
Diagnostic Value of Conventional PET Parameters and Radiomic Features Extracted from 18F-FDG-PET/CT for Histologic Subtype Classification and Characterization of Lung Neuroendocrine Neoplasms


 ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Inclusion Criteria
2.2. Clinical Evaluation and Lu-NEN Classification
2.3. PET/CT Protocol
2.4. Conventional PET Parameters and RFs Extraction
- Four conventional and volumetric PET parameters (SUVmax, SUVmean, metabolic tumor volume (MTV) and total lesion glycolysis (TLG)). The MTV represents the volume of the segmented VOI; TLG is calculated by multiplying the MTV of each lesion with its corresponding SUVmean value [29];
- Forty-one RFs: six descriptors of the image intensity histogram: HISTO_Skewness (asymmetry), HISTO_Kurtosis (flatness), HISTO_ExcessKurtosis (peakedness), HISTO_Energy (uniformity), HISTO_Entropy_log2, and _log10 (randomness); three shape-based features that describe the shape of the VOI: SHAPE_Sphericity, SHAPE_Surface (mm2), and SHAPE_Compacity; thirty-two textural features: (a) seven features from the grey-level co-occurrence matrix (GLCM): describing the correlation between a pair of voxels in 13 directions of a three-dimensional space; (b) eleven features from the grey-level run-length matrix (GLRLM): describing the number and length of the run with a certain level of grey in 13 directions of a three-dimensional space; (c) eleven features from the grey-level zone length matrix (GLZLM): describing the number and size of the zone with a certain level of grey in 13 directions of a three-dimensional space; and (d) three features from the neighborhood grey-level different matrix (NGLDM): describing the difference between a voxel and its connected neighbors.
2.5. Statistical Analysis
2.5.1. Conventional PET Parameters
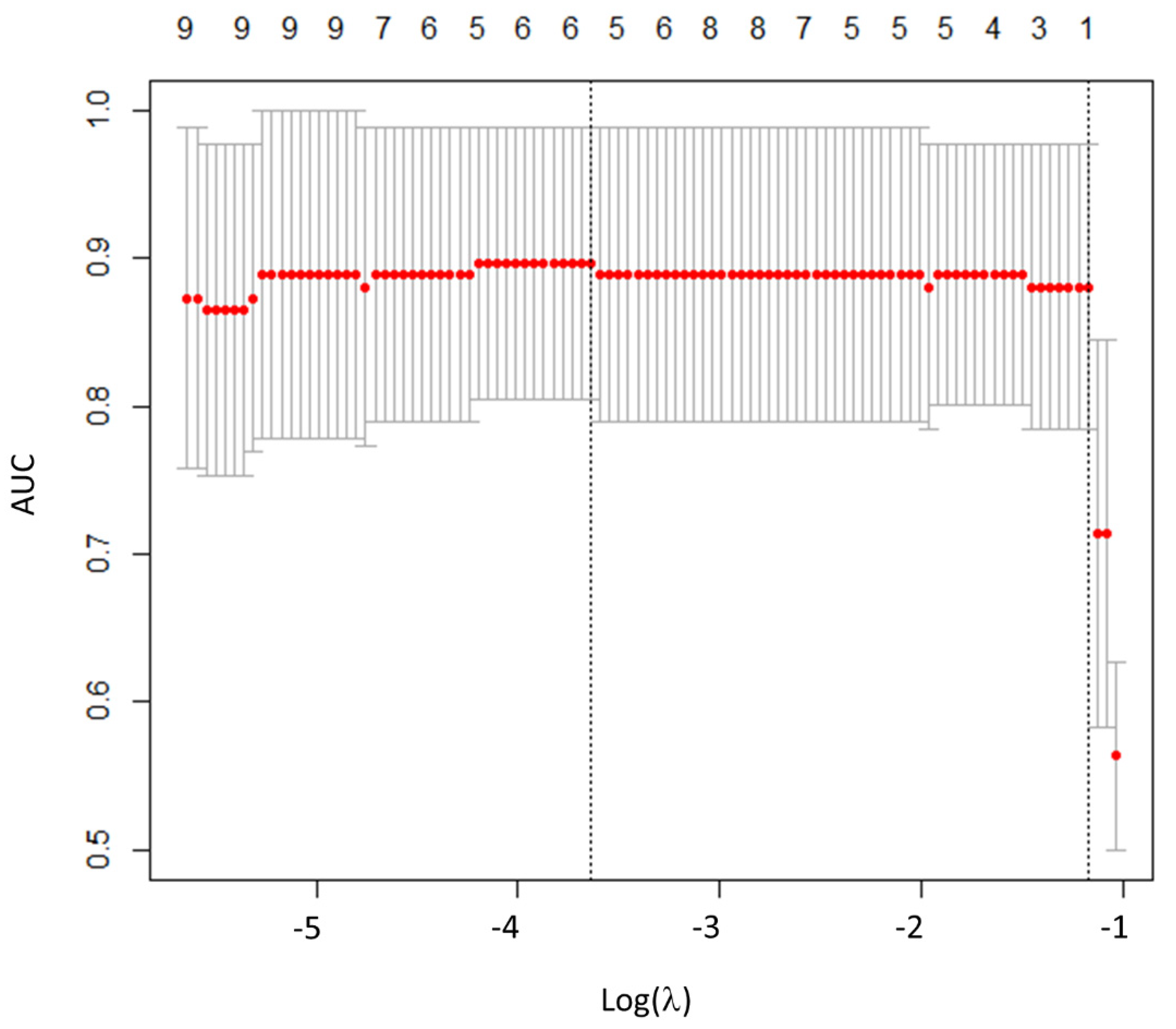
2.5.2. Radiomics Features Selection
3. Results
3.1. Patient Population
