affecting the Adult Brain. Cold Spring Harb. Perspect. Biol. 2015, 7, a019034. [Google Scholar] [CrossRef]
- Nakayama, H.; Jørgensen, H.S.; Raaschou, H.O.; Olsen, T.S. Recovery of upper extremity function in stroke patients: The Copenhagen stroke study. Arch. Phys. Med. Rehabil. 1994, 75, 394–398. [Google Scholar] [CrossRef]
- Cuartero, M.; De La Parra, J.; Pérez-Ruiz, A.; Bravo-Ferrer, I.; Durán-Laforet, V.; Garcia-Culebras, A.; García-Segura, J.M.; Dhaliwal, J.; Frankland, P.W.; Lizasoain, I.; et al. Abolition of aberrant neurogenesis ameliorates cognitive impairment after stroke in mice. J. Clin. Investig. 2019, 129, 1536–1550. [Google Scholar] [CrossRef]
- Khlif, M.S.; Werden, E.; Egorova, N.; Boccardi, M.; Redolfi, A.; Bird, L.; Brodtmann, A. Assessment of longitudinal hippocampal atrophy in the first year after ischemic stroke using automatic segmentation techniques. NeuroImage Clin. 2019, 24, 102008. [Google Scholar] [CrossRef]
- Brodtmann, A.; Khlif, M.S.; Egorova, N.; Veldsman, M.; Bird, L.J.; Werden, E. Dynamic Regional Brain Atrophy Rates in the First Year After Ischemic Stroke. Stroke 2020, 51, e183–e192. [Google Scholar] [CrossRef]
- Schaapsmeerders, P.; Tuladhar, A.M.; Maaijwee, N.A.M.; Rutten-Jacobs, L.C.A.; Arntz, R.M.; Schoonderwaldt, H.C.; Dorresteijn, L.D.A.; Van Dijk, E.J.; Kessels, R.P.C.; De Leeuw, F.-E. Lower Ipsilateral Hippocampal Integrity after Ischemic Stroke in Young Adults: A Long-Term Follow-Up Study. PLoS ONE 2015, 10, e0139772. [Google Scholar] [CrossRef] [PubMed]
- Ter Telgte, A.; Van Leijsen, E.M.C.; Wiegertjes, K.; Klijn, C.; Tuladhar, A.M.; De Leeuw, F.-E. Cerebral small vessel disease: From a focal to a global perspective. Nat. Rev. Neurol. 2018, 14, 387–398. [Google Scholar] [CrossRef]
- Kim, Y.J.; Kwon, H.K.; Lee, J.M.; Cho, H.; Kim, H.J.; Park, H.K.; Jung, N.; Lee, J.S.; Lee, J.; Jang, Y.K. Gray and white matter changes linking cerebral small vessel disease to gait disturbances. Neurology 2016, 86, 1199–1207. [Google Scholar] [CrossRef]
- Staals, J.; Makin, S.; Doubal, F.N.; Dennis, M.S.; Wardlaw, J.M. Stroke subtype, vascular risk factors, and total MRI brain small-vessel disease burden. Neurology 2014, 83, 1228–1234. [Google Scholar] [CrossRef] [PubMed]
- Duering, M.; Righart, R.; Csanadi, E.; Jouvent, E.; Hervé, D.; Chabriat, H.; Dichgans, M. Incident subcortical infarcts induce focal thinning in connected cortical regions. Neurology 2012, 79, 2025–2028. [Google Scholar] [CrossRef]
- Peng, C.-Y.; Chen, Y.-C.; Cui, Y.; Zhao, D.-L.; Jiao, Y.; Tang, T.-Y.; Ju, S.; Teng, G.-J. Regional Coherence Alterations Revealed by Resting-State fMRI in Post-Stroke Patients with Cognitive Dysfunction. PLoS ONE 2016, 11, e0159574. [Google Scholar] [CrossRef]
- Tuladhar, A.M.; Snaphaan, L.; Shumskaya, E.; Rijpkema, M.; Fernandez, G.; Norris, D.G.; De Leeuw, F.-E. Default Mode Network Connectivity in Stroke Patients. PLoS ONE 2013, 8, e66556. [Google Scholar] [CrossRef]
- Liu, J.; Wang, Q.; Liu, F.; Song, H.; Liang, X.; Lin, Z.; Hong, W.; Yang, S.; Huang, J.; Zheng, G.; et al. Altered functional connectivity in patients with post-stroke memory impairment: A resting fMRI study. Exp. Ther. Med. 2017, 14, 1919–1928. [Google Scholar] [CrossRef]
- Aguayo, R.D.; Grana, M.; Fernández-Andújar, M.; López-Cancio, E.; Cáceres, C.; Bargalló, N.; Barrios, M.; Clemente, I.; Monserrat, P.T.; Sas, M.A.; et al. Structural Integrity of the Contralesional Hemisphere Predicts Cognitive Impairment in Ischemic Stroke at Three Months. PLoS ONE 2014, 9, e86119. [Google Scholar]
- Vinciguerra, L.; Lanza, G.; Puglisi, V.; Fisicaro, F.; Pennisi, M.; Bella, R.; Cantone, M. Update on the Neurobiology of Vascular Cognitive Impairment: From Lab to Clinic. Int. J. Mol. Sci. 2020, 8, 2977. [Google Scholar] [CrossRef]
- Li, J.; Zhao, Y.; Mao, J. Association between the extent of white matter damage and early cognitive impairment following acute ischemic stroke. Exp. Ther. Med. 2017, 13, 909–912. [Google Scholar] [CrossRef]
- Mok, V.C.; Liu, W.Y.; Wong, A. Detection of amyloid plaques in patients with post-stroke dementia. Hong Kong Med. J. 2016, 22, S40–S42. [Google Scholar] [PubMed]
- Akinyemi, R.O.; Allan, L.M.; Oakley, A.; Kalaria, R.N. Hippocampal Neurodegenerative Pathology in Post-stroke Dementia Compared to Other Dementias and Aging Controls. Front. Neurosci. 2017, 11, 717. [Google Scholar] [CrossRef]
- Jokinen, H.; Kalska, H.; Mäntylä, R.; Ylikoski, R.; Hietanen, M.; Pohjasvaara, T.; Kaste, M.; Erkinjuntti, T. White matter hyperintensities as a predictor of neuropsychological deficits post-stroke. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1229–1233. [Google Scholar] [CrossRef]
- Wollenweber, F.A.; Därr, S.; Müller, C.; Duering, M.; Buerger, K.; Zietemann, V.; Malik, R.; Brendel, M.; Ertl-Wagner, B.; Bartenstein, P.; et al. Prevalence of Amyloid Positron Emission Tomographic Positivity in Poststroke Mild Cognitive Impairment. Stroke 2016, 47, 2645–2648. [Google Scholar] [CrossRef]
- Del Brutto, O.H.; Mera, R.M.; Zambrano, M.; Lama, J. Cognitive performance in community-dwelling older adults with stroke and the contribution of age and diffuse subcortical damage: A population-based study in rural Ecuador (The Atahualpa Project). Aging Clin. Exp. Res. 2015, 27, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Casolla, B.; Caparros, F.; Cordonnier, C.; Bombois, S.; Hénon, H.; Bordet, R.; Orzi, F.; Leys, D. Biological and imaging predictors of cognitive impairment after stroke: A systematic review. J. Neurol. 2019, 266, 2593–2604. [Google Scholar] [CrossRef]
- Kliper, E.; Ben Assayag, E.; Tarrasch, R.; Artzi, M.; Korczyn, A.D.; Shenhar-Tsarfaty, S.; Aizenstein, O.; Hallevi, H.; Mike, A.; Shopin, L.; et al. Cognitive State following Stroke: The Predominant Role of Preexisting White Matter Lesions. PLoS ONE 2014, 9, e105461. [Google Scholar] [CrossRef]
- Kim, B.J.; Oh, M.-Y.; Jang, M.S.; Han, M.-K.; Lee, J.; Lee, J.; Kang, Y.; Yu, K.-H.; Lee, B.-C.; Kim, S.; et al. Medial Temporal Atrophy and Memory Dysfunction in Poststroke Cognitive Impairment-No Dementia. J. Clin. Neurol. 2012, 8, 43–50. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Molad, J.; Hallevi, H.; Korczyn, A.D.; Kliper, E.; Auriel, E.; Bornstein, N.M.; Ben Assayag, E. Vascular and Neurodegenerative Markers for the Prediction of Post-Stroke Cognitive Impairment: Results from the TABASCO Study. J. Alzheimer’s Dis. 2019, 70, 889–898. [Google Scholar] [CrossRef]
- Firbank, M.J.; Burton, E.J.; Barber, R.; Stephens, S.; Kenny, R.A.; Ballard, C.; Kalaria, R.N.; O’Brien, J. Medial temporal atrophy rather than white matter hyperintensities predict cognitive decline in stroke survivors. Neurobiol. Aging 2007, 28, 1664–1669. [Google Scholar] [CrossRef]
- Yang, J.; Wong, A.; Wang, Z.; Liu, W.; Au, L.; Xiong, Y.; Chu, W.W.; Leung, E.Y.; Chen, S.; Lau, C.; et al. Risk factors for incident dementia after stroke and transient ischemic attack. Alzheimer’s Dement. 2015, 11, 16–23. [Google Scholar] [CrossRef]
- Christ, N.; Mocke, V.; Fluri, F. Cerebral microbleeds are associated with cognitive decline early after ischemic stroke. J. Neurol. 2019, 266, 1091–1094. [Google Scholar] [CrossRef] [PubMed]
- Mok, V.C.T.; Lam, B.Y.K.; Wang, Z.; Liu, W.; Au, L.; Leung, E.Y.L.; Chen, S.; Yang, J.; Chu, W.C.W.; Lau, A.Y.L.; et al. Delayed-onset dementia after stroke or transient ischemic attack. Alzheimers Dement 2016, 12, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Mok, V.; Xiong, Y.; Wong, K.K.; Wong, A.; Schmidt, R.; Chu, W.W.; Hu, X.; Leung, E.Y.L.; Chen, S.; Chen, Y.; et al. Predictors for cognitive decline in patients with confluent white matter hyperintensities. Alzheimer’s Dement. 2012, 8, S96–S103. [Google Scholar] [CrossRef] [PubMed]
- Dufouil, C.; Godin, O.; Chalmers, J.; Coskun, O.; MacMahon, S.; Tzourio-Mazoyer, N.; Bousser, M.-G.; Anderson, C.; Mazoyer, B.; Tzourio, C. Severe Cerebral White Matter Hyperintensities Predict Severe Cognitive Decline in Patients with Cerebrovascular Disease History. Stroke 2009, 40, 2219–2221. [Google Scholar] [CrossRef]