3.2. Tumor Subtypes Classification According to Histology
3.2.1. Lu-NECs vs. Lu-NETs
3.2.2. Lu-NETs: Typical vs. Atypical Carcinoid Tumors
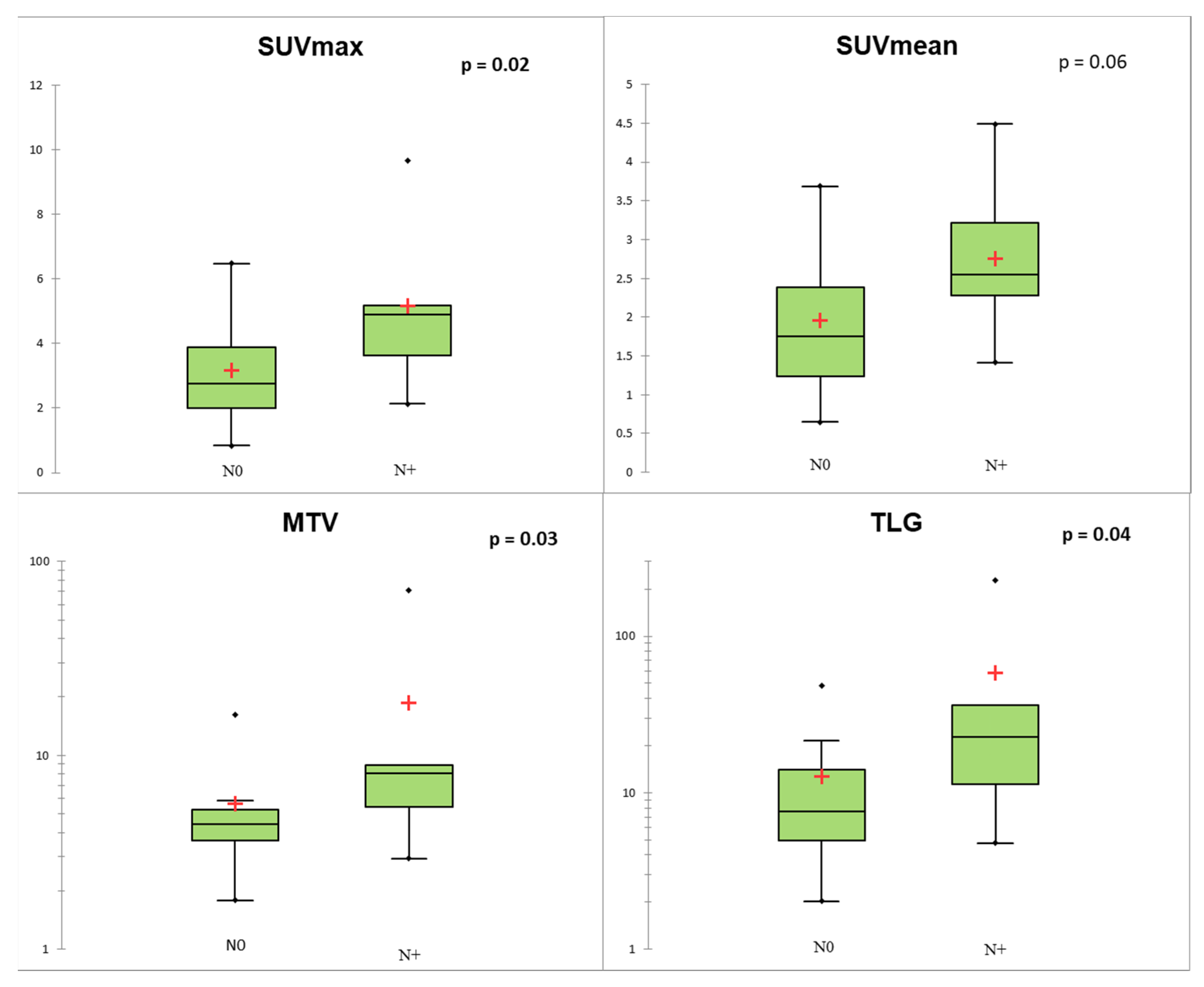
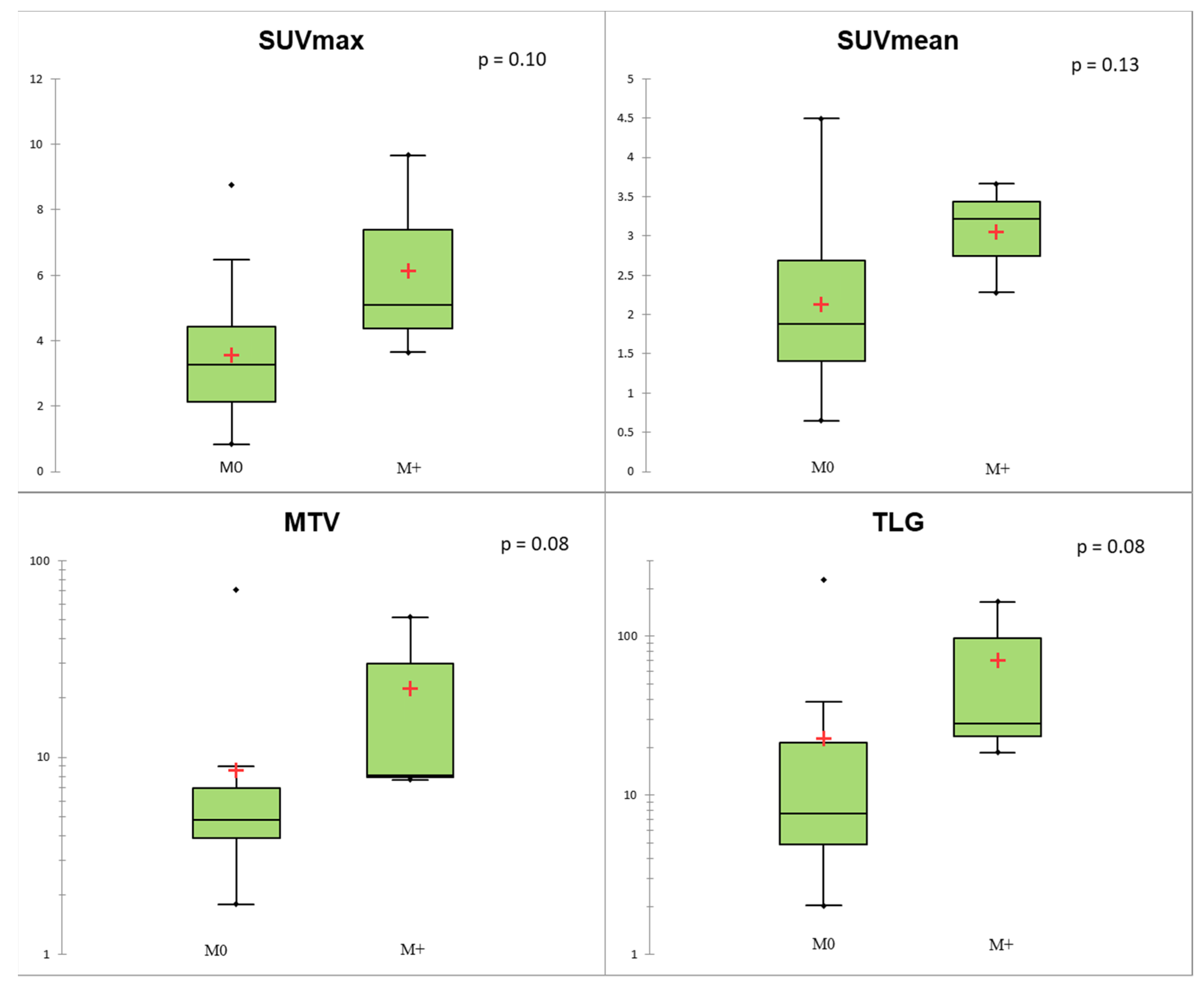
3.3. Comparison between Histological Data and TNM Status in Lu-NETs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef]
- Skuladottir, H.; Hirsch, F.R.; Hansen, H.H.; Olsen, J.H. Pulmonary neuroendocrine tumors: Incidence and prognosis of histological subtypes. A population-based study in Denmark. Lung Cancer 2002, 37, 127–135. [Google Scholar] [CrossRef]
- Filosso, P.L.; Ferolla, P.; Guerrera, F.; Ruffini, E.; Travis, W.D.; Rossi, G.; Lausi, P.O.; Oliaro, A. Multidisciplinary management of advanced lung neuroendocrine tumors. J. Thorac. Dis. 2015, 7, S163–S171. [Google Scholar] [PubMed]
- Hilal, T. Current understanding and approach to well differentiated lung neuroendocrine tumors: An update on classification and management. Ther. Adv. Med Oncol. 2017, 9, 189–199. [Google Scholar] [CrossRef]
- Grøndahl, V.; Binderup, T.; Langer, S.; Petersen, R.; Nielsen, K.; Kjaer, A.; Federspiel, B.; Knigge, U. Characteristics of 252 patients with bronchopulmonary neuroendocrine tumours treated at the Copenhagen NET Centre of Excellence. Lung Cancer 2019, 132, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Hou, G.; Cheng, W. The utility of 18F-FDG and 68Ga-DOTA-Peptide PET/CT in the evaluation of primary pulmonary carcinoid. Medicine 2019, 98, 4769. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, M.F.; Virgolini, I.; Balogova, S.; Beheshti, M.; Rubello, D.; Decristoforo, C.; Ambrosini, V.; Kjaer, A.; Delgado-Bolton, R.; Kunikowska, J.; et al. Guideline for PET/CT imaging of neuroendocrine neoplasms with 68Ga-DOTA-conjugated somatostatin receptor targeting peptides and 18F–DOPA. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1588–1601. [Google Scholar] [CrossRef]