- Liu, W.; Wong, A.; Au, L.; Yang, J.; Wang, Z.; Leung, E.Y.L.; Chen, S.; Ho, C.L.; Mok, V.C.T. Influence of Amyloid-β on Cognitive Decline After Stroke/Transient Ischemic Attack: Three-Year Longitudinal Study. Stroke 2015, 46, 3074–3080. [Google Scholar] [CrossRef]
- Gao, Q.; Fan, Y.; Mu, L.-Y.; Ma, L.; Song, Z.-Q.; Zhang, Y.-N. S100B and ADMA in cerebral small vessel disease and cognitive dysfunction. J. Neurol. Sci. 2015, 354, 27–32. [Google Scholar] [CrossRef]
- Castellazzi, M.; Trentini, A.; Romani, A.; Valacchi, G.; Bellini, T.; Bonaccorsi, G.; Fainardi, E.; Cavicchio, C.; Passaro, A.; Zuliani, G.; et al. Decreased arylesterase activity of paraoxonase-1 (PON-1) might be a common denominator of neuroinflammatory and neurodegenerative diseases. Int. J. Biochem. Cell Biol. 2016, 81, 356–363. [Google Scholar] [CrossRef]
- Fleszar, M.G.; Wiśniewski, J.; Zboch, M.; Diakowska, D.; Gamian, A.; Krzystek-Korpacka, M. Targeted metabolomic analysis of nitric oxide/L-arginine pathway metabolites in dementia: Association with pathology, severity, and structural brain changes. Sci. Rep. 2019, 9, 13764. [Google Scholar] [CrossRef]
- Wu, J.-X.; Xue, J.; Zhuang, L.; Liu, C.-F. Plasma parameters and risk factors of patients with post-stroke cognitive impairment. Ann. Palliat. Med. 2020, 9, 45–52. [Google Scholar] [CrossRef]
- Prodjohardjono, A.; Vidyanti, A.N.; Susianti, N.A.; Sudarmanta; Sutarni, S.; Setyopranoto, I. Higher level of acute serum VEGF and larger infarct volume are more frequently associated with post-stroke cognitive impairment. PLoS ONE 2020, 15, e0239370. [Google Scholar] [CrossRef]
- Liu, M.; Zhou, K.; Li, H.; Dong, X.; Tan, G.; Chai, Y.; Wang, W.; Bi, X. Potential of serum metabolites for diagnosing post-stroke cognitive impairment. Mol. BioSyst. 2015, 11, 3287–3296. [Google Scholar] [CrossRef]
- Chi, N.-F.; Chao, S.-P.; Huang, L.-K.; Chan, L.; Chen, Y.-R.; Chiou, H.-Y.; Hu, C.-J. Plasma Amyloid Beta and Tau Levels Are Predictors of Post-stroke Cognitive Impairment: A Longitudinal Study. Front. Neurol. 2019, 10, 715. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, H.; Zhao, K.; He, W.; Lin, S.; He, J. High levels of plasma fibrinogen are related to post-stroke cognitive impairment. Brain Behav. 2019, 9, e01391. [Google Scholar] [CrossRef]
- Guo, J.; Su, W.; Fang, J.; Chen, N.; Zhou, M.; Zhang, Y.; He, L. Elevated CRP at admission predicts post-stroke cognitive impairment in Han Chinese patients with intracranial arterial stenosis. Neurol. Res. 2018, 40, 292–296. [Google Scholar] [CrossRef]
- Ben Assayag, E.; Tene, O.; Korczyn, A.; Shopin, L.; Auriel, E.; Molad, J.; Hallevi, H.; Kirschbaum, C.; Bornstein, N.; Shenhar-Tsarfaty, S.; et al. High hair cortisol concentrations predict worse cognitive outcome after stroke: Results from the TABASCO prospective cohort study. Psychoneuroendocrinology 2017, 82, 133–139. [Google Scholar] [CrossRef]
- Ran, F.; Liu, F.; Zhang, Y.; Chen, L. Serum Uric Acid and High-Sensitivity C-Reactive Protein as Predictors of Cognitive Impairment in Patients with Cerebral Infarction. Dement. Geriatr. Cogn. Disord. 2020, 49, 235–242. [Google Scholar] [CrossRef]
- Pascoe, M.C.; Linden, T. Folate and MMA predict cognitive impairment in elderly stroke survivors: A cross sectional study. Psychiatry Res. 2016, 243, 49–52. [Google Scholar] [CrossRef]
- Yang, Z.; Wang, H.; Edwards, D.; Ding, C.; Yan, L.; Brayne, C.; Mant, J. Association of blood lipids, atherosclerosis and statin use with dementia and cognitive impairment after stroke: A systematic review and meta-analysis. Ageing Res. Rev. 2020, 57, 100962. [Google Scholar] [CrossRef]
- Zhu, Z.; Zhong, C.; Guo, D.; Bu, X.; Xu, T.; Guo, L.; Liu, J.; Zhang, J.; Li, D.; Zhang, J.; et al. Multiple biomarkers covering several pathways improve predictive ability for cognitive impairment among ischemic stroke patients with elevated blood pressure. Atherosclerosis 2019, 287, 30–37. [Google Scholar] [CrossRef]
- Li, P.; Quan, W.; Lu, D.; Wang, Y.; Zhang, H.-H.; Liu, S.; Jiang, R.-C.; Zhou, Y.-Y. Association between Metabolic Syndrome and Cognitive Impairment after Acute Ischemic Stroke: A Cross-Sectional Study in a Chinese Population. PLoS ONE 2016, 11, e0167327. [Google Scholar] [CrossRef] [PubMed]
- Tong, Z.; Wang, W.; Luo, W.; Lv, J.; Li, H.; Luo, H.; Jia, J.; He, R. Urine Formaldehyde Predicts Cognitive Impairment in Post-Stroke Dementia and Alzheimer’s Disease. J. Alzheimer’s Dis. 2016, 55, 1031–1038. [Google Scholar] [CrossRef]
- Zhang, X.; Bi, X. Post-Stroke Cognitive Impairment: A Review Focusing on Molecular Biomarkers. J. Mol. Neurosci. 2020, 70, 1244–1254. [Google Scholar] [CrossRef]
- Wagle, J.; Farner, L.; Flekkøy, K.; Wyller, T.B.; Sandvik, L.; Eiklid, K.L.; Fure, B.; Stensrød, B.; Engedal, K. Cognitive impairment and the role of the ApoE epsilon4-allele after stroke—A 13 months follow-up study. Int. J. Geriatr. Psychiatry 2010, 25, 833–842. [Google Scholar] [CrossRef]
- Wagle, J.; Farner, L.; Flekkøy, K.; Wyller, T.B.; Sandvik, L.; Eiklid, K.L.; Fure, B.; Stensrød, B.; Engedal, K. Association between ApoE epsilon4 and cognitive impairment after stroke. Dement Geriatr. Cogn. Disord. 2009, 27, 525–533. [Google Scholar] [CrossRef]
- Rezaei, S.; Mobarake, K.A.; Saberi, A. BDNF (rs6265) Val <Met polymorphism can buffer cognitive functions against post stroke CT/MRI pathological findings. Appl. Neuropsychol. Adult 2020, 2, 1–12. [Google Scholar]
- Pendlebury, S.T.; Poole, D.; Burgess, A.; Duerden, J. APOE-ε4 Genotype and Dementia Before and After Transient Ischemic Attack and Stroke: Population-Based Cohort Study. Stroke 2020, 51, 751–758. [Google Scholar] [CrossRef]
- Donnellan, C.; Redha, N.; Al Banna, M.; Al Sharoqi, I.; Al-Jishi, A.; Bakhiet, M.; Taha, S.; Abdulla, F.; Walsh, P. Associations between ApoE gene and psychological consequences post stroke in a Bahraini cohort. Asian J. Psychiatry 2019, 39, 135–142. [Google Scholar] [CrossRef]
- Pohjasvaara, T.; Mäntylä, R.; Salonen, O.; Aronen, H.J.; Ylikoski, R.; Hietanen, M.; Kaste, M.; Erkinjuntti, T. How Complex Interactions of Ischemic Brain Infarcts, White Matter Lesions, and Atrophy Relate to Poststroke Dementia. Arch. Neurol. 2000, 57, 1295–1300. [Google Scholar] [CrossRef]
- Béjot, Y.; Aboa-Eboule, C.; Durier, J.; Rouaud, O.; Agnes; Ponavoy, J.E.; Richard, D.; Moreau, T.; Giroud, M. Prevalence of early dementia after first-ever stroke: A 24-year population-based study. Stroke 2011, 42, 607–612. [Google Scholar] [CrossRef]
- Ding, X.; Li, C.-Y.; Wang, Q.-S.; Du, F.-Z.; Ke, Z.-W.; Peng, F.; Wang, J.; Chen, L. Patterns in default-mode network connectivity for determining outcomes in cognitive function in acute stroke patients. Neuroscience 2014, 277, 637–646. [Google Scholar] [CrossRef]
- Hagberg, G.; Ihle-Hansen, H.; Fure, B.; Thommessen, B.; Ihle-Hansen, H.; Øksengård, A.R.; Beyer, M.K.; Wyller, T.B.; Müller, E.G.; Pendlebury, S.T.; et al. No evidence for amyloid pathology as a key mediator of neurodegeneration post-stroke—A seven-year follow-up study. BMC Neurol. 2020, 20, 174. [Google Scholar] [CrossRef]
- Wollenweber, F.A.; Zietemann, V.; Rominger, A.; Opherk, C.; Bayer-Karpinska, A.; Gschwendtner, A.; Andrews, L.C.; Bürger, K.; Duering, M.; Dichgans, M. The Determinants of Dementia after Stroke (DEDEMAS) Study: Protocol and Pilot Data. Int. J. Stroke 2013, 9, 387–392. [Google Scholar] [CrossRef]
- Huang, K.-L.; Hsiao, I.-T.; Ho, M.-Y.; Hsu, J.-L.; Chang, Y.-J.; Chang, T.-Y.; Liu, C.-H.; Chang, C.-H.; Wu, Y.-M.; Wu, K.-Y.; et al. Investigation of reactive astrogliosis effect on post-stroke cognitive impairment. J. Neuroinflammation 2020, 17, 308. [Google Scholar] [CrossRef]
- Rothwell, P.M.; Howard, S.C.; Dolan, E.; O’Brien, E.; Dobson, J.; Dahlöf, B.; Sever, P.S.; Poulter, N.R. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet 2010, 375, 895–905. [Google Scholar] [CrossRef]
- Yu, J.-M.; Kong, Q.-Y.; Schoenhagen, P.; Shen, T.; He, Y.-S.; Wang, J.-W.; Zhao, Y.-P.; Shi, D.-N.; Zhong, B.-L. The prognostic value of long-term visit-to-visit blood pressure variability on stroke in real-world practice: A dynamic cohort study in a large representative sample of Chinese hypertensive population. Int. J. Cardiol. 2014, 177, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Lau, K.-K.; Wong, Y.-K.; Teo, K.-C.; Chang, R.S.; Chan, K.-H.; Hon, S.F.; Wat, K.-L.; Cheung, R.T.; Li, L.S.; Siu, C.-W.; et al. Long-Term Prognostic Implications of Visit-to-Visit Blood Pressure Variability in Patients with Ischemic Stroke. Am. J. Hypertens. 2014, 27, 1486–1494. [Google Scholar] [CrossRef] [PubMed]