- Abgral, R.; Leboulleux, S.; Déandreis, D.; Aupérin, A.; Lumbroso, J.; Dromain, C.; Duvillard, P.; Elias, D.; De Baere, T.; Guigay, J.; et al. Performance of 18Fluorodeoxyglucose-Positron Emission Tomography and Somatostatin Receptor Scintigraphy for High Ki67 (≥10%) Well-Differentiated Endocrine Carcinoma Staging. J. Clin. Endocrinol. Metab. 2011, 96, 665–671. [Google Scholar] [CrossRef]
- Daniels, C.E.; Lowe, V.J.; Aubry, M.C.; Allen, M.S.; Jett, J.R. The Utility of Fluorodeoxyglucose Positron Emission Tomography in the Evaluation of Carcinoid Tumors Presenting as Pulmonary Nodules. Chest 2007, 131, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Pattenden, A.H.; Leung, M.; Beddow, E.; Dusmet, M.; Nicholson, A.G.; Shackcloth, M.; Mohamed, S.; Darr, A.; Naidu, B.; Iyer, S.; et al. Test performance of PET-CT for mediastinal lymph node staging of pulmonary carcinoid tumours. Thorax 2014, 70, 379–381. [Google Scholar] [CrossRef]
- Chong, S.; Lee, K.S.; Kim, B.T.; Choi, J.Y.; Yi, A.C.; Chung, M.J.; Oh, D.K.; Lee, J.Y. Integrated PET/CT of Pulmonary Neuroendocrine Tumors: Diagnostic and Prognostic Implications. Am. J. Roentgenol. 2007, 188, 1223–1231. [Google Scholar] [CrossRef] [PubMed]
- Kayani, I.; Conry, B.G.; Groves, A.M.; Win, T.; Dickson, J.; Caplin, M.; Bomanji, J.B. A Comparison of 68Ga-DOTATATE and 18F-FDG PET/CT in Pulmonary Neuroendocrine Tumors. J. Nucl. Med. 2009, 50, 1927–1932. [Google Scholar] [CrossRef] [PubMed]
- Jindal, T.; Kumar, A.; Venkitaraman, B.; Dutta, R.; Kumar, R. Role of68Ga-DOTATOC PET/CT in the Evaluation of Primary Pulmonary Carcinoids. Korean J. Intern. Med. 2010, 25, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Venkitaraman, B.; Karunanithi, S.; Kumar, A.; Khilnani, G.C.; Kumar, R. Role of 68Ga-DOTATOC PET/CT in initial evaluation of patients with suspected bronchopulmonary carcinoid. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 856–864. [Google Scholar] [CrossRef]
- Lococo, F.; Perotti, G.; Cardillo, G.; De Waure, C.; Filice, A.; Graziano, P.; Rossi, G.; Sgarbi, G.; Stefanelli, A.; Giordano, A.; et al. Multicenter Comparison of 18F-FDG and 68Ga-DOTA-Peptide PET/CT for Pulmonary Carcinoid. Clin. Nucl. Med. 2015, 40, e183–e189. [Google Scholar] [CrossRef]
- Hatt, M.; Tixier, F.; Pierce, L.; Kinahan, P.E.; Le Rest, C.C.; Visvikis, D. Characterization of PET/CT images using texture analysis: The past, the present… any future? Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 151–165. [Google Scholar] [CrossRef]
- Van Velden, F.H.P.; Cheebsumon, P.; Yaqub, M.; Smit, E.F.; Hoekstra, O.S.; Lammertsma, A.A.; Boellaard, R. Evaluation of a cumulative SUV-volume histogram method for parameterizing heterogeneous intratumoural FDG uptake in non-small cell lung cancer PET studies. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1636–1647. [Google Scholar] [CrossRef]
- Pugachev, A.; Ruan, S.; Carlin, S.; Larson, S.M.; Campa, J.; Ling, C.C.; Humm, J.L. Dependence of FDG uptake on tumor microenvironment. Int. J. Radiat. Oncol. 2005, 62, 545–553. [Google Scholar] [CrossRef]
- Van Baardwijk, A.; Bosmans, G.; Van Suylen, R.J.; Van Kroonenburgh, M.; Hochstenbag, M.; Geskes, G.; Lambin, P.; De Ruysscher, D. Correlation of intra-tumour heterogeneity on 18F-FDG PET with pathologic features in non-small cell lung cancer: A feasibility study. Radiother. Oncol. 2008, 87, 55–58. [Google Scholar] [CrossRef]
- Hockel, M.; Schlenger, K.; Aral, B.; Mitze, M.; Schaffer, U.; Vaupel, P. Association between tumor hypoxia and malignant progression in advanced cancer of the uterine cervix. Cancer Res. 1996, 56, 4509–4515. [Google Scholar]
- Kim, B.S.; Kim, S.J.; Pak, K. Diagnostic value of metabolic heterogeneity as a reliable parameter for differentiating malignant parotid gland tumors. Ann. Nucl. Med. 2016, 30, 346–354. [Google Scholar] [CrossRef]