- Lau, K.K.; Wong, Y.K.; Chang, R.S.K.; Teo, K.C.; Hon, S.F.K.; Chan, K.H.; Wat, K.L.; Cheung, R.T.F.; Li, L.S.W.; Siu, C.W.; et al. Visit-to-visit systolic blood pressure variability predicts all-cause and cardiovascular mortality after lacunar infarct. Eur. J. Neurol. 2013, 21, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Launer, L.J.; Ross, G.W.; Petrovitch, H.; Masaki, K.; Foley, D.; White, L.R.; Havlik, R.J. Midlife blood pressure and dementia: The Honolulu-Asia aging study. Neurobiol. Aging 2000, 21, 49–55. [Google Scholar] [CrossRef]
- Kivipelto, M.; Helkala, E.-L.; Laakso, M.; Hänninen, T.; Hallikainen, M.; Alhainen, K.; Soininen, H.; Tuomilehto, J.; Nissinen, A. Midlife vascular risk factors and Alzheimer’s disease in later life: Longitudinal, population based study. BMJ 2001, 322, 1447–1451. [Google Scholar] [CrossRef]
- Yamada, M.; Kasagi, F.; Sasaki, H.; Masunari, N.; Mimori, Y.; Suzuki, G. Association Between Dementia and Midlife Risk Factors: The Radiation Effects Research Foundation Adult Health Study. J. Am. Geriatr. Soc. 2003, 51, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Whitmer, R.A.; Sidney, S.; Selby, J.; Johnston, S.C.; Yaffe, K. Midlife cardiovascular risk factors and risk of dementia in late life. Neurology 2005, 64, 277–281. [Google Scholar] [CrossRef]
- Yoshitake, T.; Kiyohara, Y.; Kato, I.; Ohmura, T.; Iwamoto, H.; Nakayama, K.; Ohmori, S.; Nomiyama, K.; Kawano, H.; Ueda, K.; et al. Incidence and risk factors of vascular dementia and Alzheimer’s disease in a defined elderly Japanese population: The Hisayama Study. Neurology 1995, 45, 1161–1168. [Google Scholar] [CrossRef] [PubMed]
- Qin, H.; Zhu, B.; Hu, C.; Zhao, X. Later-Onset Hypertension Is Associated with Higher Risk of Dementia in Mild Cognitive Impairment. Front. Neurol. 2020, 11, 557977. [Google Scholar] [CrossRef] [PubMed]
- Zúñiga-Salazar, G.A.; Hincapié-Arias, S.M.; Salazar-Bolaños, E.E.; Lara-Terán, J.J.; Cáceres-Vinueza, S.V.; Duarte-Vera, Y.C. Impact of arterial hypertension on the cognitive function of patients between 45 and 65 years. Luis Vernaza Hospital, Guayaquil, Ecuador. Arch. Cardiol. Mex. 2020, 90, 284–292. [Google Scholar] [PubMed]
- Bahchevanov, K.M.; Dzhambov, A.M.; Chompalov, K.; Massaldjieva, R.; Atanassova, P.; Mitkov, M.D. Contribution of Components of Metabolic Syndrome to Cognitive Performance in Middle-Aged Adults. Arch. Clin. Neuropsychol. 2021, 36, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Boo, Y.Y.; Jutila, O.-E.; Cupp, M.A.; Manikam, L.; Cho, S.-I. The identification of established modifiable mid-life risk factors for cardiovascular disease which contribute to cognitive decline: Korean Longitudinal Study of Aging (KLoSA). Aging Clin. Exp. Res. 2021. [Google Scholar] [CrossRef]
- Sun, D.; Thomas, E.A.; Launer, L.J.; Sidney, S.; Yaffe, K.; Fornage, M. Association of blood pressure with cognitive function at midlife: A Mendelian randomization study. BMC Med. Genom. 2020, 13, 121. [Google Scholar] [CrossRef] [PubMed]
- Shim, Y.S.; Shin, H.-E. Impact of the ambulatory blood pressure monitoring profile on cognitive and imaging findings of cerebral small-vessel disease in older adults with cognitive complaints. J. Hum. Hypertens. 2021. [Google Scholar] [CrossRef]
- Antonazzo, B.; Marano, G.; Romagnoli, E.; Ronzoni, S.; Frati, G.; Sani, G.; Janiri, L.; Mazza, M. Impact of arterial hypertension and its management strategies on cognitive function and dementia: A comprehensive umbrella review. Minerva Cardioangiol 2020. [Google Scholar] [CrossRef]
- Kuller, L.H.; Lopez, O.L.; Newman, A.B.; Beauchamp, N.J.; Burke, G.; Dulberg, C.; Fitzpatrick, A.; Fried, L.; Haan, M.N. Risk Factors for Dementia in the Cardiovascular Health Cognition Study. Neuroepidemiology 2003, 22, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Tyas, S.L.; Manfreda, J.; Strain, L.; Montgomery, P.R. Risk factors for Alzheimer’s disease: A population-based, longitudinal study in Manitoba, Canada. Int. J. Epidemiol. 2001, 30, 590–597. [Google Scholar] [CrossRef]
- Carmona-Abellan, M.; Trzeciak, M.; Fernández, M.; Echeveste, B.; Imaz, L.; Luquin, M.-R.; Riverol, M. Blood Pressure and Risk of Cognitive Impairment: The Role of Vascular Disease in Neurodegeneration. Brain Sci. 2021, 11, 385. [Google Scholar] [CrossRef]
- Hestad, K.; Engedal, K.; Schirmer, H.; Strand, B.H. The Effect of Blood Pressure on Cognitive Performance. An 8-Year Follow-Up of the Tromsø Study, Comprising People Aged 45–74 Years. Front. Psychol. 2020, 11, 607. [Google Scholar] [CrossRef]
- Shang, S.; Li, P.; Deng, M.; Jiang, Y.; Chen, C.; Qu, Q. The Age-Dependent Relationship between Blood Pressure and Cognitive Impairment: A Cross-Sectional Study in a Rural Area of Xi’an, China. PLoS ONE 2016, 11, e0159485. [Google Scholar] [CrossRef]
- Feng, R.; Rolls, E.T.; Cheng, W.; Feng, J. Hypertension is associated with reduced hippocampal connectivity and impaired memory. EBioMedicine 2020, 61, 103082. [Google Scholar] [CrossRef]
- Li, H.; Sun, D.; Lu, D.; Zhang, J.; Zeng, J. Low Hippocampal Dentate Gyrus Volume Associated with Hypertension-Related Cognitive Impairment. Am. J. Alzheimer’s Dis. Other Dementiasr 2020, 35, 1533317520949782. [Google Scholar]
- Triantafyllou, A.; Ferreira, J.P.; Kobayashi, M.; Micard, E.; Xie, Y.; Kearney-Schwartz, A.; Hossu, G.; Rossignol, P.; Bracard, S.; Benetos, A. Longer Duration of Hypertension and MRI Microvascular Brain Alterations Are Associated with Lower Hippocampal Volumes in Older Individuals with Hypertension. J. Alzheimer’s Dis. 2020, 74, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Lane, C.; Barnes, J.; Nicholas, J.M.; Sudre, C.; Cash, D.M.; Parker, T.D.; Malone, I.B.; Lu, K.; James, S.-N.; Keshavan, A.; et al. Associations between blood pressure across adulthood and late-life brain structure and pathology in the neuroscience substudy of the 1946 British birth cohort (Insight 46): An epidemiological study. Lancet Neurol. 2019, 18, 942–952. [Google Scholar] [CrossRef]
- Mok, V.; Kim, J.S. Prevention and Management of Cerebral Small Vessel Disease. J. Stroke 2015, 17, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Dong, Y.-H.; Lyu, P.-Y.; Chen, W.-H.; Li, R. Hypertension-Induced Cerebral Small Vessel Disease Leading to Cognitive Impairment. Chin. Med. J. 2018, 131, 615–619. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, K.A.; Emadi, N.; Pearlson, G.D.; Winkler, A.M.; Taylor, B.; Dulipsingh, L.; King, D.; Pittman, B.; Blank, K. Hyperinsulinemia and elevated systolic blood pressure independently predict white matter hyperintensities with associated cognitive decrement in the middle-aged offspring of dementia patients. Metab. Brain Dis. 2017, 32, 849–857. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.W.; Panenka, W.J.; Al-Momen, G.; Gicas, K.M.; Thornton, A.E.; Jones, A.A.; Woodward, M.; Heran, M.K.S.; Vertinsky, A.T.; Su, W.; et al. Cerebral Small Vessel Disease, Risk Factors, and Cognition in Tenants of Precarious Housing. Stroke 2020, 51, 3271–3278. [Google Scholar] [CrossRef]
- Mortensen, K.N.; Sanggaard, S.; Mestre, H.; Lee, H.; Kostrikov, S.; Xavier, A.L.; Gjedde, A.; Benveniste, H.; Nedergaard, M. Impaired Glymphatic Transport in Spontaneously Hypertensive Rats. J. Neurosci. 2019, 39, 6365–6377. [Google Scholar] [CrossRef]
- Held, F.; Morris, A.W.; Pirici, D.; Niklass, S.; Sharp, M.M.; Garz, C.; Assmann, A.; Heinze, H.-J.; Schreiber, F.; Carare, R.O.; et al. Vascular basement membrane alterations and β-amyloid accumulations in an animal model of cerebral small vessel disease. Clin. Sci. 2017, 131, 1001–1013. [Google Scholar] [CrossRef]
- Bender, A.R.; Raz, N. Age-related differences in memory and executive functions in healthy APOE ɛ4 carriers: The contribution of individual differences in prefrontal volumes and systolic blood pressure. Neuropsychologia 2012, 50, 704–714. [Google Scholar] [CrossRef][Green Version]