- Budiawan, H.; Cheon, G.J.; Im, H.-J.; Lee, S.J.; Paeng, J.C.; Kang, K.W.; Chung, J.K.; Lee, D.S. Heterogeneity Analysis of 18F-FDG Uptake in Differentiating Between Metastatic and Inflammatory Lymph Nodes in Adenocarcinoma of the Lung: Comparison with Other Parameters and its Application in a Clinical Setting. Nucl. Med. Mol. Imaging 2013, 47, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuze, S.; Soussan, M.; Robert, C.; Barakat, C.; Buvat, I. A Freeware for Tumor Heterogeneity Characterization in PET, SPECT, CT, MRI and US to Accelerate Advances in Radiomics. J. Nucl. Med. 2017, 58, 1316. [Google Scholar]
- Han, Y.; Ma, Y.; Wu, Z.; Zhang, F.; Zheng, D.; Liu, X.; Tao, L.; Liang, Z.; Yang, Z.; Li, X.; et al. Histologic subtype classification of non-small cell lung cancer using PET/CT images. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 350–360. [Google Scholar] [CrossRef]
- Polverari, G.; Ceci, F.; Bertaglia, V.; Reale, M.L.; Rampado, O.; Gallio, E.; Passera, R.; Liberini, V.; Scapoli, P.; Arena, V.; et al. 18F-FDG Pet Parameters and Radiomics Features Analysis in Advanced Nsclc Treated with Immunotherapy as Predictors of Therapy Response and Survival. Cancers 2020, 12, 1163. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Burke, A.P.; Marx, A.; Nicholson, A.G. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart; International Agency for Research on Cancer: Lyon, France, 2015. [Google Scholar]
- Cattoni, M.; Vallières, E.; Brown, L.M.; Sarkeshik, A.A.; Margaritora, S.; Siciliani, A.; Filosso, P.L.; Guerrera, F.; Imperatori, A.; Rotolo, N.; et al. Improvement in TNM staging of pulmonary neuroendocrine tumors requires histology and regrouping of tumor size. J. Thorac. Cardiovasc. Surg. 2018, 155, 405–413. [Google Scholar] [CrossRef]
- Pelosi, G.; Sonzogni, A.; Harari, S.; Albini, A.; Bresaola, E.; Marchiò, C.; Massa, F.; Righi, L.; Gatti, G.; Papanikolaou, N.; et al. Classification of pulmonary neuroendocrine tumors: New insights. Transl. Lung Cancer Res. 2017, 6, 513–529. [Google Scholar] [CrossRef]