- Presa, J.L.; Saravia, F.; Bagi, Z.; Filosa, J.A. Vasculo-Neuronal Coupling and Neurovascular Coupling at the Neurovascular Unit: Impact of Hypertension. Front. Physiol. 2020, 11, 584135. [Google Scholar] [CrossRef]
- Nilsson, P.M. Early Vascular Aging in Hypertension. Front. Cardiovasc. Med. 2020, 7, 6. [Google Scholar] [CrossRef]
- Iulita, M.F.; De La Colina, A.N.; Girouard, H. Arterial stiffness, cognitive impairment and dementia: Confounding factor or real risk? J. Neurochem. 2018, 144, 527–548. [Google Scholar] [CrossRef]
- MacIntosh, B.J.; Shirzadi, Z.; Atwi, S.; Detre, J.A.; Dolui, S.; Bryan, R.N.; Launer, L.J.; Swardfager, W. Metabolic and vascular risk factors are associated with reduced cerebral blood flow and poorer midlife memory performance. Hum. Brain Mapp. 2019, 41, 855–864. [Google Scholar] [CrossRef] [PubMed]
- Iadecola, C. The Neurovascular Unit Coming of Age: A Journey through Neurovascular Coupling in Health and Disease. Neuron 2017, 96, 17–42. [Google Scholar] [CrossRef] [PubMed]
- de Montgolfier, O.; Pouliot, P.; Gillis, M.; Ferland, G.; Lesage, F.; Thorin-Trescases, N.; Thorin, É. Systolic hypertension-induced neurovascular unit disruption magnifies vascular cognitive impairment in middle-age atherosclerotic LDLr(−/−):hApoB(+/+) mice. Geroscience 2019, 41, 511–532. [Google Scholar] [CrossRef]
- de Montgolfier, O. High Systolic Blood Pressure Induces Cerebral Microvascular Endothelial Dysfunction, Neurovascular Unit Damage, and Cognitive Decline in Mice. Hypertension 2019, 73, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Iadecola, C. The Pathobiology of Vascular Dementia. Neuron 2013, 80, 844–866. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, G.A. Extracellular matrix inflammation in vascular cognitive impairment and dementia. Clin. Sci. 2017, 131, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Pantoni, L. Cerebral small vessel disease: From pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 2010, 9, 689–701. [Google Scholar] [CrossRef]
- Katsi, V.; Marketou, M.; Maragkoudakis, S.; Didagelos, M.; Charalambous, G.; Parthenakis, F.; Tsioufis, C.; Tousoulis, D. Blood–brain barrier dysfunction: The undervalued frontier of hypertension. J. Hum. Hypertens. 2020, 34, 682–691. [Google Scholar] [CrossRef]
- Yamazaki, Y.; Kanekiyo, T. Blood-Brain Barrier Dysfunction and the Pathogenesis of Alzheimer’s Disease. Int. J. Mol. Sci. 2017, 18, 1965. [Google Scholar] [CrossRef]
- Santoro, J.D. Diminished Blood Pressure Profiles in Children with Down Syndrome. Hypertension 2020, 75, 819–825. [Google Scholar] [CrossRef]
- Lao, P.J.; Gutierrez, J.; Keator, D.; Rizvi, B.; Banerjee, A.; Igwe, K.C.; Laing, K.K.; Sathishkumar, M.; Moni, F.; Andrews, H.; et al. Alzheimer-Related Cerebrovascular Disease in Down Syndrome. Ann. Neurol. 2020, 88, 1165–1177. [Google Scholar] [CrossRef]
- Bayen, E.; Possin, K.L.; Chen, Y.; de Langavant, L.C.; Yaffe, K. Prevalence of Aging, Dementia, and Multimorbidity in Older Adults with Down Syndrome. JAMA Neurol. 2018, 75, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Walker, K.A.; Sharrett, A.R.; Wu, A.; Schneider, A.L.C.; Albert, M.; Lutsey, P.L.; Bandeen-Roche, K.; Coresh, J.; Gross, A.L.; Windham, B.G.; et al. Association of Midlife to Late-Life Blood Pressure Patterns with Incident Dementia. JAMA 2019, 322, 535–545. [Google Scholar] [CrossRef]
- Höcht, C. Blood Pressure Variability: Prognostic Value and Therapeutic Implications. ISRN Hypertens. 2013, 2013, 398485. [Google Scholar] [CrossRef]
- Parati, G.; Ochoa, J.E.; Lombardi, C.; Bilo, G. Blood Pressure Variability: Assessment, Predictive Value, and Potential as a Therapeutic Target. Curr. Hypertens. Rep. 2015, 17, 537. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Wolters, F.J.; Chibnik, L.B.; Licher, S.; Ikram, M.K.; Hofman, A. Variation in blood pressure and long-term risk of dementia: A population-based cohort study. PLoS Med. 2019, 16, e1002933. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, A.; Satoh, M.; Kikuya, M.; Ohkubo, T.; Hirano, M.; Inoue, R.; Hashimoto, T.; Hara, A.; Hirose, T.; Obara, T.; et al. Day-to-day variability in home blood pressure is associated with cognitive decline: The Ohasama study. Hypertension 2014, 63, 1333–1338. [Google Scholar] [CrossRef]
- Yano, Y.; Griswold, M.; Wang, W.; Greenland, P.; Lloyd-Jones, D.M.; Heiss, G.; Gottesman, R.F.; Mosley, T.H. Long-Term Blood Pressure Level and Variability From Midlife to Later Life and Subsequent Cognitive Change: The ARIC Neurocognitive Study. J. Am. Heart Assoc. 2018, 7, e009578. [Google Scholar] [CrossRef]
- Godai, K.; SONIC Study Group; Kabayama, M.; Gondo, Y.; Yasumoto, S.; Sekiguchi, T.; Noma, T.; Tanaka, K.; Kiyoshige, E.; Akagi, Y. Day-to-day blood pressure variability is associated with lower cognitive performance among the Japanese community-dwelling oldest-old population: The SONIC study. Hypertens. Res. 2019, 43, 404–411. [Google Scholar] [CrossRef]
- de Heus, R.A.A.; Rikkert, M.G.M.O.; Tully, P.J.; Lawlor, B.A.; Claassen, J.A.H.R. Blood Pressure Variability and Progression of Clinical Alzheimer Disease. Hypertension 2019, 74, 1172–1180. [Google Scholar] [CrossRef]
- Oishi, E.; Ohara, T.; Sakata, S.; Fukuhara, M.; Hata, J.; Yoshida, D.; Shibata, M.; Ohtsubo, T.; Kitazono, T.; Kiyohara, Y.; et al. Day-to-Day Blood Pressure Variability and Risk of Dementia in a General Japanese Elderly Population: The Hisayama Study. Circulation 2017, 136, 516–525. [Google Scholar] [CrossRef]
- Cho, N.; Hoshide, S.; Nishizawa, M.; Fujiwara, T.; Kario, K. Relationship Between Blood Pressure Variability and Cognitive Function in Elderly Patients with Good Blood Pressure Control. Am. J. Hypertens. 2017, 31, 293–298. [Google Scholar] [CrossRef]
- Fujiwara, T.; Hoshide, S.; Kanegae, H.; Eguchi, K.; Kario, K. Exaggerated blood pressure variability is associated with memory impairment in very elderly patients. J. Clin. Hypertens. 2018, 20, 637–644. [Google Scholar] [CrossRef]
- Liu, Z.; Zhao, Y.; Zhang, H.; Chai, Q.; Cui, Y.; Diao, Y.; Xiu, J.; Sun, X.; Jiang, G. Excessive variability in systolic blood pressure that is self-measured at home exacerbates the progression of brain white matter lesions and cognitive impairment in the oldest old. Hypertens. Res. 2016, 39, 245–253. [Google Scholar] [CrossRef]
- McDonald, C.; Pearce, M.S.; Kerr, S.R.J.; Newton, J.L. Blood pressure variability and cognitive decline in older people: A 5-year longitudinal study. J. Hypertens. 2017, 35, 140–147. [Google Scholar] [CrossRef]
- Nagai, M.; Hoshide, S.; Nishikawa, M.; Masahisa, S.; Kario, K. Visit-to-visit blood pressure variability in the elderly: Associations with cognitive impairment and carotid artery remodeling. Atherosclerosis 2014, 233, 19–26. [Google Scholar] [CrossRef]
- Yıldırım, E.; Ermis, E.; Allahverdiyev, S.; Ucar, H.; Yavuzer, S.; Yavuzer, H.; Cengiz, M. Relationship between blood pressure variability and cognitive function in geriatric hypertensive patients with well-controlled blood pressure. Aging Clin. Exp. Res. 2019, 32, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Tsang, S.; Sperling, S.; Park, M.H.; Helenius, I.M.; Williams, I.C.; Manning, C. Blood Pressure Variability and Cognitive Function Among Older African Americans: Introducing a New Blood Pressure Variability Measure. Cogn. Behav. Neurol. 2017, 30, 90–97. [Google Scholar] [CrossRef] [PubMed]
- van Middelaar, T.; van Dalen, J.W.; van Gool, W.A.; van den Born, B.H.; van Vught, L.A.; van Charante, E.P.M.; Richard, E. Visit-To-Visit Blood Pressure Variability and the Risk of Dementia in Older People. J. Alzheimers Dis. 2018, 62, 727–735. [Google Scholar] [CrossRef]
- Qin, B.; Viera, A.J.; Muntner, P.; Plassman, B.L.; Edwards, L.; Adair, L.S.; Popkin, B.M.; Mendez, M.A. Visit-to-Visit Variability in Blood Pressure Is Related to Late-Life Cognitive Decline. Hypertension 2016, 68, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Alpérovitch, A.; Blachier, M.; Soumaré, A.; Ritchie, K.; Dartigues, J.-F.; Richard-Harston, S.; Tzourio, C. Blood pressure variability and risk of dementia in an elderly cohort, the Three-City Study. Alzheimer’s Dement. 2013, 10, S330–S337. [Google Scholar] [CrossRef] [PubMed]