- Boellaard, R.R.; Bolton, D.R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Leijenaar, R.T.H.; Nalbantov, G.; Carvalho, S.; Van Elmpt, W.J.C.; Troost, E.G.C.; Boellaard, R.; Aerts, H.J.W.L.; Gillies, R.J.; Lambin, P. The effect of SUV discretization in quantitative FDG-PET Radiomics: The need for standardized methodology in tumor texture analysis. Sci. Rep. 2015, 5, 1075. [Google Scholar] [CrossRef] [PubMed]
- Orlhac, F.; Nioche, C.; Soussan, M.; Buvat, I. Understanding Changes in Tumor Texture Indices in PET: A Comparison between Visual Assessment and Index Values in Simulated and Patient Data. J. Nucl. Med. 2016, 58, 387–392. [Google Scholar] [CrossRef]
- Orlhac, F.; Soussan, M.; Chouahnia, K.; Martinod, E.; Buvat, I. 18F-FDG PET-Derived Textural Indices Reflect Tissue-Specific Uptake Pattern in Non-Small Cell Lung Cancer. PLoS ONE 2015, 10, 5063. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef]
- Traverso, A.; Wee, L.; Dekker, A.; Gillies, R. Repeatability and Reproducibility of Radiomic Features: A Systematic Review. Int. J. Radiat. Oncol. 2018, 102, 1143–1158. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Yin, G.; Zhang, Y.; Dai, D.; Liu, J.; Chen, P.; Zhu, L.; Ma, W.; Xu, W. Predictive Power of a Radiomic Signature Based on 18F-FDG PET/CT Images for EGFR Mutational Status in NSCLC. Front. Oncol. 2019, 9, 1062. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.; Liang, T.B.; Zhang, Q.; Guo, C.; Zhang, X.; Lao, M.; Shen, Y.; Xiao, W.; Ying, S.; Sun, K.; et al. Development of a Novel Multiparametric MRI Radiomic Nomogram for Preoperative Evaluation of Early Recurrence in Resectable Pancreatic Cancer. J. Magn. Reson. Imaging 2020, 52, 231–245. [Google Scholar] [CrossRef] [PubMed]
- R: A Language and Environment for Statistical Computing. Available online: https://www.gbif.org/fr/tool/81287/r-a-language-and-environment-for-statistical-computing (accessed on 7 September 2020).