- Epstein, N.U.; Lane, K.A.; Farlow, M.R.; Risacher, S.L.; Saykin, A.; Gao, S.; Initiative, T.A.D.N. Cognitive Dysfunction and Greater Visit-to-Visit Systolic Blood Pressure Variability. J. Am. Geriatr. Soc. 2013, 61, 2168–2173. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.L.; Kroon, A.A.; Van Sloten, T.T.; Van Boxtel, M.P.; Verhey, F.R.; Schram, M.; Köhler, S.; Stehouwer, C.D.; Henry, R.M. Greater Blood Pressure Variability Is Associated with Lower Cognitive Performance. Hypertension 2019, 73, 803–811. [Google Scholar] [CrossRef]
- Rouch, L.; Cestac, P. Visit-to-Visit Blood Pressure Variability Is Associated with Cognitive Decline and Incident Dementia: The S.AGES Cohort. Hypertension 2020, 76, 1280–1288. [Google Scholar] [CrossRef]
- Sabayan, B.; Wijsman, L.W.; Foster-Dingley, J.C.; Stott, D.J.; Ford, I.; Buckley, B.M.; Sattar, N.; Jukema, J.W.; Van Osch, M.J.P.; Van Der Grond, J.; et al. Association of visit-to-visit variability in blood pressure with cognitive function in old age: Prospective cohort study. BMJ 2013, 347, f4600. [Google Scholar] [CrossRef]
- Yoo, J.E.; Shin, D.W.; Han, K.; Kim, D.; Lee, S.-P.; Jeong, S.-M.; Lee, J.; Kim, S. Blood Pressure Variability and the Risk of Dementia. Hypertension 2020, 75, 982–990. [Google Scholar] [CrossRef]
- Lattanzi, S.; Luzzi, S.; Provinciali, L.; Silvestrini, M. Blood pressure variability predicts cognitive decline in Alzheimer’s disease patients. Neurobiol. Aging 2014, 35, 2282–2287. [Google Scholar] [CrossRef]
- Sible, I.J.; Nation, D.A. Long-term blood pressure variability across the clinical and biomarker spectrum of Alzheimer’s disease. J. Alzheimers Dis. 2020, 77, 1655–1669. [Google Scholar] [CrossRef] [PubMed]
- Lattanzi, S.; Luzzi, S.; Provinciali, L.; Silvestrini, M. Blood Pressure Variability in Alzheimer’s Disease and Frontotemporal Dementia: The Effect on the Rate of Cognitive Decline. J. Alzheimer’s Dis. 2015, 45, 387–394. [Google Scholar] [CrossRef]
- Lattanzi, S.; Brigo, F.; Vernieri, F.; Silvestrini, M. Visit-to-visit variability in blood pressure and Alzheimer’s disease. J. Clin. Hypertens. 2018, 20, 918–924. [Google Scholar] [CrossRef]
- Iadecola, C.; Parikh, N.S. Blood Pressure Ups and Downs Foreshadow Cerebral Microangiopathy. J. Am. Coll. Cardiol. 2020, 75, 2400–2402. [Google Scholar] [CrossRef]
- Zhou, T.L.; Rensma, S.P.; van der Heide, F.C.; Henry, R.M.; Kroon, A.A.; Houben, A.J.; Jansen, J.F.; Backes, W.H.; Berendschot, T.T.; Schouten, J.S.; et al. Blood pressure variability and microvascular dysfunction: The Maastricht Study. J. Hypertens. 2020, 38, 1541–1550. [Google Scholar] [CrossRef] [PubMed]
- Anselmino, M.; Scarsoglio, S.; Saglietto, A.; Gaita, F.; Ridolfi, L. Transient cerebral hypoperfusion and hypertensive events during atrial fibrillation: A plausible mechanism for cognitive impairment. Sci. Rep. 2016, 6, 28635. [Google Scholar] [CrossRef] [PubMed]
- De Leeuw, F.-E.; De Groot, J.C.; Oudkerk, M.; Kors, J.A.; Hofman, A.; Van Gijn, J.; Breteler, M.M. Atrial fibrillation and the risk of cerebral white matter lesions. Neurology 2000, 54, 1795–1801. [Google Scholar] [CrossRef] [PubMed]
- Stefansdottir, H.; Arnar, D.O.; Aspelund, T.; Sigurdsson, S.; Jónsdóttir, M.K.; Hjaltason, H.; Launer, L.J.; Gudnason, V. Atrial Fibrillation is Associated with Reduced Brain Volume and Cognitive Function Independent of Cerebral Infarcts. Stroke 2013, 44, 1020–1025. [Google Scholar] [CrossRef] [PubMed]
- Miao, C.-Y.; Su, D.-F. The importance of blood pressure variability in rat aortic and left ventricular hypertrophy produced by sinoaortic denervation. J. Hypertens. 2002, 20, 1865–1872. [Google Scholar] [CrossRef]
- Nagai, M.; Dote, K.; Kato, M.; Sasaki, S.; Oda, N.; Kagawa, E.; Nakano, Y.; Yamane, A.; Higashihara, T.; Miyauchi, S.; et al. Visit-to-Visit Blood Pressure Variability and Alzheimer’s Disease: Links and Risks. J. Alzheimer’s Dis. 2017, 59, 515–526. [Google Scholar] [CrossRef] [PubMed]
- Yano, Y.; Reis, J.P.; Levine, D.A.; Bryan, R.N.; Viera, A.J.; Shimbo, D.; Tedla, Y.G.; Allen, N.B.; Schreiner, P.J.; Bancks, M.P.; et al. Visit-to-Visit Blood Pressure Variability in Young Adulthood and Hippocampal Volume and Integrity at Middle Age: The CARDIA Study (Coronary Artery Risk Development in Young Adults). Hypertension 2017, 70, 1091–1098. [Google Scholar] [CrossRef]
- Ma, Y.; Tully, P.J.; Hofman, A.; Tzourio, C. Blood Pressure Variability and Dementia: A State-of-the-Art Review. Am. J. Hypertens. 2020, 33, 1059–1066. [Google Scholar] [CrossRef]
- de Heus, R.A.A.; Reumers, S.F.I.; van der Have, A.; Tumelaire, M.; Tully, P.J.; Claassena, J.A.H.R. Day-to-Day Home Blood Pressure Variability is Associated with Cerebral Small Vessel Disease Burden in a Memory Clinic Population. J. Alzheimers Dis. 2020, 74, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, Y.; Wada, M.; Sato, H.; Nagasawa, H.; Koyama, S.; Takahashi, Y.; Kawanami, T.; Kato, T. Impact of Ambulatory Blood Pressure Variability on Cerebral Small Vessel Disease Progression and Cognitive Decline in Community-Based Elderly Japanese. Am. J. Hypertens. 2014, 27, 1257–1267. [Google Scholar] [CrossRef] [PubMed]
- Tully, P.J.; Debette, S.; Tzourio, C. The association between systolic blood pressure variability with depression, cognitive decline and white matter hyperintensities: The 3C Dijon MRI study. Psychol. Med. 2017, 48, 1444–1453. [Google Scholar] [CrossRef] [PubMed]
- Tully, P.J.; Yano, Y.; Launer, L.J.; Kario, K.; Nagai, M.; Mooijaart, S.P.; Claassen, J.A.H.R.; Lattanzi, S.; Vincent, A.D.; Tzourio, C.; et al. Association between Blood Pressure Variability and Cerebral Small-Vessel Disease: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2020, 9, e013841. [Google Scholar] [CrossRef]
- Ma, Y.; Yilmaz, P.; Bos, D.; Blacker, D.; Viswanathan, A.; Ikram, M.A.; Hofman, A.; Vernooij, M.W. Blood Pressure Variation and Subclinical Brain Disease. J. Am. Coll. Cardiol. 2020, 75, 2387–2399. [Google Scholar] [CrossRef]
- Ma, Y. Blood Pressure Variability and Cerebral Small Vessel Disease: A Systematic Review and Meta-Analysis of Population-Based Cohorts. Stroke 2020, 51, 82–89. [Google Scholar] [CrossRef]
- Gong, L.; Gu, Y.; Yu, Q.; Wang, H.; Zhu, X.; Dong, Q.; Xu, R.; Zhao, Y.; Liu, X. Prognostic Factors for Cognitive Recovery Beyond Early Poststroke Cognitive Impairment (PSCI): A Prospective Cohort Study of Spontaneous Intracerebral Hemorrhage. Front. Neurol. 2020, 11, 278–278. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Wang, J.; Liu, N.; Xiao, X.; Geng, S.; Meng, P.; Ji, N.; Sun, Y.; Xu, B.; Xu, Y.; et al. Effects of Blood Pressure in the Early Phase of Ischemic Stroke and Stroke Subtype on Poststroke Cognitive Impairment. Stroke 2018, 49, 1610–1617. [Google Scholar] [CrossRef]
- Levine, D.A.; Galecki, A.T.; Okullo, D.; Briceño, E.M.; Kabeto, M.U.; Morgenstern, L.B.; Langa, K.M.; Giordani, B.; Brook, R.; Sanchez, B.N.; et al. Association of Blood Pressure and Cognition after Stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 104754. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Nagakane, Y.; Tomii, Y.; Akiguchi, I. High Morning and Bedtime Home Blood Pressures Strongly Predict for Post-Stroke Cognitive Impairment. J. Stroke Cerebrovasc. Dis. 2016, 25, 1856–1863. [Google Scholar] [CrossRef]
- Sachdev, P.; Brodaty, H.; Valenzuela, M.; Lorentz, L.; Looi, J.; Berman, K.; Ross, A.; Wen, W.; Zagami, A. Clinical Determinants of Dementia and Mild Cognitive Impairment following Ischaemic Stroke: The Sydney Stroke Study. Dement. Geriatr. Cogn. Disord. 2006, 21, 275–283. [Google Scholar] [CrossRef]
- Ihle-Hansen, H.; Thommessen, B.; Fagerland, M.; Oksengard, A.; Wyller, T.; Engedal, K.; Fure, B. Blood pressure control to prevent decline in cognition after stroke. Vasc. Health Risk Manag. 2015, 11, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.-H.; Li, J.; Li, X.-L.; Ding, M.; Mao, C.-J.; Zhu, X.-Y.; Liu, C.-F. Hypertension with Hyperhomocysteinemia Increases the Risk of Early Cognitive Impairment after First-Ever Ischemic Stroke. Eur. Neurol. 2020, 82, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Geng, S.; Liu, N.; Meng, P.; Ji, N.; Sun, Y.; Xu, Y.; Zhang, G.; He, X.; Cai, Z.; Wang, B.; et al. Midterm Blood Pressure Variability Is Associated with Poststroke Cognitive Impairment: A Prospective Cohort Study. Front. Neurol. 2017, 8, 365. [Google Scholar] [CrossRef]