- Lee, K.W.; Lee, Y.; Oh, S.W.; Jin, K.N.; Goo, J.M. Large cell neuroendocrine carcinoma of the lung: CT and FDG PET findings. Eur. J. Radiol. 2015, 84, 2332–2338. [Google Scholar] [CrossRef]
- Guezennec, C.; Bourhis, D.; Orlhac, F.; Robin, P.; Corre, J.B.; Delcroix, O.; Gobel, Y.; Schick, U.; Salaün, P.Y.; Abgral, R. Inter-observer and segmentation method variability of textural analysis in pre-therapeutic FDG PET/CT in head and neck cancer. PLoS ONE 2019, 14, 4299. [Google Scholar] [CrossRef]
- Hatt, M.; Majdoub, M.; Vallières, M.; Tixier, F.; Le Rest, C.C.; Groheux, D.; Hindié, E.; Martineau, A.; Pradier, O.; Hustinx, R.; et al. 18F-FDG PET Uptake Characterization Through Texture Analysis: Investigating the Complementary Nature of Heterogeneity and Functional Tumor Volume in a Multi-Cancer Site Patient Cohort. J. Nucl. Med. 2015, 56, 38–44. [Google Scholar] [CrossRef]
- Zidan, L.; Iravani, A.; Kong, G.; Akhurst, T.; Michael, M.; Hicks, R.J. Theranostic implications of molecular imaging phenotype of well-differentiated pulmonary carcinoid based on 68Ga-DOTATATE PET/CT and 18F-FDG PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 204–216. [Google Scholar] [CrossRef]
- Gasparri, R.; Rezende, G.C.; Fazio, N.; Maisonneuve, P.; Brambilla, D.; Travaini, L.L.; Paganelli, G.; Petrella, F.; Galetta, D.; Spaggiari, L. Fluorodeoxyglucose positron emission tomography in pulmonary carcinoid tumors. Q. J. Nucl. Med. Mol. Imaging. 2015, 59, 446–454. [Google Scholar]
- Tatci, E.; Ozmen, O.; Gökcek, A.; Biner, I.U.; Özaydin, E.; Kaya, S.; Arslan, N. 18F-FDG PET/CT rarely provides additional information other than primary tumor detection in patients with pulmonary carcinoid tumors. Ann. Thorac. Med. 2014, 9, 227. [Google Scholar] [CrossRef]
- Stefani, A.; Franceschetto, A.; Nesci, J.; Aramini, B.; Proli, C.; Kaleci, S.; Casolo, A.; Massi, L.; Casali, C.; Morandi, U. Integrated FDG-PET/CT imaging is useful in the approach to carcinoid tumors of the lung. J. Cardiothorac. Surg. 2013, 8, 223. [Google Scholar] [CrossRef]
- Rindi, G.; Klersy, C.; Inzani, F.; Fellegara, G.; Ampollini, L.; Ardizzoni, A.; Campanini, N.; Carbognani, P.; De Pas, T.M.; Galetta, D.; et al. Grading the neuroendocrine tumors of the lung: An evidence-based proposal. Endocr. Relat. Cancer 2014, 21, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Marchiò, C.; Gatti, G.; Massa, F.; Bertero, L.; Filosso, P.; Pelosi, G.; Cassoni, P.; Volante, M.; Papotti, M. Distinctive pathological and clinical features of lung carcinoids with high proliferation index. Virchows Arch. 2017, 471, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Rubino, M.; Scoazec, J.; Pisa, E.; Faron, M.; Spaggiari, L.; Hadoux, J.; Spada, F.; Planchard, D.; Cella, C.; Leboulleux, S.; et al. Lung carcinoids with high proliferative activity: Further support for the identification of a new tumor category in the classification of lung neuroendocrine neoplasms. Lung Cancer 2020, 148, 149–158. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Sex, n (%) | |
| Male | 23 (52.3) |
| Female | 21 (47.7) |
| Age (years); moy (DS) | 62.8 (10.1) |
| Lesion side, n (%) | |
| Right | 29 (63) |
| Left | 17 (37) |
| Size (mm); moy (DS) | 30.5 (16) |
| T-classification, n (%) | |
| 1 | 17 (37.0) |
| 2 | 11 (23.9) |
| 3 | 8 (17.4) |
| 4 | 0 (0) |
| X | 10 (21.7) |
| N-classification, n (%) | |
| 0 | 26 (56.5) |
| 1 | 20 (43.5) |
| M-classification, n (%) | |
| 0 | 41 (89.1) |
| 1 | 5 (10.9) |
| Histological subtypes | |
| TC | 15 (32.6) |
| AC | 11 (23.9) |
| TC or AC | 1 (2.2) |
| LCNEC | 16 (34.8) |
| SCLC | 3 (6.5) |
| Mitosis/mm2 (n = 35) | |
| <2 | 15 (42.8) |
| 2–10 | 10 (28.6) |
| 10/mm2 | 10 (28.6) |
| Ki67% (n = 45) | |
| ≤5% | 15 (33.3) |
| >5 and ≤20% | 10 (22.2) |
| >20% | 20 (44.4) |
| Lung-NETs * | Lung-NECs | p Value | p Value | |||||
|---|---|---|---|---|---|---|---|---|
| Total (n = 27) * | TC (n = 15) | AC (n = 11) | Total (n = 19) | LCNEC (n = 16) | SCLC (n = 3) | (NETs vs. NECs) | (TCs vs. ACs) | |
| SUVmax | 3.52 (0.84–9.66) | 3.62 (0.84–6.48) | 2.81 (1.84–9.66) | 10.71 (2.27–22.65) | 12.74 (2.27–22.65) | 10.52 (4.60–15.66) | <0.001 | 0.68 |
| SUVmean | 2.23 (0.65–4.49) | 2.37 (0.65–3.69) | 1.62 (1.13–4.49) | 6.14 (1.43–10.09) | 6.49 (1.43–10.09) | 5.97 (3.47–7.72) | <0.001 | 0.65 |
| MTV | 4.93 (1.79–70.91) | 4.93 (2.62–70.91) | 4.93 (1.79–51.39) | 27.01 (2.88–376.38) | 27.97 (2.88–376.38) | 9.09 (4.16–27.78) | <0.001 | 0.51 |
| TLG | 11.38 (2.03–226.1) | 11.68 (2.83–226.11) | 7.69 (2.03–70.91) | 167.74 (4.11–2578.64) | 185.00 (4.11–2578.64) | 54.21 (14.43–214.61) | <0.001 | 0.45 |
| HISTO_Entropy_log10 | 0.77 (0.27–1.26) | 0.77 (0.27–1.12) | 0.77 (0.49–1.26) | 1.3 (0.68–1.71) | 1.40 (0.68–1.71) | 1.30 (0.76–1.48) | <0.001 | 0.96 |
| Parameters | AUC | CI 95% | p Value | Cut-Off Value | Se (%) | Sp (%) | Acc (%) |
|---|---|---|---|---|---|---|---|
| SUVmax | 0.91 | (0.82–1.00) | <0.001 | 5.16 | 84.2 | 85.2 | 84.8 |
| SUVmean | 0.91 | (0.82–1.00) | <0.001 | 3.69 | 78.9 | 96.3 | 89.1 |
| MTV (ml) | 0.80 | (0.66–0.93) | <0.001 | 8.96 | 68.4 | 85.2 | 78.3 |
| TLG (g) | 0.86 | (0.74–0.97) | <0.001 | 38.67 | 78.9 | 88.9 | 84.8 |
| HISTO_Entropy_log10 | 0.90 | (0.81–0.99) | <0.001 | 0.94 | 89.5 | 77.8 | 82.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thuillier, P.; Liberini, V.; Rampado, O.; Gallio, E.; De Santi, B.; Ceci, F.; Metovic, J.; Papotti, M.; Volante, M.; Molinari, F.; et al. Diagnostic Value of Conventional PET Parameters and Radiomic Features Extracted from 18F-FDG-PET/CT for Histologic Subtype Classification and Characterization of Lung Neuroendocrine Neoplasms. Biomedicines 2021, 9, 281. https://doi.org/10.3390/biomedicines9030281
Thuillier P, Liberini V, Rampado O, Gallio E, De Santi B, Ceci F, Metovic J, Papotti M, Volante M, Molinari F, et al. Diagnostic Value of Conventional PET Parameters and Radiomic Features Extracted from 18F-FDG-PET/CT for Histologic Subtype Classification and Characterization of Lung Neuroendocrine Neoplasms. Biomedicines. 2021; 9(3):281. https://doi.org/10.3390/biomedicines9030281
Chicago/Turabian StyleThuillier, Philippe, Virginia Liberini, Osvaldo Rampado, Elena Gallio, Bruno De Santi, Francesco Ceci, Jasna Metovic, Mauro Papotti, Marco Volante, Filippo Molinari, and et al. 2021. "Diagnostic Value of Conventional PET Parameters and Radiomic Features Extracted from 18F-FDG-PET/CT for Histologic Subtype Classification and Characterization of Lung Neuroendocrine Neoplasms" Biomedicines 9, no. 3: 281. https://doi.org/10.3390/biomedicines9030281
APA StyleThuillier, P., Liberini, V., Rampado, O., Gallio, E., De Santi, B., Ceci, F., Metovic, J., Papotti, M., Volante, M., Molinari, F., & Deandreis, D. (2021). Diagnostic Value of Conventional PET Parameters and Radiomic Features Extracted from 18F-FDG-PET/CT for Histologic Subtype Classification and Characterization of Lung Neuroendocrine Neoplasms. Biomedicines, 9(3), 281. https://doi.org/10.3390/biomedicines9030281