- Lee, J.-H.; Oh, E.; Oh, M.S.; Kim, C.; Jung, S.; Park, J.-H.; Kang, Y.; Yu, K.-H.; Lee, B.-C. Highly Variable Blood Pressure as a Predictor of Poor Cognitive Outcome in Patients with Acute Lacunar Infarction. Cogn. Behav. Neurol. 2014, 27, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y. Blood pressure variability is related to faster cognitive decline in ischemic stroke patients: PICASSO subanalysis. Sci. Rep. 2021, 11, 5049. [Google Scholar] [CrossRef]
- Ishitsuka, K.; Kamouchi, M.; Hata, J.; Fukuda, K.; Matsuo, R.; Kuroda, J.; Ago, T.; Kuwashiro, T.; Sugimori, H.; Nakane, H.; et al. High Blood Pressure After Acute Ischemic Stroke Is Associated with Poor Clinical Outcomes. Hypertension 2014, 63, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Stead, L.G.; Gilmore, R.M.; Decker, W.W.; Weaver, A.L.; Brown, R.D. Initial emergency department blood pressure as predictor of survival after acute ischemic stroke. Neurology 2005, 65, 1179–1183. [Google Scholar] [CrossRef] [PubMed]
- Bath, P.M.; Appleton, J.P.; Krishnan, K.; Sprigg, N. Blood Pressure in Acute Stroke. Stroke 2018, 49, 1784–1790. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [PubMed]
- Sandset, E.C.; Anderson, C.S.; Bath, P.M.; Christensen, H.; Fischer, U.; Gąsecki, D.; Lal, A.; Manning, L.S.; Sacco, S.; Steiner, T.; et al. European Stroke Organisation (ESO) guidelines on blood pressure management in acute ischaemic stroke and intracerebral haemorrhage. Eur. Stroke J. 2021, 6, 23969873211012133. [Google Scholar] [CrossRef]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 2021. [Google Scholar] [CrossRef]
- Ahmed, H.A.; Ishrat, T.; Pillai, B.; Fouda, A.; Sayed, M.A.; Eldahshan, W.; Waller, J.L.; Ergul, A.; Fagan, S.C. RAS modulation prevents progressive cognitive impairment after experimental stroke: A randomized, blinded preclinical trial. J. Neuroinflammation 2018, 15, 229. [Google Scholar] [CrossRef]
- Jackson, L.; Dong, G.; Althomali, W.; Sayed, M.A.; Eldahshan, W.; Baban, B.; Johnson, M.H.; Filosa, J.; Fagan, S.C.; Ergul, A. Delayed Administration of Angiotensin II Type 2 Receptor (AT2R) Agonist Compound 21 Prevents the Development of Post-stroke Cognitive Impairment in Diabetes Through the Modulation of Microglia Polarization. Transl. Stroke Res. 2020, 11, 762–775. [Google Scholar] [CrossRef] [PubMed]
- Oh, M.S.; Yu, K.-H.; Hong, K.-S.; Kang, D.-W.; Park, J.-M.; Bae, H.-J.; Koo, J.; Lee, J.; Lee, B.-C. Modest Blood Pressure Reduction with Valsartan in Acute Ischemic Stroke: A Prospective, Randomized, Open-Label, Blinded-End-Point Trial. Int. J. Stroke 2015, 10, 745–751. [Google Scholar] [CrossRef]
- Sandset, E.C.; Bath, P.; Boysen, G.; Jatuzis, D.; Kõrv, J.; Lüders, S.; Murray, G.D.; Richter, P.S.; Roine, R.; Terént, A.; et al. The angiotensin-receptor blocker candesartan for treatment of acute stroke (SCAST): A randomised, placebo-controlled, double-blind trial. Lancet 2011, 377, 741–750. [Google Scholar] [CrossRef]
- Li, N.-C.; Le, K.; Whitmer, R.; Kivipelto, M.; Lawler, E.; Kazis, L.; Wolozin, B. Use of angiotensin receptor blockers and risk of dementia in a predominantly male population: Prospective cohort analysis. BMJ 2010, 340, b5465. [Google Scholar] [CrossRef]
- Anderson, C.; Teo, K.; Gao, P.; Arima, H.; Dans, A.; Unger, T.; Commerford, P.; Dyal, L.; Schumacher, H.; Pogue, J.; et al. Renin-angiotensin system blockade and cognitive function in patients at high risk of cardiovascular disease: Analysis of data from the ONTARGET and TRANSCEND studies. Lancet Neurol. 2011, 10, 43–53. [Google Scholar] [CrossRef]
- Group, T.P.C. Effects of Blood Pressure Lowering with Perindopril and Indapamide Therapy on Dementia and Cognitive Decline in Patients with Cerebrovascular Disease. Arch. Intern. Med. 2003, 163, 1069–1075. [Google Scholar]
- Ölmestig, J.; Marlet, I.R.; Hansen, R.H.; Rehman, S.; Krawcyk, R.S.; Rostrup, E.; Lambertsen, K.L.; Kruuse, C. Tadalafil may improve cerebral perfusion in small-vessel occlusion stroke—a pilot study. Brain Commun. 2020, 2, 11. [Google Scholar] [CrossRef] [PubMed]
- ENOS Trial Investigators. Efficacy of nitric oxide, with or without continuing antihypertensive treatment, for management of high blood pressure in acute stroke (ENOS): A partial-factorial randomised controlled trial. Lancet 2015, 385, 617–628. [Google Scholar] [CrossRef]
- O’Brien, E.C.; Greiner, M.A.; Xian, Y.; Fonarow, G.; Olson, D.M.; Schwamm, L.H.; Bhatt, D.L.; Smith, E.E.; Maisch, L.; Hannah, D.; et al. Clinical Effectiveness of Statin Therapy After Ischemic Stroke: Primary Results From the Statin Therapeutic Area of the Patient-Centered Research Into Outcomes Stroke Patients Prefer and Effectiveness Research (PROSPER) Study. Circulation 2015, 132, 1404–1413. [Google Scholar] [CrossRef]
- Parfenov, V.; Belavina, G.R.; Vakhnina, N.V.; Gusev, V.V.; Levin, I.; Markin, S.P.; Starchina, I. Use of omaron in patients with post-stroke cognitive disorders. Zhurnal Nevrol. Psikhiatrii Korsakova 2009, 109, 41–45. [Google Scholar]
- Shozawa, H.; Oguchi, T.; Tsuji, M.; Yano, S.; Kiuchi, Y.; Ono, K. Supratherapeutic concentrations of cilostazol inhibits β-amyloid oligomerization in vitro. Neurosci. Lett. 2018, 677, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Park, S.Y.; Heo, H.J.; Lee, W.S.; Hong, K.W.; Kim, C.D. Multitarget-directed cotreatment with cilostazol and aripiprazole for augmented neuroprotection against oxidative stress-induced toxicity in HT22 mouse hippocampal cells. Eur. J. Pharmacol. 2019, 857, 172454. [Google Scholar] [CrossRef]
- Senda, J.; Ito, K.; Kotake, T.; Kanamori, M.; Kishimoto, H.; Kadono, I.; Nakagawa-Senda, H.; Wakai, K.; Katsuno, M.; Nishida, Y.; et al. Cilostazol use is associated with FIM cognitive improvement during convalescent rehabilitation in patients with ischemic stroke: A retrospective study. Nagoya J. Med. Sci. 2019, 81, 359–373. [Google Scholar] [PubMed]
- Lim, J.-S.; Kwon, S.U.; Yu, K.-H.; Yu, S.; Park, J.-H.; Lee, B.-C.; Oh, M.S.; Kim, Y.-J.; Rha, J.-H.; Hwang, Y.-H.; et al. Cilostazol and Probucol for Cognitive Decline after Stroke: A Cognitive Outcome Substudy of the PICASSO Trial. J. Stroke 2021, 23, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.H.; Park, Y.H.; Ohn, S.H.; Park, C.-H.; Lee, P.K.W.; Kim, Y.-H. Neural correlates of donepezil-induced cognitive improvement in patients with right hemisphere stroke: A pilot study. Neuropsychol. Rehabil. 2011, 21, 502–514. [Google Scholar] [CrossRef] [PubMed]
- Narasimhalu, K.; Effendy, S.; Sim, C.H.; Lee, J.M.; Chen, I.; Hia, S.B.; Xue, H.L.; Corrales, M.P.; Chang, H.M.; Wong, M.C.; et al. A randomized controlled trial of rivastigmine in patients with cognitive impairment no dementia because of cerebrovascular disease. Acta Neurol. Scand. 2010, 121, 217–224. [Google Scholar] [CrossRef]
- Gagnon, D.J.; Leclerc, A.M.; Riker, R.R.; Brown, C.S.; May, T.; Nocella, K.; Cote, J.; Eldridge, A.; Seder, D.B. Amantadine and Modafinil as Neurostimulants During Post-stroke Care: A Systematic Review. Neurocritical Care 2020, 33, 283–297. [Google Scholar] [CrossRef]
- Du, Y. Effect of acupuncture treatment on post-stroke cognitive impairment: A randomized controlled trial. Medicine 2020, 99, e23803. [Google Scholar] [CrossRef]
- Zhou, L.; Wang, Y.; Qiao, J.; Wang, Q.M.; Luo, X. Acupuncture for Improving Cognitive Impairment After Stroke: A Meta-Analysis of Randomized Controlled Trials. Front. Psychol. 2020, 11, 549265. [Google Scholar] [CrossRef]
- Shih, C.-C.; Yeh, C.-C.; Hu, C.-J.; Lane, H.-L.; Tsai, C.-C.; Chen, T.-L.; Liao, C.-C. Risk of dementia in patients with non-haemorrhagic stroke receiving acupuncture treatment: A nationwide matched cohort study from Taiwan’s National Health Insurance Research Database. BMJ Open 2017, 7, e013638. [Google Scholar] [CrossRef] [PubMed]
- Cumming, T.B.; Tyedin, K.; Churilov, L.; Morris, M.E.; Bernhardt, J. The effect of physical activity on cognitive function after stroke: A systematic review. Int. Psychogeriatrics 2011, 24, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Teuschl, Y.; Matz, K.; Brainin, M. Prevention of post-stroke cognitive decline: A review focusing on lifestyle interventions. Eur. J. Neurol. 2012, 20, 35–49. [Google Scholar] [CrossRef]
- Reale, M.; Costantini, E.; Jagarlapoodi, S.; Khan, H.; Belwal, T.; Cichelli, A. Relationship of Wine Consumption with Alzheimer’s Disease. Nutrients 2020, 12, 206. [Google Scholar] [CrossRef] [PubMed]
- Moroney, J.T.; Bagiella, E.; Tatemichi, T.K.; Paik, M.C.; Stern, Y.; Desmond, D.W. Dementia after stroke increases the risk of long-term stroke recurrence. Neurology 1997, 48, 1317–1325. [Google Scholar] [CrossRef]
- Fisicaro, F.; Lanza, G.; Pennisi, M.; Vagli, C.; Cantone, M.; Pennisi, G.; Ferri, R.; Bella, R. Moderate Mocha Coffee Consumption Is Associated with Higher Cognitive and Mood Status in a Non-Demented Elderly Population with Subcortical Ischemic Vascular Disease. Nutrients 2021, 13, 536. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, J.; Qian, L.; Zang, X.-F.; Zhang, S.-Y.; Jin, J.-L.; Zhu, X.-L.; Zhang, X.-B.; Wang, Z.-Y.; Xu, Y. Icariin promotes histone acetylation and attenuates post-stroke cognitive impairment in the central cholinergic circuits of mice. Neuroscience 2013, 236, 281–288. [Google Scholar] [CrossRef]
- Pennisi, M.; Lanza, G.; Cantone, M.; D’Amico, E.; Fisicaro, F.; Puglisi, V.; Vinciguerra, L.; Bella, R.; Vicari, E.; Malaguarnera, G. Acetyl-L-Carnitine in Dementia and Other Cognitive Disorders: A Critical Update. Nutrients 2020, 12, 1389. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Choi, H.; Lee, C.-N.; Kim, Y.B.; Kwak, Y.T. A Multicenter, Randomized, Double-blind, Placebo-controlled Clinical Trial for Efficacy of Acetyl-L-carnitine in Patients with Dementia Associated with Cerebrovascular Disease. Dement. Neurocognitive Disord. 2018, 17, 1–10. [Google Scholar] [CrossRef]
- Li, Y.; Luo, H.; Yu, Q.; Yin, L.; Li, K.; Li, Y.; Fu, J. Cerebral Functional Manipulation of Repetitive Transcranial Magnetic Stimulation in Cognitive Impairment Patients After Stroke: An fMRI Study. Front. Neurol. 2020, 11, 977. [Google Scholar] [CrossRef]
- Yin, M.; Liu, Y.; Zhang, L.; Zheng, H.; Peng, L.; Ai, Y.; Luo, J.; Hu, X. Effects of rTMS Treatment on Cognitive Impairment and Resting-State Brain Activity in Stroke Patients: A Randomized Clinical Trial. Front. Neural Circuits 2020, 14, 563777. [Google Scholar] [CrossRef]
- Hara, T.; Shanmugalingam, A.; McIntyre, A.; Burhan, A. The Effect of Non-Invasive Brain Stimulation (NIBS) on Attention and Memory Function in Stroke Rehabilitation Patients: A Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 227. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Zhang, Z.; Su, Y.; Kang, L.; Geng, D.; Wang, Y.; Luan, F.; Wang, M.; Cui, H. Magnetic stimulation modulates structural synaptic plasticity and regulates BDNF-TrkB signal pathway in cultured hippocampal neurons. Neurochem. Int. 2013, 62, 84–91. [Google Scholar] [CrossRef]
- Sun, L.; Lu, H.; Zhang, T.; Wen, M. Impact of Repetitive Transcranial Magnetic Stimulation on Post-Stroke Dysmnesia and the Role of BDNF Val66Met SNP. Med. Sci. Monit. 2015, 21, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Chen, J.; Li, C.; An, D.; Tang, Z.; Wen, H. High-Frequency rTMS Improves Cognitive Function by Regulating Synaptic Plasticity in Cerebral Ischemic Rats. Neurochem. Res. 2021, 46, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Liu, M.; Cheng, Y.; Jia, C.; Pan, X.; Gou, Q.; Liu, X.; Cao, H.; Zhang, L. Repetitive transcranial magnetic stimulation for the treatment of post-stroke depression: A systematic review and meta-analysis of randomized controlled clinical trials. J. Affect. Disord. 2017, 211, 65–74. [Google Scholar] [CrossRef]
- Baylan, S.; Swann-Price, R.; Peryer, G.; Quinn, T. The effects of music listening interventions on cognition and mood post-stroke: A systematic review. Expert Rev. Neurother. 2016, 16, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Särkämö, T.; Tervaniemi, M.; Laitinen, S.; Forsblom, A.; Soinila, S.; Mikkonen, M.; Autti, T.; Silvennoinen, H.M.; Erkkilä, J.; Laine, M.; et al. Music listening enhances cognitive recovery and mood after middle cerebral artery stroke. Brain 2008, 131, 866–876. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author and Year | Population | Measurement and Duration | Case Number | Outcome Measure | Blood Pressure Parameter | Result |
|---|---|---|---|---|---|---|
| Launer, L.J. et al. [100] | Middle-aged Japanese American, male | Prospective, 20–25 years follow up | 3703 normal population | CASI, IQCODE | SBP, DBP | BP↑→Risk for dementia↑in drug naïve men |
| Kivipelto, M. et al. [101] | Mild-aged, Finnish | Prospective, 21 (SD 4.9) years follow up | 1449 normal population | MMSE | SBP, DBP | SBP↑→Risk for dementia↑ |
| Yamada M. et al. [102] | Geriatric, Japanese | Retrospective 25–30 years | No dementia: 1660 Dementia: 114 | CASI, MMSE, Hasegawa Dementia Scale (HDS) | SBP | SBP↑→Risk for dementia↑ |
| Whitmer, R.A et al. [103] | Middle-aged, American | Prospective 20–30 years follow up | 8845 normal population | Diagnosis of Dementia | Diagnosis of hypertension | Hypertension →Risk for dementia↑ |
| Yoshitake, T et al. [104] | Geriatric, Japanese | Prospective 7 years follow up | 828 normal population | MMSE, HDS | SBP | SBP↑→Risk for dementia↑ |
| Qin, H. et. al. [105] | Middle-aged to geriatric, Chinese | Prospective 7 years follow up | 277 MCI patients | MMSE, MoCA, CDR | Diagnosis of hypertension | Hypertension →Risk for dementia↑ |
| Zúñiga-Salazar, G.A., et al. [106] | Middle-aged, Ecuadorian | Cross section, observational | Hypertensive, non-demented 60 | MoCA | SBP, DBP, Diagnosis of HTN | Hypertension duration↑→ MoCA score↓ SBP↑→ MoCA score↓ |
| Bahchevanov, K.M., et al. [107] | Middle-aged, Bulgarian | Cross section | No dementia: 112 | Consortium to Establish a Registry for Alzheimer’s disease Neuropsychological Battery (CERAD-NB) | Diagnosis of HTN | Hypertension → CERAD-NB score↓ |
| Boo, Y.Y., et al. [108] | Middle-aged, Korean | Prospective 14 years follow up | 4289 normal population | MMSE | BP | BP↑→Risk for dementia↑ |
| Sun, D., et al. [109] | Middle-aged, American | Prospective 30 years follow up | 1369 normal population | Verbal learning Test, Digital Symbol Substitution Test (DSST), Stroop Interference Test | SBP, DBP, PP | 10 mmHg ↑in SBP, DBP, PP →DSST score↓ |
| Shim, Y.S. and H.E. Shin [110] | Geriatric, Korean | Cross section | Impaired cognition: 174 | MMSE | SBP, short-term BPV | SBP →↑→Risk for dementia↑ |
| Kuller, L.H. et al. [112] | Geriatric, American | Retrospective | 3608 normal population | MMSE, IQCODE | Diagnosis of hypertension | No relation between hypertension and dementia |
| Tyas, S.L. et al. [113] | Geriatric, Canadian | Prospective 7 years follow up | Normal cognition: 1335 Impaired cognition: 42 | Modified MMSE | Diagnosis of hypertension | No relation between hypertension and dementia |
| Carmona-Abellan, M., et al. [114] | Middle-aged to geriatric, Spain | Retrospective >2.5 years follow up | Normal cognition: 2087 | Diagnosis of dementia, MCI | SBP, DBP | ↓SBP, BP → Risk of cognitive impairment ↑ |
| Hestad, K., et al. [115] | Middle-aged to geriatric, Norwegian | Prospective 8 years follow up | 4465 normal population | MMSE, Digit symbol Test, Twelve-word test | BP | Male ≤ 65↑SBP,↑DBP → Cognition↓; reverse in male >65 Female≤ 65↑SBP → Cognition ↑; reverse in female >65 |
| Feng, R. et al. [117] | UK biobank | Cross section | Hypertensive: 2720 Normal BP: 12366 | prospective memory, numeric memory, fluid intelligence, reaction time | Diagnosis of hypertension | Hypertension →Risk for dementia↑ |
| Li, H. et al. [118] | Middle-aged, Chinese | Cross section | cognitive impairment: 59 | MoCA, Stroop test, Verbal fluency test | SBP, SBP variability (SBPV) | ↑SBP, SBP variability → ↓dentate gyrus volume |
| Walker, K.A., et al. [143] | Middle-aged, American | Prospective 24 years follow up | 4761 normal population | Comprehensive neuropsychological battery, CDR, diagnosis of dementia | SBP, DBP | midlife hypertension and late-life hypotension → risk for dementia ↑ |
| Ma, Y. et al. [146] | Geriatric, Dutch | Prospective 14 years follow up | Normal cognition: 5273 | MMSE | Long-term SBPV, Long-term DBPV | ↑long-term SBPV,↑DBPV→ Risk of cognitive impairment↑ |
| Yano, Y. et al. [148] | Middle-aged, American | Prospective 25 years follow up | 15792 normal population | Delay Word Recall Test, Digit Symbol Substitution Test, Word Fluency Test | SBP, DBP, SBPV, DBPV, | ↑SBPV,↑DBPV→ Cognitive function ↓ SBP, DBP → No association |
| Godai Si, K. et al. [149] | Geriatric, Japanese | Cross section | 111 normal population | MoCA | Short-term BPV | ↑short-term BPV → Risk of cognitive impairment↑ |
| de Haus, R.A.A. et al. [150] | Geriatric, Dutch | Prospective 1.5 years follow up | 460 mild-to-moderate AD patients | Alzheimer’s Disease Assessment Scale–cognitive subscale (ADAS-cog) | Long-term BPV Short-term BPV | ↑short-term BPV, ↑long-term BPV → Risk of cognitive impairment↑ |
| Oishi, E. et al. [151] | Geriatric, Japanese | Prospective 5 years follow up | 1674 normal population | MMSE, HDS | Day-to-day BPV Daily BPV SBP | ↑Day-to-day BPV→ risk of cognitive impairment↑ ↑SBP →Risk of VaD↑ |
| Cho, N. et al. [152] | Geriatric, Japanese | Cross section | 232 normal population | MoCA | SBP, BPV | ↑BPV → Risk of cognitive impairment↑ |
| Fujiwara, T. et al. [153] | Geriatric, Japanese | Prospective 1 year follow up | 524 normal population | Working memory test | Short-term BPV Long-term BPV | ↑BPV → Risk of cognitive impairment↑ |
| Liu, Z. et al. [154] | Geriatric, Chinese | Prospective 2.3 years follow up | 248 normal population | MMSE | SBPV | ↑SBPV → Speed of cognitive impairment↑ |
| McDonald, C. et al. [155] | Geriatric, UK | Prospective 5 years follow up | 353 normal population | MMSE, Cambridge Cognitive Examination (CAMCOG) | Day-time BPV | ↑SBPV, DBPV → Risk of cognitive impairment↑, Speed of cognitive impairment↑ |
| Nagai, M. et al. [156] | Geriatric, Japanese | Prospective 1 year follow up | 201 patients high risk for CVD | MMSE | Long-term BPV Short-term BPV | ↑long-term BPV → Risk of cognitive dysfunction↑ |
| Yildirim, E. et al. [157] | Geriatric, Turkish | Prospective 1 year follow up | 435 hypertensive patients | Standardized mini mental test (sMMT) | Short-term BPV | ↑short-term BPV → Risk of cognitive dysfunction↑ |
| Tsang, S. et al. [158] | Middle-aged to geriatric, American | Cross section | Normal cognition: 94 | MMSE, Computer Assessment of Mild Cognitive Impairment (CAMCI) | SBPV, DBPV | No association of BPV and dementia |
| van Middelaar, T. et al. [159] | Geriatric, Dutch | Prospective 6.4 (SD 0.8) years follow up | 2305 normal population | MMSE | Long-term BPV | No association of BPV and dementia |
| Qin, B. et al. [160] | Middle-aged to geriatric, Chinese | Prospective 3.2 years follow up | 976 normal population | Telephone Interview for Cognitive Status–modified (TICS-m) | Long-term BPV | ↑long-term BPV → Risk of cognitive dysfunction↑ in middle-aged; but no association in geriatric patients |
| Alpérovitch, A. et al. [161] | Geriatric, French | Prospective 8 years follow up | 6506 normal population | MMSE | Long-term SBPV | ↑SBPV → Risk of dementia↑ |
| Epstein, N.U. et al. [162] | Middle-aged to geriatric, American | Prospective 3 years follow up | Normal cognition: 181 MCI 247 | MMSE, CDR, ADAS-COG, Trail B, Digit Symbol Test, Rey auditory learning test | Long-term BPV | ↑Long-term SBPV → Risk cognitive dysfunction ↑ |
| Zhou, T.L. et al. [163] | Middle-aged to geriatric, American | Cross section | 1804 normal population | Memory function Processing speed Executive function | Ultra-short BPV Daily BPV Long-term BPV | ↑ultra-short, ↑daily SBPV, ↑DBPV → Cognitive performance↓ |
| Rouch, L. et al. [164] | Geriatric, French | Prospective 3 years follow up | 3319 normal population | MMSE | Long-term SBPV Long-term DBPV MAP, PPV | ↑long-term SBPV, long-term DBPV → Risk of dementia↑ |
| Sabayan, B. et al. [165] | Geriatric, European | Prospective 3.2 years follow up | 5461 patients with CV risk without cognitive impairment | Stroop color and word test, letter-digit coding test, picture-word learning test, | SBP, DBP Long-term SBPV Long-term DBPV DBPV | ↑long-term BPV → Risk of cognitive impairment↑ |
| Yoo, J.E. et al. [166] | Korean data base | Retrospective 6.2 years follow up | 7,844,814 patients | Diagnosis of dementia | SBPV, DBPV | ↑long-term BPV → Risk of all dementia↑, AD↑, VaD↑ |
| Lattanzi, S. et al. [167] | Geriatric, Italian | Prospective 12 months follow up | 240 patients with dementia | MMSE | SBP, DBP, SBPV, DBPV | ↑SBPV → Progression of cognitive decline↑ |
| Sible, I.J. et al. [168] | Middle-aged to geriatric American and Canadian | Prospective 12 months follow up | 681 normal cognition 479 MCI 261 AD | MMSE, CDR | SBP, DBP, BPV, Long-term BPV | In AD patients there is↑BPV ↑BPV → ↑progression in MCI |
| Lattanzi, S. et al. [169] | Geriatric, Italian | Prospective 12 months follow up | 248 AD 81 FTD | MMSE | BP, BPV | ↑SBPV → ↑progression in AD |
| Yano, Y. et al. [178] | Young adult, American | Prospective 25 years follow up | 5115 normal population | SBP, DBP Long-term BPV | ↑BPV in early age → ↓hippocampal volume and integrity |
| Author and Year | Follow up after Stroke | Case Numbers | Special Condition | Outcome Measure | Blood Pressure | Result |
|---|---|---|---|---|---|---|
| Gong, L. et al. [186] | Prospective, 6 months follow up | 141 | Early PSCI | MoCA | SBP | ↑Acute phase SBP →↓ Cognitive performance |
| He, M. et al. [187] | Prospective, 12 months follow up | 796 | MoCA | SBP, DBP Ultra-short BPV Daily BPV Long-term BPV | High and lower SBP → Risk of early PSCI↑ | |
| Levine, D.A. et al. [188] | Cross section, 90 days after stroke | 432 | Non-demented No cognitive impairment | Modified MMSE, Trails A, and Trails B | SBP, DBP, PP, MAP | Lower DBP →Lower trails B score |
| Yamamoto, Y. et al. [189] | Prospective, 4.1 years follow up | 249 | MMSE | Home BP (HBP) | ↑HBP → Risk of late PSCI↑ | |
| Sachdev, P.S., et al. [190] | Cross section, 3-6 months after stroke Case control | 169 stroke 103 Control | Comprehensive Neuropsychological Assessment | Diagnosis of Hypertension | Hypertension is not a risk factor for PSCI | |
| Ihle-Hansen, H. et al. [191] | Prospective, 1 ear follow up | 166 | First-ever stroke | Diagnosis of MCI Diagnosis of dementia | SBP, DBP | No association of BP level and dementia or MCI |
| Lu, Z.H. et al., [192] | Prospective, 6 months follow up | 232 | First-ever stroke | MoCA | Diagnosis of hypertension | Hypertension with hyperhomocysteinemia → Risk of early PSCI↑; but not in HTN only patients |
| Geng, S., et al. [193] | Prospective, 12 months follow up | 796 | MoCA | SBP, DBP SBPV, DBPV | ↑early SBPV→ Risk of late PSCI↑ | |
| Lee, J.H. et al. [194] | Prospective 3 months follow up | 36 | Lacunar infarction | MMSE, Controlled Oral Word Association Test, Digit Symbol Coding test | DBPV, SBPV | ↑early SBPV→ Risk of early PSCI↑, especially frontal lobe dysfunction |
| Kim, Y., et al. [195] | Prospective, 2.6 years follow up | 746 | MMSE, MoCA | SBP, DBP SBPV, DBPV | ↑BPV→ Risk of late PSCI ↑ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.-P.; Chang, A.Y.W.; Sung, P.-S. Association between Blood Pressure, Blood Pressure Variability, and Post-Stroke Cognitive Impairment. Biomedicines 2021, 9, 773. https://doi.org/10.3390/biomedicines9070773
Lee K-P, Chang AYW, Sung P-S. Association between Blood Pressure, Blood Pressure Variability, and Post-Stroke Cognitive Impairment. Biomedicines. 2021; 9(7):773. https://doi.org/10.3390/biomedicines9070773
Chicago/Turabian StyleLee, Kang-Po, Alice Y. W. Chang, and Pi-Shan Sung. 2021. "Association between Blood Pressure, Blood Pressure Variability, and Post-Stroke Cognitive Impairment" Biomedicines 9, no. 7: 773. https://doi.org/10.3390/biomedicines9070773
APA StyleLee, K.-P., Chang, A. Y. W., & Sung, P.-S. (2021). Association between Blood Pressure, Blood Pressure Variability, and Post-Stroke Cognitive Impairment. Biomedicines, 9(7), 773. https://doi.org/10.3390/biomedicines9070773